Rationale: To address this knowledge gap by examining the relationship between impulsivity and planning/decision-making in OCD using the Tower of London (TOL) task using EEG.
Aim/Objective: This study aims to investigate the impact of impulsivity on planning and decision-making in OCD using EEG and the TOL task.
Hypothesis: Individuals with OCD will exhibit distinct patterns of latency and spectral power during the TOL task compared to controls, reflecting increased impulsivity and cognitive effort during decision-making.
Planning & decision-making in obsessive-compulsive disorder (OCD) through the lens of ERP: a comparative analysis
Overthinking: Necessity or Disruption?
Let's unpack the story of the decision-making and planning process in the brain for OCD
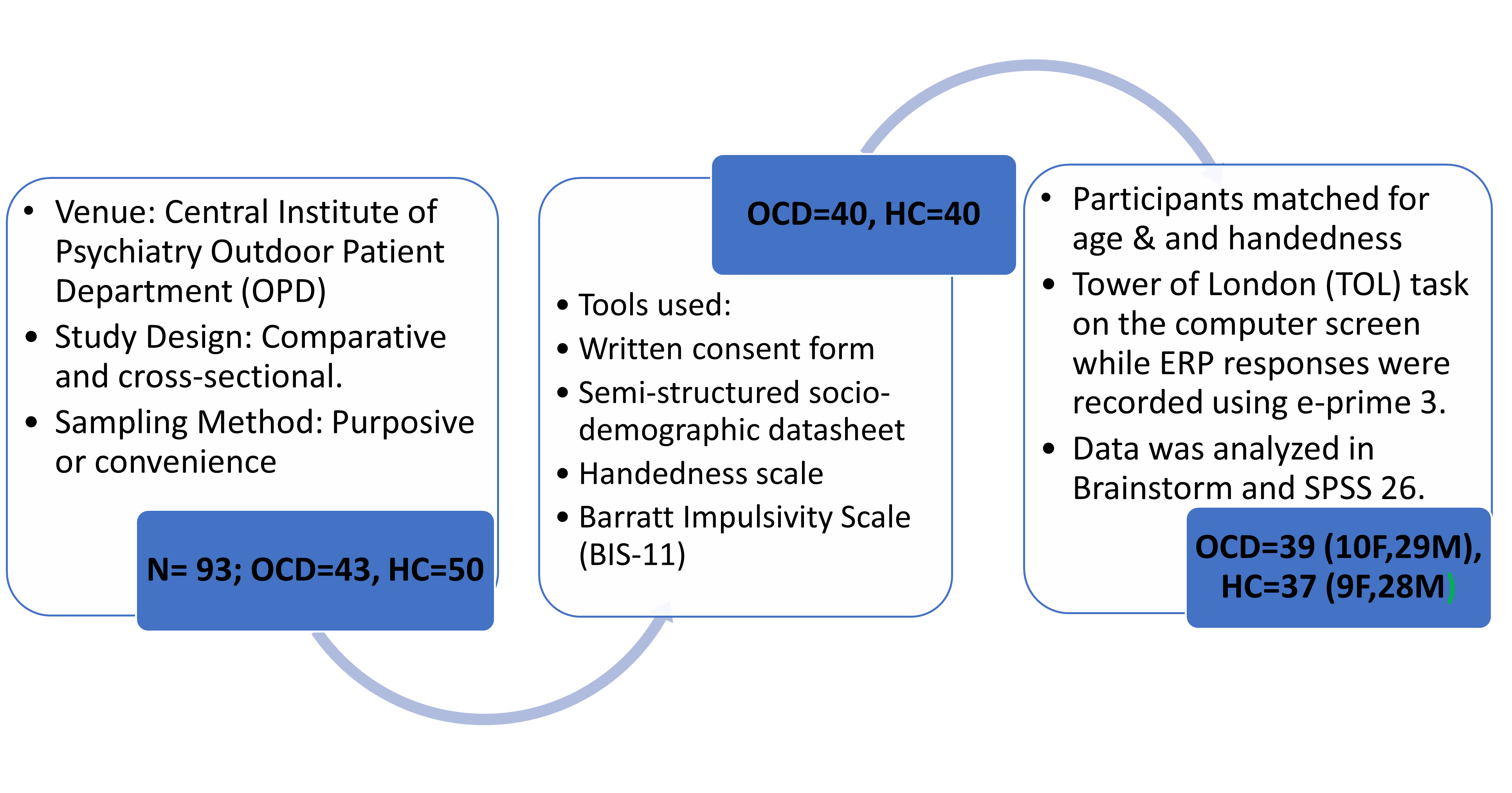
Methods:
Results
Mean Rank, Mann-Whitney U score, and 2-tailed significance level of TOL tasks’ (completed with 3, 4, 5 & 6 moves) amplitudes and latencies.| Variables | OCD (n=39) | Control (n=37) | ||
| Left Frontal | Mean Rank | Mean Rank | U score | Sig. 2-tailed |
| 3 moves Amplitude | 41.87 | 34.95 | 590.000 | .172 |
| 3 moves Latency | 21.91 | 55.99 | 74.500 | .001 |
| 4 moves Amplitude | 41.44 | 35.41 | 607.000 | .234 |
| 4 moves latency | 38.73 | 38.26 | 712.500 | .925 |
| 5 moves Amplitude | 38.27 | 38.74 | 699.000 | .815 |
| 5 moves latency | 42.56 | 34.22 | 563.000 | .099 |
| 6 moves Amplitude | 40.41 | 36.49 | 647.000 | .439 |
| 6 moves Latency | 39.95 | 36.97 | 665.000 | .557 |
| Total Amplitude | 38.44 | 38.57 | 719.000 | .979 |
| Total Latency | 39.44 | 37.51 | 685.000 | .704 |
- The groups could be matched for age & handedness.
- The OCD group scored significantly higher than the control group in domains of attention, planning & total scores in the BIS-11 scale indicative of relatively poor sustained attention and impulsive planning in the OCD group than HCs.
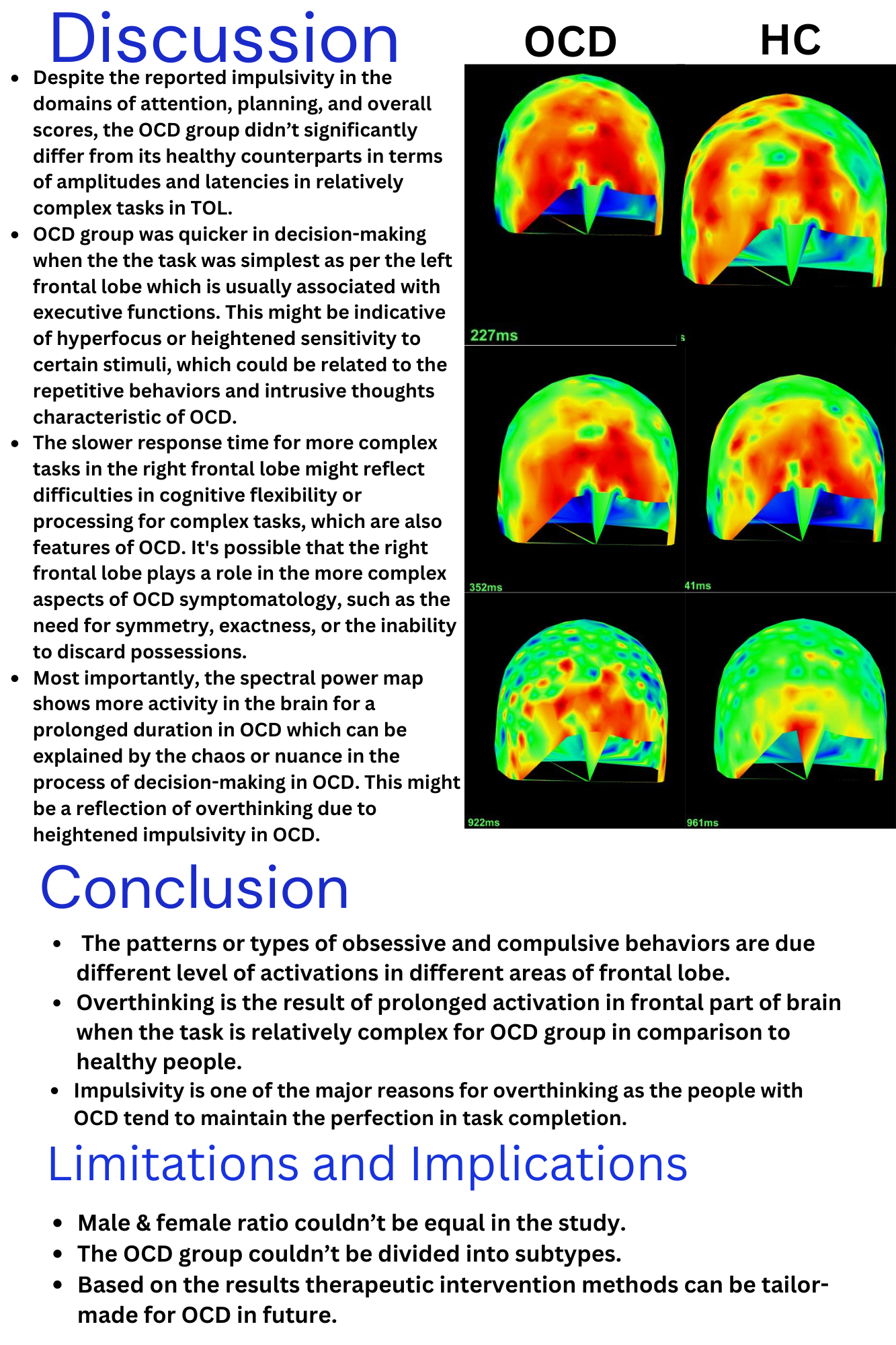
- In the left frontal, the latency for the least complex task (3 moves) was significantly higher in the control group.
- There were no significant differences in amplitude or latencies for more complex tasks.
Weill-Marchesani Syndrome – a rare etiology for bilateral carpal tunnel syndrome in children
INTRODUCTION
- Evaluation of neurological symptoms in a child differs from adults; for example, the presentation of carpal tunnel syndrome in children warrants careful considerations of secondary underlying etiologies
- We present a case of a five-year-old female with bilateral hand motor and sensory symptoms with accompanying skeletal and ocular abnormalities
- This case illustrates the importance of systemic evaluation in neurologic presentations. Understanding the underlying cause of otherwise common presentations is paramount to guide management and counseling.
CASE REPORT
- A five-year-old female presented with a three-year history of progressive difficulty with fine motor tasks involving the bilateral index and thumb, such as holding a pencil or cutlery and managing zippers or buttons
- other symptoms include: difficulty flexing the PIP and DIP joints of all fingers (excluding the thumb) on the right and index and long fingers on the left, lack of pain sensation when removing splinters lodged in the thumb and index fingers, use of ring finger to sense the temperature of items, stiffness in both her wrist and ankle joints
- Otherwise a normal developing child
- Physical exam: height averaged in the 10-20th percentile and her weight averaged in the 40-50th percentile, normal facial features and range of motion in wrists and ankles, dactylitis, bilateral thenar wasting, bilateral restriction of flexor tendon movement at the level of A1 and A2 pulleys with components of pulley and tendon thickening leading to both incomplete finger flexion and extension deficits at the level of distal interphalangeal joints in her index and long fingers, bilateral weakness of the abductor pollicus brevis (MRC 2-3/5) and decreased sensation to light touch in the thumb, index, and long fingers
- see Table 1 for investigations
- patient underwent bilateral carpal tunnel release and neurolysis of the median nerves. In the same operation, she also had bilateral index and long finger pulley release and tenosynovectomy (Figure 1)
- However, she continued to have neurological symptoms and a repeat procedure was done 2 years later. After her second operation, she continues to have neurological symptoms.
Figure 1. Intra-operative photograph of first carpal tunnel release procedure. Note the excessive connective tissue obsuring the view of the carpal tunnel.

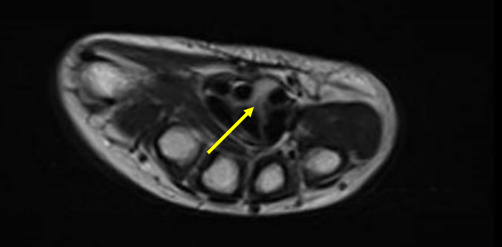
Figure 2. Pre and Post-operative neuromuscular ultrasound of bilateral median nerves (yellow arrow) at the carpal tunnel
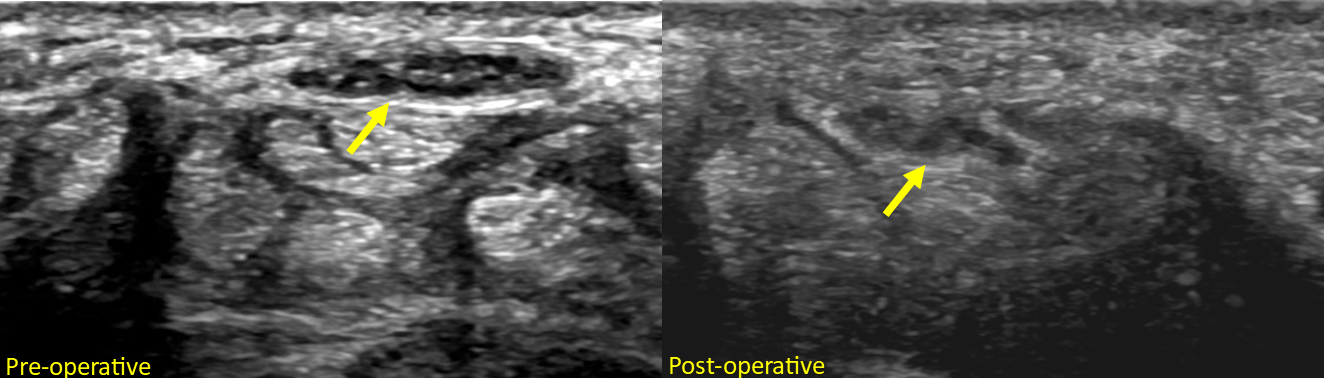
Table 1. Investigations
| Investigations | Outcome |
|
Trio whole exome sequencing
|
two de novo likely pathogenic variants in ADAMTS10: c.1174delC, p.H392TfsX9 and a deletion of exons 3-8 |
| Neuromuscular ultrasound bilateral wrists |
pre-operative (Figure 2):
|
| Nerve Conduction Studies |
pre-operative:
|
| MRI of the right wrist |
pre-operative (Figure 3):
|
DISCUSSION
- Carpal tunnel syndrome (CTS) is less common in children compared to adults but can be associated with significant morbidity
- In adults, most common causes are mechanical trauma and ischemic damage to the nerve, in children this is more likely to be associated with a secondary condition such as metabolic storage diseases (i.e. mucopolysaccharidoses (MPS)), familial syndromes (i.e. familial carpal tunnel syndrome), genetic syndromes (i.e. Weill–Marchesani Syndrome (WMS), Hereditary neuropathy with liability to pressure palsies, other causative genes include COMP, BGN, ACAN, COL5A1, and IL6R), anatomical variants (i.e. skeletally smaller carpal tunnel), intrinsic nerve tumors (perineuriomas, neurolipomatosis), and extrinsic compressive lesions (cysts)
- WMS is a genetic connective tissue disorder with manifestations including brachydactyly, camptodactyly, thickened skin, ocular abnormalities and short stature
- Mutation of ADAMTS10 can cause aberrant fibrillin microfibrils and lead to tenosynovial thickening which can compress the median nerve within the carpal tunnel
- Identifying WMS as the etiology for CTS has significant implications on management, particularly when considering surgical options. Open carpal tunnel release is the most common approach for children with CTS, and in the case of MPS, early intervention may improve functional outcomes. However, due to the relative rarity of WMS and the underlying structural abnormalities, less is known regarding the outcomes of surgery
- In the case of our patient, surgery provided some improvement seen on NCS and imaging, but she had remaining significant deficits. Potential causes include prolonged nerve compression resulting in no or little reinnervation potential, inadequate decompression, or the nerve being compressed/injured intrinsically. In the case of the latter etiology, secondary surgeries could be considered to improve function (e.g. gain more thumb abduction/opposition)
- Awareness of this diagnosis would allow for better patient counseling and informed management decisions
Figure 3. pre-operative MRI of the right wrist at the carpal tunnel (T2, axial). Note the loss of normal nerve architecture of the median nerve.
fMRI-based deep brain stimulation programming: a blinded, crossover clinical trial
Background
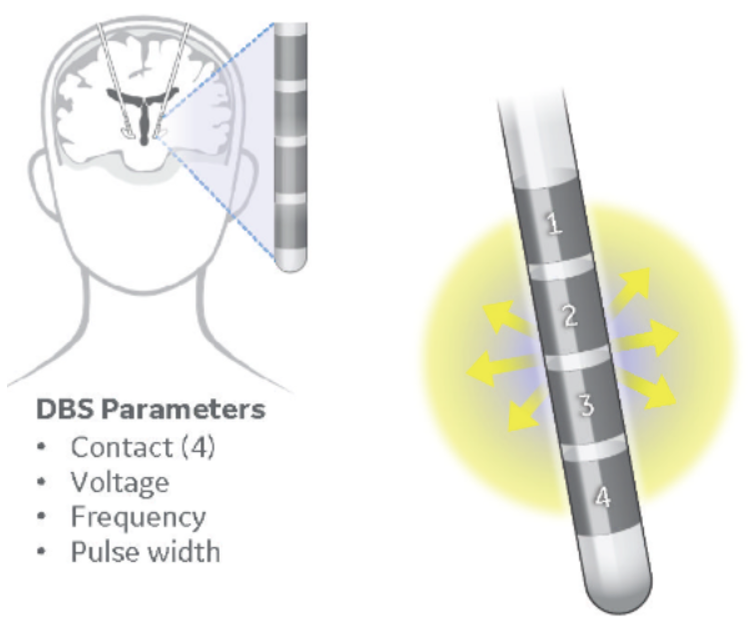
Deep brain stimulation (DBS) success relies on careful titration of stimulation settings.
There is often a delay between setting changes and visible clinical response.
There is often a delay between setting changes and visible clinical response.
- Making features like bradykinesia, axial instability, cognitive… difficult to optimally treat during limited clinical visits.
Current trial-and-error optimization can require >1yr of frequent/costly specialist appointments.
An objective rapidly acquired biomarker of stimulation success is desirable.
Together with improved construction of DBS hardware, our group has developed and tested a safe fMRI acquisition protocol during stimulation.
Uses the standard Medtronic programmer and MRI operational software. No special equipment required.
An objective rapidly acquired biomarker of stimulation success is desirable.
Together with improved construction of DBS hardware, our group has developed and tested a safe fMRI acquisition protocol during stimulation.
Uses the standard Medtronic programmer and MRI operational software. No special equipment required.

Optimal stimulation settings result in an identifiable pattern of functional network engagement.
Acute changes fMRI response is predictive of long-term outcome, preceding changes in symptoms that may take hours/days to reappear.
Acute changes fMRI response is predictive of long-term outcome, preceding changes in symptoms that may take hours/days to reappear.
Objective
Prospectively compare fMRI-based stimulation optimization with >1yr of standard-of-care (SoC) programming in a double-blind, crossover, non-inferiority trial.
Study Design
22 PD STN-DBS subjects prospectively enrolled for fMRI prior to SoC stimulation optimization.
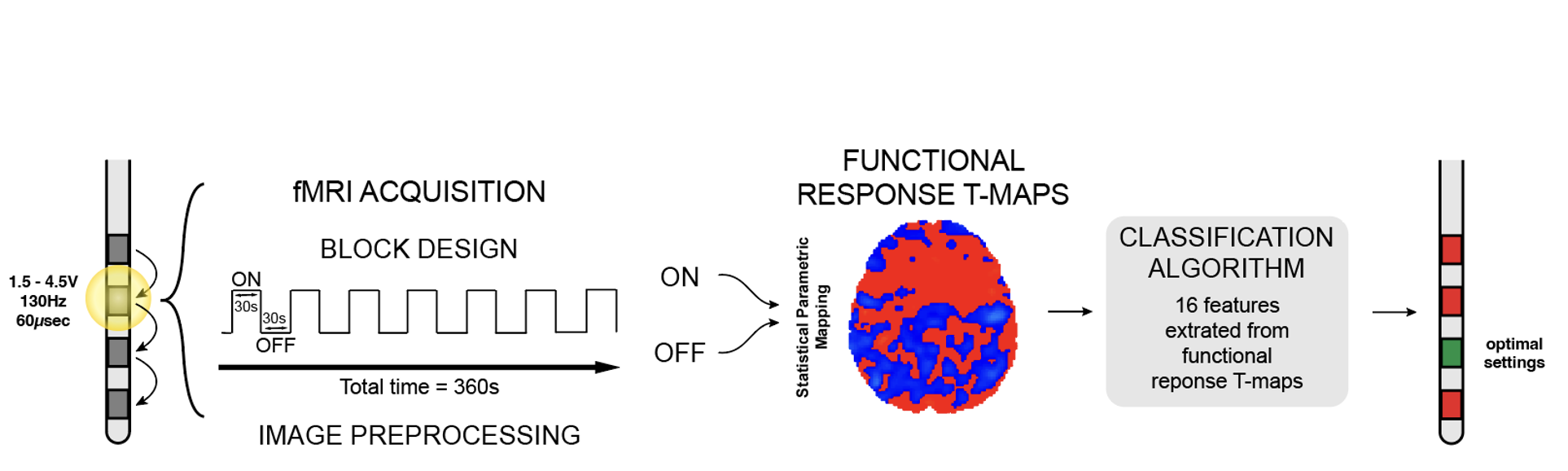
Enrolled subjects underwent STN-DBS implantation and fMRI optimal contact and voltage screening. fMRI was acquired in a stimulation-block design, where functional response t-maps are formed by comparing stimulation-ON and OFF blocks. T-maps undergo feature extraction and classification with a published model to identify optimal settings.
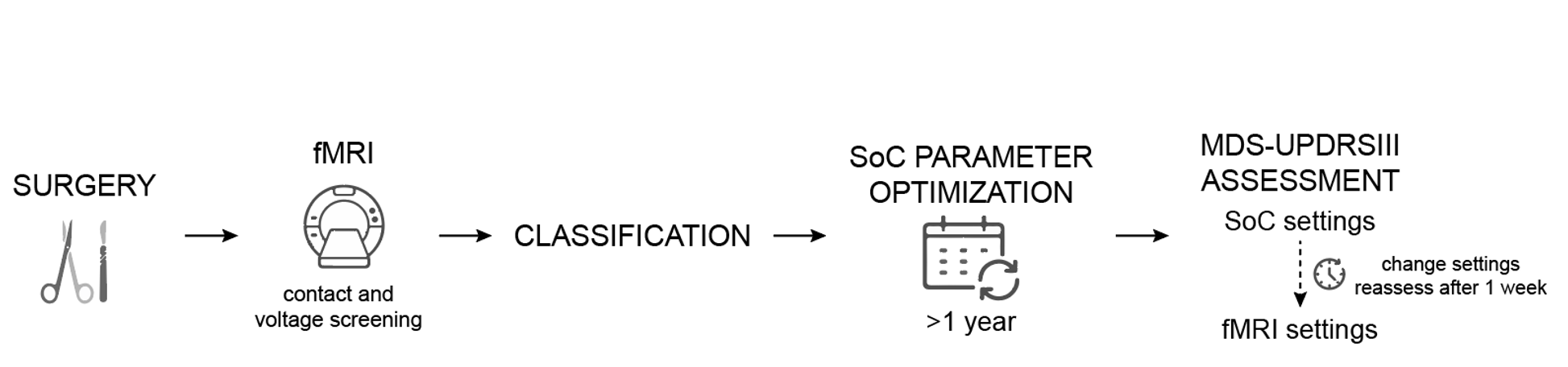
All subjects underwent 1 year of SoC clinical programming before assessment on SoC settings and fMRI-based settings.
Subjects were examined after 1wk on settings to ensure washout and stimulation effect. Subject and examiner blinded to setting change.
A 5-point difference was deemed clinically significant.
Subjects were examined after 1wk on settings to ensure washout and stimulation effect. Subject and examiner blinded to setting change.
A 5-point difference was deemed clinically significant.
Funding Sources

Results
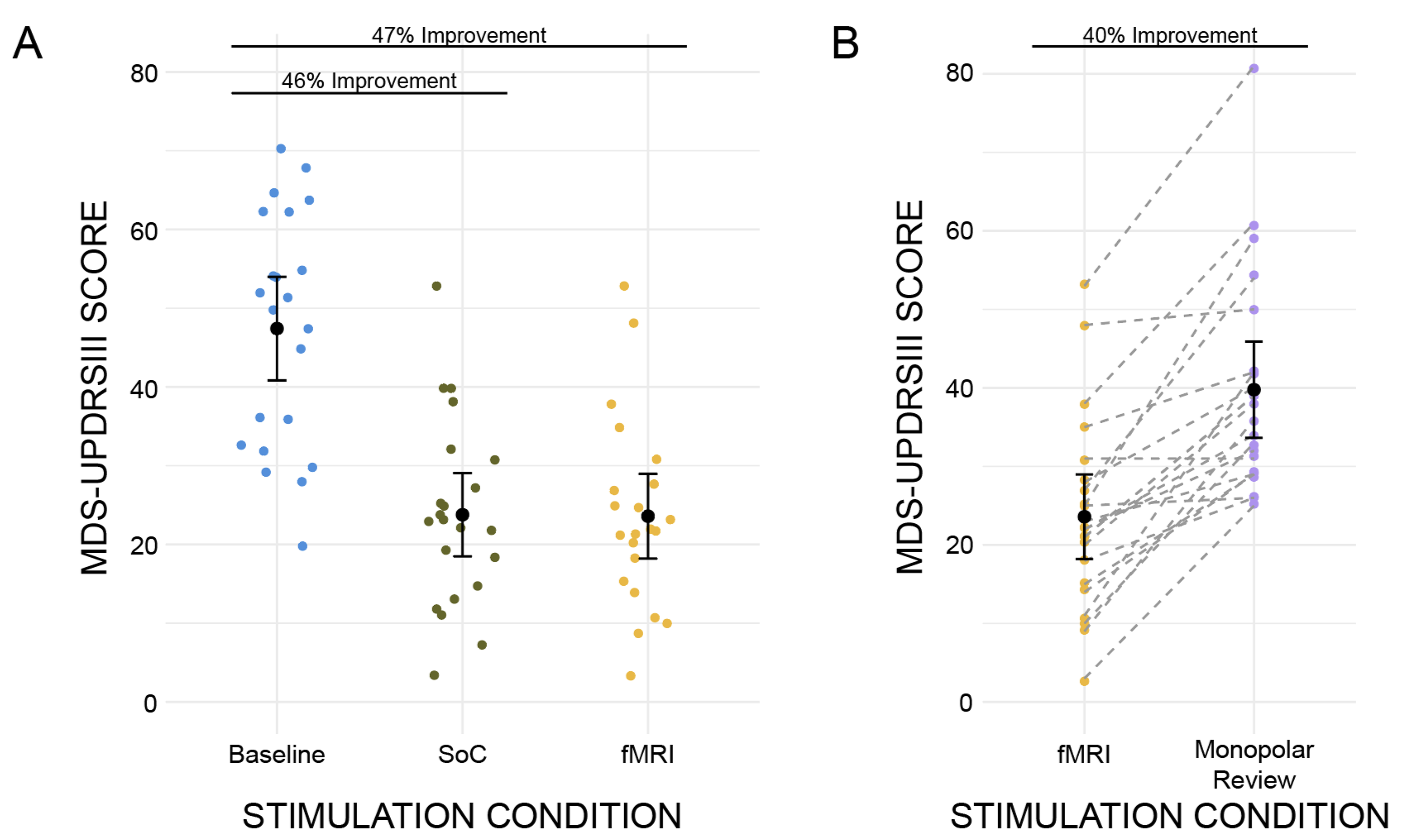
- Average of 15mo (SD=4) of SoC programming before comparison.
- fMRI matched the same left and right contact as SoC in 50%
- Significant improvement in both SoC and fMRI conditions.
- fMRI condition is significantly better than negative control from monopolar review (p<0.001).
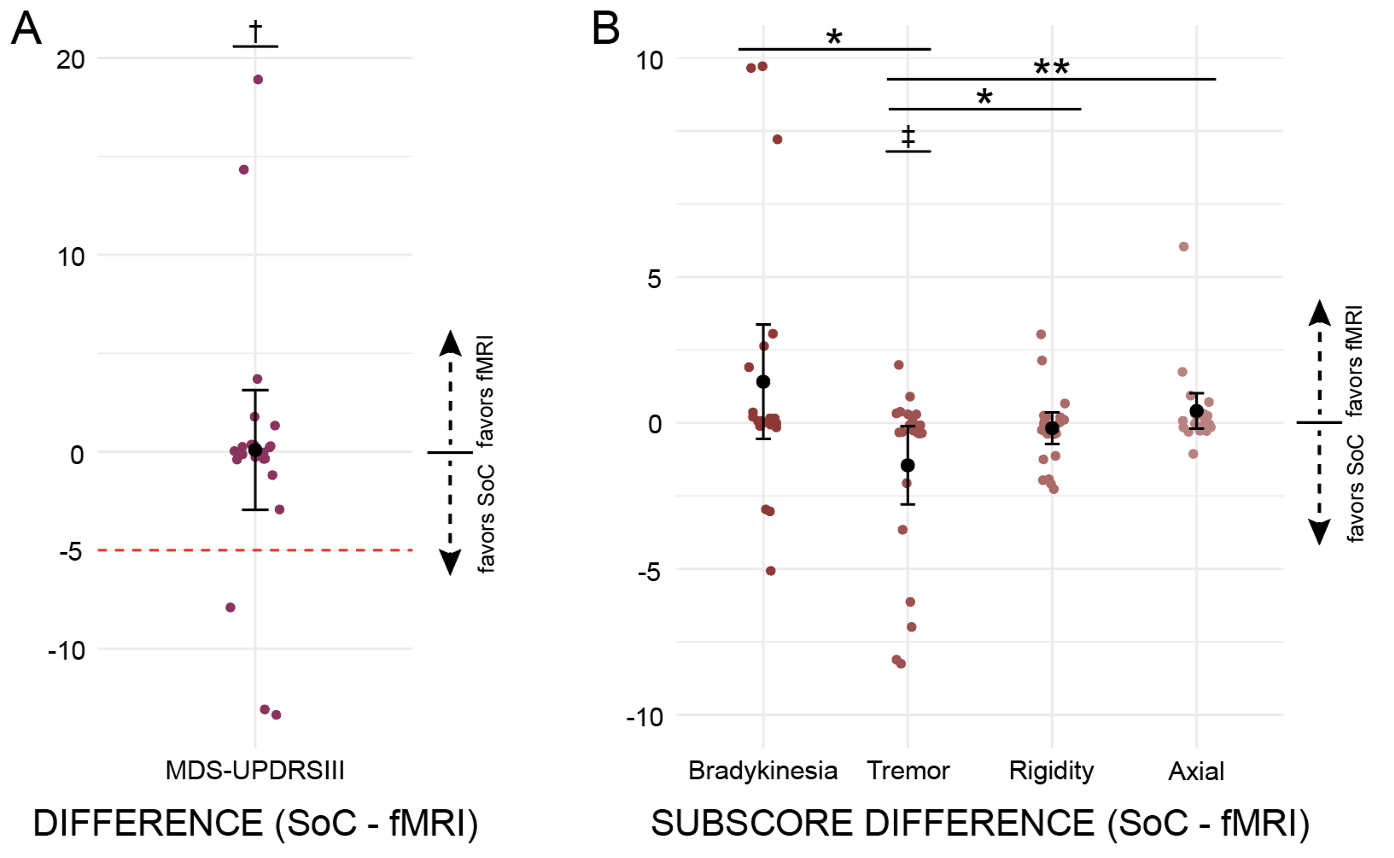
- Mean difference in scores was 0.1 (SD=6.9, 95% CI -3 to 3.1).
- Non-inferiority margin not contained within the 95% CI (p=0.001).
- Tremor improvement is better with SoC (p=0.017).
- Bradykinesia and axial improvement trend towards favoring fMRI.
Conclusion
- Data suggests fMRI-based programming may be non-inferior to conventional clinical programming.
- Tremor improvement may be better with SoC programming. However, improvements in bradykinesia and axial instability may be better with fMRI.
- Equivalent overall outcomes may be achieved in 3hrs of early post-op fMRI vs 1yr SoC.
Spinal Cord Demyelination Predicts Neurological Deterioration in Patients with Mild Degenerative Cervical Myelopathy
Introduction
- Degenerative Cervical Myelopathy (DCM) is the most common form of non-traumatic spinal cord injury worldwide [1].
- DCM diagnosis implies a neurological impairment due to spinal cord compression from degenerative breakdown of spinal structures [2].
- Neurological symptoms include: gait imbalance, numbness in the hands, sphincter dysfunction, and pain in the upper extremities [3].
- The only current treatment for DCM that is symptomatically progressive or severe is surgery.
- It is unclear whether patients exhibiting mild symptoms (mild DCM) will benefit from surgery or not. Most mild DCM patients are non-operatively managed.
- There is a large gap in clinical literature surrounding whether surgery will benefit patients with mild DCM.
- Purpose: We aim to develop a supervised machine learning model capable of identifying mild DCM patients at risk of neurological deterioration.
Methods
- 49 mild DCM patients underwent MRI scans, including T2w, diffusion tensor imaging (DTI), and magnetization transfer (MT) scans, along with a series of clinical metrics.
- Quantitative MRI metrics were derived above and below the maximally compressed cervical level.
- Random forest classifier, support vector machine, and logistic regression models were trained and tested to predict six-month neurological deterioration
- SHAP and LIME model interpretation were used to extract feature importance at the global and local level
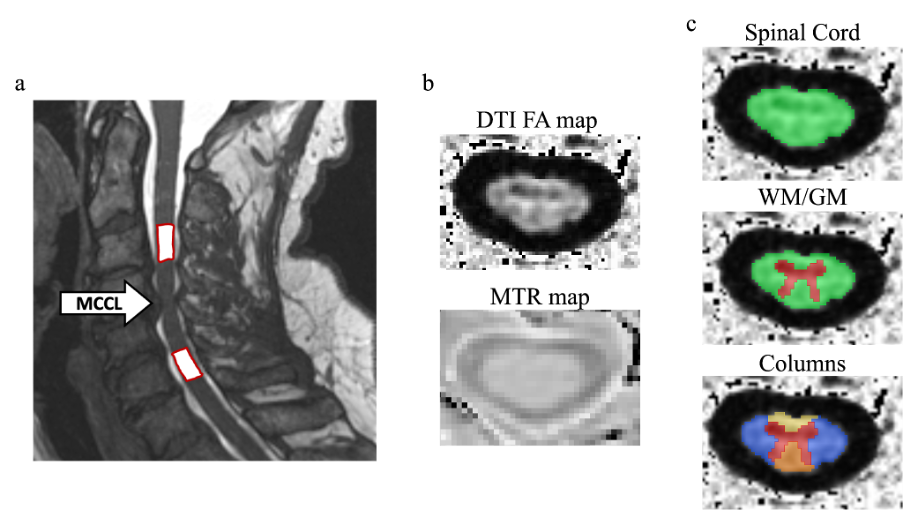
Figure 1. Representation of collected metrics above and below MCCL.
MCCL: maximally compressed cervical level, DTI: Diffusion Tensor Imaging, FA: Fractional Anisotropy, MTR: Magnetization Transfer Ratio, WM: White Matter, GM: Grey Matter
MCCL: maximally compressed cervical level, DTI: Diffusion Tensor Imaging, FA: Fractional Anisotropy, MTR: Magnetization Transfer Ratio, WM: White Matter, GM: Grey Matter
Results
- The best-performing models consistently contained the dataset with a combination of qMRI-derived and clinical metrics.
- MTR in the dorsal and ventral funiculi showed greater importance to model performance than DTI metrics.
- A vast majority of metrics were redundant, with ~32 of 171 being the most important unique metrics.
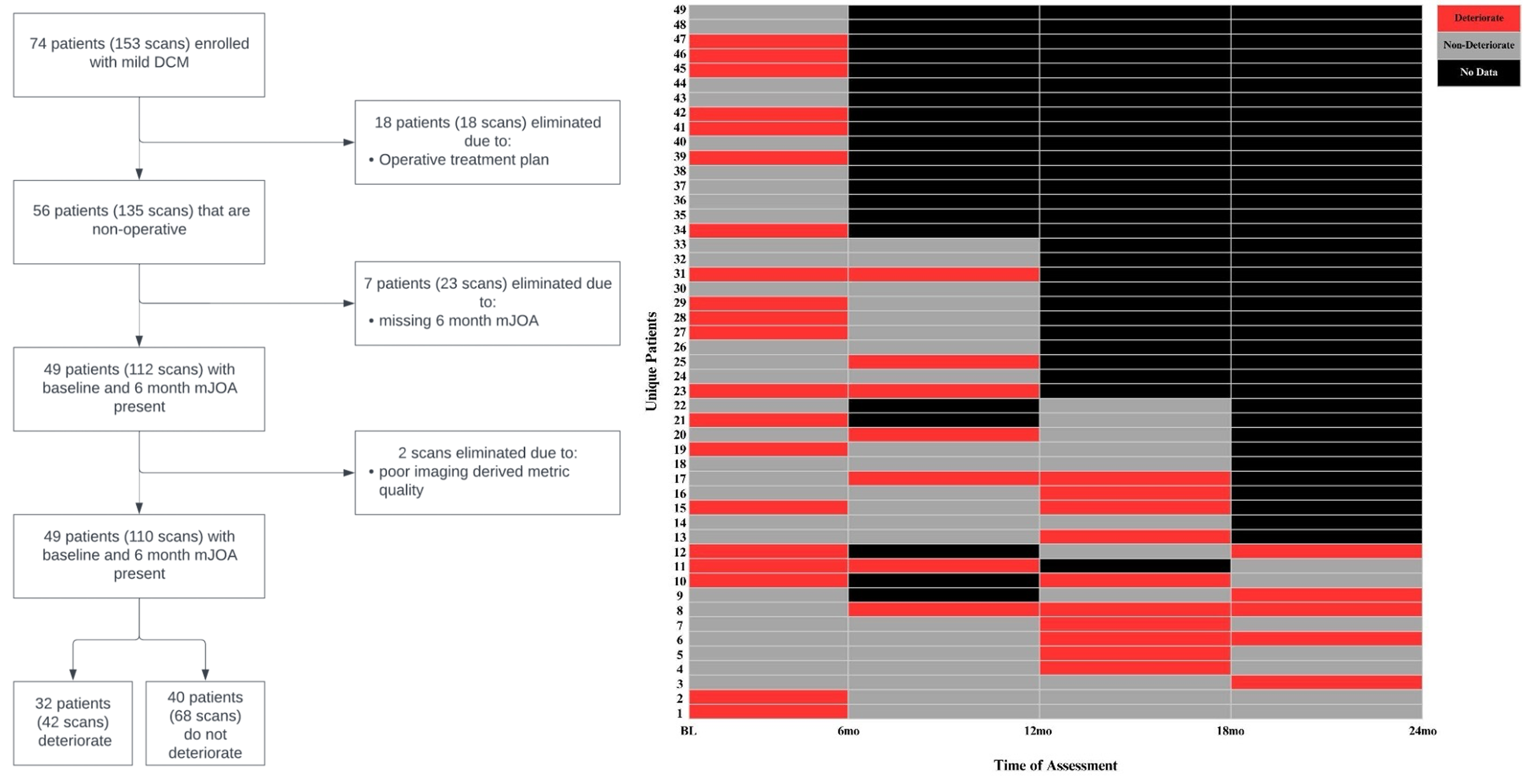
Figure 2. Patient Enrolment Overview (left) and Representation of the change in neurological condition of each unique enrolled patient (right)
Table 1. Tuned ML model testing set performance on differing dataset variations
| Dataset Variation | Model Type | Balanced Accuracy | F1 Score | Sensitivity | Specificity |
|
Imaging Metrics Only |
LR | 0.464 | 0.400 | 0.500 | 0.429 |
| RFC | 0.616 | 0.462 | 0.375 | 0.857 | |
| SVC | 0.643 | 0.533 | 0.500 | 0.786 | |
|
Clinical Metrics Only |
LR | 0.634 | 0.556 | 0.625 | 0.643 |
| RFC | 0.670 | 0.588 | 0.625 | 0.714 | |
| SVC | 0.732 | 0.667 | 0.750 | 0.714 | |
|
Combined Metrics |
LR | 0.795 | 0.737 | 0.875 | 0.714 |
| RFC | 0.821 | 0.762 | 1.000 | 0.643 | |
| SVC | 0.830 | 0.778 | 0.875 | 0.786 |
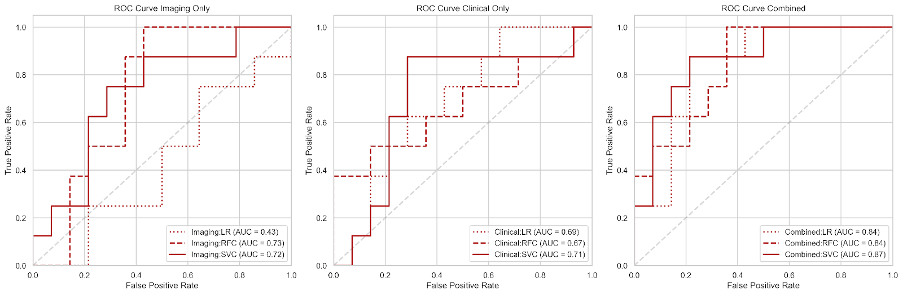
Figure 4. Receiver Operating Characteristic (ROC) curves for imaging-only, clinical-only, and combined feature datasets across varying model types.

Figure 5. The twenty most important features for model performance represented through SHAPely values.

Figure 6. Model prediction feature importance for individual cases of the most reliably predicted patients in each cohort.
Discussion and Impact
- Mild DCM patients would benefit from MT scans to assess the degree of demyelination, particularly rostral to the point of compression.
- Decreased MTR in the dorsal/ventral funiculi in combination with moderate tingling in the arm, should, or hand acts as an indicator for six-month neurological deterioration in mild DCM.
- Further validation of the proposed model on a multi-center, national dataset is needed.
References
1. Fehlings, M. G. et al. A global perspective on the outcomes of surgical decompression in patients with cervical spondylotic myelopathy: results from the prospective multicenter AOSpine international study on 479 patients. Spine 40, 1322–1328 (2015).
2. Nouri, A., Tetreault, L., Singh, A., Karadimas, S. K. & Fehlings, M. G. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine 40, E675-93 (2015).
3. Davies, B. M., Mowforth, O. D., Smith, E. K. & Kotter, M. R. Degenerative cervical myelopathy. BMJ 360, k186 (2018).
Contact: Abdul Al-Shawwa, abduljawwad.alshawwa@ucalgary.ca
Rate and Clinical Utility of Early Postoperative CT Head in Adult Craniotomy

BACKGROUND
Early postoperative CT (EPCT) head imaging
-
Computed tomography (CT) head scan within 24 hours of brain surgery (i.e., craniotomies)
- Used to detect surgical complications (e.g., bleeding, ischemia)
- For QI purposes (e.g., residual subdural hematoma or tumor)
-
Problems with EPCT
- Resource intensive
- Transfer risk to unstable patients (i.e., ICU patients, EVD dislodgement)
- Radiation exposure
-
EPCT in the literature
- Optimal timing of postop CT head – Scans performed 0-7h postop failed to predict CT changes that may develop over time or impact medical management (Khaldi et al., 2010)
- EPCT following elective craniotomy in neuro-preserved patients is not supported (Blumrich et al., 2021)
- Failure to extubate within 1h warrants EPCT due to increased risk of repeat surgery (Schär et al., 2016)
STUDY QUESTION & OBJECTIVE
Postoperative cranial neurosurgical imaging practices are highly variable
- Study Question: Does routine early postoperative computed tomography (EPCT) change management?
- Objective: To evaluate the rate and utility of EPCT, defined as a CT head scan within 24 hours of brain surgery, in consecutive adult craniotomies
METHODS
Review of postop CT head use
- Review of electronic medical records
- Adult neurosurgical patients admitted to the University of Alberta
-
Consecutive craniotomies performed >1 year ago
- Excluded surgeries: Non-craniotomies, mini craniotomies for biopsy, craniectomies, cranial burr holes for hematoma evacuation
-
Extracted data:
- Rate, timing, and utility (rate of unexpected/adverse findings) of EPCT
- Rate of surgical complications, neurologic deterioration, and the need for further surgical intervention
- Collected from progress notes, operative notes, and radiology reports
RESULTS
1. Breakdown of neurosurgical cases
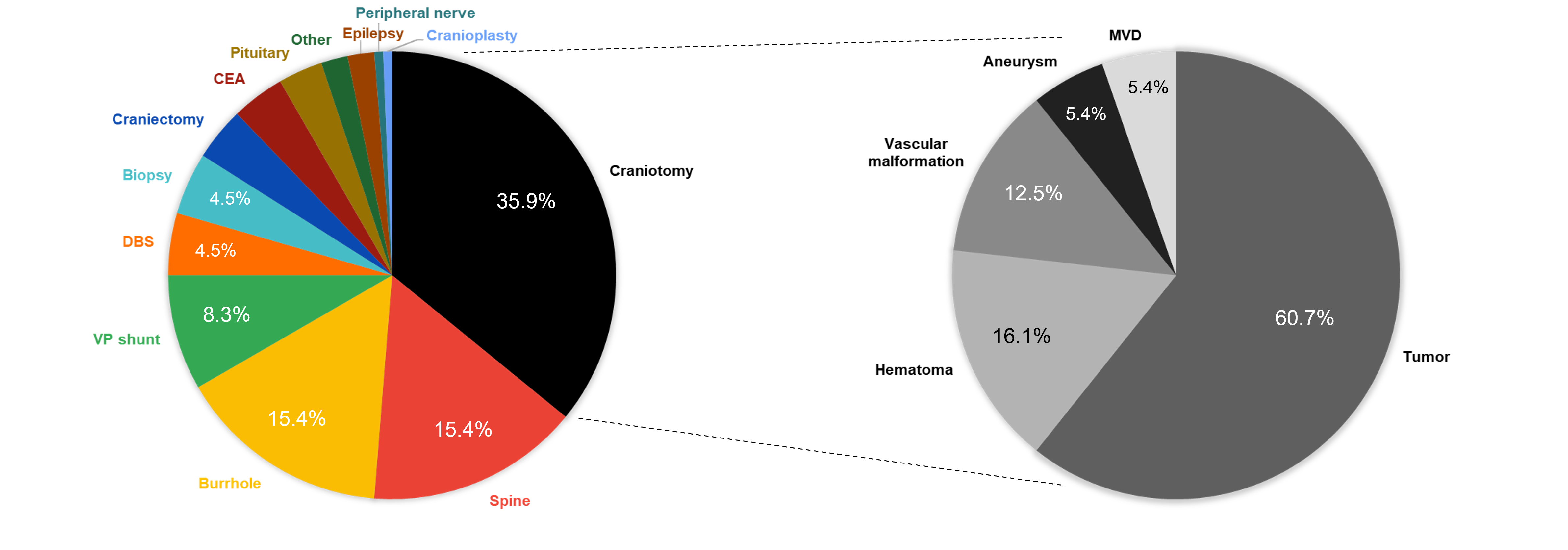
Figure 1. An overview of neurosurgical cases. 156 adult neurosurgical procedures were recorded over a 45-day period (17/09/2022 to 01/11/2022). Procedures were filtered using the keyword 'craniotomy', which resulted in a total of N=56 cases (35.9%) included in the study.
2. Early postop CT head is routine practice
-
Identified N=56 (35.9%) craniotomies of 156 neurosurgical procedures
- 27 female; avg age 55.5 ± 2.1 years, range 19-84 years
-
All patients underwent EPCT
- POD 0 = 10/56 (17.9%)
- POD 1 = 46/56 (82.1%)
3. Radiological and clinical changes are related

Figure 2. Contingency table of EPCT head vs. new neuro deficits. 8/56 (14.3%) patients had radiological changes on EPCT (e.g., bleeding, extensive pneumocephalus, edema, ischemia). 10/56 (17.8%) patients had neurologic deterioration on clinical exam (e.g., weakness, aphasia, visual impairment, seizure, decreased LOC). Radiological changes on EPCT correlate with new neuro deficits, p = 5.16e-06, X2 (1, N=56) = 20.8.
4. Repeat surgery is rare if adverse EPCT and no new neuro deficit
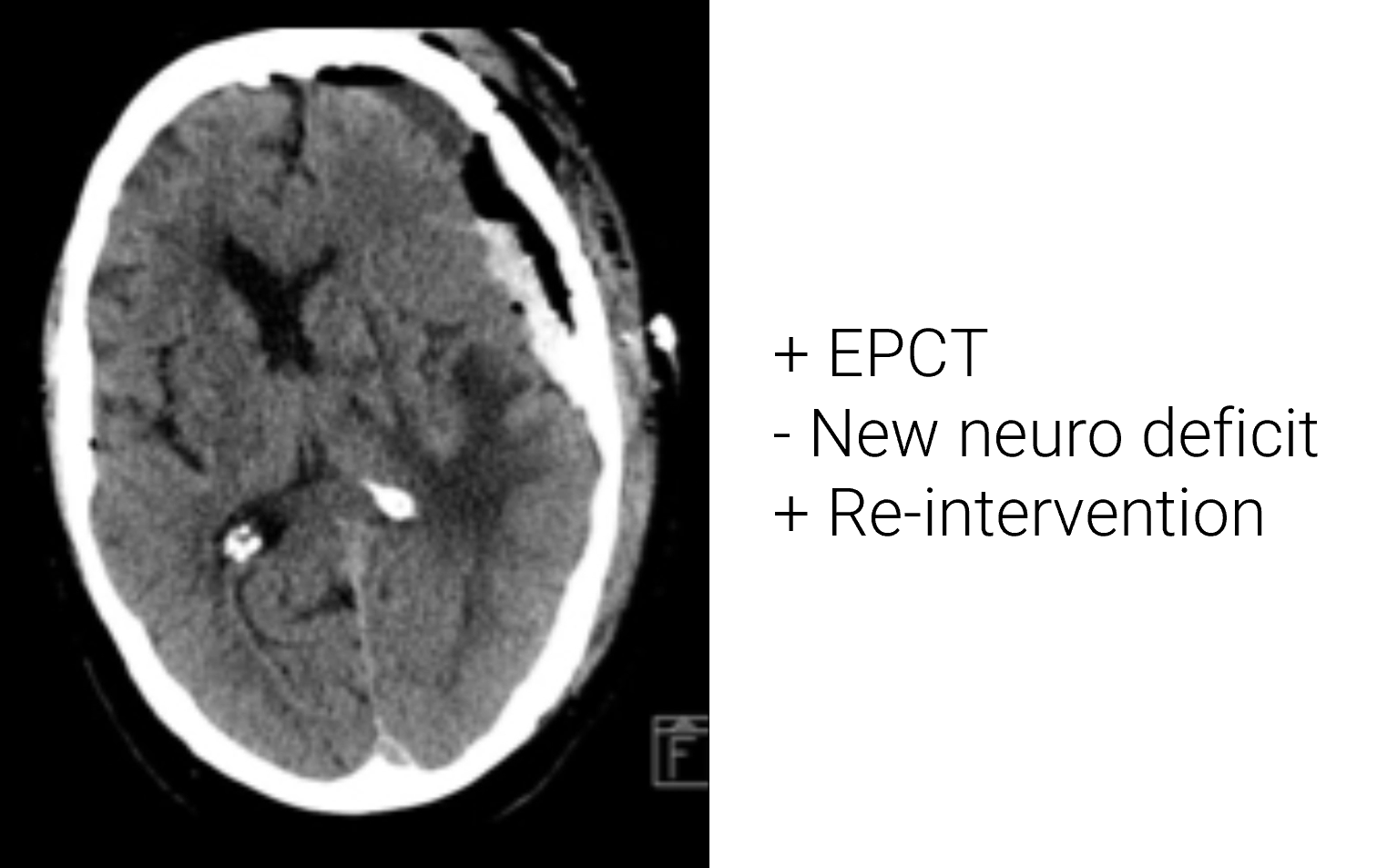
Figure 3. Axial CT head of a patient managed surgically with adverse EPCT but no new neuro deficit. 2/56 (3.6%) underwent repeat surgical intervention (e.g., subdural, epidural hematoma evacuation), of which 1/56 (1.8%) had an adverse EPCT but no new neuro deficit. 56 scans are needed to diagnose 1 clinically silent alteration requiring surgery.
STUDY LIMITATIONS
-
Small sample size
- An additional 444 craniotomies (N=500 total) will be evaluated
-
Single-centre study
- Surgeon-specific post-operative neuroimaging practices may skew results
-
One data extractor
- Unable to assess inter-rater reliability
- Retrospective (vs. prospective) design
CONCLUSIONS
May omit EPCT if neurologically intact
- Low rate of repeat surgery in the absence of neuro deficits despite abnormal EPCT
- Routine EPCT may not be justified in the absence of clinical deterioration
- Improve patient safety (i.e., minimize radiation exposure, limit transfer risk of unstable patients)
- Optimize resource allocation
- Decrease healthcare spending
Blumrich et al. Routine postoperative CT scan after craniotomy. Neurosurg Rev. 2021 Oct;44(5):2523-2531.
Khaldi et al. Clinical significance and optimal timing of postoperative CT. J Neurosurg. 2010 Nov;113(5):1021-5.
Schär et al. No routine postoperative head CT following elective craniotomy. PLoS One. 2016 Apr 14;11(4):e0153499.
Khaldi et al. Clinical significance and optimal timing of postoperative CT. J Neurosurg. 2010 Nov;113(5):1021-5.
Schär et al. No routine postoperative head CT following elective craniotomy. PLoS One. 2016 Apr 14;11(4):e0153499.
Distinct neuropsychiatric symptom trajectories in frontotemporal dementia across genetic mutations
INTRODUCTION
- Frontotemporal dementia (FTD) is a common cause of presenile dementia, which presents with heterogeneous combinations of behavioral, language and motor symptoms.[1] Approximately 40% of all FTD cases are familial, with ~10% of the total cases caused by autosomal dominant mutations in one of the microtubule associated protein tau (MAPT), chromosome 9 open reading frame 72 (C9orf72), or progranulin (GRN) genes.[1]
- Neuropsychiatric symptoms (NPS) often begin prior to the onset of FTD, and progress throughout the stages of FTD.
- Particularly, familial FTD due to autosomal dominant genetic mutations might display genetic variant-specific NPS profiles.
- We hypothesized distinct rates of change in NPS ratings scales among C9orf72, GRN, and MAPT mutation carriers during their transition from presymptomatic to symptomatic stages of FTD.
METHODS
- Participants were recruited through the ARTFL-LEFFTDS Longitudinal Frontotemporal Lobar Degeneration (ALLFTD) Study. All participants provided informed consents.
- The participants underwent genetic testing for mutations associated with FTD, including C9orf72, GRN, and MAPT. They also underwent annual neurologic examinations, cognitive, neuropsychological, and MRI assessments.
- Follow-up duration ranged from 2-5 years (two to five visits per participant).
- Conversion was defined as reaching the CDR-plus-NACC-FTLD global score 1, during follow-up.
- We included N=1662 participants, with 342 C9orf72, 148 GRN, 168 MAPT mutation carriers, and 1004 noncarriers.
PARTICIPANT STRATIFICATION
- We used the CDR plus NACC FTLD global scores to define the conversion status, and stratified participants into four stages of progression:
- Presymptomatic (CDR=0 throughout the follow-up; N=559),
- Early conversion (began with CDR=0, then increased to 0.5 during the follow-up; N=33),
- Advanced conversion (began with CDR=0.5, then increased to 1.0 or above; N=56),
- Symptomatic (CDR>1.0 throughout; N=1024).
NPS RATINGS SCALE
- We used the Neuropsychiatric Inventory Questionnaire (NPI-Q) to assess the changes in NPS.[2]
-
We analyzed the NPI-Q total scores and the following NPI-Q subsyndromes, adapted from Aalten et al., Dem Geriatr Cogn Disord 2007 [3]:
- Hyperactivity (Agitation, Disinhibition, Irritability, Aberrant Motor Behavior)
- Affective (Anxiety, Depression)
- Psychosis (Delusions, Hallucinations, Nighttime Behavior)
- Apathy (Apathy, Appetite)
ANALYSIS
- We used generalized linear mixed models to compare the rates of NPI-Q score changes among C9orf72, GRN, MAPT mutation carriers, and noncarriers.
- The models were adjusted for age, sex, education, and baseline NPI-Q scores. Years from baseline was used as the time variable.
RESULTS
Predicted NPI-Q Total Scores
Thick lines indicate group average; Shades indicate 95% CI
Thick lines indicate group average; Shades indicate 95% CI

- NPI-Q trajectories were similar among carriers and noncarriers during presymptomatic stages.
- However, in the early conversion stage, C9orf72 (p=0.04) and GRN (p=0.004) carriers exhibited significantly higher NPI-Q score increases compared to MAPT carriers. During this stage, potential differences were observed in the hyperactivity and psychosis domains.
- In the advanced and symptomatic stages, the rates of NPI-Q changes were similar across the groups.
CONCLUSIONS
- This study suggests that people with familial FTD, particularly those predicted to have underlying TDP-43 pathology, may experience faster progression of neuropsychiatric symptoms like psychosis or hyperactivity as they progress from presymptomatic to prodromal phases. The rates of NPI-Q increase during this stage appear faster than those with tau pathology or sporadic FTD.
- Further studies are warranted to understand these unique progression patterns and their implications for FTD management.
REFERENCES
[1] Bang et al., Lancet 2015, PMID: 26595641
[2] Cummings et al., Neurology 1994, PMID: 7991117
[3] Aalten et al., Dement Geriatr Cogn Disord 2007, PMID: 17986816
[2] Cummings et al., Neurology 1994, PMID: 7991117
[3] Aalten et al., Dement Geriatr Cogn Disord 2007, PMID: 17986816
Review of imaging changes, cognitive decline, and dementia risk in cancer survivors after chemotherapy
BACKGROUND
- Improvements in cancer survival rates have led to a growing number of cancer survivors within or entering the age range at risk of dementia development.1,2
- A significant number of cancer patients experience issues with cognitive functions after treatment, known as cancer-related cognitive impairment (CRCI).3
- CRCI may be associated with structural and functional changes in the brain.
- Additionally, CRCI may alter the trajectory of normal aging, and may impact the future risk of developing dementia.
OBJECTIVES
- To summarize the current knowledge on changes in brain imaging, cognitive performance, and the association between cancer survivorship and dementia risk in adult non-CNS cancer survivors who received chemotherapy.
METHODS
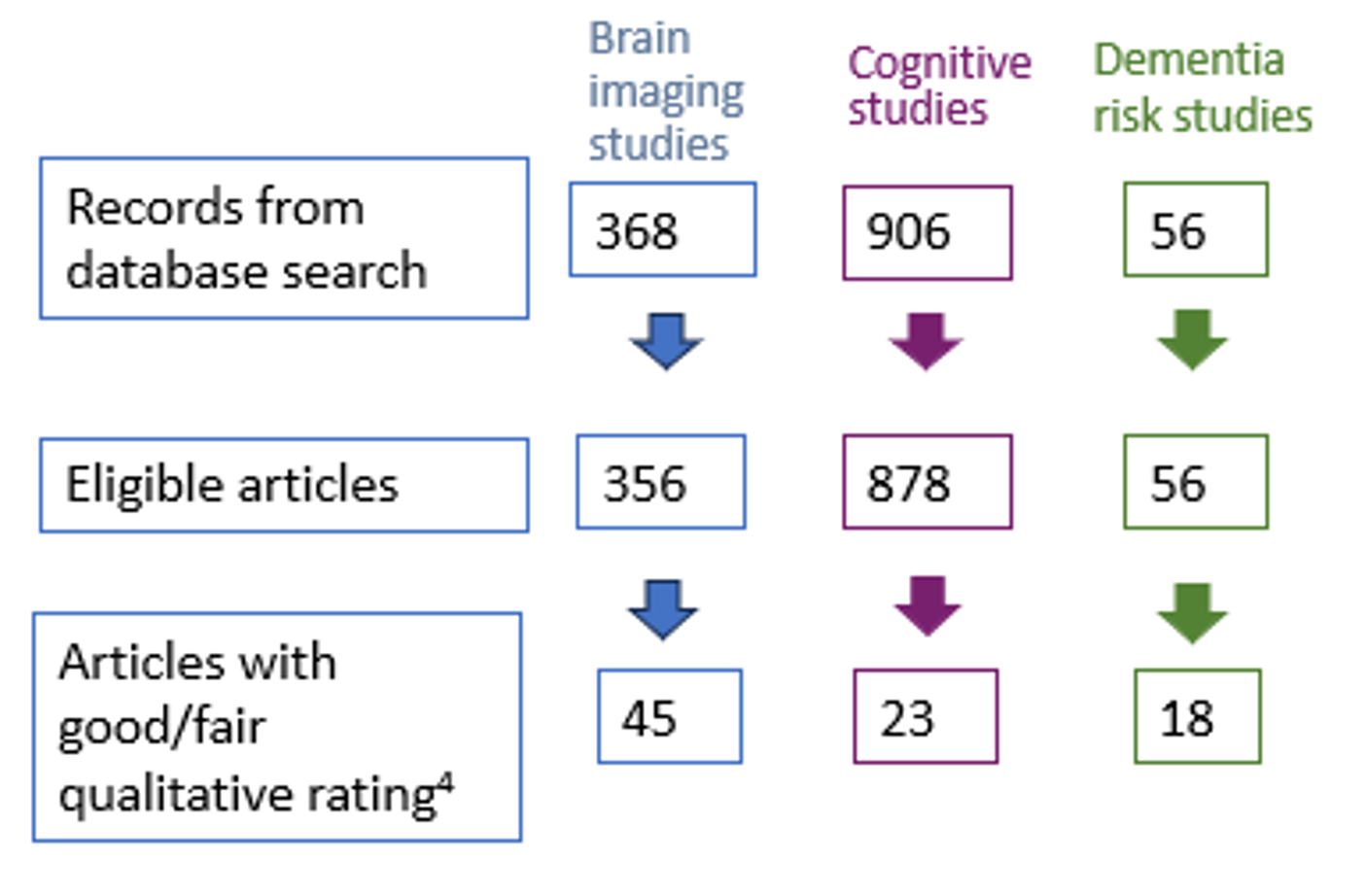
- We conducted a PRISMA-guided search on PubMed for primary studies between 2010 and 2023.
- The quality of the eligible studies was evaluated using the National Heart, Lung, and Blood Institute Study Quality Assessment Tools.4
RESULTS
Studies of brain imaging changes (45 total)
| Frontal | Temporal | Parietal | Occipital | Cerebellar | Others | |
|---|---|---|---|---|---|---|
| Voxel-based Studies (Primarily GM) (N=15) |
8/15 | 4/15 | 6/15 | 5/15 | 5/15 | 5/15 (e.g. Thalamus, Caudate) |
| Diffusion-based Studies (WM) (N=16) |
4/16 | 3/16 | 1/16 | 1/16 | - | 14/16 (WM blundles e.g. Corpus Callosum, Corona Radiata) |
| fMRI Studies (N=13) |
7/13 | 7/13 | 6/13 | 1/13 | - | 6/13 (e.g. Cingulate, Caudate) |
| CMB Studies (N=2) | - | - | - | - | - | 1/2 (Infratentorial) |
| Hippocampal Shape/Volume Analyses (N=3) | - | 3/3 | - | - | - | - |
| Brain Volume & Cortical Thickness Studies (N=3) | - | 1/3 | - | - | - | 2/3 |
Studies of cognitive performance changes (23 total)
| Number of studies reporting significant decline | |
| Visuomotor | 2/9 (22%) |
| Attention | 7/17 (41%) |
| Working Memory | 3/7 (43%) |
| Verbal Memory | 2/10 (20%) |
| Non-Verbal Memory | 2/7 (29%) |
| General Memory | 3/7 (43%) |
| Executive Function | 3/13 (23%) |
| Processing Speed | 2/10 (20%) |
| Language Skills | 4/7 (57%) |
| Global Cognition | 4/10 (40%) |
RESULTS
Studies of future dementia risk among survivors (18 total)
| Studies with patients <5 year since cancer dx (on average) |
Studies with patients >=5 year since cancer dx (on average) |
Studies with varied time since cancer dx (i.e. included incidental cases) | |
| Found lower risk of dementia | 4 | 4 | 5 |
| Found higher risk of dementia | - | 4 | - |
| Found no association | - | 2 | 1 |
DISCUSSION
Imaging Studies
- We observed global changes in gray matter, white matter, and functional networks, with particularly pronounced changes in the frontal, temporal, and parietal regions.
- Cognitive decline was most consistently reported in attention, language skills, and memory, although heterogeneity was greater than that observed among imaging findings.
- ~70% of the studies reported a lower risk of dementia in cancer survivors.
CONCLUSION
- Significant imaging changes were noted in the studies, particularly in the regions commonly affected in types of dementia such as Alzheimer’s or Frontotemporal dementia.
- Since most studies only had up to 1 or 2 years of follow-up, the evidence is limited for drawing a robust conclusion regarding whether CRCI is reversible or irreversible.
- The 'protective' effect of cancer on dementia should be interpreted with caution, particularly considering whether the follow-up timeframe was sufficient to include long-term (>5 years) survivors.
- Future studies should explore the link between CRCI and dementia risk, examining the influence of cancer type and treatment, genetic predisposition, and lifestyle factors.
Outcome of psychogenic nonepileptic seizures following diagnosis in the epilepsy monitoring unit

Objective:
To study the outcome of patients with psychogenic non-epileptic seizures (PNES) after their diagnosis in the epilepsy monitoring unit (EMU).
Methods:
Patients diagnosed in our EMU with definite PNES between January 2009 and May 2023 were contacted by phone, and those who agreed to participate were asked a set of predetermined questions.
Comparative analyses were carried out on several variables before and after diagnosis:
To study the outcome of patients with psychogenic non-epileptic seizures (PNES) after their diagnosis in the epilepsy monitoring unit (EMU).
Methods:
Patients diagnosed in our EMU with definite PNES between January 2009 and May 2023 were contacted by phone, and those who agreed to participate were asked a set of predetermined questions.
Comparative analyses were carried out on several variables before and after diagnosis:
- number of participants with daily PNES
- number of visits to the emergency department
- number of participants who consulted their general practitioner or a neurologist outside of a scheduled follow-up
- number of participants who took antiseizure medications (ASMs) or psychotropic drugs
- employment status
Burden of PNES on participants before and after diagnosis.
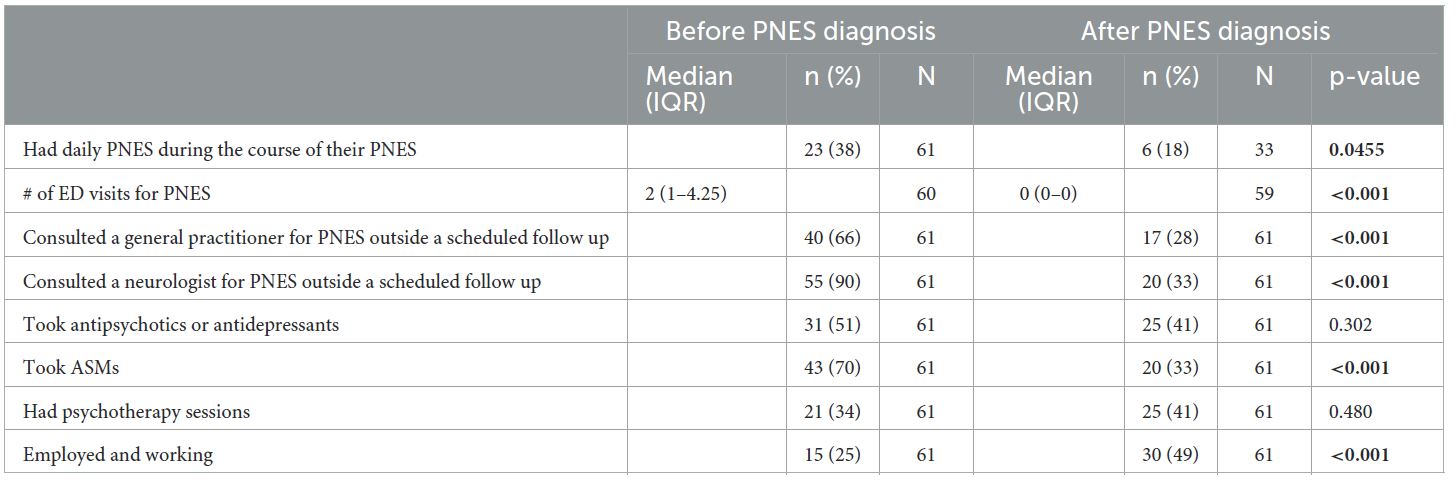
Continuous variables were compared using paired Mann-Whitney U-tests, and binary variables were compared using McNemar’s tests.
The significance level was set at 0.05. Statistically significant results are shown in bold.
The significance level was set at 0.05. Statistically significant results are shown in bold.
Prognostic outcomes in participants who still had PNES at data collection.
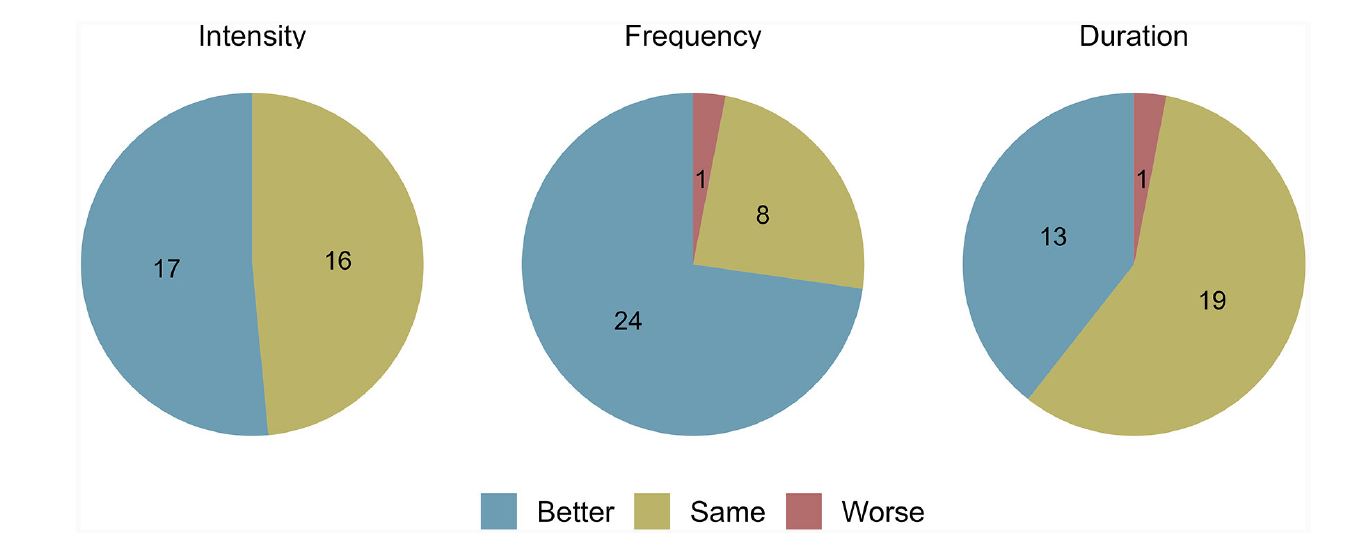
The intensity, frequency, and duration of PNES in the 33 participants who still had PNES episodes are depicted here.
Results in bullets:
Conclusion:
Our study revealed a relatively favorable long-term outcome of definite PNES diagnosed in the EMU that translated in significant reductions in PNES frequency, health care utilization and ASM use, as well as a significant increase in employment rate.
- 103 patients with a definite diagnosis of PNES.
- 61 patients accepted to participate in our study.
- 79% female.
- 35 yo Median age at PNES onset.
- 3 years Median delay to diagnosis.
- 62% receiving ASMs and 40% psychotropic drugs.
- 5 days mean stay at the EMU.
- 89% accepted PNES diagnosis.
- 46% no longer had PNES.
- 32% immediately upon communication of the diagnosis.
- 51 months median follow-up duration.
- 18 (vs. 38%) patients had daily seizures after the diagnosis.
- Significantly lower ER, GP and neurologists visits.
- 33% (vs 70%) still took ASM, with only one for its antiseizure property.
- 49% (vs 25%) had work.
Conclusion:
Our study revealed a relatively favorable long-term outcome of definite PNES diagnosed in the EMU that translated in significant reductions in PNES frequency, health care utilization and ASM use, as well as a significant increase in employment rate.
Real-world effectiveness of intravenous eptinezumab in patients with chronic migraine and previous subcutaneous preventive migraine treatment
Introduction
- Eptinezumab (Vyepti) is a humanized mAb that specifically targets the CGRP ligand and is indicated for prevention of migraine in adults.1
- Eptinezumab is administered intravenously (IV),2 while other anti-CGRP monoclonal antibodies (fremanezumab/Ajovy,3 galcanezumab/Emgality,4 and erenumab/Aimovig5) are administered subcutaneously.
-
Minimal evidence exists evaluating the real-world effectiveness of switching from a subcutaneous anti-CGRP mAb to an intravenous anti-CGRP mAb.
Methods
- REVIEW was an observational, multi-site (4 tertiary headache centers), US-based study that evaluated real- world experiences of patients being treated with eptinezumab for chronic migraine (CM) in the outpatient setting as well as the experiences of 4 treating principal investigators.
-
Study sites were instructed to select and recruit patients based on the key inclusion/exclusion criteria outlined below:
- Eligible patients were ≥18 years of age, had a diagnosis of CM (per the patient chart), and had completed ≥2 consecutive eptinezumab infusion cycles (i.e., 6 months’ exposure).
-
Patients were excluded if they were enrolled in a clinical trial or had been treated with eptinezumab in a clinical trial setting (no time limit).
Results
- Ninety-four patients enrolled (Figure 1).
- Regardless of prior exposure to a CGRP ligand blocker (galcanezumab and fremanezumab) or receptor blocker (erenumab), the number of “good” days per month more than doubled following eptinezumab treatment (Figure 3).
- Regardless of the number of prior subcutaneous anti-CGRP mAbs used, the number of “good” days/month at least doubled following eptinezumab treatment. (Figure 4).
Figure 1: Baseline demographics



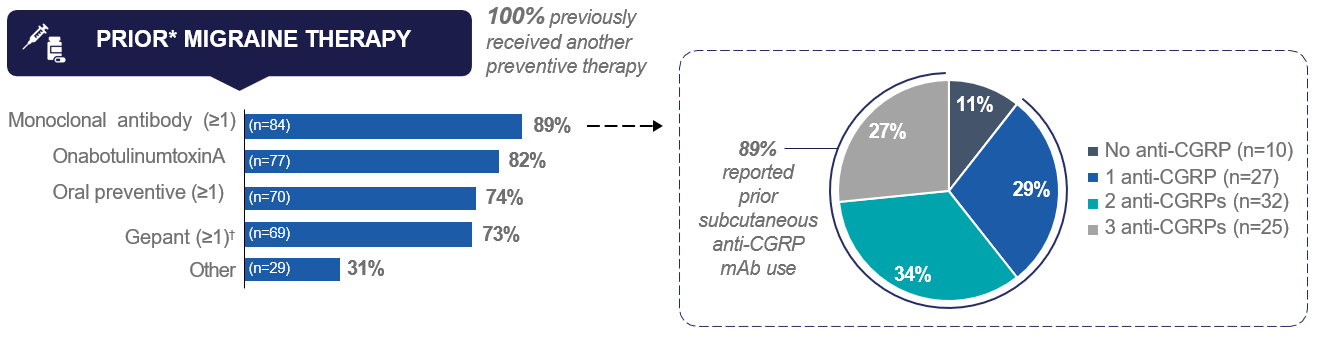
N=94. Results were self-reported by the patients. GI, gastrointestinal (“digestive system”; e.g., Crohn’s disease, ulcers, or irritable bowel syndrome). *May have been used concomitantly after eptinezumab initiation. Includes atogepant, ubrogepant, and rimegepant; therefore, captures both acute and preventive use.
Figure 2. Average number of “good” days per month before and after eptinezumab treatment in the total sample
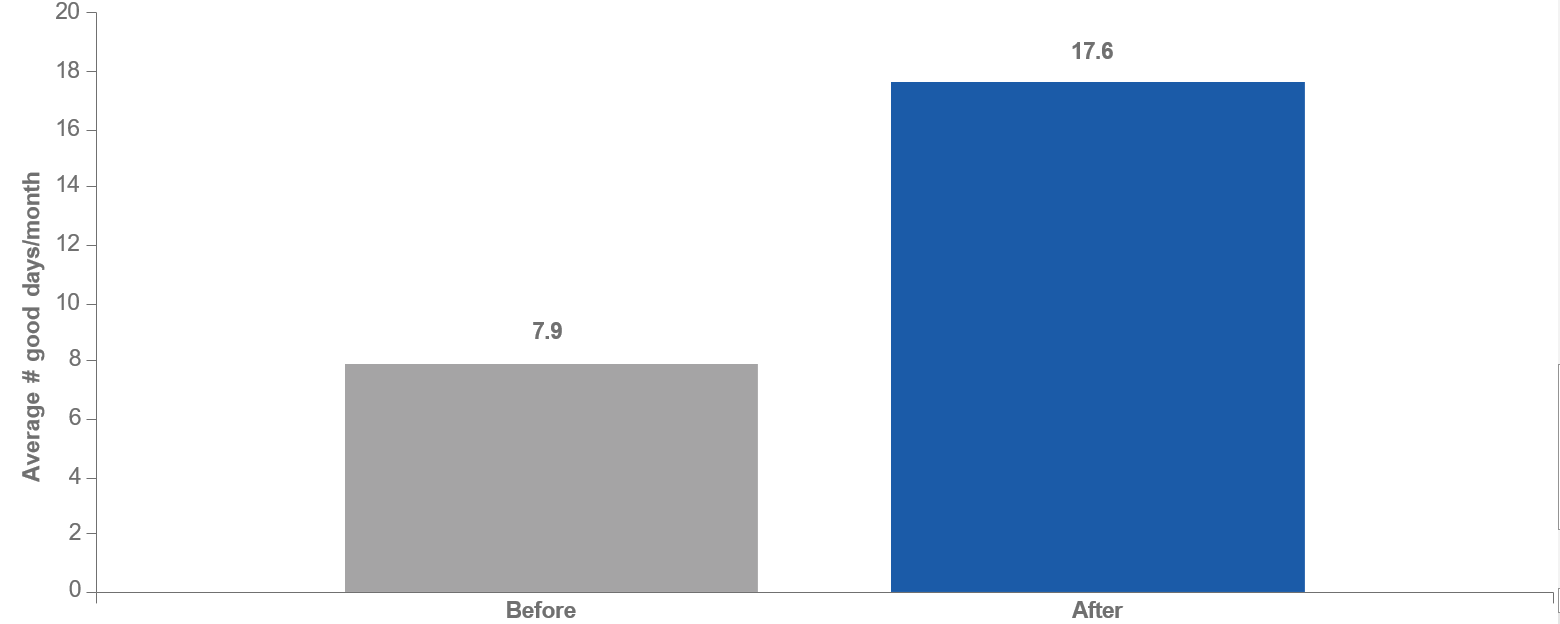
N=93. Patients were prompted: “On average, how many good days per month did you experience before/after starting on Vyepti? Please indicate the number of days, 1–31.”
Figure 3. Average number of “good” days per month by type of prior subcutaneous anti-CGRP mAb use before and after eptinezumab treatment
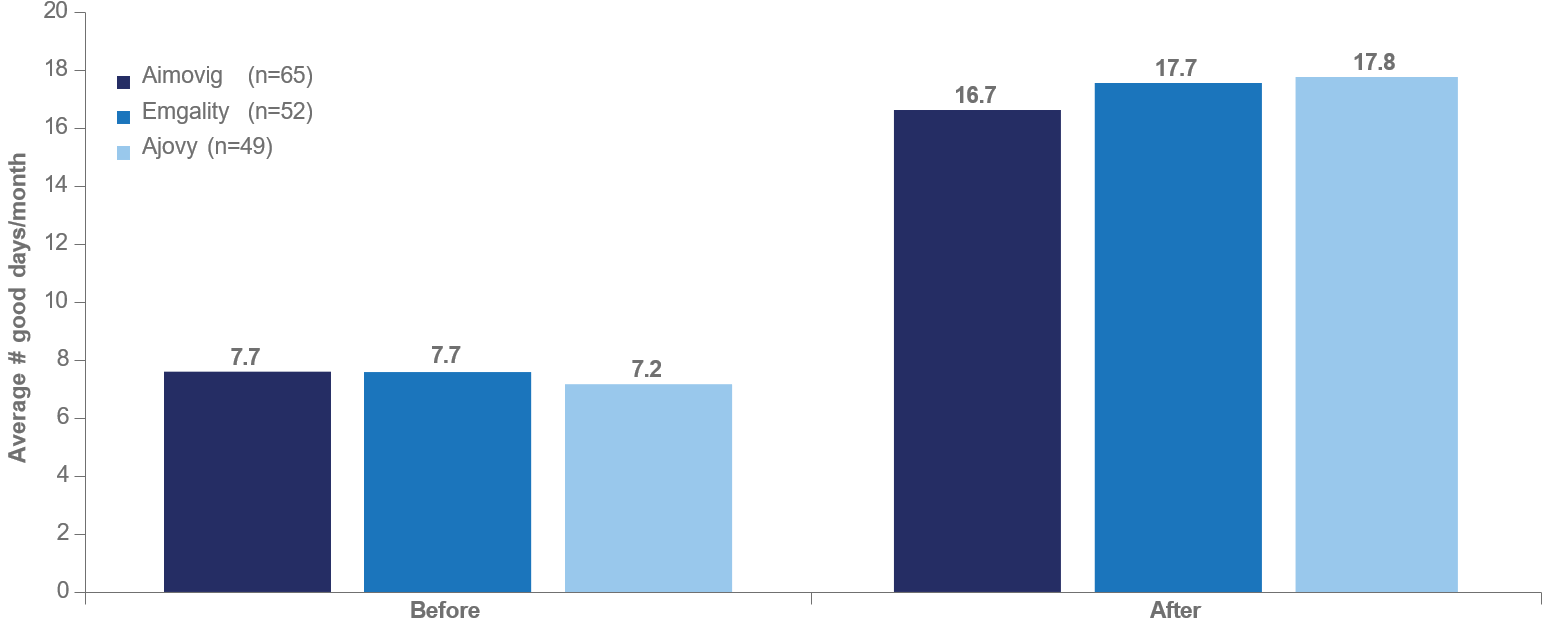

Patient Prompt: “On average, how many good days per month did you experience before/after starting on Vyepti? Please indicate the number of days, 1-31.” Subgroups are not mutually exclusive; patients could be included in more than one sub-analysis.
Figure 4. Average number of “good” days per month by number of prior subcutaneous anti-CGRP mAbs used before and after eptinezumab
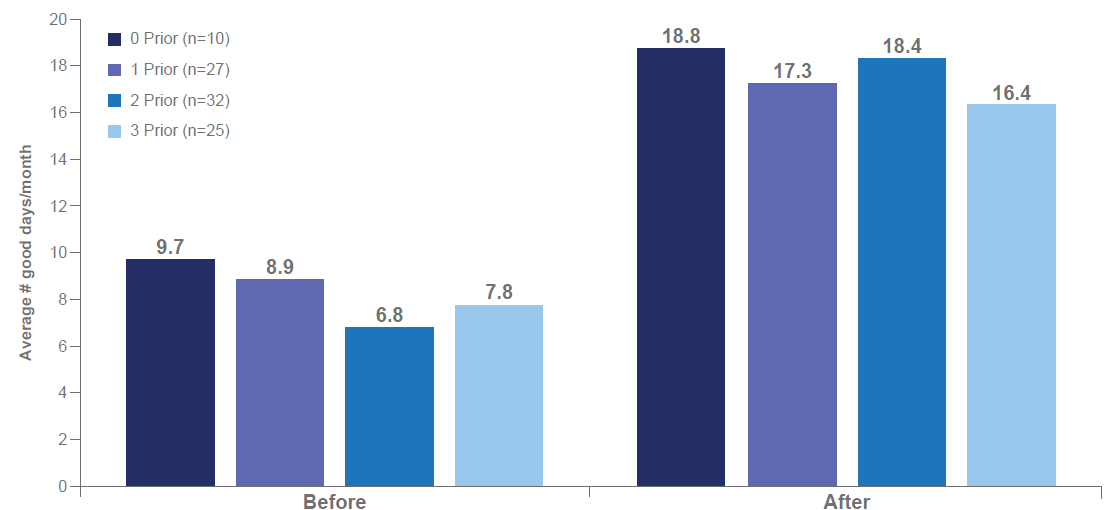

N = 94. Patient Prompt: “On average, how many good days per month did you experience before/after starting on Vyepti? Please indicate the number of days, 1-31.”
Key points
- REVIEW was an observational, multi-site, US-based study that evaluated real-world experiences of patients being treated with eptinezumab for CM.
- The robust response, where the average number of patient-reported “good” days per month at least doubled, was irrespective of the mechanism of CGRP blockade of the previously used subcutaneous anti-CGRP mAb(s). This indicates that the switch from ligand or receptor-targeted therapy did not impact the effectiveness of eptinezumab.
- The effectiveness of eptinezumab in improving “good” days did not differ regardless of the number of previous treatments with subcutaneous anti-CGRP mAbs, suggesting that a positive response can be attained upon transitioning to IV eptinezumab without the need for multiple trials of subcutaneous anti- CGRP mAbs, thereby reducing the time to effectiveness and minimizing exposure to multiple agents in this class.
Conclusions
This real-world, patient survey showed that patients with prior exposure to subcutaneous anti-CGRP mAbs had high overall improvement in “good” days with eptinezumab treatment regardless of the number and type of previous anti-CGRP therapies used.
Eptinezumab demonstrated efficacy regardless of prior preventive migraine treatment failure: post hoc DELIVER analyses
Introduction
- Eptinezumab is an anti–calcitonin gene-related peptide monoclonal antibody (anti-CGRP mAb) indicated for the preventive treatment of migraine,1 with its efficacy and safety in adults demonstrated in multiple large-scale clinical trials.2–5
- In the DELIVER study, eptinezumab treatment resulted in statistically significant reductions in MMDs compared with placebo in patients with migraine and 2–4 prior preventive treatment failures.5
- Failure of multiple therapies is often required before receiving anti-CGRP mAb treatment; however, guidelines for how many and which therapies must fail vary by country and payor.6–9
Objective
To evaluate the efficacy of eptinezumab versus placebo across 24 weeks of treatment in the DELIVER study in subgroups defined by type of prior treatment failure
Methods
- DELIVER (NCT04418765) was a phase 3b, multicenter, parallel-group, double-blind study that randomized patients to eptinezumab 100 mg, 300 mg, or placebo via intravenous infusion every 12 weeks.5
- Eligible patients (aged 18–75 years) with episodic or chronic migraine needed documented evidence of 2–4 prior preventive treatment failures within the past 10 years.
- Patients may have had prior failures across multiple types of treatment; therefore, subgroups are not mutually exclusive.
Results
- The full analysis set included 890 patients.
Figure 1. Demographic characteristics, by prior preventive treatment failure type
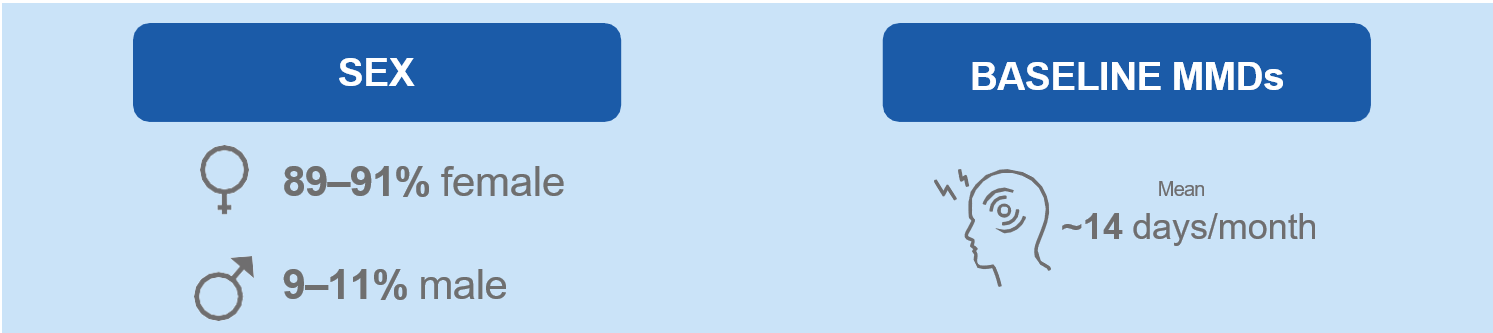

Two patients had fewer than 2 previous preventive treatment failures and represent protocol deviations: one patient receiving eptinezumab 300 mg had 1 previous failure, and one patient receiving placebo had 1 previous failure. MMDs, monthly migraine days.
Figure 2. Change from baseline in monthly migraine days over 12-week intervals, by prior preventive treatment failure type
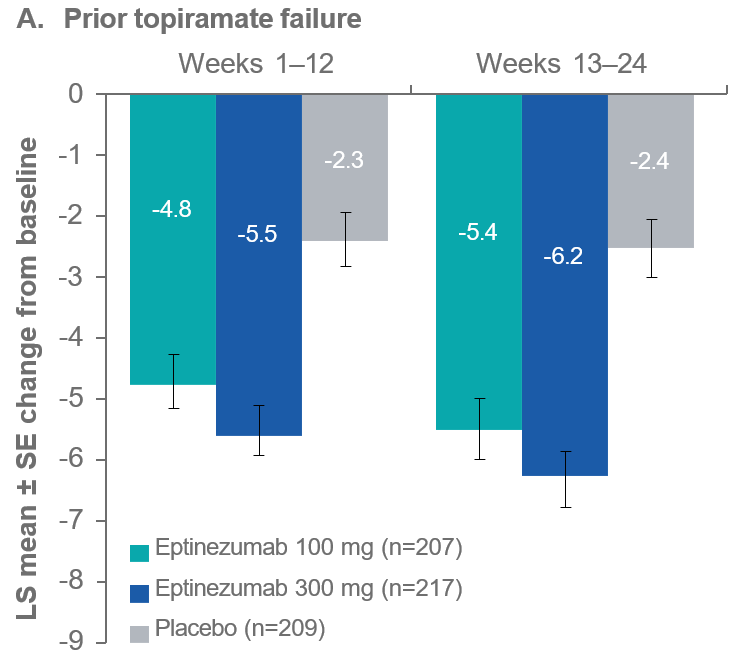

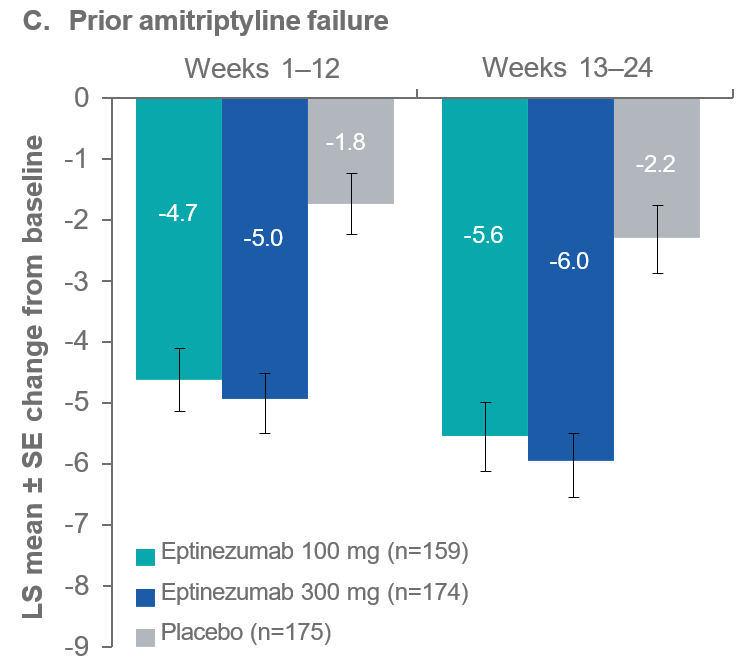
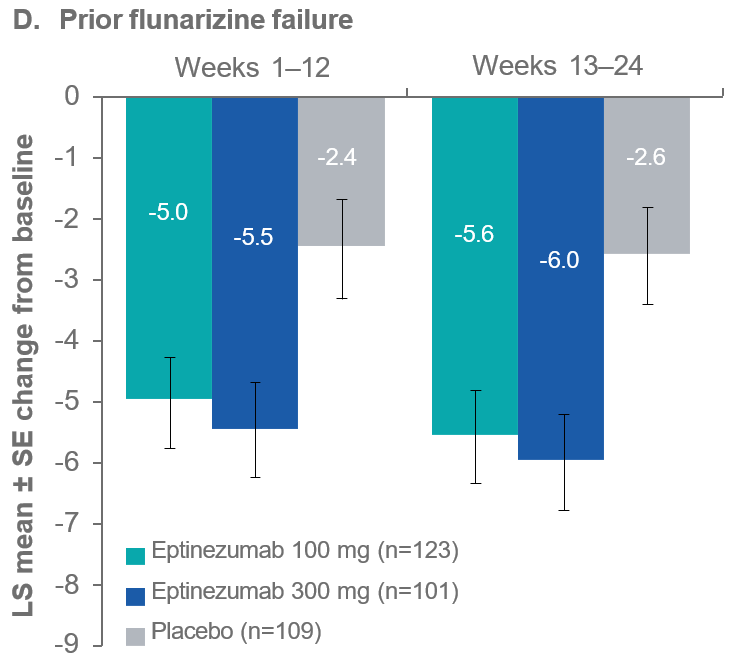
LS, least squares; SE, standard error.
Figure 3. ≥50% migraine responder rates over 12-week intervals, by prior preventive treatment failure type
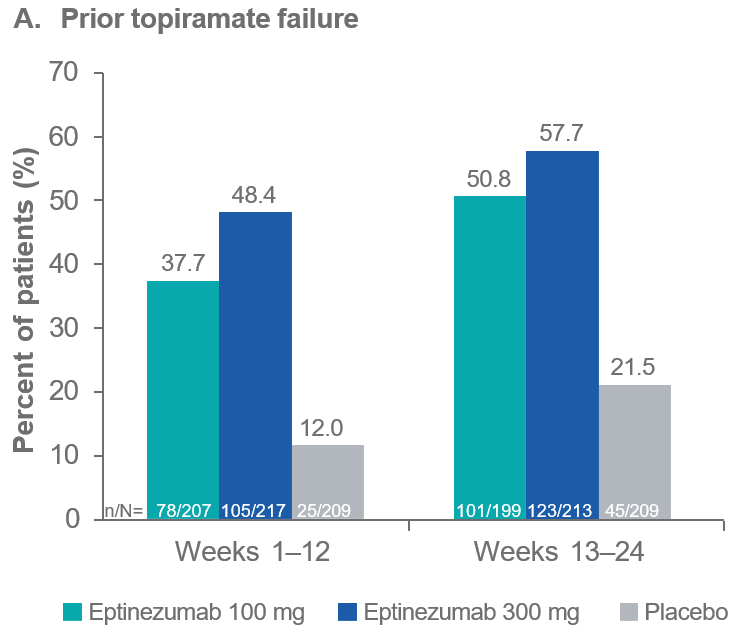

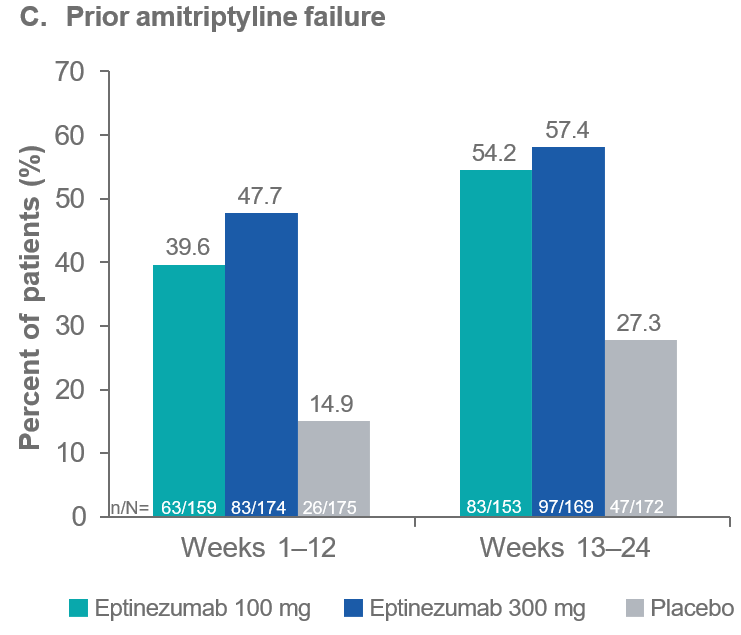
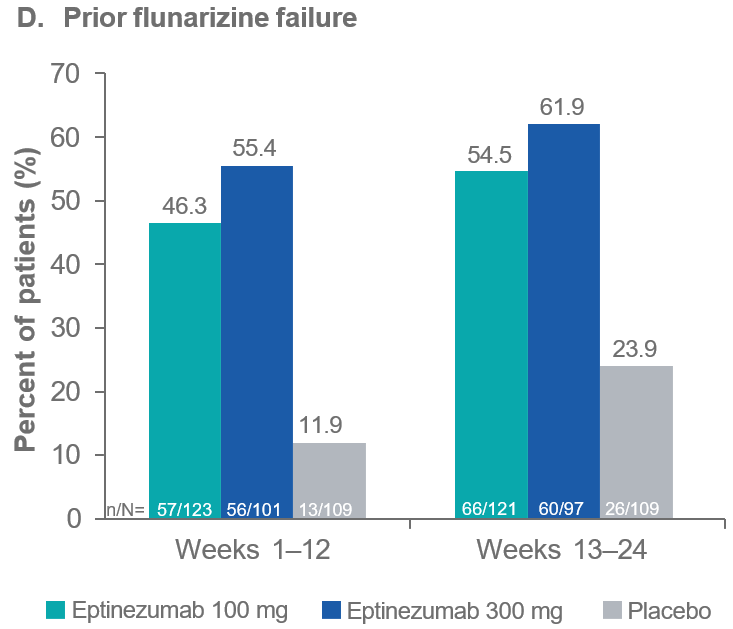
The ≥50% response threshold is calculated as the average percentage change in monthly migraine days.
Key points
- Among patients with previous preventive migraine treatment failures, eptinezumab demonstrated greater reductions in monthly migraine days (MMDs) compared with placebo across all subgroups of traditional preventive treatment types.
-
These results suggest that a second dose of eptinezumab may provide additional benefit.
Conclusions
- In all subgroups, regardless of prior preventive treatment failure type, eptinezumab demonstrated greater reductions in MMDs and larger migraine responder rates (MRRs) compared with placebo.
- Given the differences in preventive migraine treatment guidelines, it is important that the efficacy of eptinezumab does not appear to be impacted by the type of prior preventive medication that led to treatment failure.
Barriers and risk factors for emergency room visits vs smartphone app use for migraine in Canada and the United States
Background
Migraine affects more than 1 billion people worldwide [1]. Knowledge of environmental triggers for migraine attacks is limited, and has mostly been studied via emergency room (ER) visits [2]. Barriers to attending ER limit measurement to the most severe cases and introduce time lags [3]. Time lags create challenges for assessing causal links to environmental exposures.
Objective
To assess the utility of using emergency department data for understanding the relationship between air pollution and migraine.
Methods
Non-probablily online survey of ER use for migraine in Canada and the USA. Analyzed in R [2].
Table 1: Demographic and migraine diagnosis information from eligible participants
|
Variable
|
N = 3711
|
|
Age
|
43 (13, 77)
|
|
Country
|
|
|
Canada
|
159 (43%)
|
|
USA
|
212 (57%)
|
|
Ever diagnosed by a doctor
|
366 (99%)
|
|
Doctor who diagnosed migraine
|
|
|
ER doctor
|
2 (0.5%)
|
|
Family doctor, general practitioner (GP), or Primary Care Physician (PCP)
|
107 (29%)
|
|
Headache specialist
|
44 (12%)
|
|
Neurologist
|
210 (57%)
|
|
Not diagnosed
|
5 (1.3%)
|
|
Other - All of the above, Ophthalmologist, Psychiatrist
|
3 (0.8%)
|
|
Went to ER for migraine in the past 12 months
|
167 (45%)
|
|
1Mean (Range); n (%)
|
|
Results
There were 371 female respondents who were diagnosed and/or met ICHD-3 criteria. Migraine symptoms were similar in both countries. Canadians more likely to lack alternative access to urgent care and to avoid discomforts at the ER and COVID-19 exposure. Americans were more likely to avoid visiting ER due to financial concerns. The attack was recorded by 46 % of those who went to or considered ER. Time between migraine onset and reporting was up to 38 days for ER visits, and 0-2 days in a Migraine Buddy dataset.
Table 2: Participant’s responses to the question: “Why did you go to or think about going to the Emergency Room?”
|
Reason for attending ER
|
Canada, N = 1411
|
USA, N = 1631
|
|
Sent by a medical professional
|
17 (12%)
|
30 (18%)
|
|
Unbearable pain
|
103 (73%)
|
123 (75%)
|
|
Worried about symptoms other than pain
|
42 (30%)
|
52 (32%)
|
|
Vomiting too much or feeling too sick to eat or drink
|
33 (23%)
|
54 (33%)
|
|
Attack felt like something other than a migraine
|
32 (23%)
|
46 (28%)
|
|
No other place to see a doctor quickly enough
|
18 (13%)
|
11 (6.7%)
|
|
Other - Needed medicines available at ER
|
6 (4.3%)
|
5 (3.1%)
|
|
Other - Attack was too long
|
8 (5.7%)
|
6 (3.7%)
|
|
1n (%)
|
||

Table 3: Participants’ responses to the question “Why didn’t you go to the Emergency Room when you had a migraine attack?”
|
Reason for not attending ER
|
Canada, N = 621
|
USA, N = 751
|
|
Did not need to go to emergency room
|
13 (21%)
|
27 (36%)
|
|
Avoid long wait time, bright lights, noises and other discomforts
|
50 (81%)
|
51 (68%)
|
|
Got medical help somewhere else
|
7 (11%)
|
7 (9.3%)
|
|
Attack ended or got better
|
13 (21%)
|
26 (35%)
|
|
Too hard to get to ER
|
6 (9.7%)
|
14 (19%)
|
|
Too expensive
|
0 (0%)
|
30 (40%)
|
|
Avoid exposure to COVID-19 or other infectious illnesses
|
19 (31%)
|
11 (15%)
|
|
Other - Fear of or previous experience of ineffective medical treatment
|
2 (3.2%)
|
5 (6.7%)
|
|
Other - Fear of or previous experience of unkind treatment from staff at ER
|
1 (1.6%)
|
4 (5.3%)
|
|
1n (%)
|
||
Conclusions
Not all severe migraine attacks are recorded by smartphone users. However, smartphone app records may have fewer barriers to creation and shorter time lags compared to ER records. Smartphone app records may be a rich source of data for research on transient neurologic health outcomes such as migraine and environmental exposures. Upcoming work will measure the association between ambient air pollution and smartphone app records for migraine.
References
1. James SL, Abate D, Hassen Abate K, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018; 392(November): 1789-1858.
2. Portt AE, Orchard C, Chen H, Ge E, Lay C, Smith PM. Migraine and air pollution: A systematic review. Headache. 2023; 63(9): 1203-1219.
3. Minen MT, Loder E, Friedman B. Factors associated with emergency department visits for migraine: An observational study. Headache. 2014; 54(10): 1611-1618.
4. R Core team. R: a language and environment for statistical computing. Version 2024.04.0+735. https://www.r-project.org
Email: andrea.portt@mail.utoronto.ca
2. Portt AE, Orchard C, Chen H, Ge E, Lay C, Smith PM. Migraine and air pollution: A systematic review. Headache. 2023; 63(9): 1203-1219.
3. Minen MT, Loder E, Friedman B. Factors associated with emergency department visits for migraine: An observational study. Headache. 2014; 54(10): 1611-1618.
4. R Core team. R: a language and environment for statistical computing. Version 2024.04.0+735. https://www.r-project.org
Email: andrea.portt@mail.utoronto.ca
Role of neuroimaging in headache management; are we following the guidelines?
Background
Migraine has a worldwide incidence of 15-18%. Current recommendations suggest neuroimaging is not necessary in patients with stable uncomplicated headaches, particularly those meeting the criteria for migraine, yet the annual global costs due to liberal and often unnecessary use of neuroimaging in migraine patients is in the order of billions of dollars; 1$billion annually in the USA alone.
•
Criteria for imaging
Neuroimaging is not warranted in migraine patients who have a normal neurologic examination, and there are no atypical features or red flags present. Grade A.
Neuroimaging may be considered for unusual, prolonged, or persistent aura; increasing frequency, severity, or change in clinical features, first or worst migraine, migraine with brainstem aura, migraine with confusion, migraine with motor manifestations (hemiplegic migraine), late-life migraine accompaniments, aura without headache, side-locked headache, and posttraumatic headache. Most of these are consensus based with little or no literature support. Grade C.
Evans RW et. al. Neuroimaging for Migraine: The American Headache Society Systematic Review and Evidence-Based Guideline. Headache 2020;60:318-336.
Neuroimaging may be considered for unusual, prolonged, or persistent aura; increasing frequency, severity, or change in clinical features, first or worst migraine, migraine with brainstem aura, migraine with confusion, migraine with motor manifestations (hemiplegic migraine), late-life migraine accompaniments, aura without headache, side-locked headache, and posttraumatic headache. Most of these are consensus based with little or no literature support. Grade C.
Evans RW et. al. Neuroimaging for Migraine: The American Headache Society Systematic Review and Evidence-Based Guideline. Headache 2020;60:318-336.
Methods
Retrospective chart review of 100 headache patients referred to an outpatient neurology practice. We evaluated the use of CT and MRI imaging prior to referral to Neurology and the impact of neuroimaging on clinical management.
Results
Figure 1. Comparison of Imaging and Diagnostic Prevalence in a Migraine Study. The upper and middle bars show the number of patients with preexisting history of migraine (55%) and the toal number of diagnosed migraine (74%), respectively, who underwent neuroimaging (CT and/or MRI). The lower bar shows the percentage of neuroimaging conduted (77%) in 100 patients with any headache diagnosis. The graph highlights the high prevalence of imaging in migraine patients including those with a prior history of migraine, indicating a significant overlap in imaging and historical migraine diagnosis.
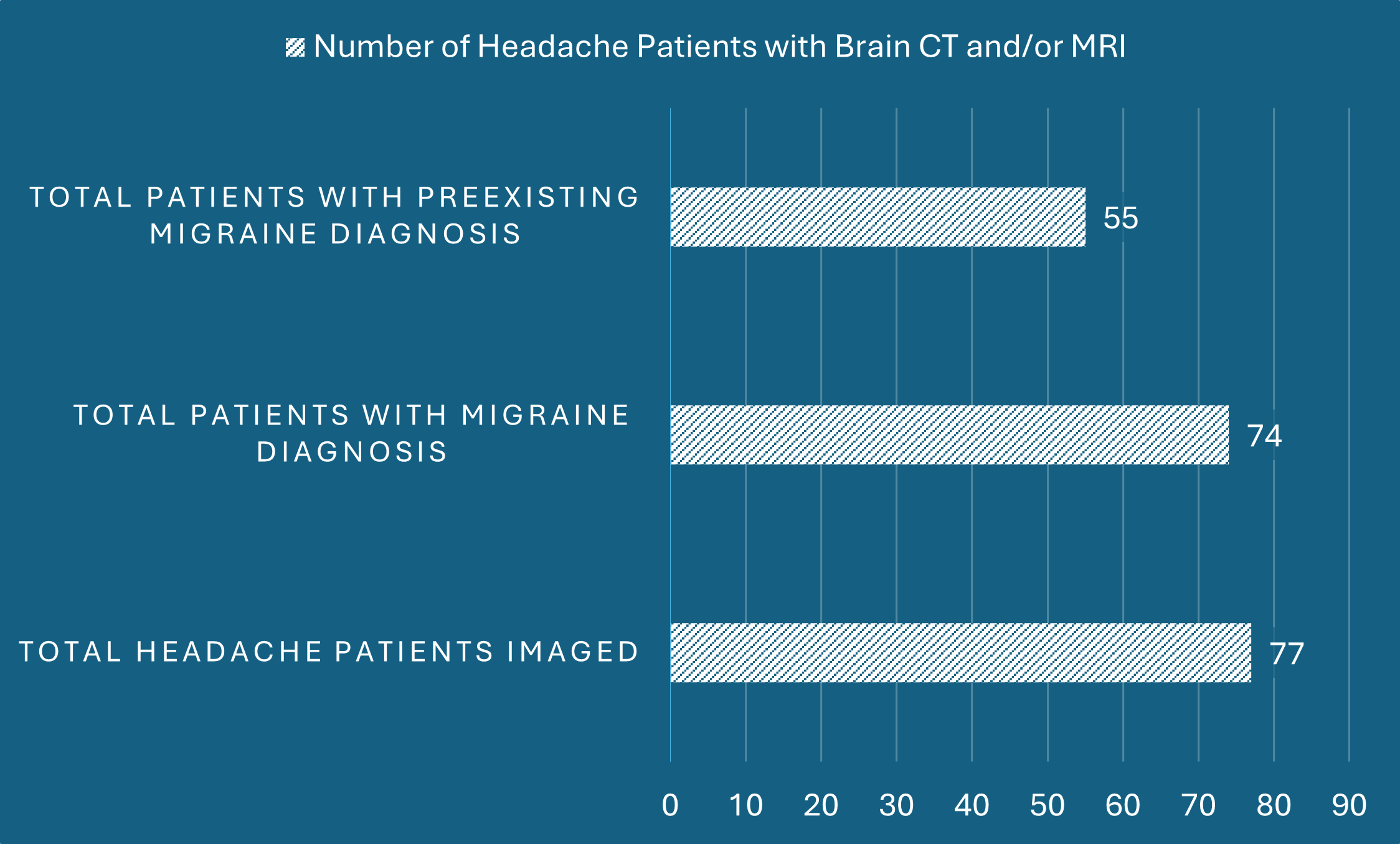
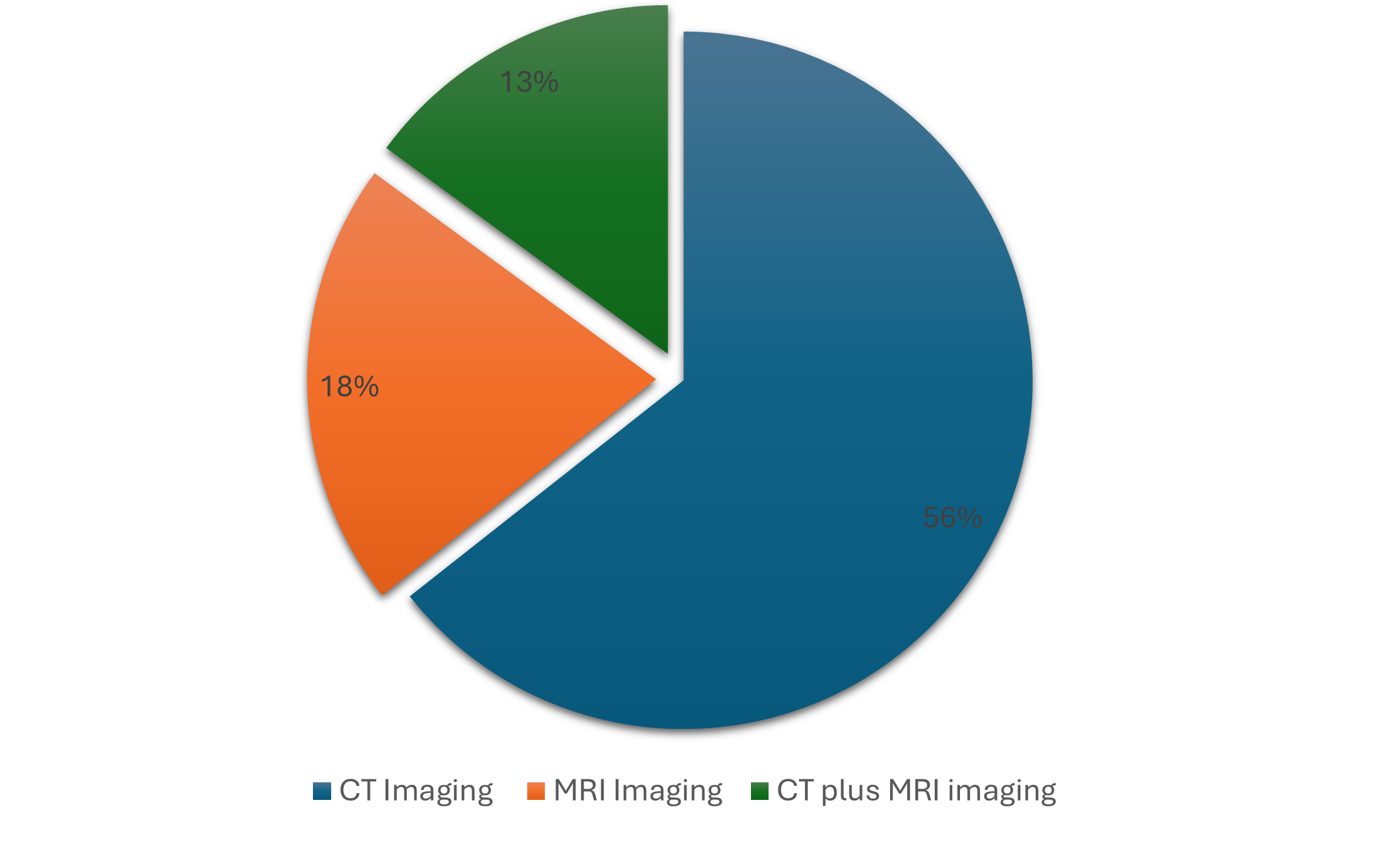
Figure 2. Distribution of Neuroimaging Among Patients with a Preexisting History of Migraine. This pie chart illustrates the proportions of different imaging types used in the evaluation of 55 patients with a known history of migraine. Independent CT scans were the most commonly used imaging technique, accounting for 56% of all imaging, followed by MRI at 32% and combined CT and MRI at 24%. Overall CT and MRI imaging were employed in 69% and 56 % of cases, resectively, emphasizing the liberal use of neuroimaging among patient with known history of Migraine.
Conclusions
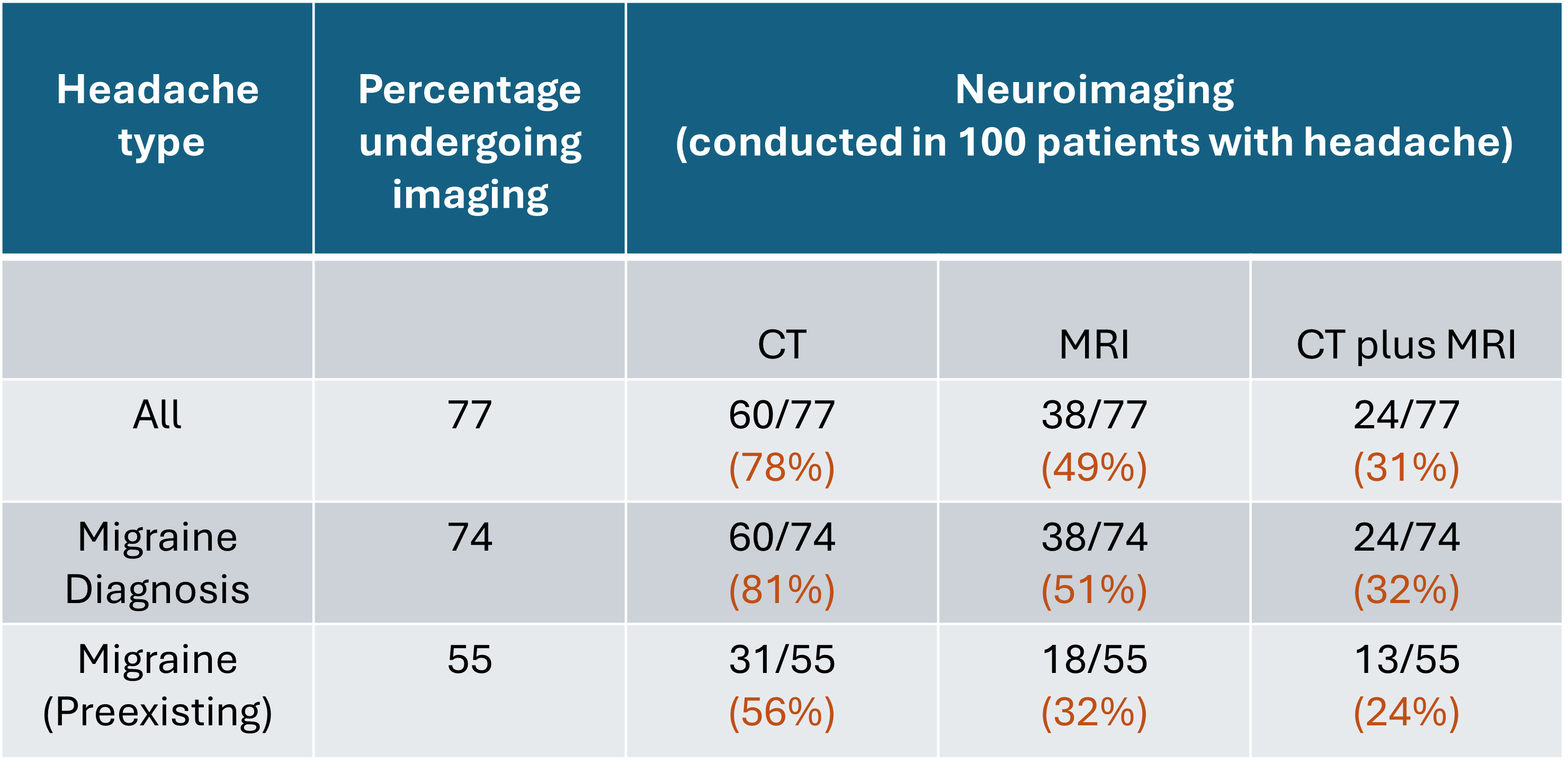
Table 1. Neuroimaging Utilization in Patients with Headache and Migraine Diagnoses. The table shows the high usage of neuroimaging in headache/migraine patients; neuroimaging did not alter headache management. The data is consistent with current guidelines suggesting that neuroimaging is not necessary in patients with stable headaches, particularly migraine.
Neuroimaging overuse might reflect:
• Lack of awareness of guideline recommendations.
• Insecurity over diagnoses.
• Medicolegal concerns.
• Busy practice conditions where tests are ordered as a shortcut.
• Addressing patients (and their families) and primary practitioners’ concerns/expectations (better safe than sorry).
Resources to help improve public and physician awareness regarding neuroimaging use in patients with stable headache may help reduce unwarranted imaging studies and could have significant financial savings for healthcare systems.
References
1.Evans RW, Burch RC, Frishberg BM et. al. Neuroimaging for Migraine: The American Headache Society Systematic Review and Evidence-Based Guideline. Headache 2020;60:318-336.
2.Detsky ME, McDonald DR, Baerlocher MO. Does this patient with headache have a migraine or need neuroimaging? JAMA 2006;296:1274-83.
3.O’Brien et al. Prevalence of Migraine headache in Canada: a population-based survey. Int. J. Epidemiology 1994;23: 1020-26
Spontaneous retropulsion in autopsy verified progressive supranuclear palsy
Background
Progressive supranuclear palsy (PSP) is a neurodegenerative disease classically presenting with parkinsonism, vertical gaze palsy, and cognitive decline.1 Since its initial description in 1964 (Steele-Richardson-Olszewski), multiple subtypes have been described.2 Postural instability is a common symptom of PSP.3 Spontaneous retropulsion involves loss of balance without external provocation. Others have reported on retropulsion in the clinical setting while testing for postural instability,4, 5 but rates of spontaneous retropulsion in the community have not been described.
Clinical diagnostic accuracy of PSP approaches 80%6 with the most recent diagnostic criteria boasting a sensitivity and specificity of 88% and 86%2 respectively. Despite increasing accuracy of recent diagnostic criteria, 20% of PSP diagnoses are incorrect6 which impacts clinical reports in the PSP literature. Most studies use patients with clinical diagnoses of PSP without pathological confirmation. Definite diagnosis of PSP requires brain autopsy, and studies with autopsy confirmed PSP therefore provide the highest degree of diagnositc accuracy.
This study aims to report on the prevalence of spontaneous retropulsion in PSP, and identify variables that may be associated with that phenomenon. The data for this study was gathered exclusively from the charts of patients with clinical and pathology-confirmed PSP.
Methods
All PSP cases assessed at the Saskatchewan Movement Disorders Program (SMDP) clinics between 1968 and 2022 with brain autopsy were considered. A retrospective chart review examined 60 patients from the SMDP with clinical and pathology-confirmed diagnosis of PSP. Information regarding patient falls were collected at each clinic visit. We identified patients who endorsed spontaneous retropulsion. The data was analysed with univariate logistic regression.
Every patient assessed in clinic has a choice of autopsy study at no cost to the family or the estate of the patient. Regardless of the wish of the patients, the autopsy decision is made by the next-of-kin after death of the individual. Movement disorders neurologists are on 24/7 call for autopsy. Typically, the neurologist is contacted by the family/caregiver soon after the death to inform that the family wants an autopsy study.
The neurologist secures autopsy consent and arranges coordination between family, funeral home and pathology department to ensure that the autopsy is done within 24 hours of death. Immediately after the autopsy, the brain is divided at midline. One-half is frozen at -80oC. The other half is fixed in formalin and studied by a Canadian certified neuropathologist. Final diagnosis is made by the treating neurologist, considering the clinical information and pathology findings.

Consent for autopsy is approved by Saskatchewan Health Authority and the use of brain tissue for diagnosis and research is approved by the Bioethics Board of the University of Saskatchewan.
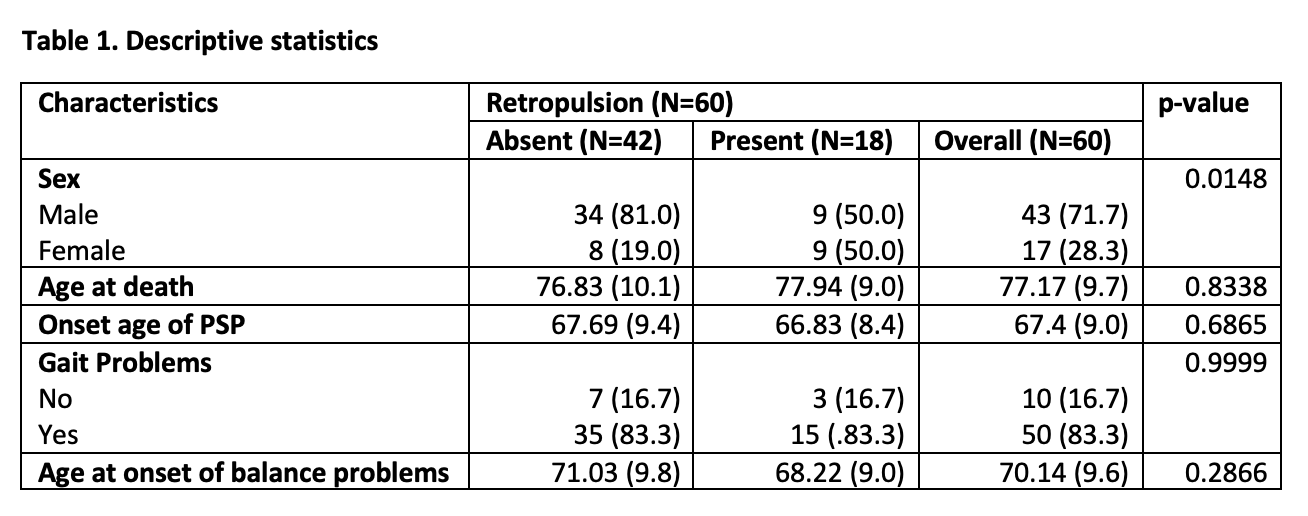
Results
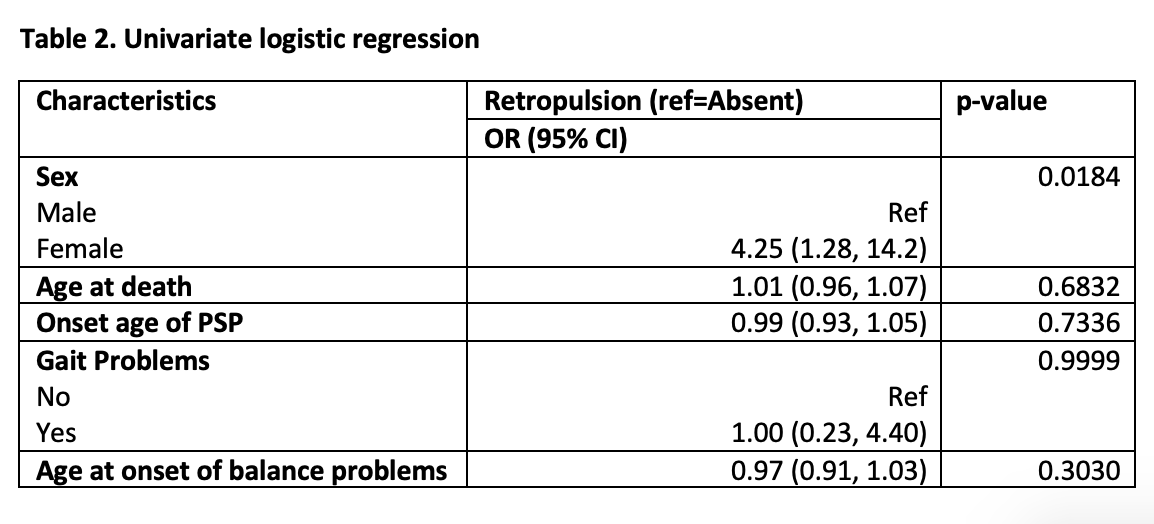
This study included 43 males and 17 females. Spontaneous retropulsion was reported in 18 (30%) patients. For categorical and continuous variables, chi-squared and Mann Whitney U tests were conducted respectively. Among the variables, only sex showed a statistical significance (p = 0.0184) with females more likely to report spontaneous retropulsion (OR = 4.25). Other variables (PSP onset age, onset age of balance impairment, gait impairment, and disease duration) were not statistically significant. Multivariate analysis was performed but did not identify significant findings.
Conclusion
Our data suggest that spontaneous retropulsion is common in PSP (30% of our patients), with females being at a significantly higher risk than males. This is useful information when counselling patients on risk-avoidance behaviour to prevent falls. It may also help with selection of ambulatory devices and influence the training of patients to use these devices to compensate for the risk of spontaneous retropulsion.
Future direction will include analysis of the prevalence of spontaneous retropulsion in Parkinson disease and other non-PSP forms of parkinsonism. In addition, sub-analysis of the PSP cases in this study may provide further insight. Retroactive application of the 2017 MDS diagnostic criteria for PSP may reveal subtypes of PSP that are more likely to exprience spontaneous retropulsion.
References
1. Steele JC., Richardson JC, Olszewski J. Progressive Supranuclear Palsy. A Heterogeneous degeneration involving the brain stem, basal ganglia and cerebellum with vertical gaze and pseudobulbar palsy, nuchal dystonia and dementia. Arch Neurol. 1964;10:333. doi: 10.1001/archneur.1964.00460160003001.
2. Höglinger GU, Respondek G, Stamelou M, et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov Disord. 2017;32:853–64. doi: 10.1002/mds.26987.
3. Birdi S, Rajput AH, Fenton M, et al. Progressive supranuclear palsy diagnosis and confounding features: report on 16 autopsied cases. Mov Disord. 2002;17:1255–64. doi: 10.1002/mds.10211.
4. Borm CDJM, Krismer F, Wenning GK, et al. Axial motor clues to identify atypical parkinsonism: A multicentre European cohort study. Parkinsonism Relat Disord. 2018;56:33–40. doi: 10.1016/j.parkreldis.2018.06.015.
5. Geroin C, Nonnekes J, Erro R, Camozzi S, Bloem BR, Tinazzi M. Shoulder‐touch test to reveal incongruencies in persons with functional motor disorders. Eur J Neurol. 2022:3508-3512. doi: 10.1111/ene.15532.
6. Osaki Y, Ben-Shlomo Y, Lees AJ, et al. Accuracy of clinical diagnosis of progressive supranuclear palsy. Mov Disord. 2004:181–9. doi: 10.1002/mds.10680.
2. Höglinger GU, Respondek G, Stamelou M, et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov Disord. 2017;32:853–64. doi: 10.1002/mds.26987.
3. Birdi S, Rajput AH, Fenton M, et al. Progressive supranuclear palsy diagnosis and confounding features: report on 16 autopsied cases. Mov Disord. 2002;17:1255–64. doi: 10.1002/mds.10211.
4. Borm CDJM, Krismer F, Wenning GK, et al. Axial motor clues to identify atypical parkinsonism: A multicentre European cohort study. Parkinsonism Relat Disord. 2018;56:33–40. doi: 10.1016/j.parkreldis.2018.06.015.
5. Geroin C, Nonnekes J, Erro R, Camozzi S, Bloem BR, Tinazzi M. Shoulder‐touch test to reveal incongruencies in persons with functional motor disorders. Eur J Neurol. 2022:3508-3512. doi: 10.1111/ene.15532.
6. Osaki Y, Ben-Shlomo Y, Lees AJ, et al. Accuracy of clinical diagnosis of progressive supranuclear palsy. Mov Disord. 2004:181–9. doi: 10.1002/mds.10680.
Acknowledgments
We wish to acknowledge the members of the neuropathology division at the University of Saskatchewan for their timely and meticulous assessment of autopsy cases for the SMDP. We also acknowledge the maintenance staff at Royal Univerisity Hospital for their time and effort spent for upkeep of the SMDP laboratory.

LONG-TERM COMPARATIVE EFFICACY OF INEBILIZUMAB IN THE AQP4+ SUBPOPULATION FROM THE N-MOMENTUM OPEN-LABEL EXTENSION VERSUS AZATHIOPRINE AND IMMUNOSUPPRESSANTS AND VERSUS PLACEBO IN PATIENTS WITH NMOSD

OBJECTIVE
- To compare the long-term efficacy of INEB treatment in the N-MOmentum open label extension period (OLP) to historical controls treated with AZA or other ISTs as well as to no treatment.
INTRODUCTION
• Neuromyelitis optica spectrum disorder (NMOSD) is a rare, severe autoimmune disease characterized by acute inflammatory attacks afflicting the central nervous system.1-2
• CD19+ B cells, including plasmablasts and plasma cells, produce AQP4 auto-antibodies that cause astroglial injury.3-6
• Approved treatments for AQP4-positive (AQP4+) NMOSD include inebilizumab (INEB), an anti-CD19 B cell-depleting antibody; satralizumab, an anti-interleukin (IL)-6 receptor antibody; and eculizumab, an anticomplement C5 antibody.7-10
• Off-label treatments include immunosuppressants (ISTs) such as azathioprine (AZA) and mycophenolate mofetil (MMF);11,12 however, there is scarce data on long-term outcomes with these frequently used oral ISTs.
• Inebilizumab efficacy and safety in NMOSD was evaluated in the N-MOmentum trial which had a randomized placebo (PBO)-controlled period of about 6 months.7 Longer-term outcomes in N-MOmentum lack parallel control groups.
Poster presented at CNSF 2024, May 20-26, Toronto, Canada.
METHODS
- N-MOmentum (NCT02200770) consisted of a 28-week randomized-controlled period (RCP). Participants in the RCP who had an adjudicated attack, completed the RCP, or were in the RCP when enrollment stopped were able to enter an into the OLP in which all participants received treatment with INEB (300 mg every 6 months) for at least 2 years.7
- In the absence of a direct PBO arm or IST comparators in the OLP, we used historical data to evaluate the long-term comparative efficacy of the INEB monotherapy.
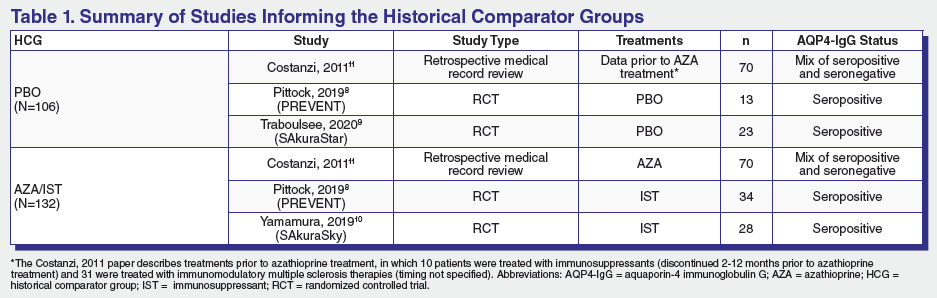
- Historical comparator groups were derived using data from published NMOSD studies to evaluate the comparative efficacy of INEB treatment (AQP4+ subgroup; N=208) over the OLP. Data from untreated patients was pooled from the observational study of AZA in NMOSD11 that was used to model the sample size from N-MOmentum as well as two contemporaneous PBO treated arms from the PREVENT8 study of eculizumab and the SAkuraStar9 study of satralizumab. Data from patients treated with AZA or other broad spectrum oral ISTs was pooled from the observational study of AZA in NMOSD, PREVENT and the SAkuraSky study of satralizumab in NMOSD (Table 1).
- Hazard ratios (HR) for the INEB group versus historical comparator groups were estimated using Cox proportional hazards regression.
- Time to NMOSD attack was modelled using parametric and flexible survival (spline) models that were fit to the INEB group and historical comparator groups. Model selection was determined by testing the Cox proportional hazards and accelerated failure time assumptions as well as assessing Akaike’s information criterion/Bayesian information criterion, visual fit, estimated attack-free survival at 4 years, and clinical validation.
RESULTS
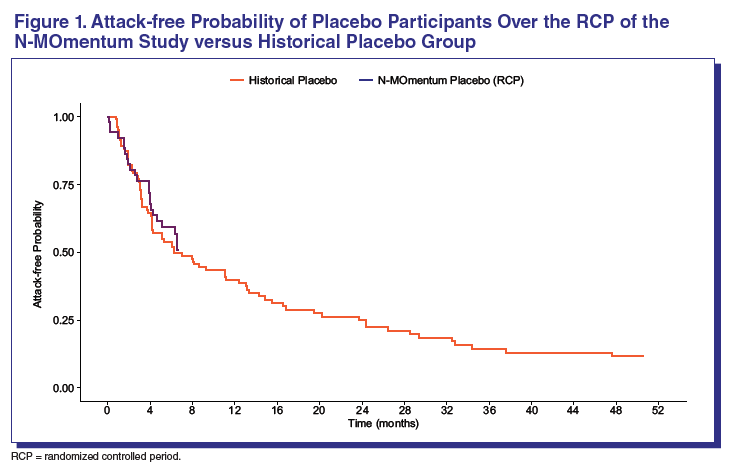
• There was no significant difference in NMOSD attack risk between the historical PBO group and those receiving PBO during the N-MOmentum RCP (HR: 1.15; 95% CI: 0.67–1.91; P value = 0.58) suggesting that the historical PBO group was similar to the population studied in N-MOmentum (Figure 1) with respect to attack risk.
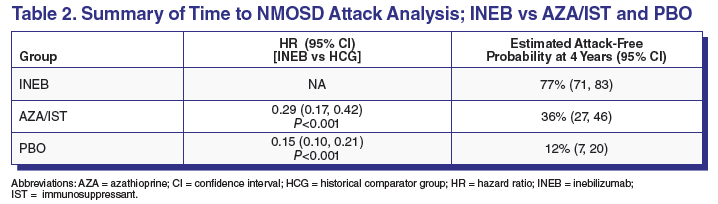
• There was a significant reduction in the risk of NMOSD attack for the INEB treatment group as compared to both the AZA/IST and historical PBO groups (Table 2).
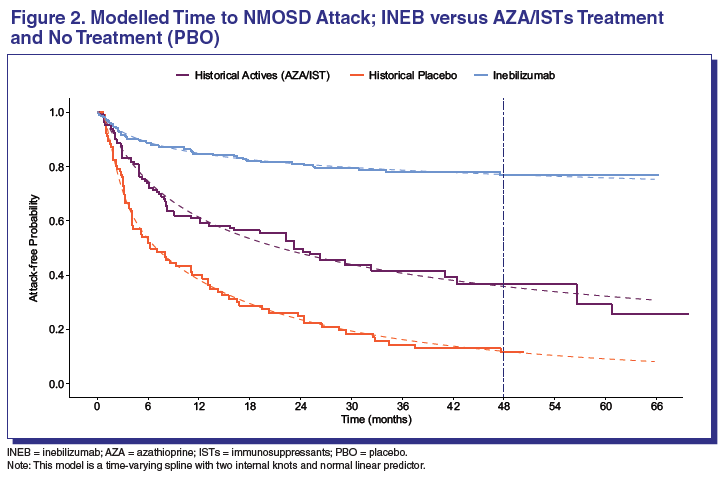
• A time-varying spline with two internal knots and normal linear predictor provided the best fit. The model estimated sustained attack-free probability for the INEB treatment group as compared to the AZA/IST and PBO groups (Figure 2).
– All time points, the risk of attack is lower with INEB than either historical control group (PBO or AZA/IST).
– The increasing separation to 4 years suggests INEB relative efficacy is maintained and may increase with duration of treatment.
• At 4 years, there was a greater difference in attack-free probability for INEB versus PBO compared to AZA/IST versus PBO, suggesting a substantial reduction in risk of attack for INEB treatment compared to both AZA/IST treatment or no treatment (PBO) (Table 2).
CONCLUSIONS
• INEB treatment was associated with a statistically significant reduction in risk of an NMOSD attack vs both AZA/IST treatment and no treatment (PBO).
• INEB treatment provided a long-term attack-free probability compared to the relative short-term probability observed with AZA/IST treatment.
• The PBO group from the RCP had a similar attack risk as the historical PBO controls, suggesting the populations are similar and supports the validity of using historical datasets for these comparisons.
SAFETY AND EFFICACY OF INEBILIZUMAB IN AQP4+ NMOSD PARTICIPANTS WITH HISTORY OF IMMUNOSUPRESSION TREATMENT PRIOR TO N-MOMENTUM STUDY

OBJECTIVE
To evaluate long-term outcomes of INEB treatment in AQP4+ NMOSD participants from the N-MOmentum trial with a history of immunosuppressant therapy with azathioprine (AZA) and/or mycophenolate mofetil (MMF) as compared to those without.
To evaluate long-term outcomes of INEB treatment in AQP4+ NMOSD participants from the N-MOmentum trial with a history of immunosuppressant therapy with azathioprine (AZA) and/or mycophenolate mofetil (MMF) as compared to those without.
INTRODUCTION
- Inebilizumab (INEB), an anti-CD19 B cell-depleting antibody, is approved for the treatment of neuromyelitis optica spectrum disorder (NMOSD) in adults seropositive for aquaporin-4 antibody (AQP4+).
-
The safety and efficacy of INEB in NMOSD was assessed in the N-MOmentum (NCT02200770) study.1
- In N-MOmentum, INEB reduced the risk of an adjudicated NMOSD attack by 77% compared with placebo.1
- INEB was generally well tolerated and reduced disability worsening, magnetic resonance imaging (MRI) lesion activity and NMOSD-related hospitalizations compared with placebo.1
- The benefits of INEB were maintained with long-term treatment.2,3
- Immunosuppressants were prohibited during the N-MOmentum pivotal trial, although many participants had a history of immunosuppressant therapy before enrollment.
METHODS
-
N-MOmentum (NCT02200770) was a double-blind, placebo controlled, randomized phase 2/3 trial that assessed the efficacy and safety of INEB in adults with NMOSD, and comprised two periods:
- Randomized control period (RCP; 3:1 to INEB [intravenous, 300 mg] or placebo) for 28 weeks or to an adjudicated attack
- Optional open-label period (OLP; INEB every 6 months) for ≥2 years
-
N-MOmentum included adults with NMOSD who had received treatment for ≥1 attack in the past year or ≥2 attacks in the past 2 years, and who had an EDSS score ≤8.0.
- The primary endpoint was time to first adjudicated attack during the RCP.
- Secondary endpoints included the annualized attack rate (AAR), disability progression assessed via the expanded disability status scale (EDSS), and number of NMOSD-related inpatient hospitalizations.
- Safety assessments included treatment-emergent adverse events (TEAEs) and treatment-emergent adverse events of special interest (AESIs).
Poster presented at CNSF 2024, May 20-26, Toronto, Canada.
- Immunosuppressant medication for the prevention or treatment of NMOSD relapses was allowed prior to dosing on Day 1 but prohibited during the trial.
- In this post hoc analysis, AQP4+ participants were grouped by no prior immunosuppression therapy beyond treatment of acute NMOSD attacks (naive), or prior azathioprine (AZA) and/or mycophenolate mofetil (MMF) therapy.
- Outcomes assessed for these two groups included: AAR, Disability progression (EDSS), NMOSD-related inpatient hospitalizations, safety assessments
RESULTS
Participants
Participants
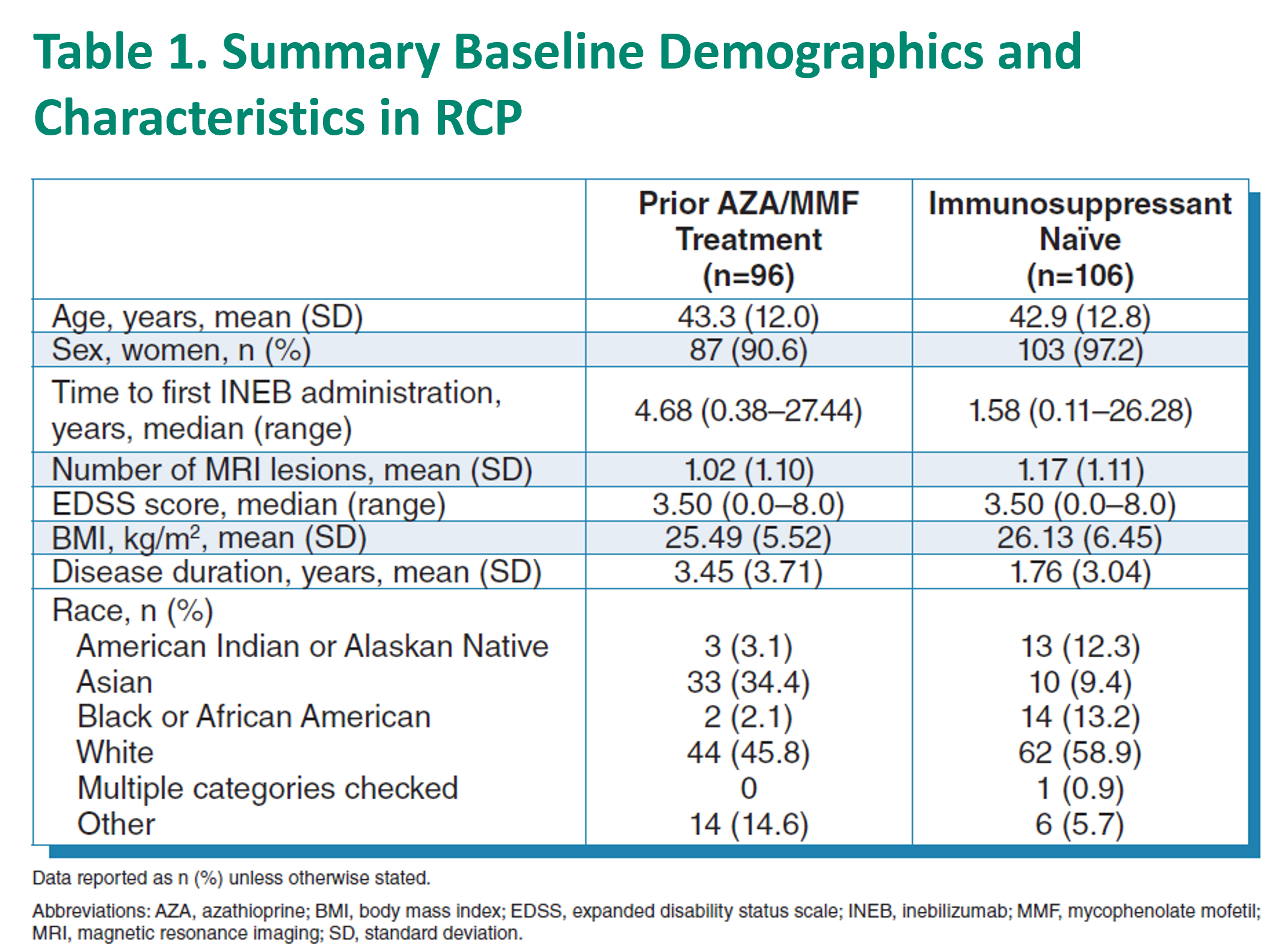
- Among participants who received any INEB during the OLP, a total of 94 had received prior AZA/MMF treatment and 103 were immunosuppressant naïve before entering the study.
- Participants in the immunosuppressant naïve group had an overall shorter duration of disease and faster time to first INEB administration.
NMOSD Attack
- During the RCP, fewer participants in both the prior AZA/MMF group and the immunosuppressant naïve group having received treatment with INEB had an adjudicated attack compared with those receiving placebo.
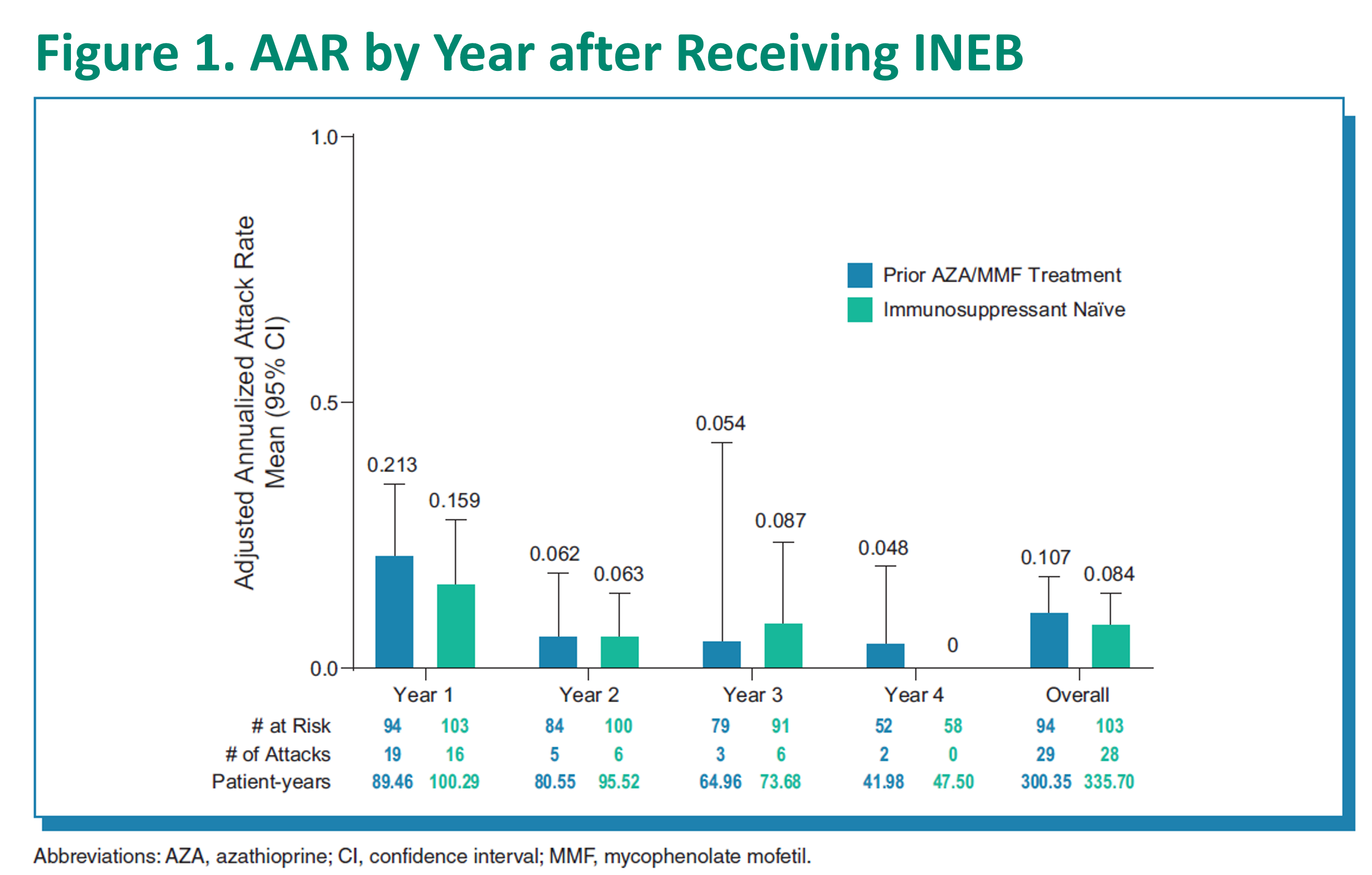
- The total patient-years of INEB treatment in the prior AZA/MMF group was 300.35 and for immunosuppressant naïve participants, 335.7.
- The AAR (95% confidence interval [CI]) for participants with prior AZA/MMF treatment was 0.11 (0.07, 0.17), compared to 0.08 (0.05, 0.14) for the immunosuppressant naïve group.
REFERENCES
1. Cree BAC, et al. Lancet. 2019;394:1352-63.
2. Cree BAC, et al. Poster A-21-00375 presented at EAN 2021.
3. Cree BAC, et al. Poster P2283 presented at AAN 2021.
1. Cree BAC, et al. Lancet. 2019;394:1352-63.
2. Cree BAC, et al. Poster A-21-00375 presented at EAN 2021.
3. Cree BAC, et al. Poster P2283 presented at AAN 2021.
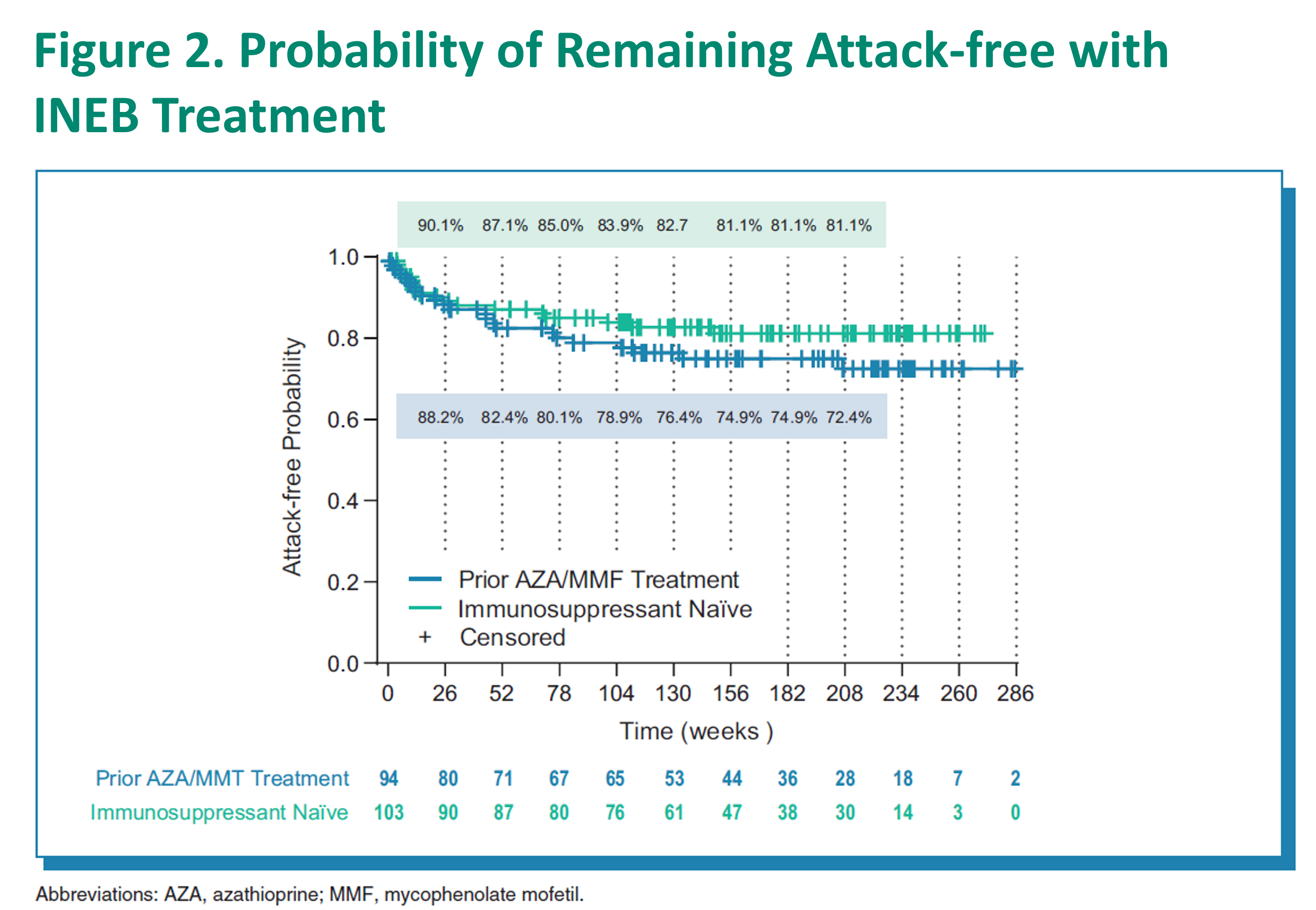
- All participants receiving INEB had a high probability of remaining attack-free over time.
- When stratified by year, the AAR was low and similar for participants having received INEB in the prior AZA/MMF treatment group and the immunosuppressant naïve group.
Disability Progression
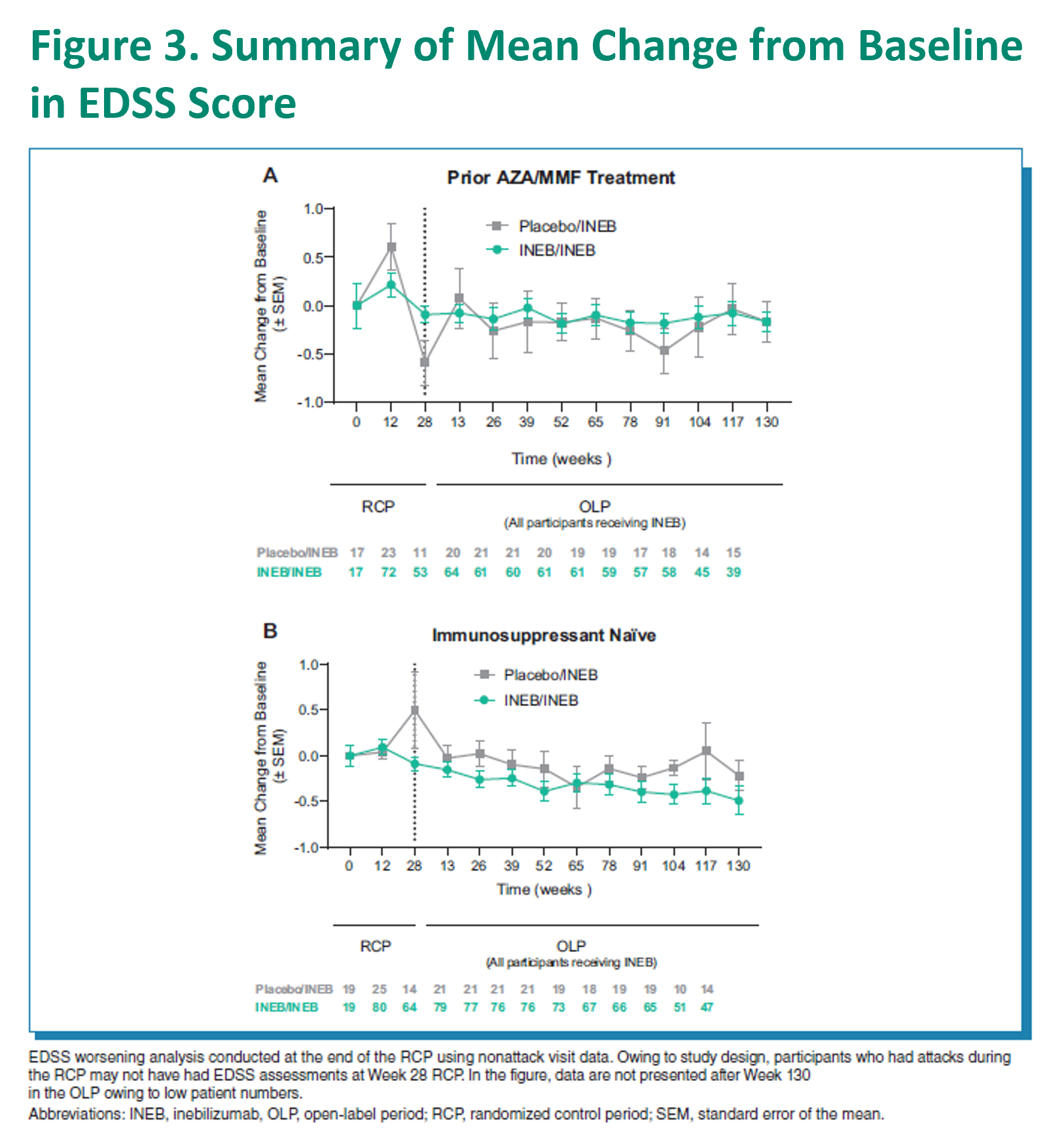
- During RCP, a smaller proportion of participants had EDSS score worsening with INEB treatment vs placebo in both participants receiving prior AZA/MMF treatment (19.2% vs 43.5%) and those in the immunosuppressant naïve group (13.6% vs 28.0%).
- Stabilization of EDSS score was seen in both groups throughout the OLP.
Rate of NMOSD-related Inpatient Hospitalizations
- During RCP, a smaller proportion of participants had NMOSD-related inpatient hospitalizations with INEB treatment vs placebo in both those having received prior AZA/MMF treatment and those in the immunosuppressant naïve group.
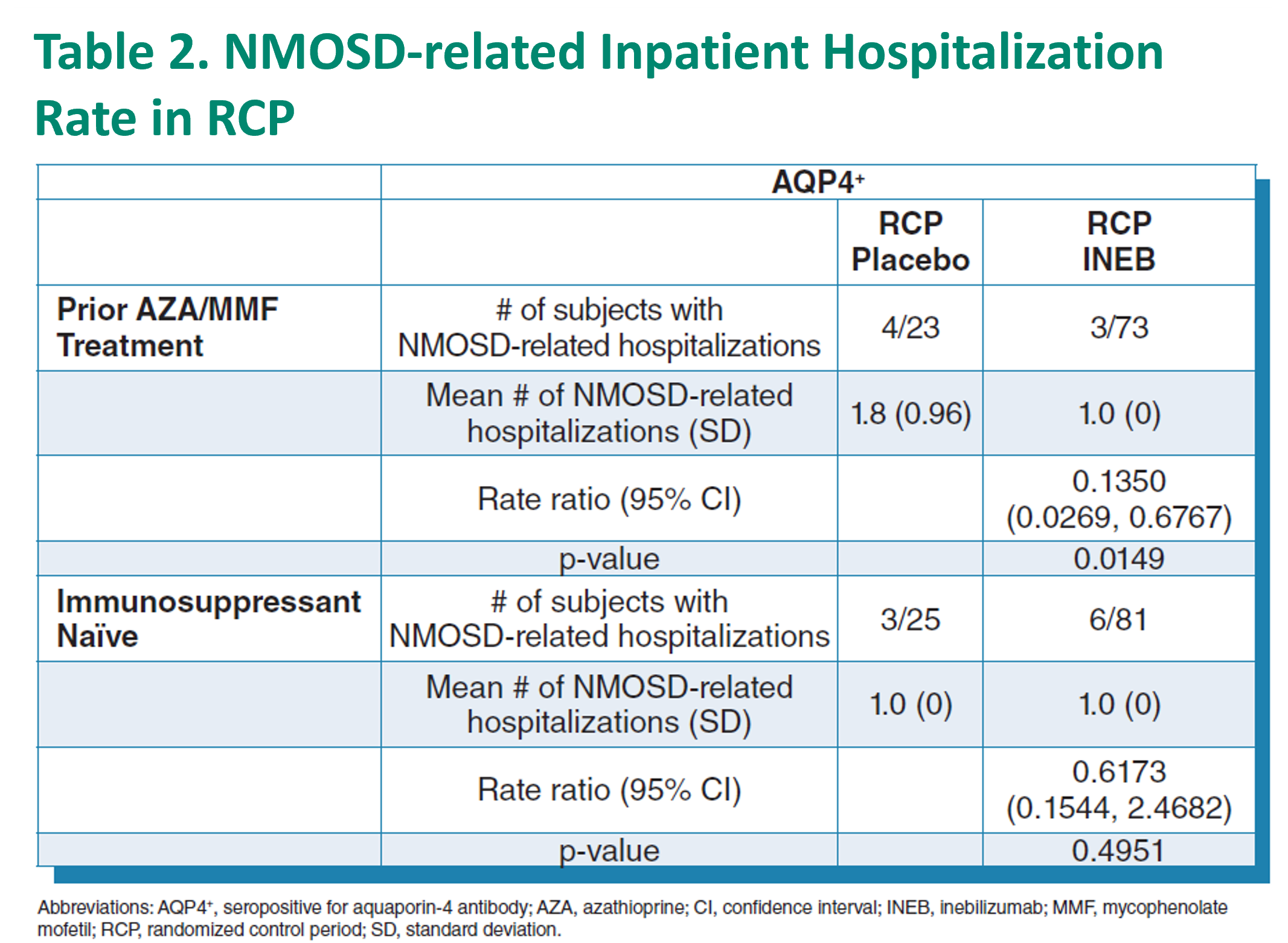
- Through the OLP, a similar number of inpatient hospitalizations were observed in the prior AZA/MMF group (40) and the immunosuppressant naive group (40).
- The annualized NMOSD-related inpatient hospitalization rate (annualized rate [95% CI]) for prior AZA/MMF treatment was 0.15 (0.08, 0.27), and 0.12 (0.06, 0.22) for immunosuppressant naïve participants.
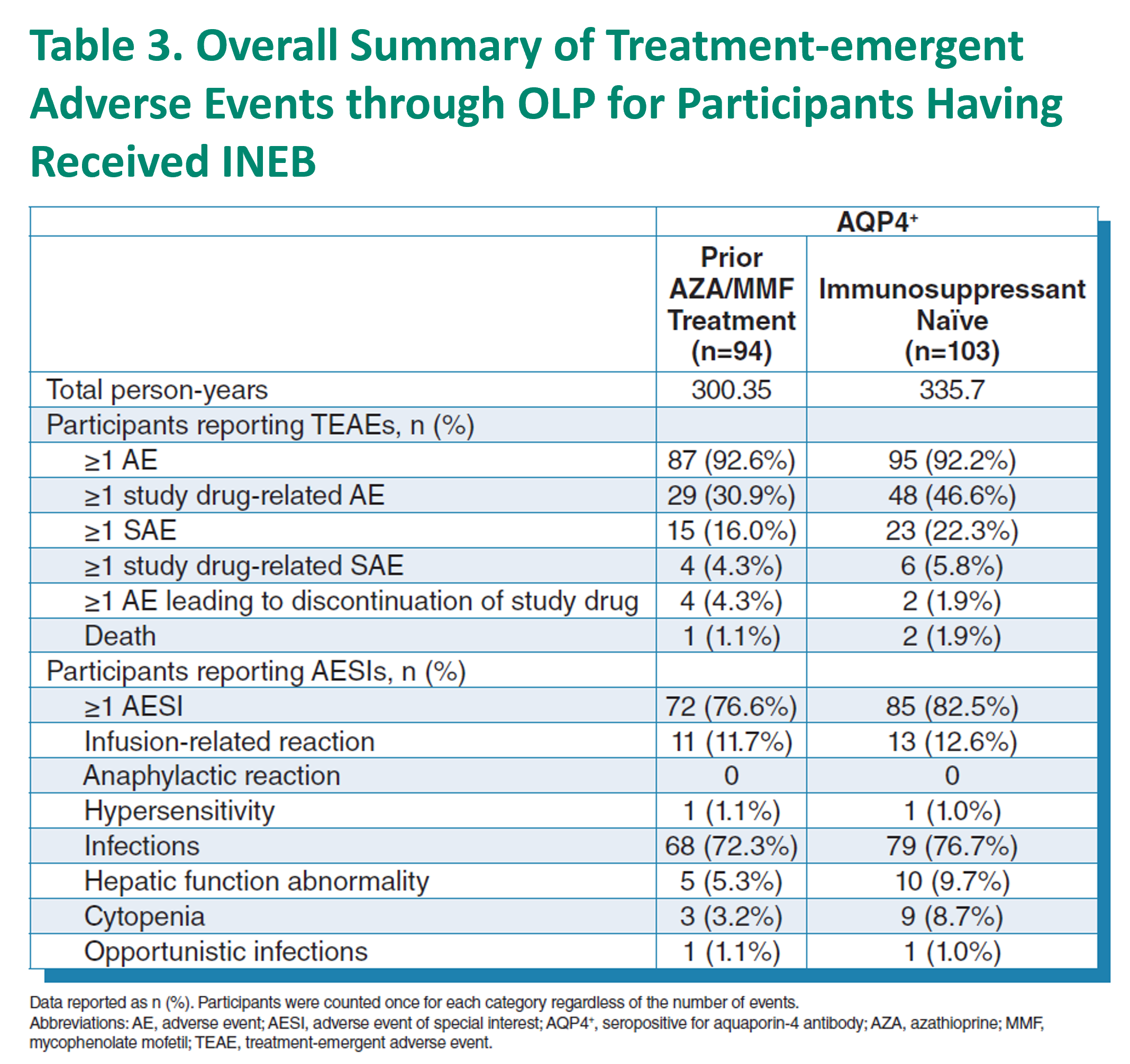
- The percentage of participants with ≥1 study drug-related TEAE was 30.9% (29/94) in the prior AZA/MMF group and 46.6% (48/103) in the immunosuppressant naive group; 4.3% (4) of prior AZA/MMF and 5.8% (6) of immunosuppressant naive reported ≥1 study drug-related serious adverse event.
- Most adverse events were infection-related for both groups; (72.3% (68/94) for prior AZA/MMF and 76.7% (79/103) for immunosuppressant naive).
CONCLUSION Outcomes of INEB in AQP4+ NMOSD participants that received prior AZA and/or MMF therapy demonstrated a similar efficacy/safety profile.
Efficacy and safety of ravulizumab in adults with AQP4+ NMOSD: interim analysis from the ongoing phase 3 CHAMPION-NMOSD trial
BACKGROUND
- Anti-aquaporin-4 antibody-positive (AQP4-Ab+) neuromyelitis optica spectrum disorder (NMOSD) is a rare autoimmune disease of the central nervous system characterized by repeated, unpredictable relapses, leading to accumulation of irreversible neurologic disability1,2
-
In the phase 3 PREVENT trial, the C5 inhibitor therapy eculizumab was well tolerated and reduced the risk of relapse in patients with AQP4-Ab+ NMOSD by 94.2% relative to placebo (Figure 1)3
- Results of this trial led to approval of eculizumab to treat AQP4-Ab+ NMOSD in adults in numerous countries and regions, including Europe, Japan, and the US4-6
-
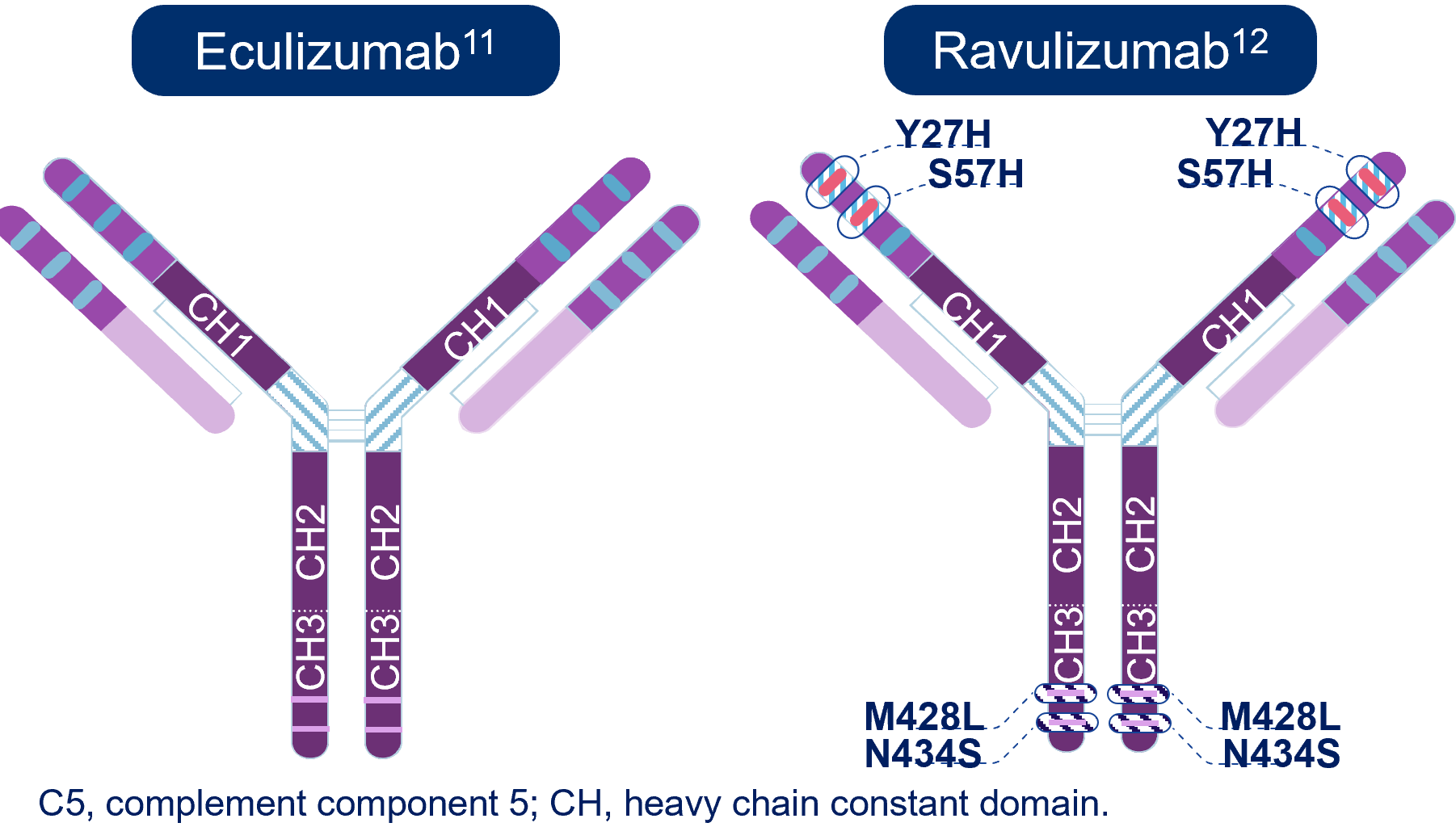
Ravulizumab was developed from and binds to the same C5 epitope as eculizumab but has a longer elimination half-life, enabling an extended dosing interval of every 8 weeks instead of every 2 weeks (Figure 1)7
- Ravulizumab is also approved to treat AQP4-Ab+ NMOSD in adults in numerous countries and regions, including Europe, Japan, and the US8-10
Figure 1. Molecular Structures of Eculizumab and Ravulizumab
OBJECTIVE
- To report the interim efficacy and safety of ravilizumab from the last data cut (June 16, 2023) of the long-term extension (LTE) period of the CHAMPION-NMOSD trial (NCT04201262) of ravulizumab in patients with AQP4-Ab+ NMOSD
METHODS
-
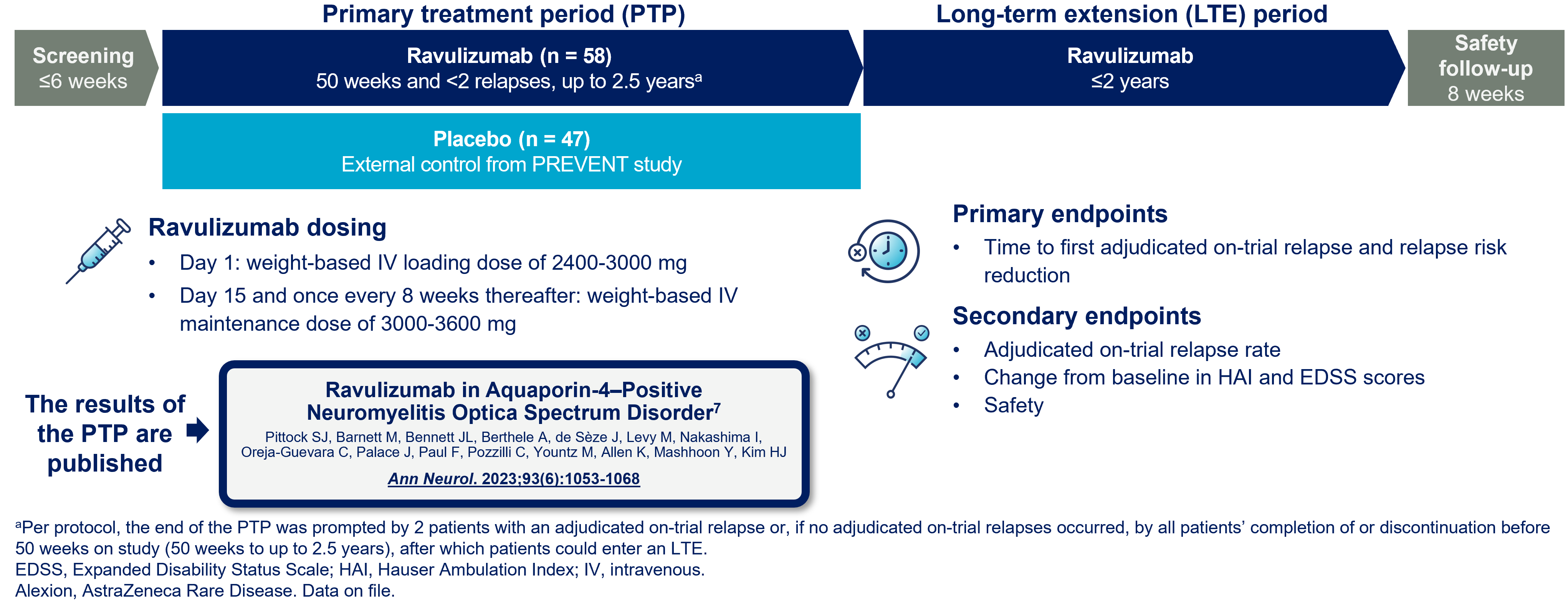
CHAMPION-NMOSD is a phase 3 pivotal, global, open-label trial of ravulizumab in patient swith AQP4-Ab+ NMOSD (Figures 2 and 3)
- The study used the placebo group from the PREVENT trial
Figure 2. CHAMPION-NMOSD Study Design

RESULTS
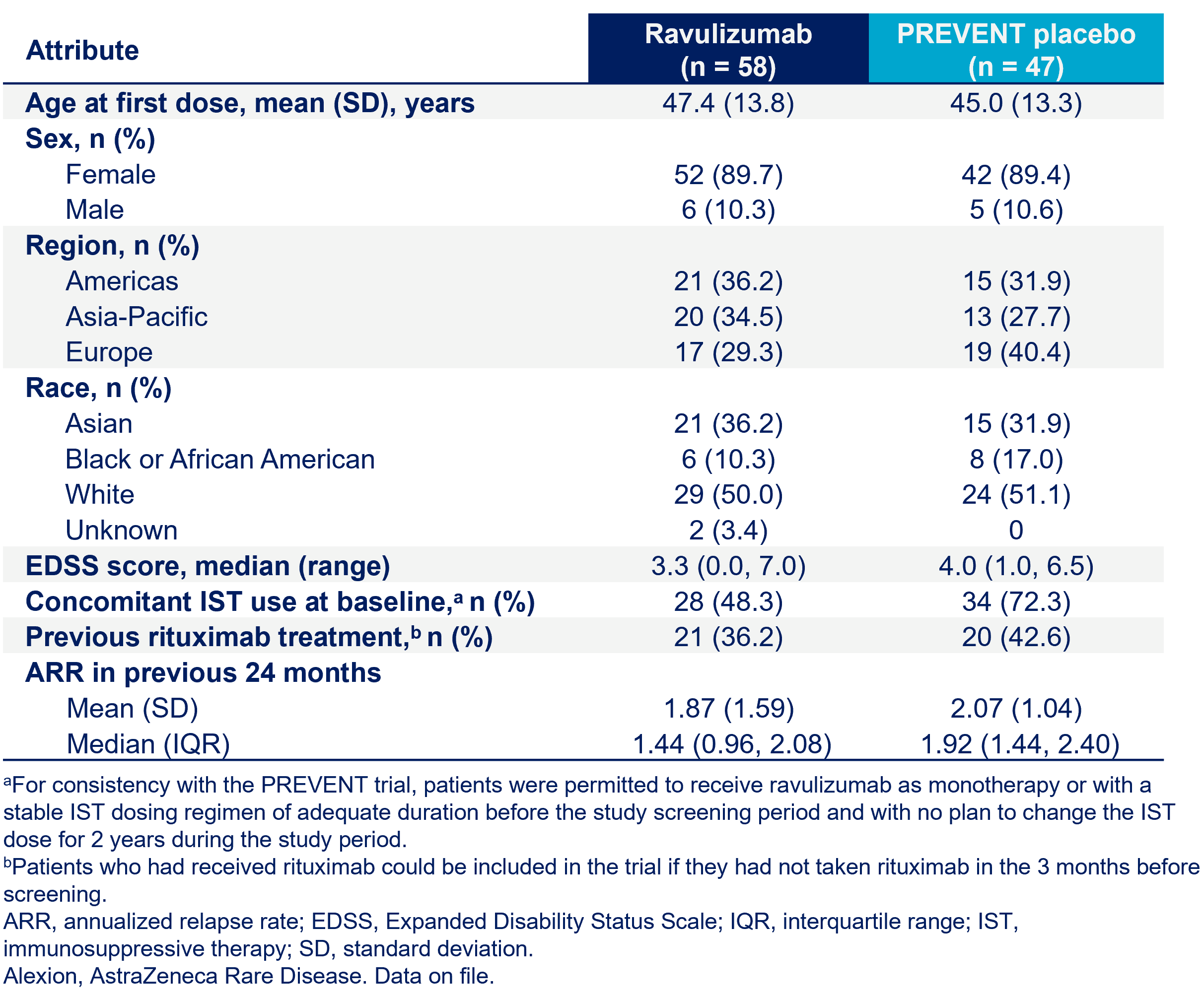
- Baseline demographics and clinical characteristics of participants treated with ravulizumab (n=58) were similar to those in the placebo group in PREVENT (n=47) (Table 1)
-
In the PTP, median (range) follow-up was 73.5 (11.0–117.7) weeks (84.0 patient-years) for ravulizumab and 36.0 (1.9–117.7) weeks (46.9 patient-years) for placebo in PREVENT
Table 1. Baseline Demographics and Clinical Characteristics7
-
Of the 58 patients being treated with ravulizumab in the PTP, 56 entered and 2 have completed the LTE as of the cutoff of June 16, 2023, with median (range) follow-up of 138.4 (11.0–183.1) weeks (153.9 patient-years)
- In the external placebo comparator group (n=47), median (range) duration of follow-up was 36.0 (1.9–183.1) weeks
-
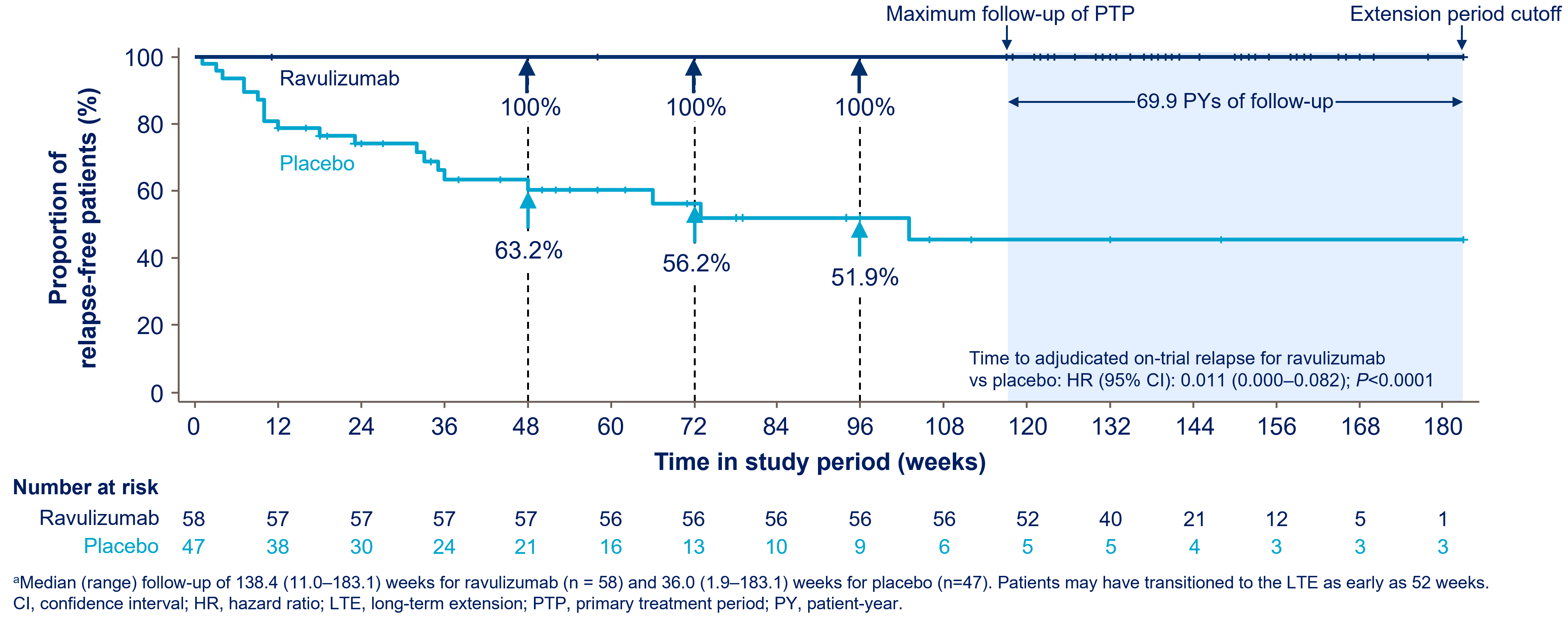
Across the PTP and LTE, no patients had an adjudicated on-trial relapse during ravulizumab treatment (153.9 patient-years of follow-up), corresponding to a 98.9% reduction in the risk of relapse with ravulizumab versus placebo (log-rank P<0.0001) (Figure 4)
- Median (range) follow-up of 138.4 (11.0–183.1) weeks for ravulizumab (n=58) and 36.0 (1.9–183.1) weeks for placebo (n=47). Patients may have transitioned to the extension period as early as 52 weeks
- HAI scores remained stable or were clinically improved in 91.4% (53/58) of patients treated with ravulizumab from baseline to the LTE cutoff (Figure 5)
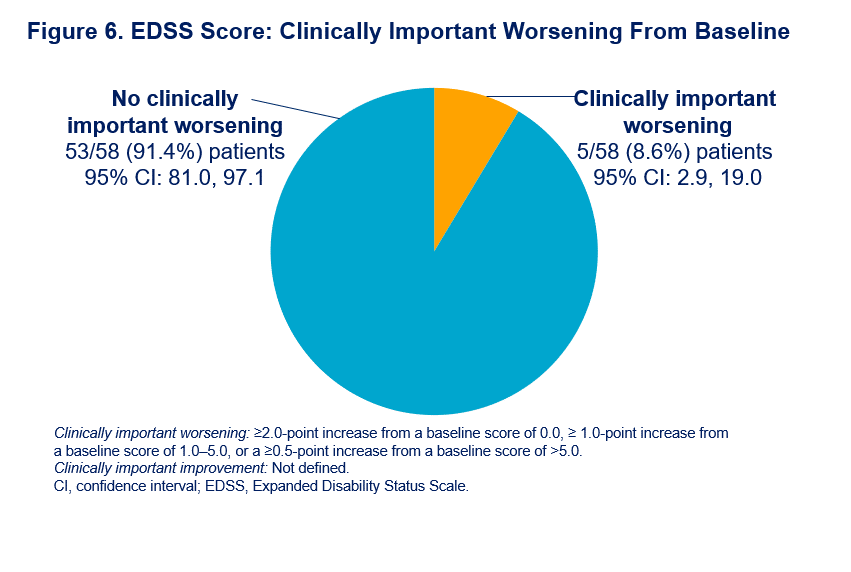
- 91.4% (53/58) of patients had no clinically important worsening in EDSS score with ravulizumab from baseline to the LTE cutoff (Figure 6)
Figure 4. Time to First Adjudicated Relapse During the PTP and LTE (data cut off: June 16, 2023)

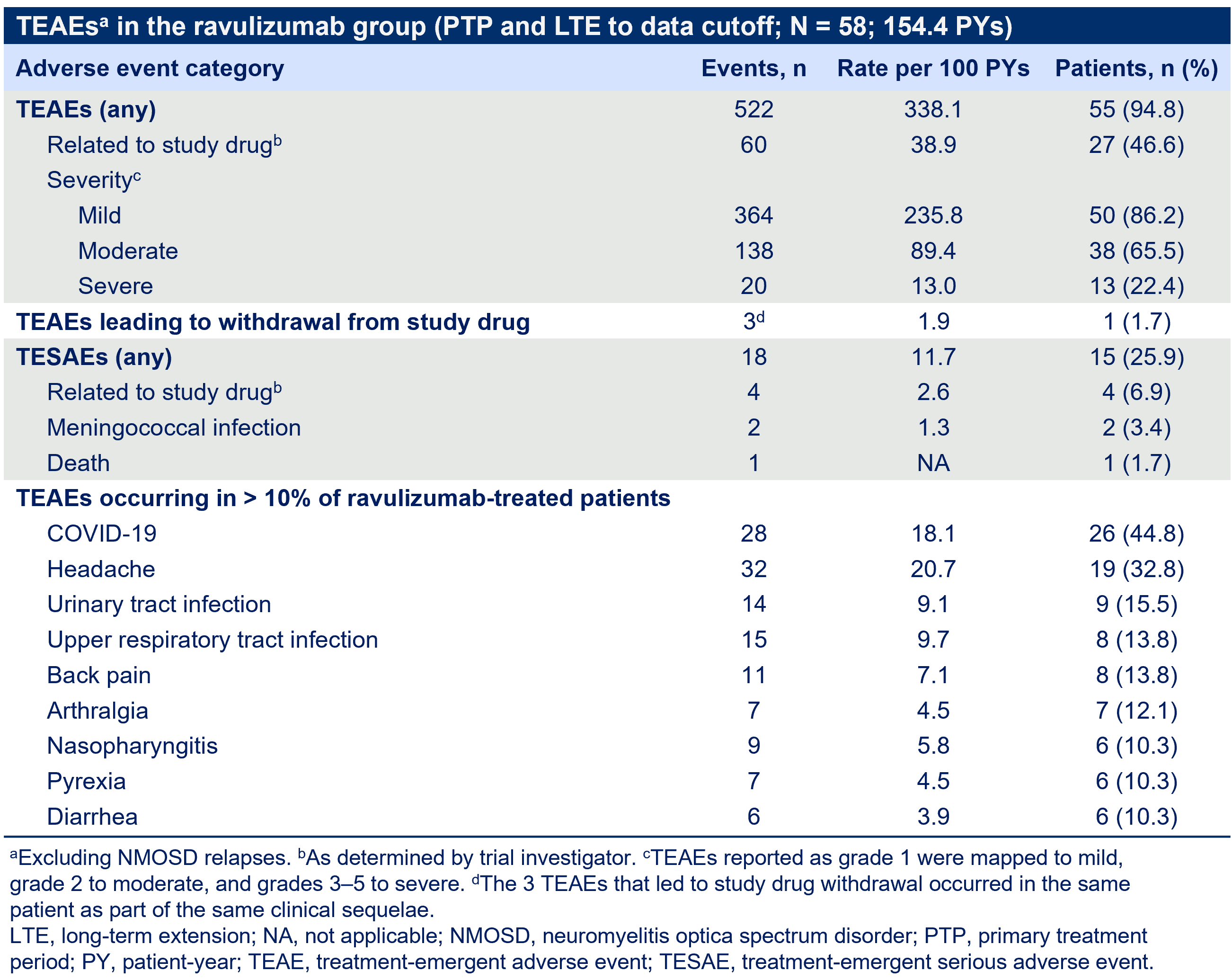
- No new safety signals were observed in the LTE (includes 69.9 patient-years of follow-up)
-
During the PTP, 2 vaccinated patients developed meningococcal infections during the PTP; both received antibiotics and intensive care and recovered with no sequelae (Table 2)
- One patient withdrew, and 1 remains in the trial
- During the LTE, no meningococcal infections occurred as of the cutoff
- One death, occurring during the LTE, was later updated to hypertensive heart disease after the data cut and assessed by the investigator as unrelated to ravulizumab
Table 2. Summary of TEAEs
CONCLUSIONS
- During a median (range) follow-up of 138.4 (11.0–183.1) weeks across the PTP (84.0 patient-years) and LTE (69.9 patient-years), no patient treated with ravulizumab experienced an adjudicated relapse
- Most patients treated with ravulizumab demonstrated stable or improved disability measures through the longer-term 138.4-week median follow-up that included the PTP and LTE
- The safety profile presented here is consistent with that observed in prior analyses, and notably no new meningococcal infections were observed beyond the 2 reported during the PTP
- Together, these findings demonstrate the long-term clinical benefit of ravulizumab in the prevention of relapses in patients with AQP4-Ab+ NMOSD
A global, long-term, prospective, observational registry of patients with AQP4+ NMOSD treated with complement component 5 inhibitor therapies eculizumab or ravulizumab
BACKGROUND
- Neuromyelitis optica spectrum disorder (NMOSD) is a rare autoimmune disease of the central nervous system characterized by repeated, unpredictable relapses, leading to accumulation of neurologic disability and reduced health-related quality of life1-3
- The complement component 5 inhibitor therapies (ALXN-C5ITs) eculizumab and ravulizumab have received or have been submitted for regulatory approval in several regions for the treatment of anti-aquaporin-4 antibody-positive (anti-AQP4+) NMOSD1,4
- In the phase 3 PREVENT study in patients with anti-AQP4+ NMOSD, eculizumab was associated with a 94.2% reduction in NMOSD relapse risk compared with placebo4
- In the phase 3 CHAMPION-NMOSD study in patients with anti-AQP4+ NMOSD, ravulizumab demonstrated a 98.6% reduction in risk of adjudicated on-trial relapse compared with external placebo1
- Real-world effectiveness and safety data from patients with anti-AQP4+ NMOSD treated with the ALXN-C5ITs are needed to supplement the existing body of scientific evidence and to better inform clinical practice
OBJECTIVE
- To present the study design of the NMO SPOTLIGHT Registry (NCT05966467),5 which will assess the long-term safety, clinical effectiveness, and real-world impact of the ALXN-C5ITs eculizumab and ravulizumab in adults with anti-AQP4+ NMOSD
STUDY DESIGN
- This global, long-term, prospective, multicenter, observational registry will enroll approximately 130 patients, with a maximum of approximately 200 patients in up to 15 countries globally (Figure 1)
- Data will be collected retrospectively from 1 year prior to ALXN-C5IT initiation through registry enrollment and prospectively for up to 5 years after enrollment for each patient; clinical data will be collected at least once annually and patient-reported outcomes data at least every 6 months (Figure 2)
- Data will be reported using descriptive statistics
- Age ≥18 years
- Confirmed diagnosis of anti-AQP4+ NMOSD
-
Receipt of treatment with ALXN-C5IT (≥1 dose) according to approved local prescribing information
- Eculizumab within the past 4 weeks OR
- Ravulizumab within the past 12 weeks
-
Available historical data
- ALXN-C5IT dosing information since initiation
- Number and types of relapses from 1 year prior to ALXN-C5IT initiation through registry enrollment
- Current enrollment or participation in an interventional clinical study for the treatment of anti-AQP4+ NMOSD in which the intervention is a drug
Figure 1. Countries taking part in the registry
Figure 2. Study design and data collection

Accuracy of Clinical Assessments with Virtual Care in an Outpatient Neurological Setting

Introduction
Virtual neurological assessments were particularly useful and increasingly used during the COVID-19 pandemic.1,2 Neurological assessments may be limited when the physical examination is not performed in person.
Objectives
To analyze the accuracy of video and telephone consultations in the setting of an outpatient neurology clinic when compared to in person assessments.
Methods
Clinical records were reviewed retrospectively at Sunnybrook Health Sciences Centre in a general neurology outpatient clinic, with predominantly MS patients (See Table 1) from March 23rd 2020 to March 23rd 2021 during the peak of the COVID-19 pandemic
1036 patients were analyzed with an initial virtual assessment and subsequently in person when COVID-19 restrictions were lifted or when patients were brought in on an urgent basis
“Clinical disparities (DISP)” were defined as:
(a) patients reporting progression virtually, but found no significant changes on exam with an alternative explanation for complaints
(b) patients reporting stable virtually, but found significant changes on in person exam
“Clarified” was defined as in person exam confirmed virtual reported findings and helped to clarify management
1036 patients were analyzed with an initial virtual assessment and subsequently in person when COVID-19 restrictions were lifted or when patients were brought in on an urgent basis
“Clinical disparities (DISP)” were defined as:
(a) patients reporting progression virtually, but found no significant changes on exam with an alternative explanation for complaints
(b) patients reporting stable virtually, but found significant changes on in person exam
“Clarified” was defined as in person exam confirmed virtual reported findings and helped to clarify management
| Neurological Disease | % with Disease (N=1036) | % DISP Among Patients with Disease |
| MS | 69.0% (n=715) | 15.5% (n=111) |
| Other Inflammatory | 12.0% (n=124) | 12.1% (n=15) |
| Migraines/Headaches/ Seizures/Epilepsy |
6.27% (n=65) | 1.54% (n=1) |
| Movement | 5.50% (n=57) | 14.0% (n=8) |
| Cognitive | 0.68% (n=7) | 28.6% (n=2) |
| Other | 6.56% (n=68) | 8.82% (n=6) |
Table 1. Prevalence of Neurological Disease in Patient Cohort. The percentage of patients with neurological disease and the percentage of those patients with clinical disparities (DISP)
Results
See Table 1 for pathologies. Of 1036 patients included in this study, 27.8% (n=288) of consultations were with video and 72.2% (n=748) with telephone. A total of 13.8% (n=143) of virtual consultations were considered DISP, specifically 13.5% (n=39) video and 13.9% (n=104) telephone consultations. Of the DISP cases, 2.32% (n=24) of all patients stated they were stable but significant changes were seen with in person exam. 3.38% (n=35) of patients stated they were rapidly deteriorating virtually but were stable in person. In person assessments confirmed 13.0% (n=135) of patients’ worsening symptoms virtually or helped to clarify management decision. See Figure 1.
Figure 1. Flow Chart of neurological virtual assessment outcomes in retrospective study. Patients are categorized into those who used video consultations versus telephone consultations. These consultations are further grouped into clinical disparities (DISP), clarified, and no changes with subsequent in person assessment.
Conclusion
Virtual assessments demonstrate to be helpful for most patients in an outpatient neurological setting during the pandemic in over 85% of cases. However, it should be noted that the in person neurological exam led to a change in clinical opinion in 13.8% of assessments. The importance the neurological exam in person was particularly important in 2.32% of patients who described clinical stability but led to different clinical management plans with significant exam findings not identified virtually, including subtle weaknesses, abnormal reflexes, sensory changes, and non-organic findings.
References
1. Yao, P ., Adam, M., Clark, S., Hsu, H., Stern, M., Sharma, R., Mages, K., Greenwald, P ., & Naik, N. (2022). A scoping review of the unassisted physical exam conducted over synchronous audio-video telemedicine. Systematic Reviews, 11(1), 1–219. https://doi.org/10.1186/s13643-022-02085-1
2. Al Hussona, M., Maher, M., Chan, D., Micieli, J. A., Jain, J. D., Khosravani, H., Izenberg, A., Kassardjian, C. D., & Mitchell, S. B. (2020). The Virtual Neurologic Exam: Instructional Videos and Guidance for the COVID-19 Era. Canadian Journal of Neurological Sciences, 47(5), 598–603. https://doi.org/10.1017/cjn.2020.
1. Yao, P ., Adam, M., Clark, S., Hsu, H., Stern, M., Sharma, R., Mages, K., Greenwald, P ., & Naik, N. (2022). A scoping review of the unassisted physical exam conducted over synchronous audio-video telemedicine. Systematic Reviews, 11(1), 1–219. https://doi.org/10.1186/s13643-022-02085-1
2. Al Hussona, M., Maher, M., Chan, D., Micieli, J. A., Jain, J. D., Khosravani, H., Izenberg, A., Kassardjian, C. D., & Mitchell, S. B. (2020). The Virtual Neurologic Exam: Instructional Videos and Guidance for the COVID-19 Era. Canadian Journal of Neurological Sciences, 47(5), 598–603. https://doi.org/10.1017/cjn.2020.
Intravenous immunoglobulin use for central nervous system disorders in British Columbia: implementation of a provincial screening program
Introduction
Intravenous Immunoglobulin (IVIg) use for Central Nervous System (CNS) conditions has increased over the last decade. In many CNS disorders, robust evidence for IVIg efficacy is still lacking. Building on the success of the British Columbia (BC) Neuromuscular IVIg utilization initiative, Guidelines for IVIg use in CNS conditions were developed. A provincial screening program was launched in 2023.
Immunoglobulin (Ig) use has continually increased year over year in British Columbia (BC) with Neurology now accounting for ~40% of all Ig use in the province (left panel). Peripheral Nervous System (PNS) still accounts for the majority of Ig use but the number of patients receiving Ig for CNS conditions has increased significantly since 2014 (right panel).
Screening Process

Condition Classification

Results
Conclusion
- IVIg may be effective in the management of some CNS inflammatory conditions
- A physician-led utilization program with targeted education to ordering physicians promotes best practice
- In over 50% of cases reviewed, alteration of IVIg dose was recommended, illustrating the potential impact of screening programs to optimize the judicious use of this limited resource
- lessons learned from the pilot screening program will inform future versions of provincial guidelines and the screening process


Spontaneous Regression of Acoustic Schwannomas: A Predictive Model
BACKGROUND
Vestibular schwannoma are benign nerve sheath tumours that arise from the vestibulocochlear nerve within the internal auditory canal (IAC) and extend into the cerebellopontine angle (CPA), where they can cause worsening clinical presentation. It is the most common tumour of the CPA with an annual incidence of 17.4/1 million. They typically demonstrate slow growth over time and as such, a reasonable approach to management of these tumours is observation. A portion of these tumours remain static and approximately 5-10% of these tumours will demonstrate spontaneous regression without intervention while under observation, including those associated with neurofibromatosis type-2. The standard treatment is surgical resection followed by radiation for residual tumour or reoccurrence, however, management recommendations encourage tailoring of care to each patient and tumour individually.
Several previous case series have attempted to create predictive models both of tumour growth and regression, but few have reached statistical significance or demonstrated reproducible findings. If factors were identified that could predict tumour growth, one could identify those who will require intervention at an earlier stage of the disease. One meta-analysis conducted on tumours that demonstrated growth identified that size at diagnosis was the only predictive factor that reached significance. In a similar vein, defining factors that reliably predicted patients who would experience spontaneous regression could prevent future patients from undergoing unnecessarily aggressive interventions. As per our review of the literature, no patient characteristics have yet predicted spontaneous regression to date. Imaging characteristics including a festooned aspect of the tumour and the presence of cerebrospinal fluid in the IAC have been identified as predictive for tumour regression in small case series (N=13-14).
METHODS
Using a clinical database of acoustic schwannomas treated by one team at our institution, we identified approximately 40 patients who have demonstrated significant spontaneous regression or complete resolution of their acoustic schwannoma. All patients recieved a survey by mail and were contacted by telephone to complete the survey. For all patients who consented to participate, radiographic and clincal data was collected from patient charts in addition to survey responses. Medical comorbidities and medications were provided through patient questionairre and cooroberated with patient charts. Tumour volume was approximated using the formula V=4/3*pi*length/2*width/2*height/2. A nominal logistic regression was completed using JMP v17, with 50% tumour reduction set as the reference value.
RESULTS
12 patients returned the survey. Two patients returned the questionnaire without the consent form and were therefor excluded. 10 patients were included in the final descriptive summary of this patient population. Tumours were generally small, L-sided (8/10), with a fungated shape (6/10), and at least partial preservation of CSF in the IAC (8/10). Significant decreases in tumour volume were used to identify and include patients in the study, however, no patient factors or radiographic factors appeared to predict the degree of tumour regression.
Vestibular schwannoma are benign nerve sheath tumours that arise from the vestibulocochlear nerve within the internal auditory canal (IAC) and extend into the cerebellopontine angle (CPA), where they can cause worsening clinical presentation. It is the most common tumour of the CPA with an annual incidence of 17.4/1 million. They typically demonstrate slow growth over time and as such, a reasonable approach to management of these tumours is observation. A portion of these tumours remain static and approximately 5-10% of these tumours will demonstrate spontaneous regression without intervention while under observation, including those associated with neurofibromatosis type-2. The standard treatment is surgical resection followed by radiation for residual tumour or reoccurrence, however, management recommendations encourage tailoring of care to each patient and tumour individually.
Several previous case series have attempted to create predictive models both of tumour growth and regression, but few have reached statistical significance or demonstrated reproducible findings. If factors were identified that could predict tumour growth, one could identify those who will require intervention at an earlier stage of the disease. One meta-analysis conducted on tumours that demonstrated growth identified that size at diagnosis was the only predictive factor that reached significance. In a similar vein, defining factors that reliably predicted patients who would experience spontaneous regression could prevent future patients from undergoing unnecessarily aggressive interventions. As per our review of the literature, no patient characteristics have yet predicted spontaneous regression to date. Imaging characteristics including a festooned aspect of the tumour and the presence of cerebrospinal fluid in the IAC have been identified as predictive for tumour regression in small case series (N=13-14).
METHODS
Using a clinical database of acoustic schwannomas treated by one team at our institution, we identified approximately 40 patients who have demonstrated significant spontaneous regression or complete resolution of their acoustic schwannoma. All patients recieved a survey by mail and were contacted by telephone to complete the survey. For all patients who consented to participate, radiographic and clincal data was collected from patient charts in addition to survey responses. Medical comorbidities and medications were provided through patient questionairre and cooroberated with patient charts. Tumour volume was approximated using the formula V=4/3*pi*length/2*width/2*height/2. A nominal logistic regression was completed using JMP v17, with 50% tumour reduction set as the reference value.
RESULTS
12 patients returned the survey. Two patients returned the questionnaire without the consent form and were therefor excluded. 10 patients were included in the final descriptive summary of this patient population. Tumours were generally small, L-sided (8/10), with a fungated shape (6/10), and at least partial preservation of CSF in the IAC (8/10). Significant decreases in tumour volume were used to identify and include patients in the study, however, no patient factors or radiographic factors appeared to predict the degree of tumour regression.
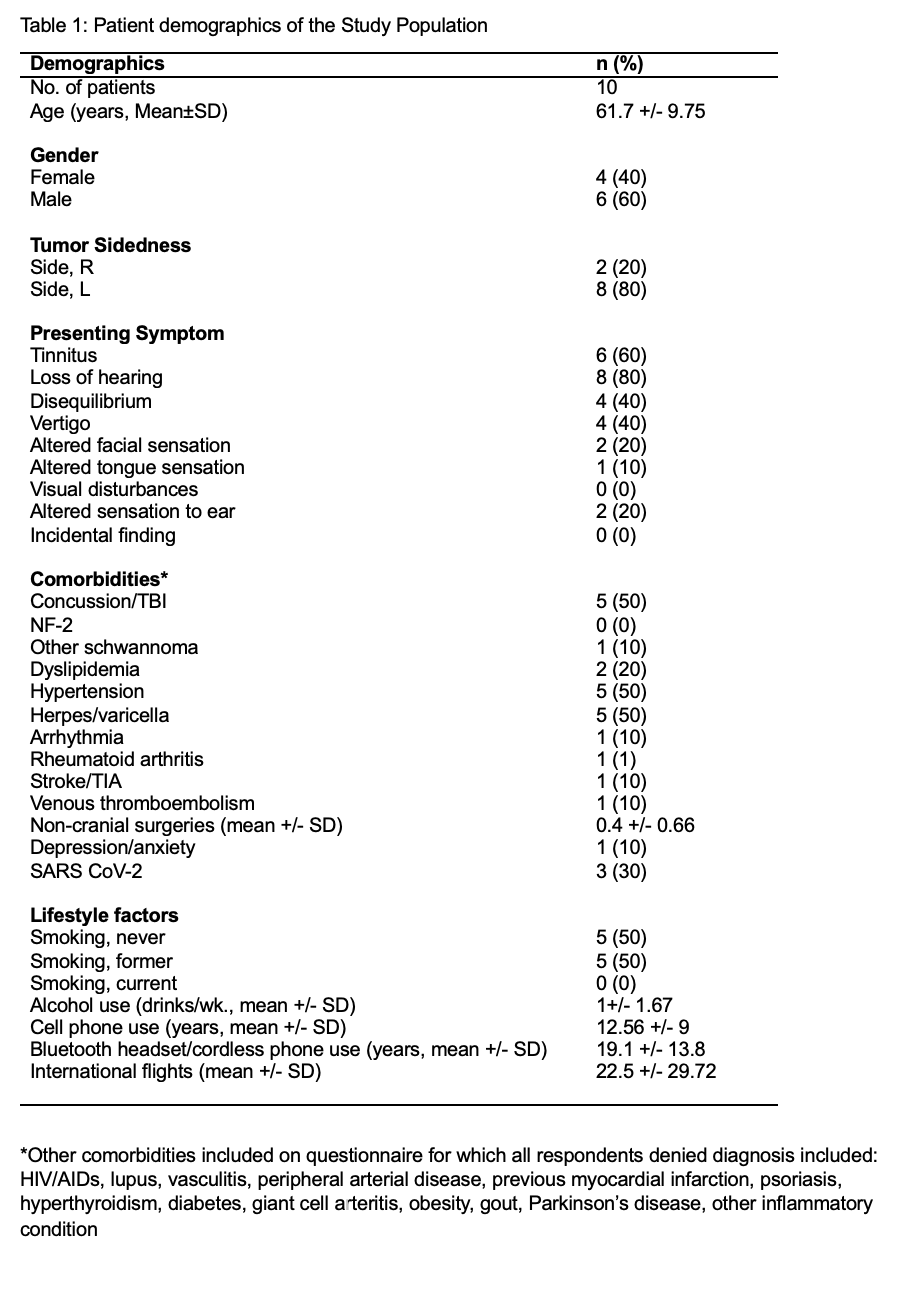
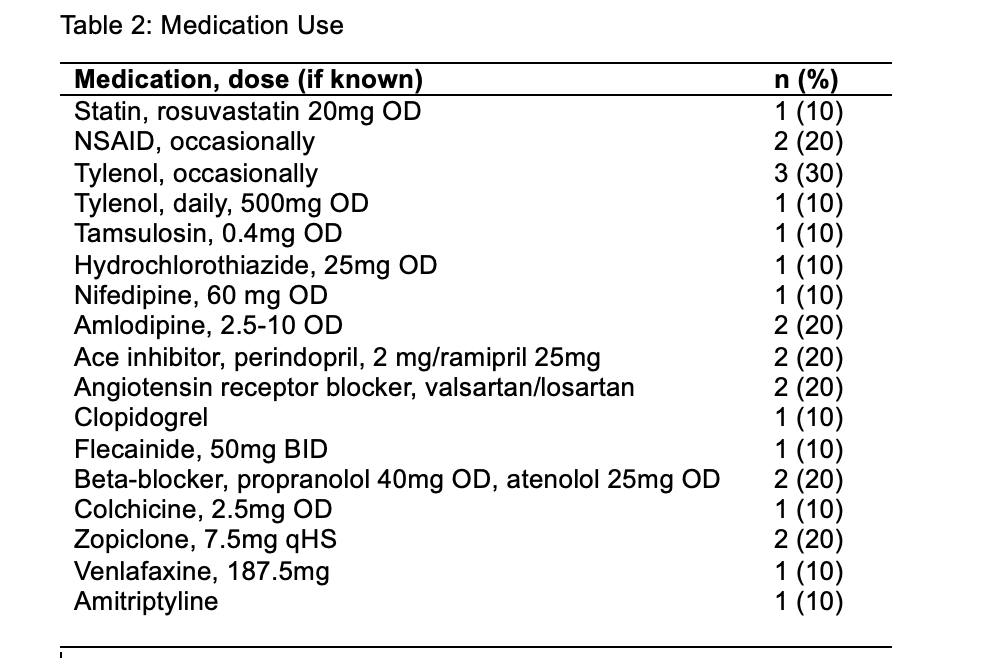
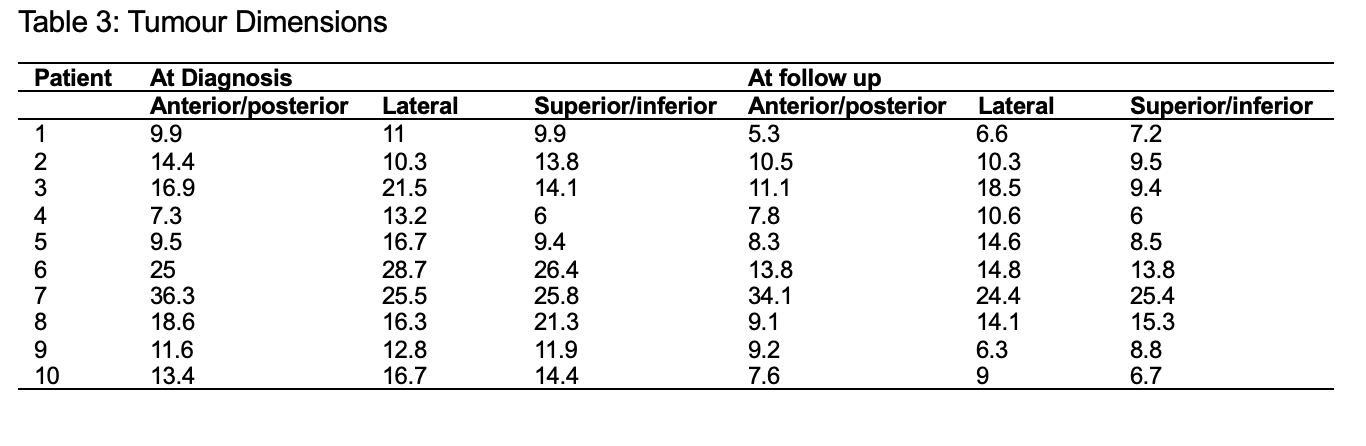
Figure 1: Tumour Volume at diagnosis vs latest follow-up
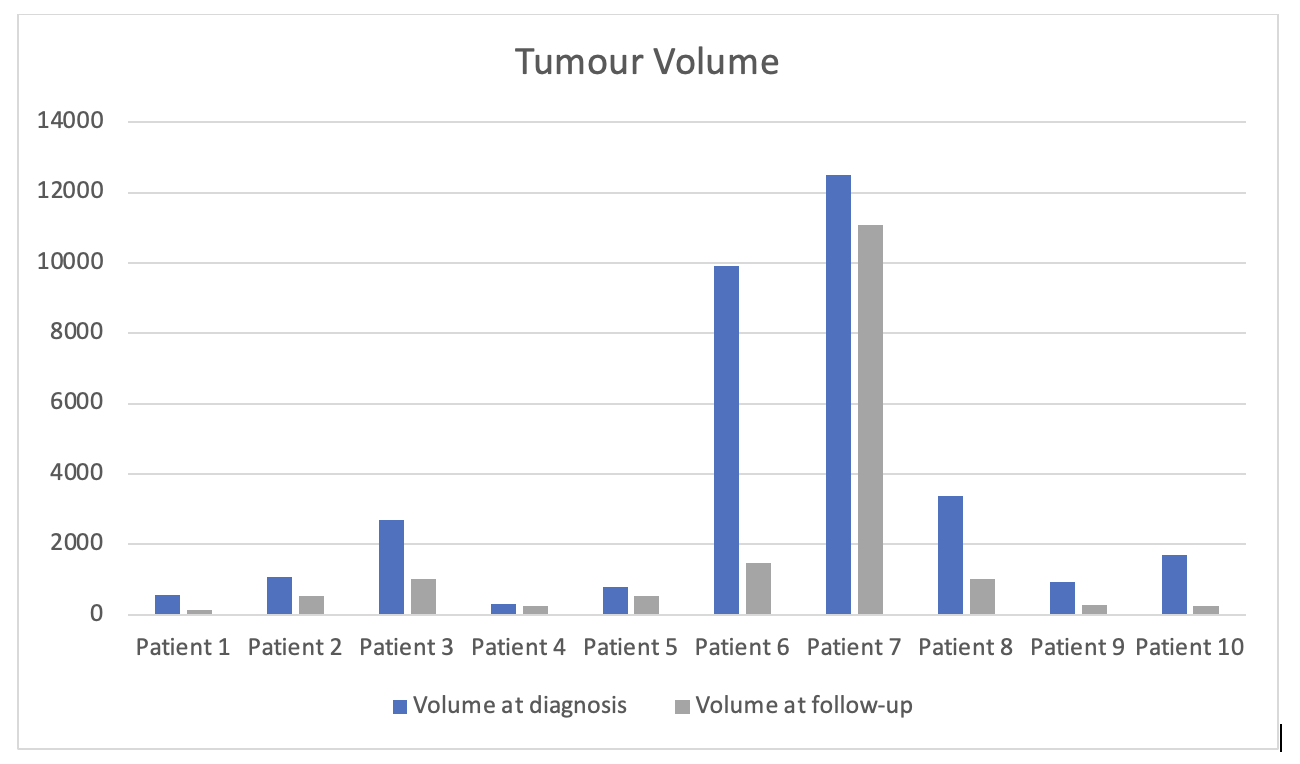
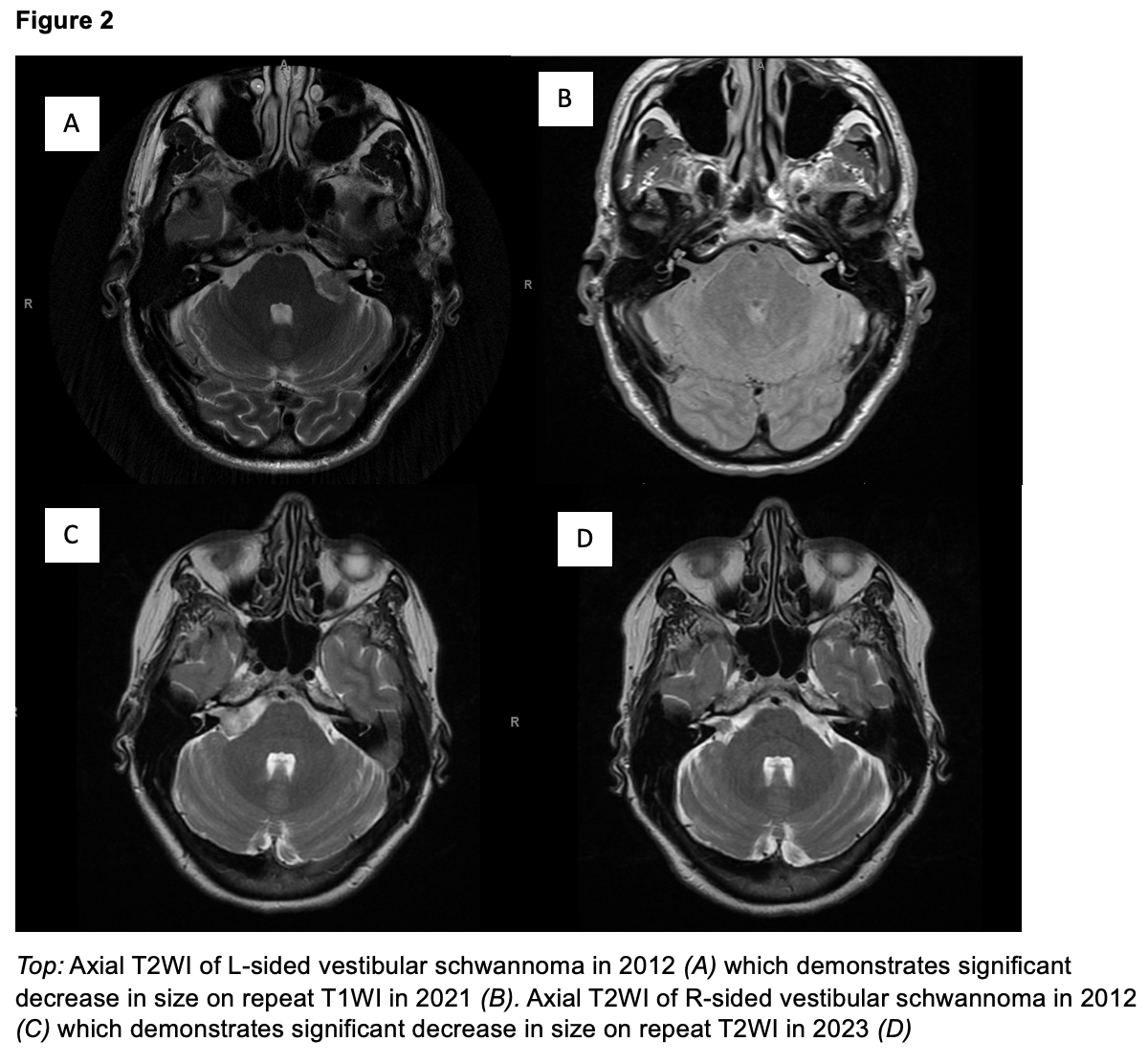
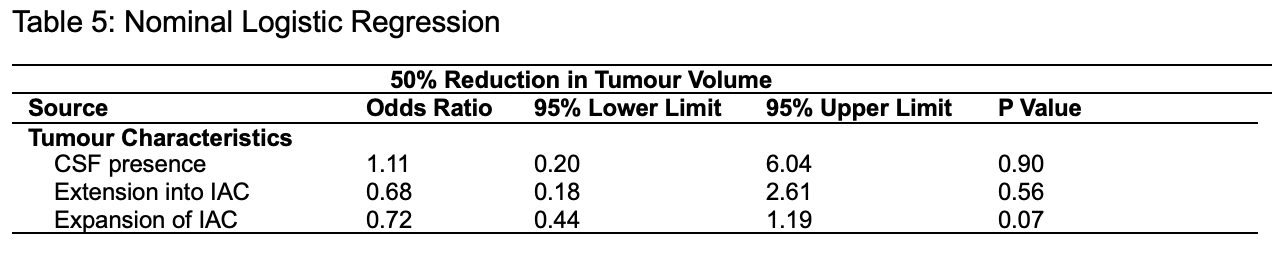
CONCLUSION
In conclusion, this is the first study to summarize patient lifestyle factors obtained through patient survey in addition to clinical and radiographic factors to describe spontaneous regression of acoustic schwannoma. No obvious clinical factors appear to be protective based on this preliminary data. No imaging characteristics, including those previously demonstrated to be predictive, such as CSF preservation in the ICA and ICA extension are predictive in this study. A case-control study including control patients who demonstrated tumour progression should be completed in future.
REFERENCES
Re-norming medical education: centering patient experience and diverse bodies in Lumbar Puncture (LP) instruction

Background
- Health education suffers from a lack of diverse representation both in how it frames expertise and who is physically represented in curricular content
-
Our project aims to address both issues by
- acknowledging patient and student expertise
- demonstrating a common health care procedure (lumbar punctures) across diverse bodies
Methods
- Interviewed patients using trauma-informed methods
- Captured Lumbar Puncture instructional videos with diverse standardized patients
- Invited Biomedical Communications students to paint spinous processes on the backs of patients
- Compiled patient stories, videos, and images into a teaching module
Patients as Experts
We interviewed five (5) stroke patients and their families to understand the patient experience of lumbar punctures. Patients are experts in how they experience health care and interactions with health care practitioners. From their stories, we learned valuable lessons on how LPs can be done in a more patient-centred way.
Communication is key
“So verbal communication when you're doing it is definitely a way to put patients at ease…. You know those kind of reassuring things are very important to the patient.”
– Sandy, LP Patient
Know when to seek help
“This is years later, so it just strikes me as as it's it is really important that if you can't get it right right away, don't try and force the issue right…. Either try something a little bit different, or get someone to help and maybe tell the person that's laying on the table.”
– Jim, LP Patient
Show confidence
“as she told me about the procedure that was going to happen and all the stuff she do it was every time she'd say something she's gonna do she said we'll try to do it or I should be able to do this and so the more she said that the more it like freaked me out it's so it's like why is she saying she should be able to do it umm so words matter in terms of how it's specifically attended to”
- Bailey, LP patient
Difference as the "norm"
We developed an LP teaching module that featured 9 Standardized Patients of different body size, genders, ages, and skin colours in an attempt to demonstrate how different bodies require different considerations when performing a lumbar puncture.
The module consists of instructional videos and images of spinous processes painted across 9 different standardized patients in order to demonstrate the different approaches to an LP and the difference in anatomical structures. (Click to move through image slideshow.)





Conclusion
- Patients need to be at the centre of health education and health care.
- By centring patient experiences and integrating diverse bodies, we are hoping to empower medical students to become more inclusive and effective doctors.
Ischemic stroke in young adults: a comparison of outcomes, stroke risk factors and etiologies between males and females

Introduction and purpose
- Few studies have explored sex differences in functional outcomes after ischemic stroke in young adults.
- The primary aim was to determine if functional outcomes among young adults with stroke differed based on sex.
- The secondary aim was to identify differences in stroke risk factors and etiologies between females and males.
Methods
- We conducted a retrospective analysis of consecutive acute ischemic stroke patients aged 18 to 55 years from a single centre stroke registry between 2018 to 2022.
- Using multivariable logistic regression, we analysed if modified Rankin Scale at 3-6 months (mRS, dichotomized 0-2 versus 3-6) was associated with sex.
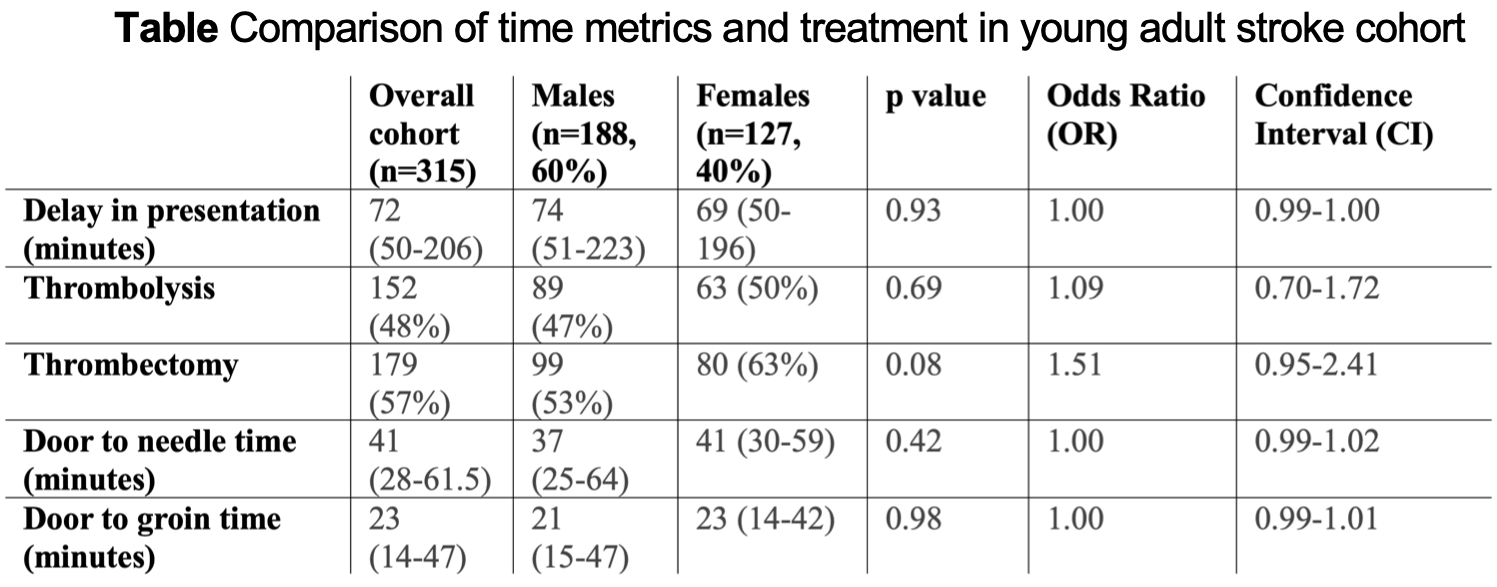
Results
- We included 315 patients (127 female) with a median age of 48 years (IQR 42-52), median NIHSS of 10 (IQR 4-19) and median mRS (at 3-6 months) of 2 (IQR 1-3).
- Following adjustment for vascular risk factors, clinical stroke characteristics, baseline mRS, thrombolysis, stroke time metrics and unknown onset of symptoms, there was no significant difference in mRS (3-6 months) based on sex (p=0.40).
- Atrial fibrillation (p=0.01) and toxic drug use (p=0.001) were more frequent in males.
- Thrombolysis, thrombectomy and mortality rates were similar in both groups.
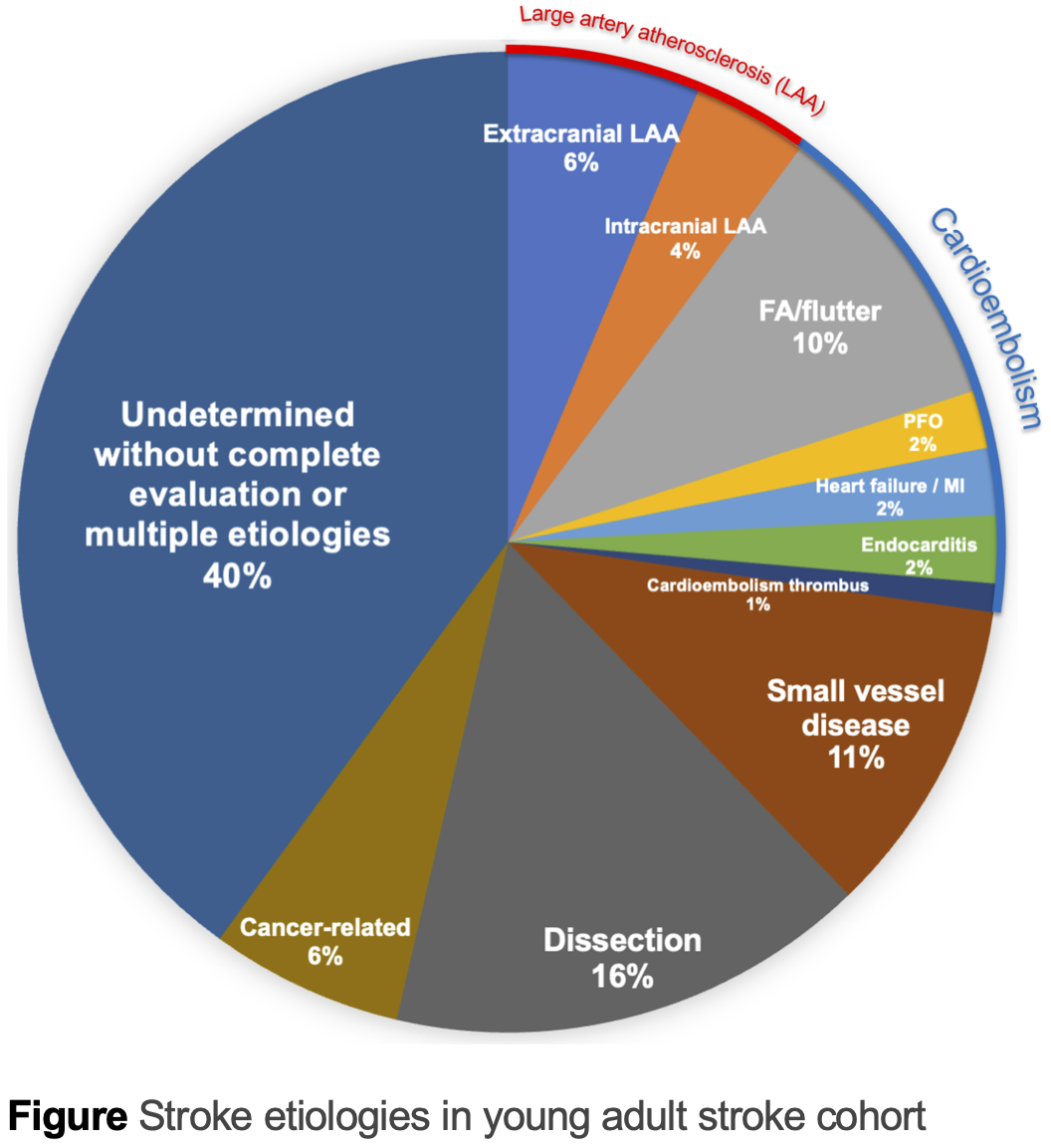
Conclusions
- Patient-oriented outcomes may be of interest in future studies as functional outcomes based on mRS do not differ between young male and female stroke patients.
- Males had a higher prevalence of risk factors including toxic drug use and atrial fibrillation.
- These findings could help develop targeted stroke prevention strategies in young adult stroke patients.

A shared decision-model toolkit for pregnancy related care in neurology
BACKGROUND
- Many patients feel they are not empowered to make independent medical decisions.1
- Women have demonstrated difficulty discussing reproductive and pregnancy-related health choices with medical practitioners.2
- The development of decision aids have greatly empowered women in making their own medical decisions by facilitating collaborative decision making in obstetrics and gynecology.3
- Webtool-based decision aids have shown efficacy in promoting shared decision making and collaborative care in these groups, but are limited to family planning, prenatal screening, and cancer management.3
- No current decision aid in the literature exists to promote shared decision-making on pharmacological pregnancy-related care.
PURPOSE
The Neurology and Pregnancy Web Tool is a guided platform designed to enable real-time shared decision-making.
- It allows the confluence of data sources, patients, and physicians to meet.
- It was developed over 2 years in collaboration between pharmacy and clinical neurology experts at the University of Waterloo and University of Toronto.
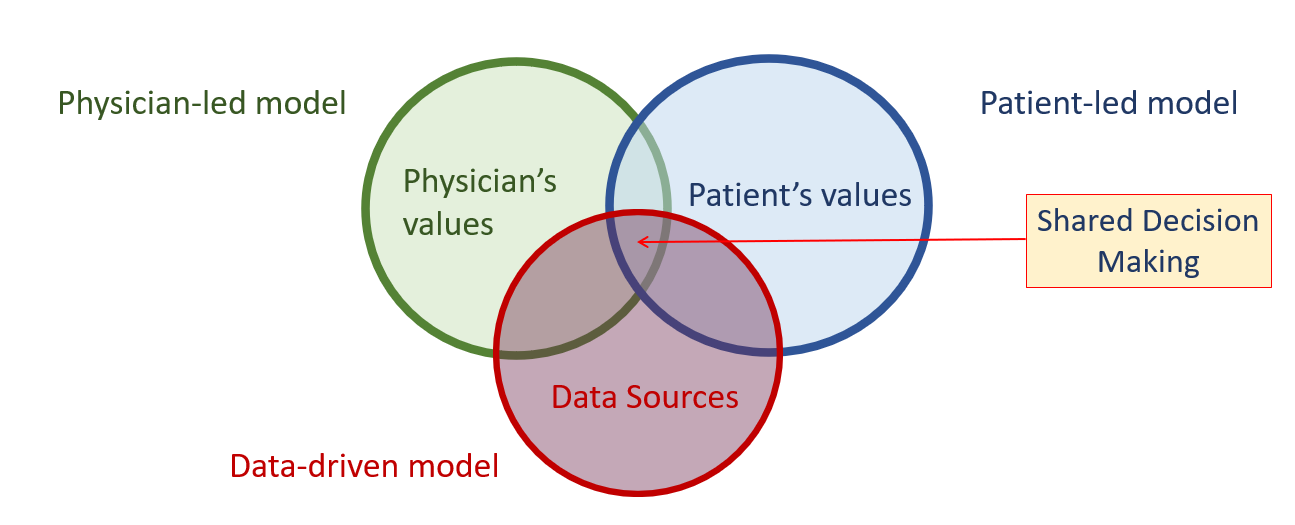
Figure 1: Illustration of Pregnancy Web tool usage in supporting Shared Decision Making
STUDY DESIGN AND METHODS
- A mixed-methods quality improvement study was used to collect patient feedback on the usability and appropriateness of a webtool focused on common issues faced by pregnant patients with chronic neurological conditions.
-
Recruited participants were asked to rate the web tool according to the Systems Usability Score (SUS), Acceptability of Intervention Measure (AIM), and Intervention Appropriateness Measure (IAM).
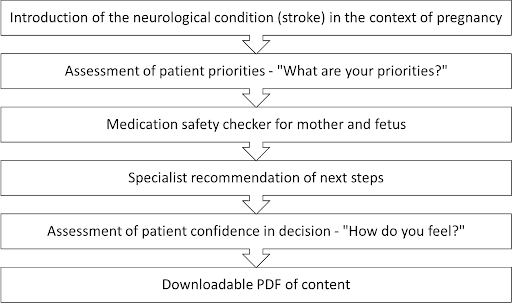
Figure 2: Web Tool Development Flow - "How safe are Blood Thinners for my Pregnancy?"
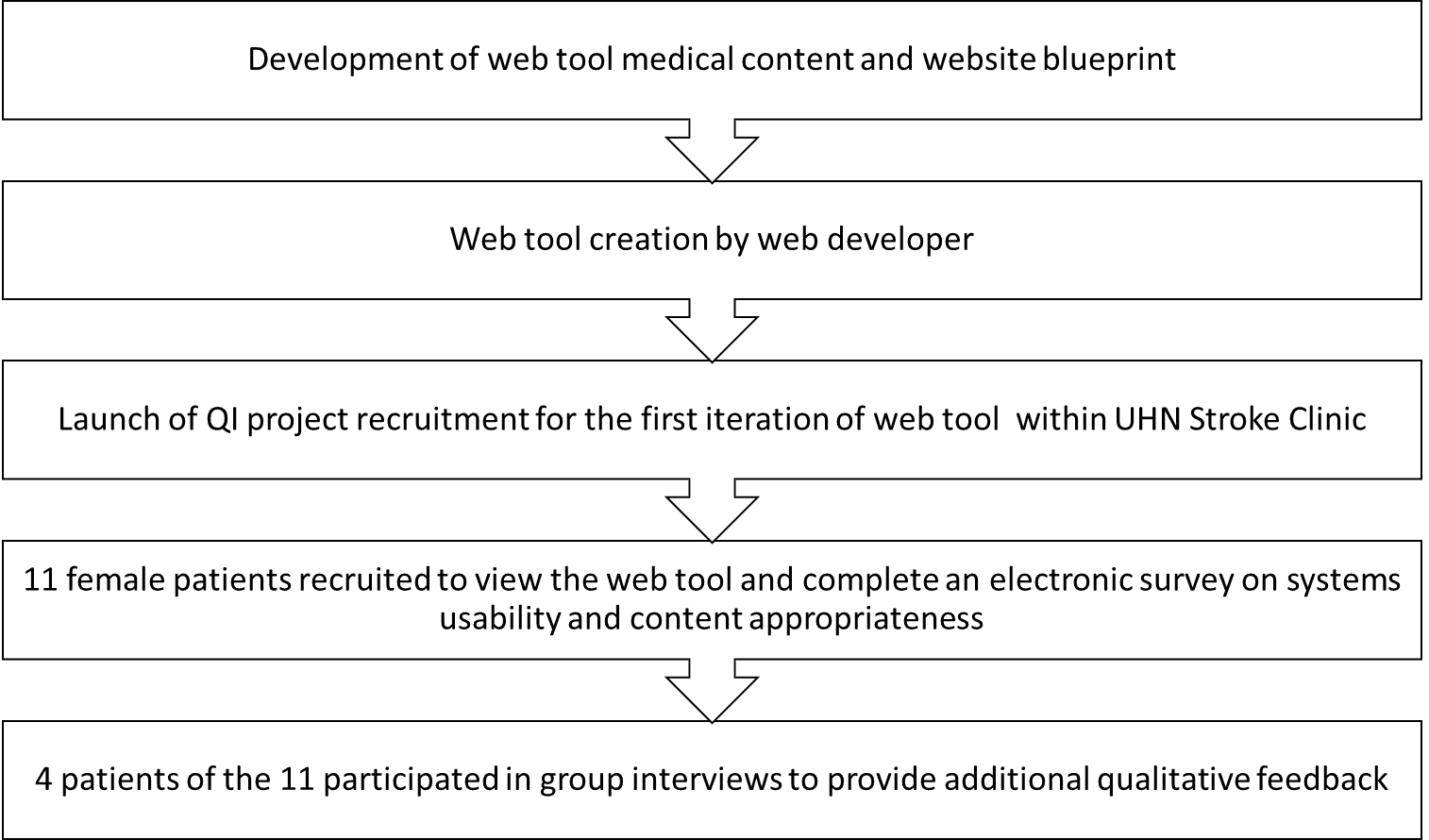
Figure 3: Study design workflow and web tool assessment by participants through electronic survey and focus groups
RESULTS
| Age (years) | 31-40 | 51-60 | 60+ | ALL (Range) |
|---|---|---|---|---|
| Count | 5 | 5 | 1 | 11 |
| Average Time spent on Web Tool (min) | 8 | 20 | N/A | 15 (5-20) |
| Average Systems Usability Score | 67 | 66 | N/A | 66.1 (42.5-90) |
Table 1: Demographic characteristics, device usage types, and rated usability scores of recruited participants
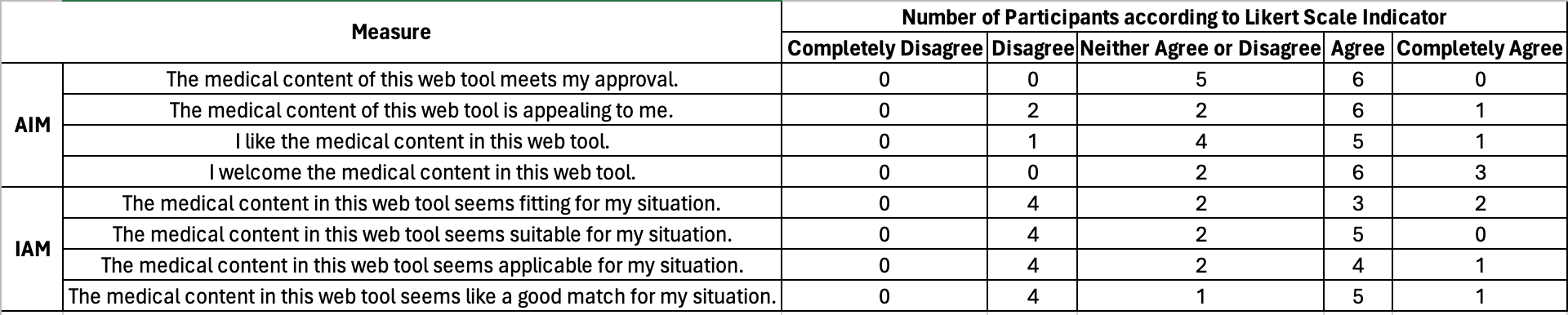
Table 2: Participant Counts according to AIM and IAM rating tools
Focus Group Thematic Results:
- Suitability and usability of the tool depends on inherent user access to healthcare and geographic resources
- Comprehension of webtool content is dependent on lived experience with the medical condition.
- User interface dictates how well users can comprehend the tool.
CONCLUSIONS AND FUTURE DIRECTIONS
- Our study demonstrates a proof of concept of a method of analysis that can be used for further refinement.
- No other similar framework currently exists within the current scope of the literature and highlights the need for future tools.
- Our study recruited patients from tertiary academic centres, further refinement of the tool would benefit from patient perspectives from more low-resourced areas.
Shifts in Daytime Functioning Items on the Insomnia Severity Scale With Lemborexant After 6 Months of Treatment
Introduction
- The presence of daytime impairments, such as reduced functioning, decreased energy, and/or fatigue, is one of the characteristics of insomnia disorder.1
- An efficacious insomnia treatment ideally should improve subject-reported disease severity, as assessed by the Insomnia Severity Index (ISI), a 7-item self-reported questionnaire. Four of the 7 items specifically assess severity of daytime functional impairments.2
- Lemborexant (LEM) is a competitive dual orexin receptor antagonist approved in multiple countries for the treatment of adults with insomnia.3,4
-
In Study E2006-G000-303 (Study 303; SUNRISE-2; NCT02952820), the ISI total score, and items 4-7 for daytime function, led to larger and statistically significant (improvement) changes from baseline with LEM treatment compared with placebo (PBO) as assessed at 1, 3, and 6 months.5
- Improvements with LEM treatment continued through 12 months.5
Objective
To assess the impact of LEM based on the level of severity of the daytime function items of the ISI in Study 303, this post-hoc analysis examined the impact of LEM compared with PBO on shifts in these items (improvements from very severe towards no problem) over 6 months, depending on baseline severity.
Methods
- Study 303 was a 12-month, phase 3, global, multicenter, randomized, PBO-controlled (for first 6 months), double-blind, 2-dose, parallel-group study in males and females (≥18 years of age) with insomnia disorder (Figure 1).6
- Additional details regarding study design, inclusion/exclusion criteria, the ISI (Table 1 - see full poster via QR code), and statistical analysis are included in the full poster.
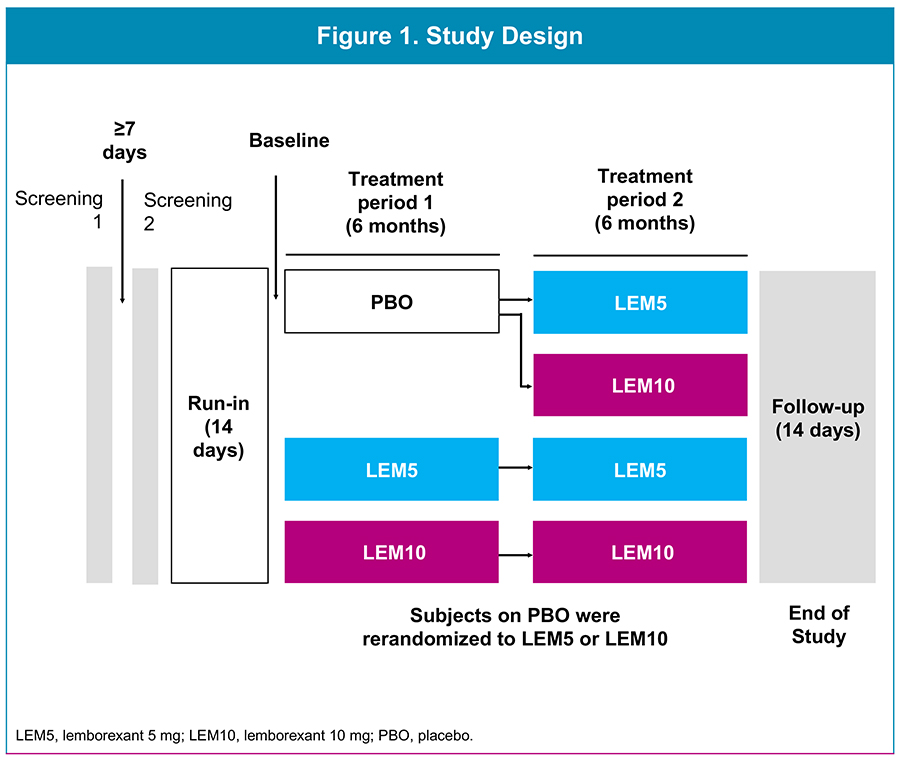
Results
Demographic Data
- Baseline demographic characteristics, including baseline ISI total score and DFS, were similar across treatment groups (Table 2).
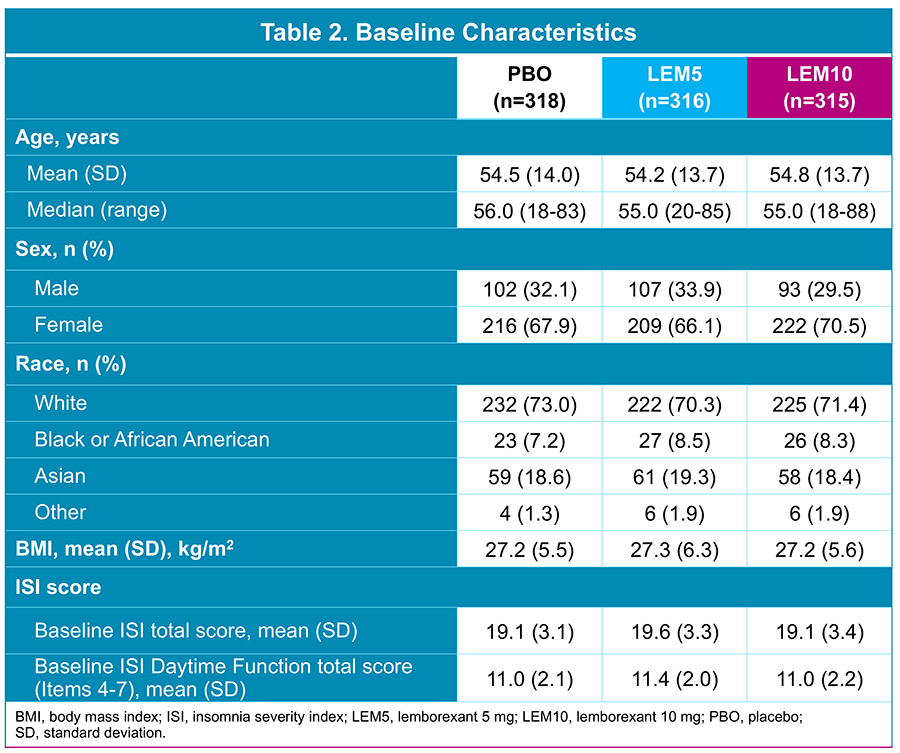
Shifts in ISI Daytime Function Items
- 749 of 949 (78.9%) subjects completed the ISI both at baseline and at the end of Treatment Period 1: PBO, n=258/318 (81.1%); LEM5, n=257/316 (81.3%); LEM10, n=234/315 (74.3%).
- Shifts from baseline to Month 6 in total DFS between chosen ranges are shown in Table 3 (see full poster via QR code).
- The shift distributions, improvement from more severe daytime functioning impairment towards no daytime functioning impairment at 6 months, were overall significantly different, favoring both LEM5 (P<0.0001) and LEM10 (P=0.008) compared with PBO.
- A significantly greater proportion of subjects who reported severe-to-very severe problems in daytime functioning at baseline (DFS total score 13-16) showed improvement to lower rates of problems, compared with staying the same, at 6 months with LEM10 compared with PBO (Figure 2).
- A greater proportion of subjects who reported moderate-to-severe problems in daytime functioning at baseline (DFS total score 9-12) showed improvement to lower rates of problems, compared with worsening or staying the same, at 6 months with LEM5 compared with PBO (Figure 3).
- In subjects who reported only mild-to-moderate problems in daytime functioning at baseline (DFS total score 5-8), 39-48% across all treatments reported an improvement at 6 months (Figure 4).
Results

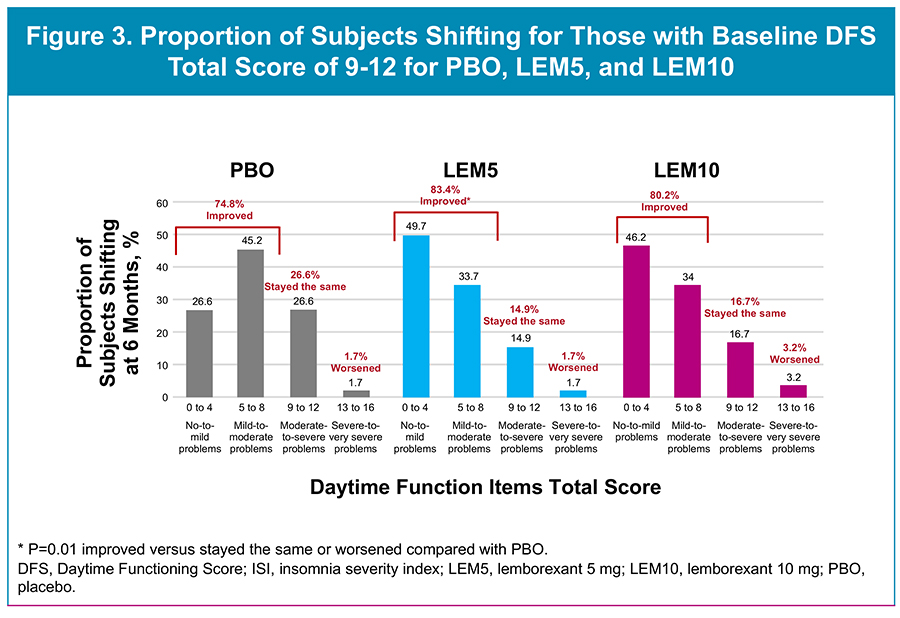
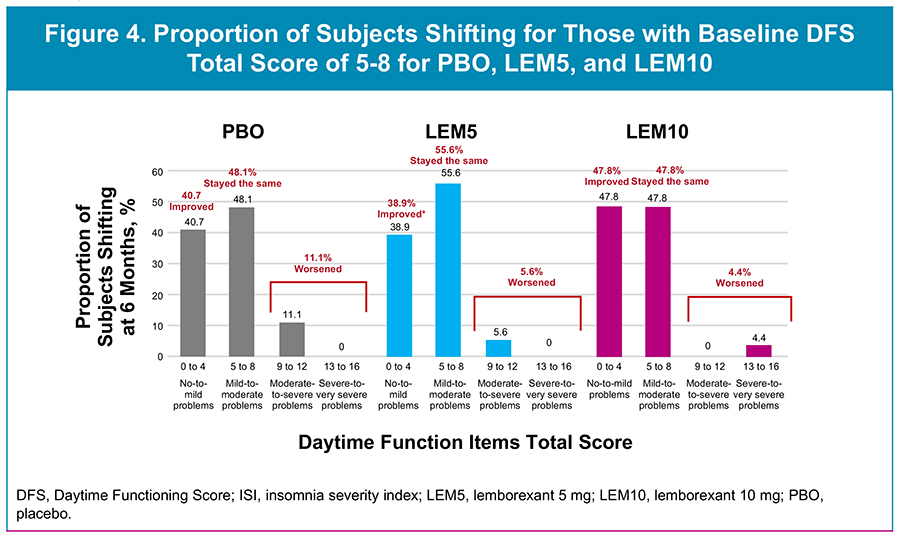
Results
Safety
- LEM was well tolerated; the majority of TEAEs were mild-to-moderate in severity (Table 4).
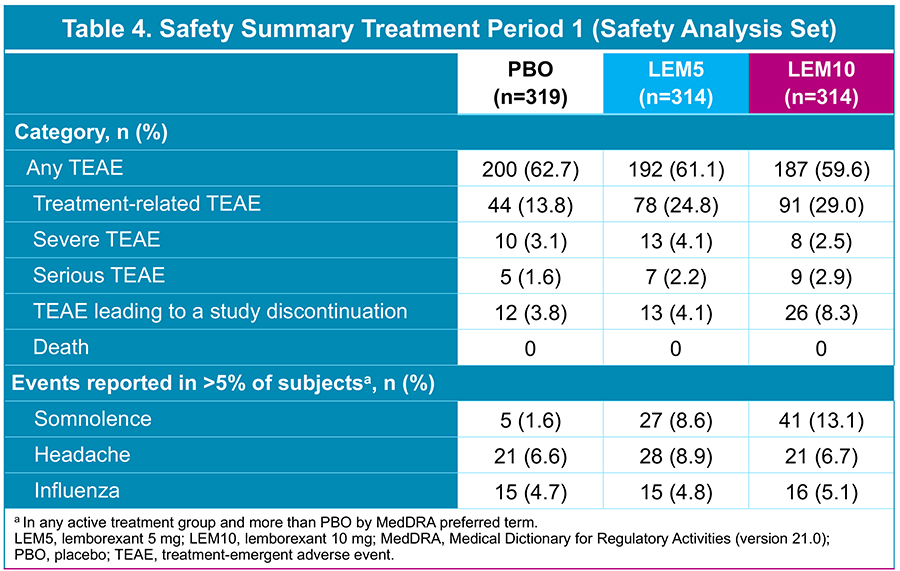
Conclusions
-
More subjects treated with LEM for 6 months were able to improve their daytime functioning, regardless of baseline severity.
- More LEM subjects’ scores moved into lower categories (eg, from reporting severe or very severe problems in daytime functioning to no or mild problems at 6 months) compared with those from subjects receiving PBO.
- In subjects reporting moderate-to-severe or severe-to-very severe problems with daytime functioning at baseline (DFS scores 9-12 or 13-16), there was a notable improvement, with ~40-50% shifting to 0-4 (no or mild problem) at 6 months with LEM treatment compared with ~25-30% for PBO.
- When added to previous findings of improved daytime functioning sustained for 12 months, these data provide further evidence that LEM may be an appropriate treatment option for patients with insomnia who report severe impairments in daytime functioning in addition to their nighttime symptoms.
Please scan the QR code for full poster details.
Nonclinical Studies of Abuse Potential With Dual Orexin-Receptor Antagonists: Concordance With Real-World Use
Introduction
- Insomnia, characterized by problems falling asleep, staying asleep, and/or early awakening, is treated by hypnotic medications with distinct mechanisms of action.1
- Many hypnotic drugs prescribed for insomnia are known to show abuse and/or dependence potential and a withdrawal syndrome; as such, some are classified under Schedule IV (CIV).2,3
-
The 3 dual orexin-receptor antagonists (DORAs; daridorexant, lemborexant [LEM], and suvorexant), members of the newest hypnotic class approved for the treatment of insomnia, were placed in CIV based largely on human abuse potential (HAP) studies,4-8 but have fewer abuse-related events in the community, suggesting a potential overestimation of risk in the HAP studies.9,10
- This conclusion is based on several factors determined in the clinical development programs: Negative nonclinical studies, no off-target binding, low rates of abuse-related treatment-emergent adverse events (AEs) in clinical trials, and a paucity of on-line chat reports recommending DORAs to others for recreational purposes, among other factors.3
- At the time of their approval, there were insufficient postmarketing data from the community for consideration in the scheduling decisions. Currently, >8 years of postmarketing data are available across the 3 approved DORAs.
Objective
- To assess the abuse potential of DORAs, and other drugs used as hypnotics (benzodiazepines [BZs] and zolpidem [ZOL]), using real-world data from publicly available United States (US) and Japanese pharmacovigilance databases and an internal Eisai Global Postmarketing Safety Surveillance System.
Methods
Study Design and Data Sources
- This was an observational retrospective study that compared AEs, including abuse and withdrawal events, and other data such as mentions of misuse across 3 drug categories with distinct mechanisms of action frequently used in the treatment of sleep difficulties: DORAs (LEM, suvorexant, daridorexant), BZs (temazepam, triazolam, estazolam, brotizolam, etizolam, flunitrazepam), and ZOL.
-
Data sources included the US FDA Adverse Event Reporting System (FAERS) database, Japan Adverse Drug Event Reporting (JADER) database, and Eisai's Global Postmarketing Safety Surveillance System (Table 1 - see full poster via QR code).
- FAERS and JADER contain AE reports submitted by healthcare professionals, consumers, and product manufacturers.
- Additional details regarding study design are included in the full poster.
Results
Analysis of FAERS
- Compared with BZs and ZOL, DORAs were associated with the lowest rates of: serious AEs (Table 2), suspected AEs of injury, poisoning, and procedural complications (as a percentage of total reports) (Figure 1), AEs (based on percentage of reports) of drug withdrawal syndrome (Figure 2A), drug abuse (Figure 3A), and drug dependence (Figure 4A).
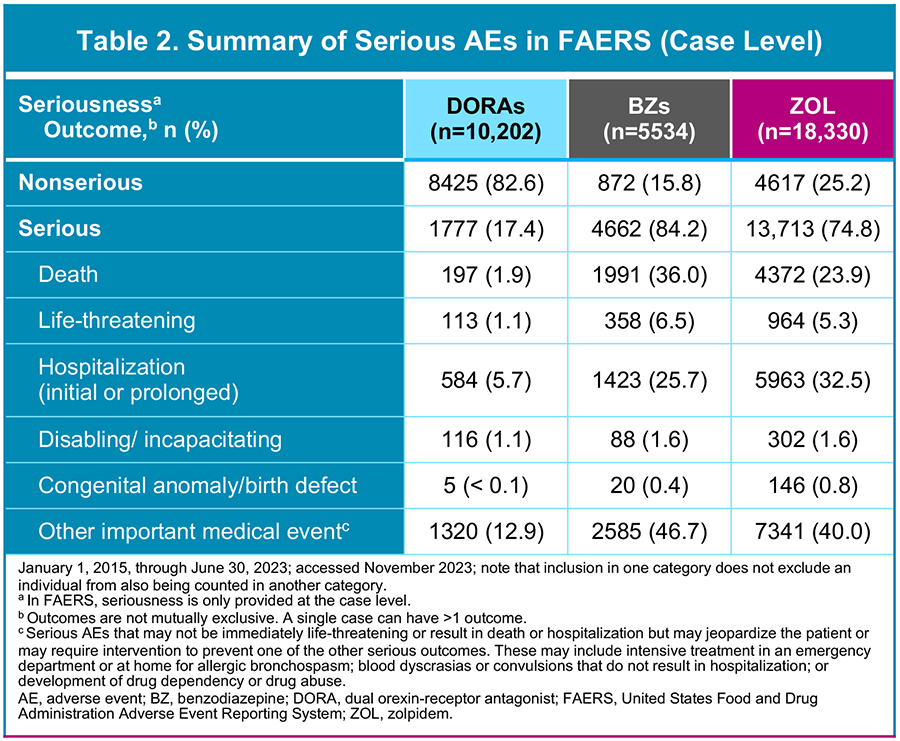
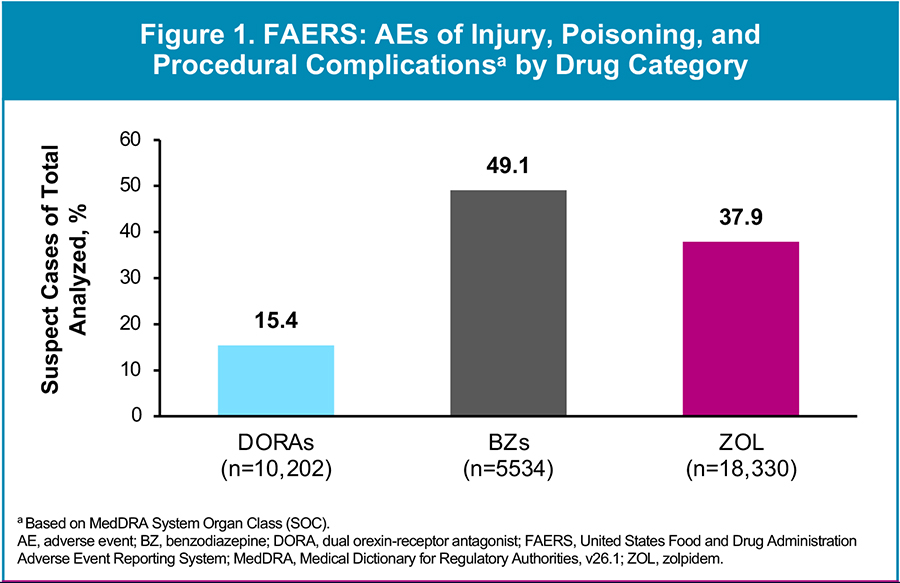
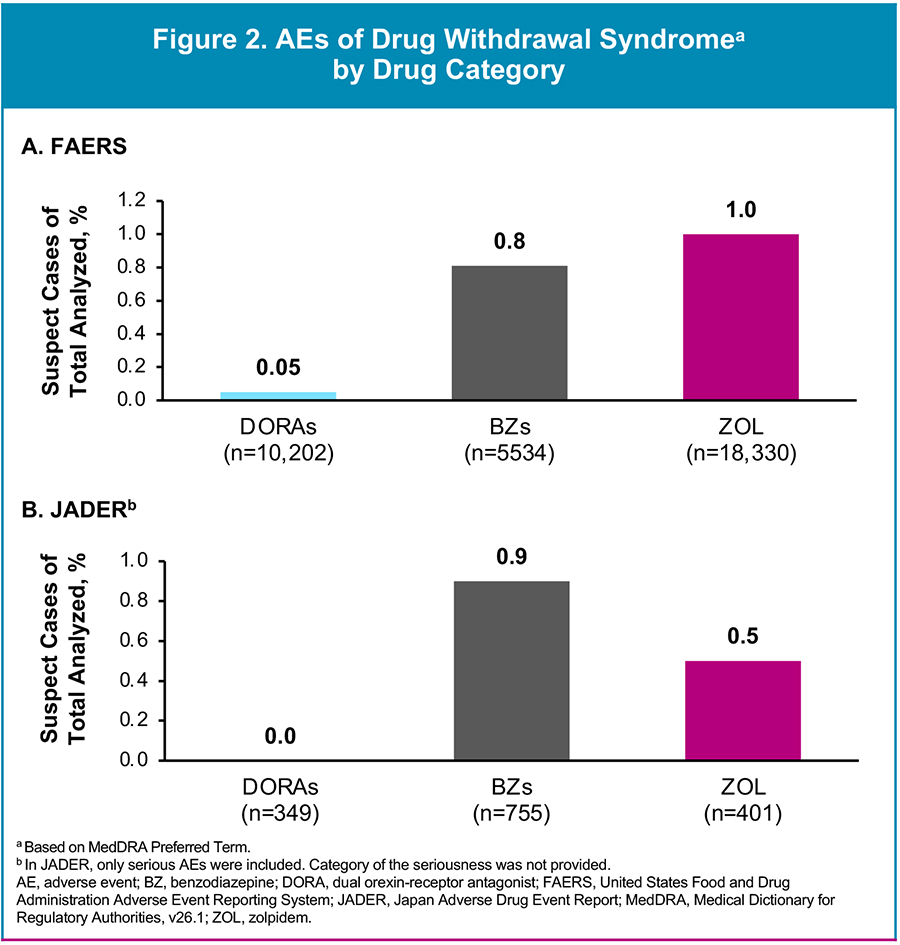
Results
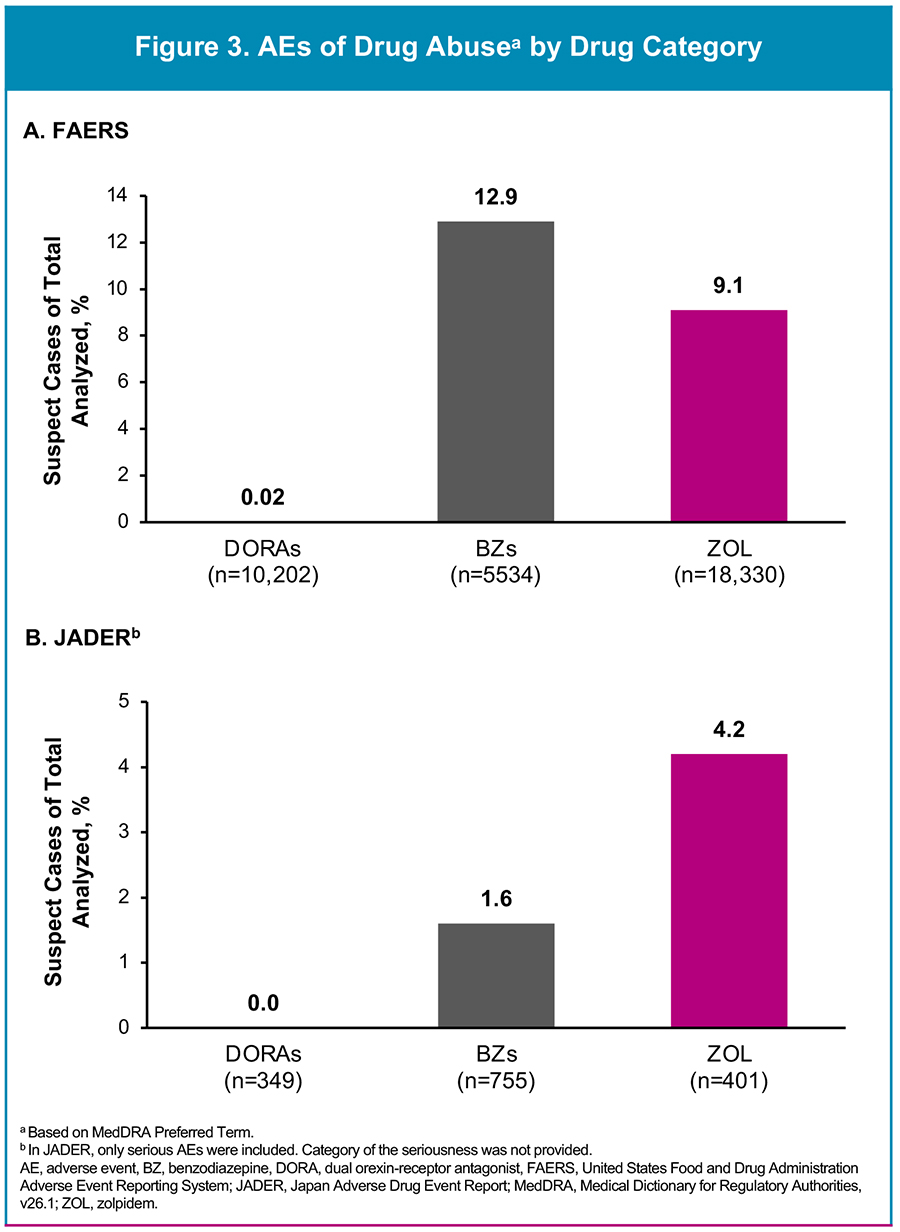
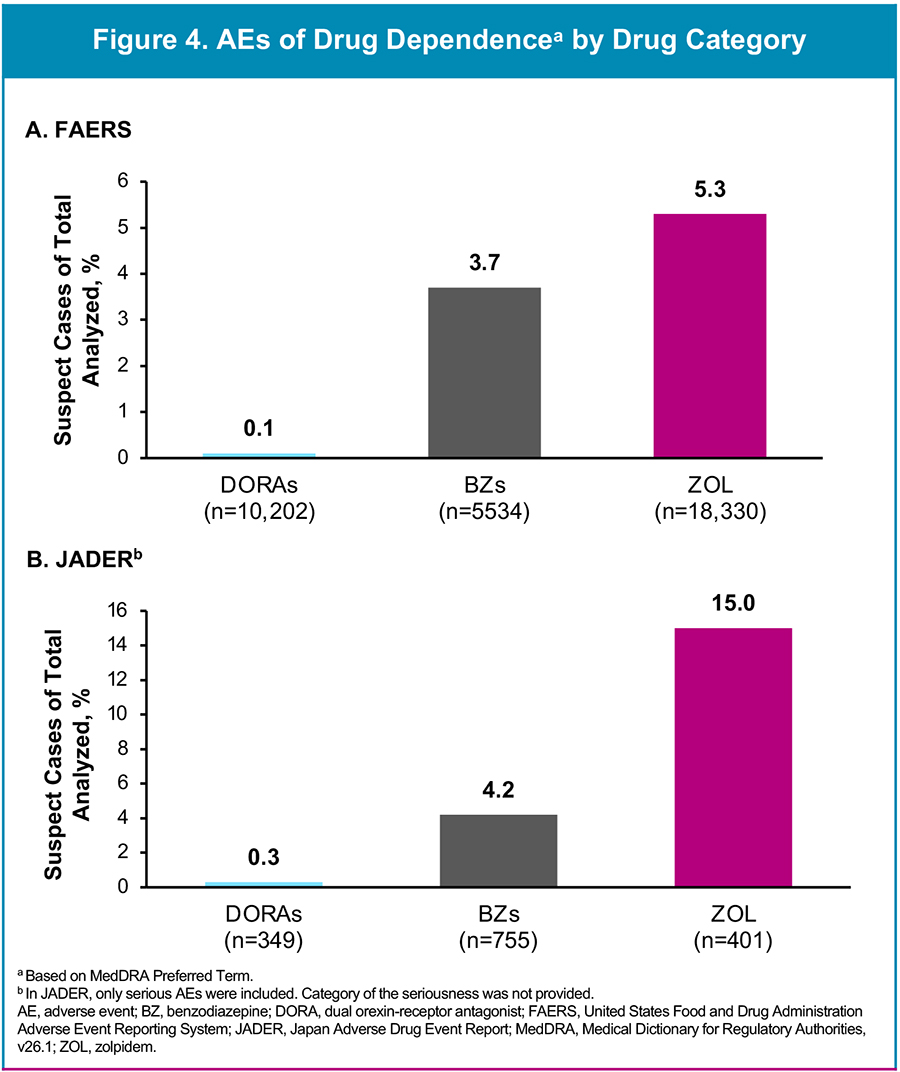
Results
Analysis of JADER
- Compared with BZs and ZOL, DORAs were associated with the lowest rates of: AEs (based on percentage of reports) of drug withdrawal syndrome (Figure 2B), drug abuse (Figure 3B), and drug dependence (Figure 4B).
Analysis of Eisai Global Postmarketing Safety Surveillance System
- Since the time of LEM's marketing approval in 2020, there have been a small number of drug abuse, drug dependence, and drug withdrawal AEs reported to Eisai from the US, Canada, and Japan (Total number of reports, N=73) (Table 3 - see full poster via QR code).
- Given the number of patients exposed postmarketing (~ 475 million patient days), and the number of reports (N=73), the calculated reporting rate corresponds to
~ 0.15 cases per million patient days of global exposure.
Conclusions
- The findings from the FAERS and JADER databases suggest that DORAs have lower real-world abuse compared with BZs and ZOL. In accordance, data from the Eisai Global Postmarketing Safety Surveillance System database also reported low real-world abuse potential with LEM, a DORA.
- The current findings are consistent with low levels of abuse events with DORAs (eg, no reinforcing effects or a withdrawal syndrome) reported in nonclinical and clinical studies3,23,24 and community-based reports from the FDA’s Controlled Substance Staff.9,10 The findings suggest that relying exclusively on HAP studies for scheduling DORAs appears to overestimate their potential for abuse in the community and DORAs may not pose meaningful abuse potential and related risks.
- Providing clinicians with a means to differentiate between classes of hypnotics by re-evaluating the placement of DORAs in CIV appears warranted.
Please scan the QR code to access the full poster.
Gender disparity in canadian institutes of health research funding within neurology
Background
- Despite improved gender representation, women face gender-based barriers in academic medicine, especially in neurology1,2
- In 2019, women accounted for only 36% of neurologists in Canada3
- Evidence suggests that gender disparity persists in the Canadian Institutes of Health Research (CIHR) funding4
Aim: To evaluate gender disparities in CIHR funding decisions for Canadian neurology divisions and departments
Methods
- Data on CIHR grant recipients, duration, quantity, and contribution within Canadian neurology divisions and departments (2008-2022) were collected from the CIHR Funding Decisions Database5
- Gender identity was determined by an application programming interface6
- Analyses conducted by Mann-Whitney U test and Glass rank biserial (rg) correlation test
Outcomes:
- Gender-based differences in CIHR grant prevalence, duration, and contribution amount within neurology
- Subgroup analysis for Canadian licensed neurologists and Project Grant awards
Results
- Of 1604 grants awarded, women received fewer grants (n=665, 42%), less funding by 2.5 times (p<0.0001), and shorter grant durations by 1.5 times (p<0.0001) annually than men
- Women were the minority of recipients (n=542; 45%) and less likely to be awarded grants (p<0.001) annually than men
- Differences were consistent in subgroup analyses
Fig. 1 Gender-stratified frequency (%) of awarded CIHR grants
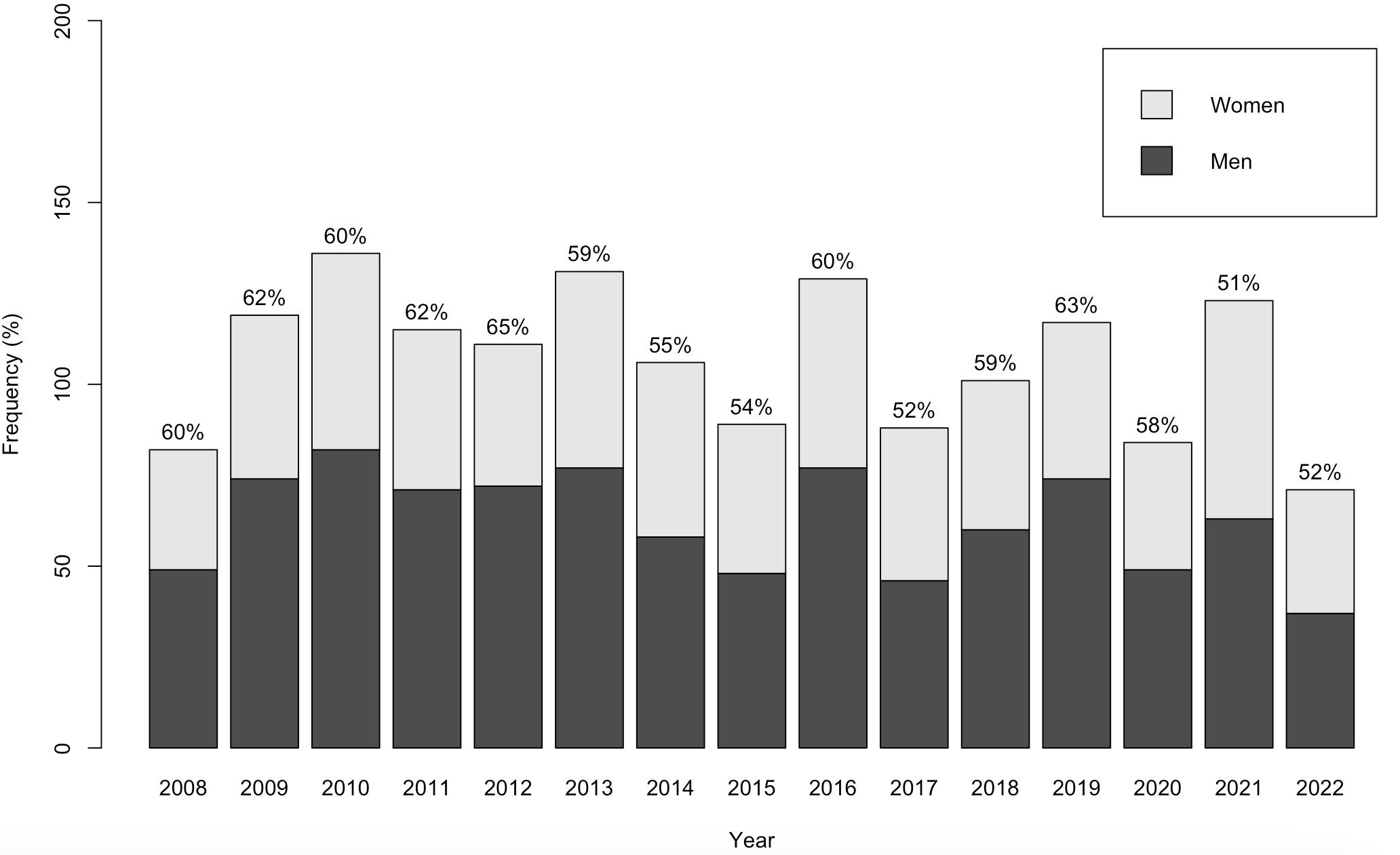
Fig. 2 Gender-stratified frequency of annual CIHR grant total contribution
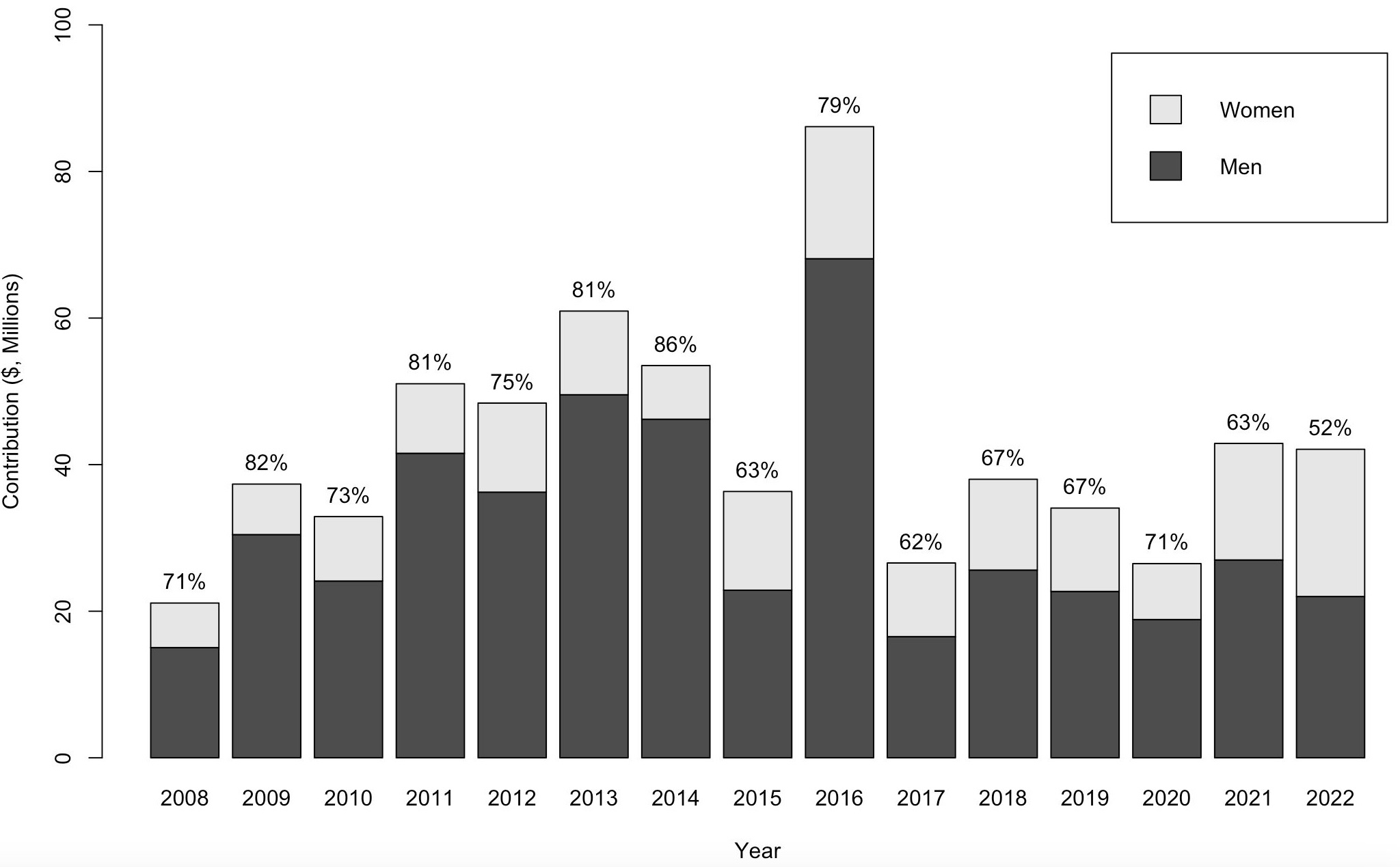
Discussion
- Gender disparities persist in CIHR funding: women receive fewer grants, lower contribution amounts, and are less likely to be recipients than men
- Current initiatives: GENDER R25 (NIH), Women Leading in Neurology program (AAN), women's neurology training and mentorship (University of Toronto)
- Future studies: trends over time, gender-diverse groups
- Future recommendations: gender-diverse reviewers, blind review, diversity training, public reporting of reviewer and recipient gender
Fig. 3 Gender-stratified frequency (%) of awarded CIHR grants to neurologists
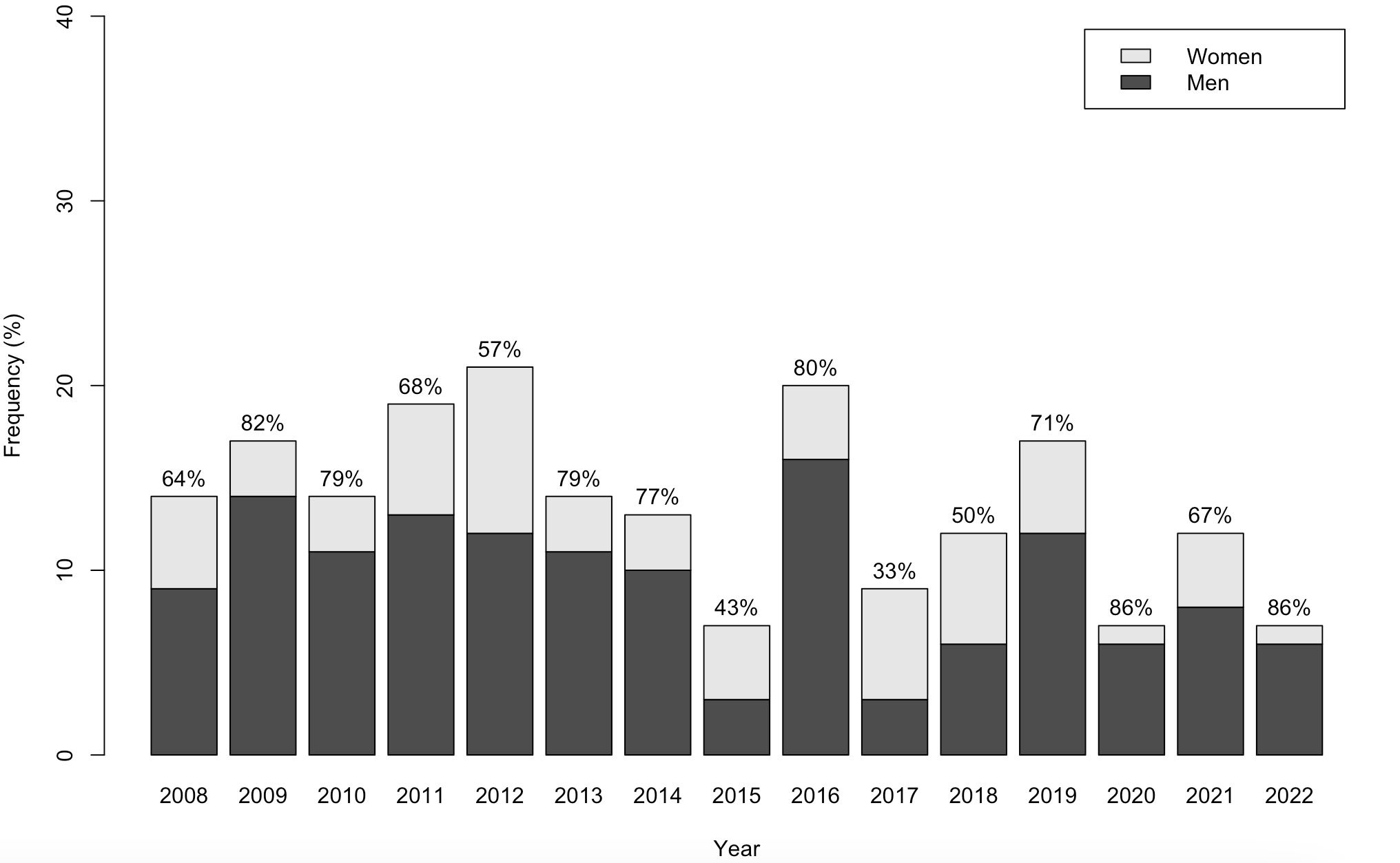
References:
- Tricco AC et al. CMAJ. 2021. PMID 33593950.
- Nguyen AX et al. Front Neurol. 2021. PMID 34497579.
- Canadian Medical Association. 2019. https://www.cma.ca/sites/default/files/2019-11/2019-06-spec-sex.pdf
- Witteman HO et al. Lancet. 2019. PMID 30729688.
- Canadian Institutes of Health Research. 2022. https://webapps.cihr-irsc.gc.ca/decisions/p/main.html?lang=en#sort=namesort%20asc&start=0&rows=20.
- Gender API. 2022. https://gender-api.com/.
Early malignant transformation of intracranial epidermoid cysts: a case report and systematic review
Background
- Intracranial epidermoid cysts (IEC) are benign intracranial lesions
- Predominantly located in the cerebellopontine angle (CPA)1
- 1% of intracranial tumors1
- Rarely undergo malignant transformation1,2
Aim: To report a case of IEC evolving into squamous cell carcinoma (SCC) 1-year post-resection and conduct a systematic review of cases of malignant transformations of IECs within 2 years.
Methods
Fig. 1 Flow diagram of the selection of articles for inclusion as searched on MEDLINE, EMBASE, and Scopus (01/1946-12/2023)
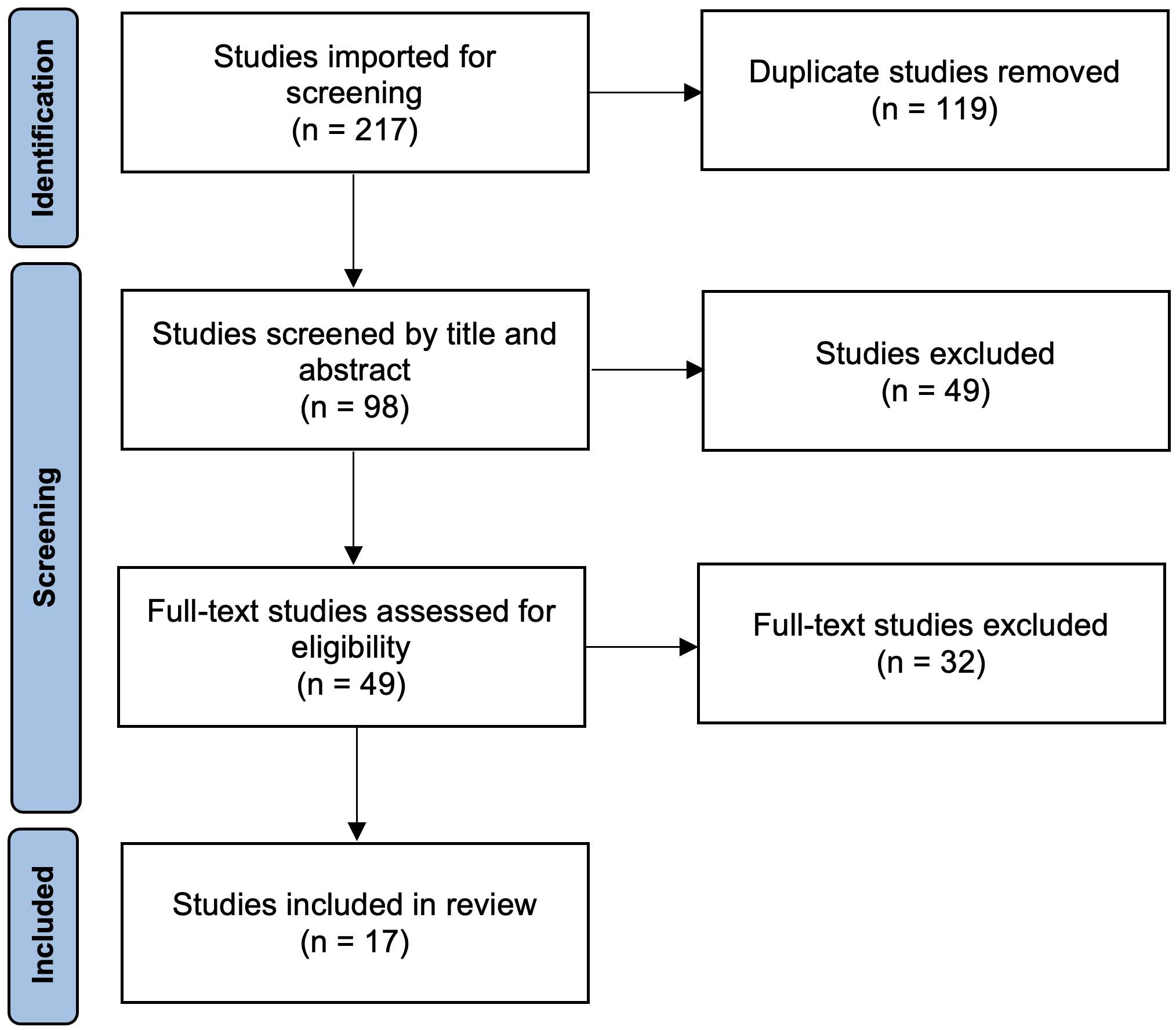
Case
- 11/2019: 48F presented with tinnitus and vertigo -> left CPA IEC on MRI
- 05/2022: Surgical resection, pathology confirmed IEC
- 07/2023: Presented with headaches, nausea, vomiting, right facial weakness, and rapid cyst progression -> cyst fenestration, pathology revealed high-grade SCC (p40+, p16-, Ki67 25-30%)
- 08/2023: Leptomeningeal involvement and enhancement of lumbar and sacral spine
- 09/2023: 26.7 Gy in 10 fractions of radiation
- 10/2023: Pembrolizumab + carboplatin x 4 cycles
- 05/2024: Continued on pembrolizumab alone
Results
- 17 (8F, 9M) underwent malignant transformation of IEC within 2 years
- Mean age at presentation: 56.06 years
- Most in CPA (n=12, 71%); all transformed to SCC, of which 2 (12%) had LC
Table 1. Characteristics of 17 included cases (1946-2023)
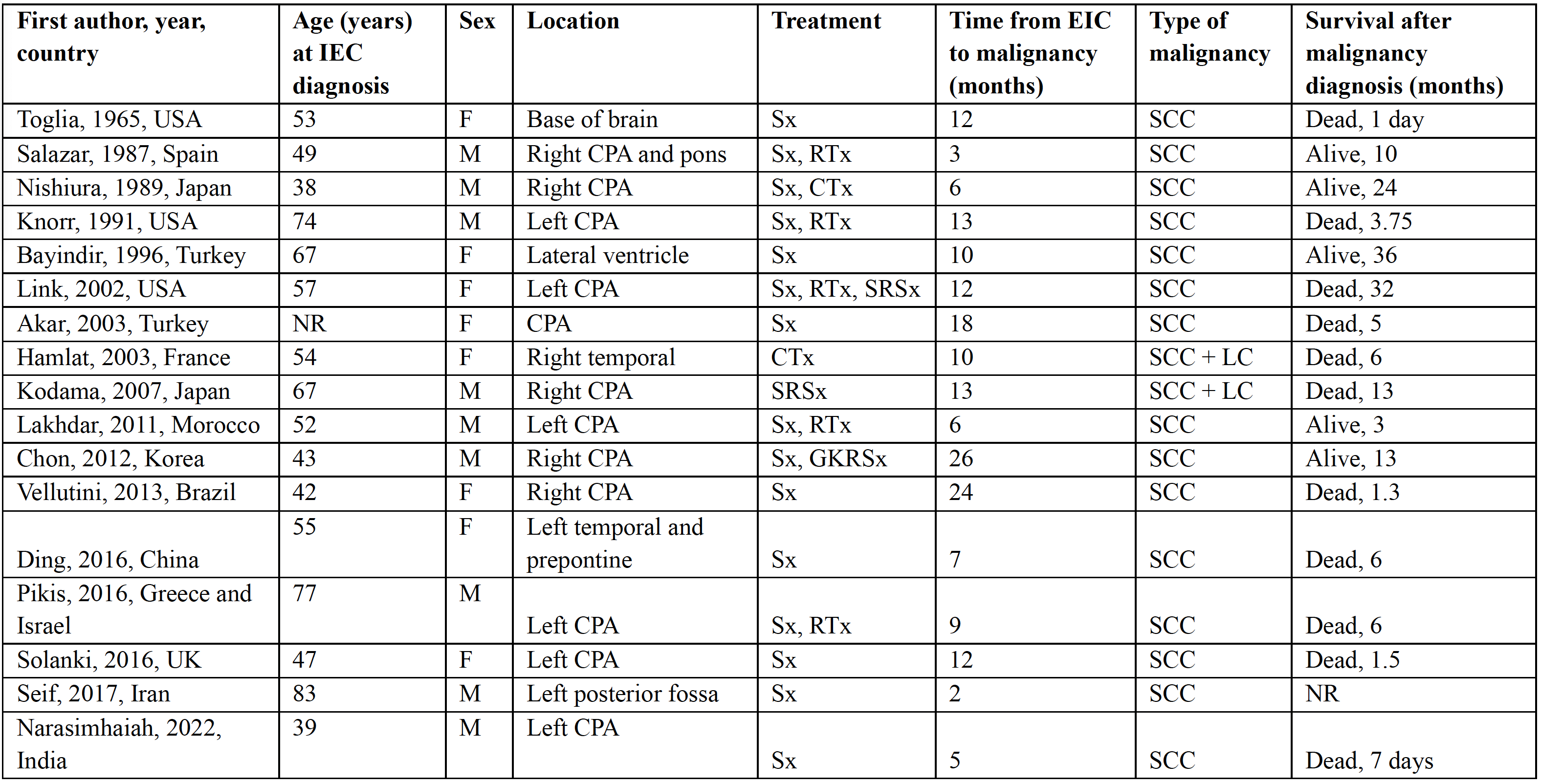
CPA, cerebellopontine angle. Sx, surgery. RTx, radiation therapy. CTx, chemotherapy. SRSx, stereotactic radiosurgery. GKRSx, gamma knife radiosurgery. SCC, squamous cell carcinoma. LC, leptomeningeal carcinomatosis. NR, not reported.
Discussion
- Malignant transformations of IECs are rare
- We report a case of transformation within 1-year post-resection
- Regular follow-up is crucial for early malignancy detection and treatment
- Future studies should evaluate factors contributing to accelerated malignant progression of IECs
Fig. 2A) MRI head axial T2 FLAIR and B) MRI head coronal T1 demonstrating left CPA tumor in 05/2023; C) Histopathology H&E stain high power and D) low power view of atypical keratinizing squamous cells infiltrating fibrous tissue.
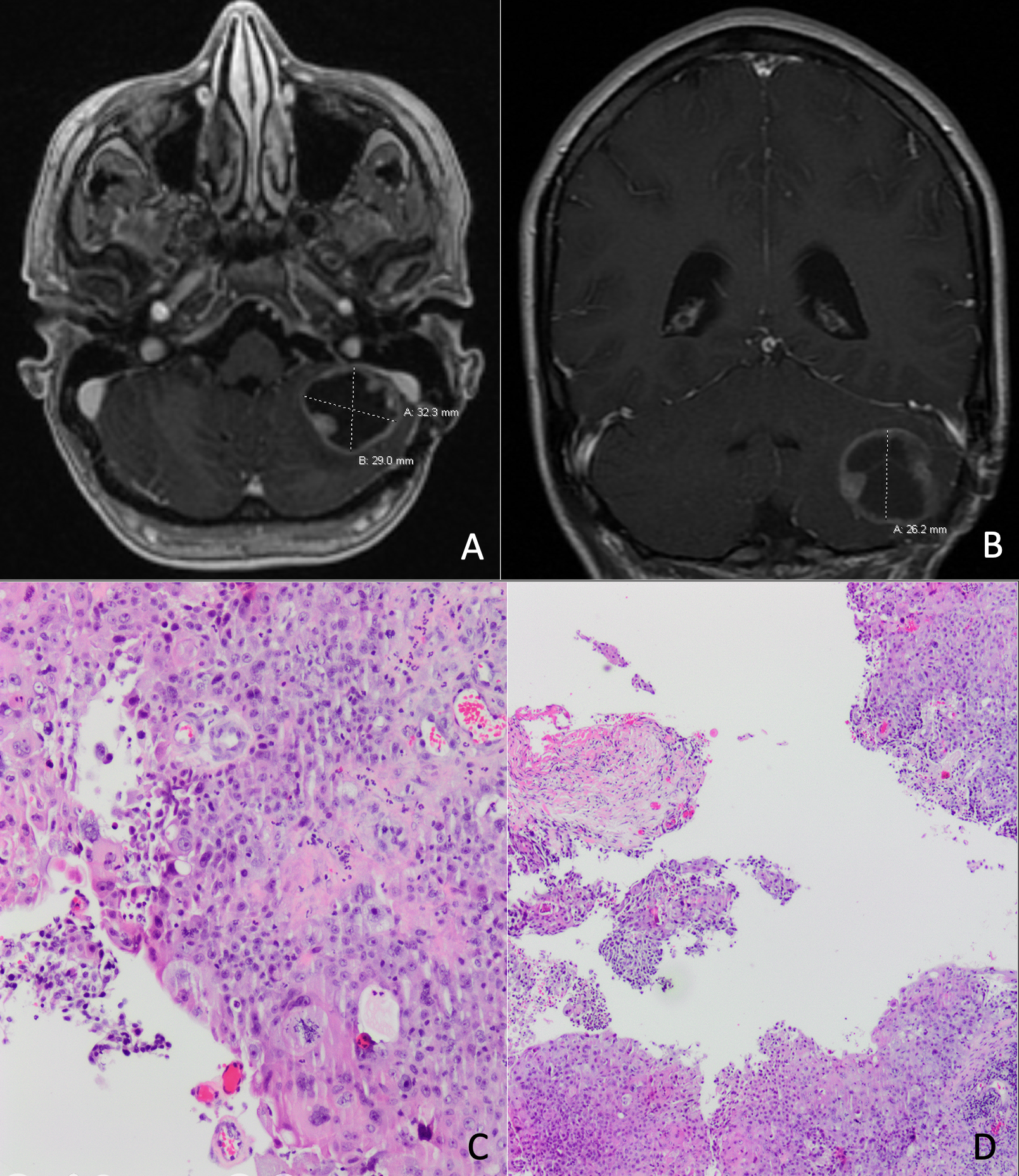
References:
- Hamlat A et al. J Neurooncol. 2005. PMID 16193391
- Vellutini EAS et al. Br J Neurosurg. 2014. PMID 24345076.
Sex and Gender in Neurological Trials: 40 Years of Inadequate Reporting

Background
- Sex and gender are distinct, non-interchangeable concepts with independent impacts on health outcomes in neurology.
- It is already known that women are under-represented in stroke and cognitive neurology research.
- There is a growing number of pharmacologic options in neurology practice. In 2023, Neurology tied with Oncology and Hematology as specialties with the most new FDA drug approvals.
- The quality of sex and gender reporting and analysis in neurological randomized controlled trials (RCTs) remains unknown.
Purpose
This poster aims to review RCTs leading to neurological drug approval by the FDA for their use of accurate sex and gender terminology and the incorporation of sex and gender into study design and discussion.
Methods
This is a cross-sectional review of peer-reviewed RCTs published between 1985 and 2023 and cited in the approval process of neurological drugs. Key steps were based on the PRISMA 2020 statement for systematic reviews and STROBE statement for reporting cross-sectional studies:
- The Drugs@FDA database was screened by two independent reviewers and experienced third party to extract all agents approved for the treatment of a neurological disorder.
- For each included drug, FDA drug labels and medical and statistical reviews were used to identify all trials cited in drug approval. Inclusion and exclusion criteria were applied to each trial.
- Data were extracted from each included trial by two independent reviewers and third party conflict resolver. Extracted data included the use of sex and gender terms and their inclusion in data analysis, as well as trial characteristics.
- Data were summarised using descriptive statistics. For continuous variables, the associations between study characteristics (e.g., publication year) and use of sex and/or gender terminology and inclusion of sex- and/or gender-based analysis were examined using logistic regression models. For binary characteristics, between-group differences were examined using Fisher exact tests.
Results
| Table 1: Study characteristics (N = 216) | |||
| Year published | n | Median no study sites | IQR |
| 1985-1994 | 14 | 46.5 | 55 |
| 1995-2004 | 74 | ||
| 2005-2014 | 58 | Median sample size | IQR |
| 2015-2024 | 71 | 294 | 545 |
| Funding source | n | Sub-specialty | n |
| Government | 3 | Epilepsy | 55 |
| Industry | 200 | Movement | 39 |
| Industry and non-profits | 1 | Headache | 34 |
| Federal funding and non-profits | 1 | Autoimmune | 31 |
| Foundation | 1 | Other | 57 |
| Not reported | 9 | ||
Figure 1: Accuracy of use of sex and gender terms for all trials.
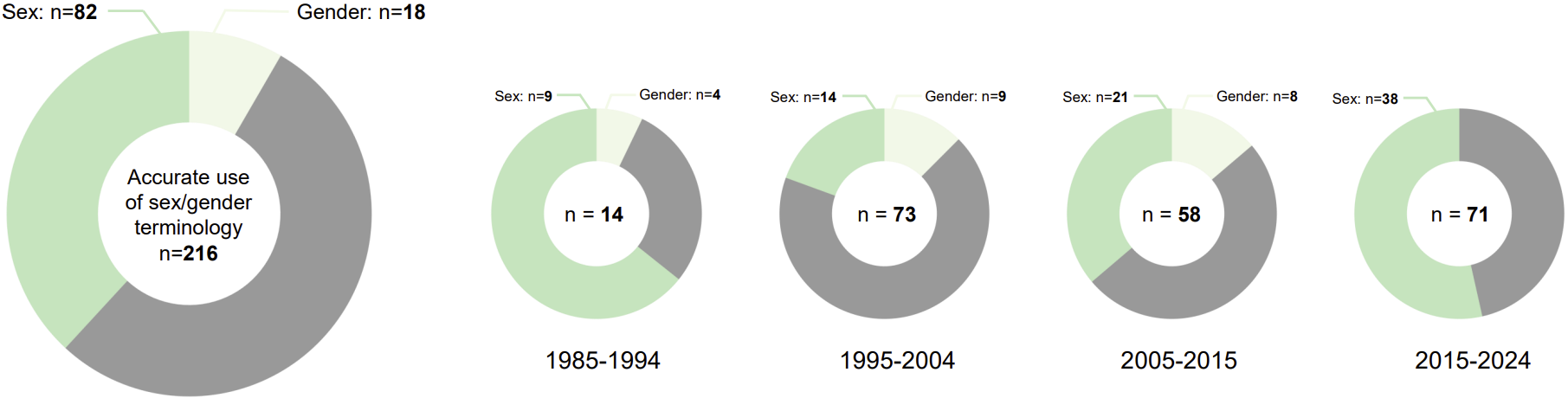
- For all trials: 82 consistently used sex-related terms (male, female; green), 18 consistently used gender-related terms (man, woman; beige), and 115 inaccurately used sex- or gender-related terms (grey), most of which (74) used sex and gender terms interchangeably. One study used no sex or gender terminology.
- By publication year: Logistic regression model found no significant relationships between publication year and correct use of sex (p = 0.024), gender (p = 0.062), or sex or gender (p = 0.154) terms after Bonferroni correction, regardless of subspecialty.
Figure 2: Proportion of trials reporting sex or gender distributions relative to primary outcomes, adverse events, deaths, or any outcome or including sex or gender in their discussion sections (5 figures).
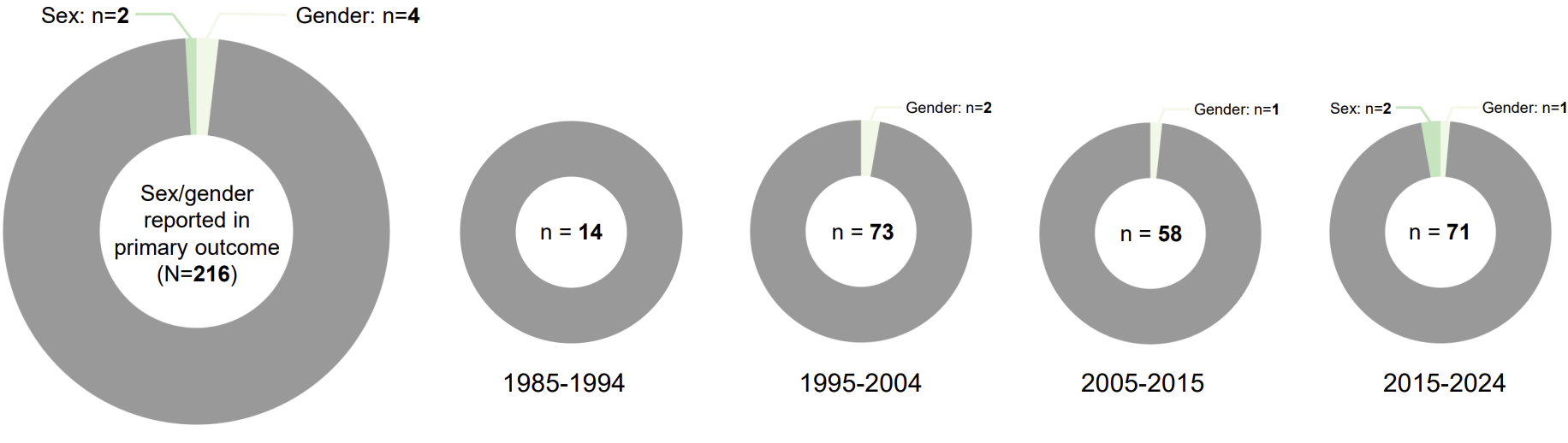
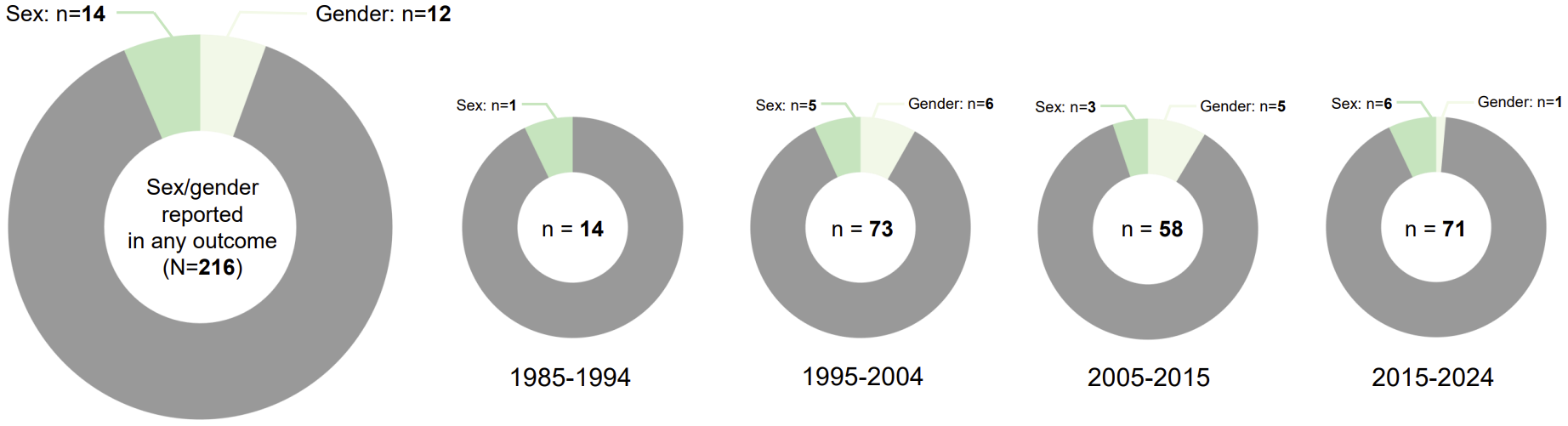
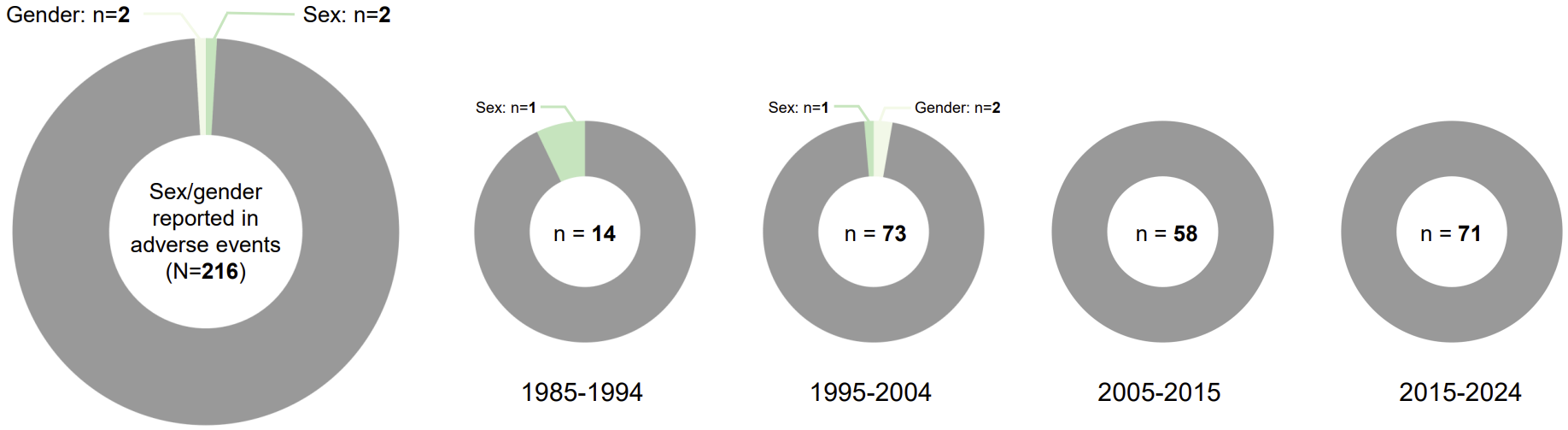
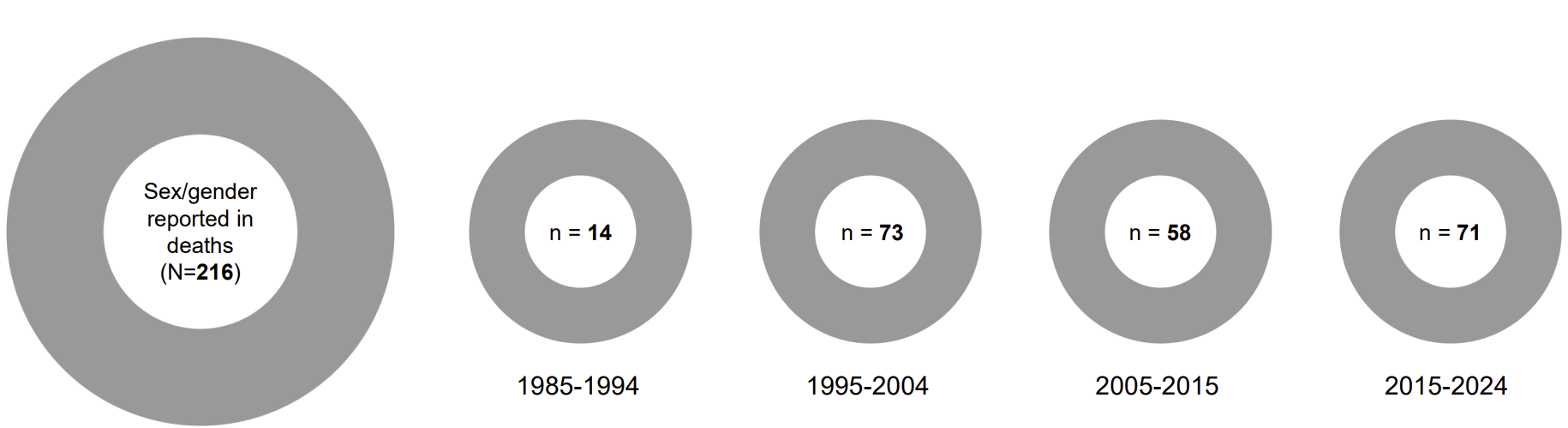
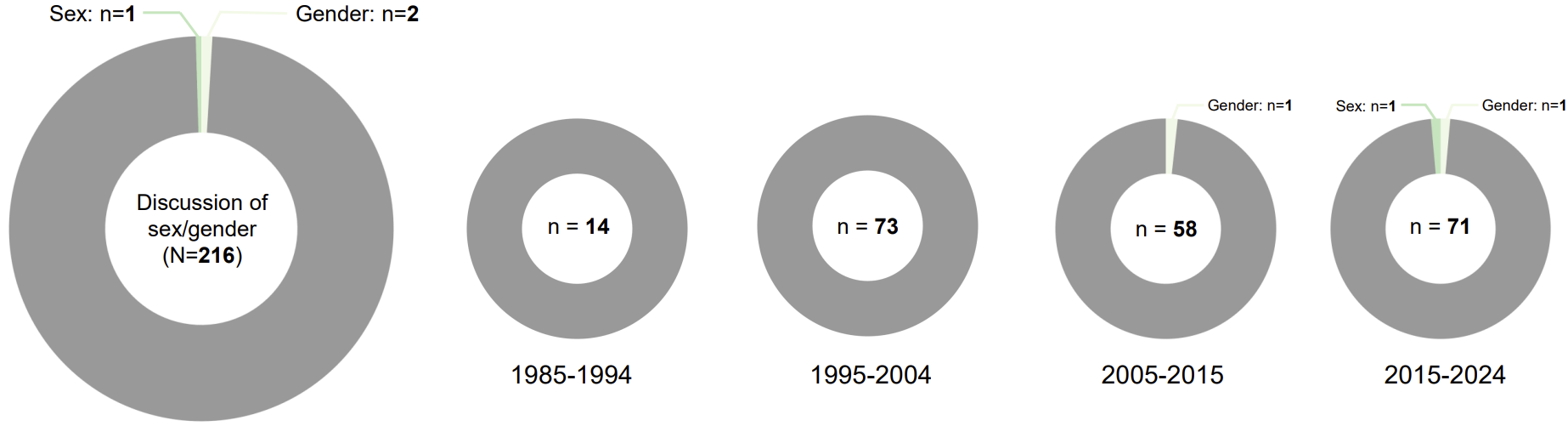
For each outcome, all trials and decade-by-decade distributions shown. Grey: Trials not reporting sex or gender. Green: Trials reporting sex. Beige: Trials reporting gender.
Discussion
Regarding study design:
- Sex- or gender-based analyses were undertaken in only a few studies (0-12%).
- Only 3 out of 216 studies mentioned sex- or gender-based analysis in their discussion sections. A further 5 studies discussed sex or gender as a limitation.
Regarding sex and gender terminology:
- Many studies (45.4%) did not use sex and gender terms rigorously.
- No studies included sex or gender minority group categories.
- Definitions of sex and gender were never provided.
Overall, there was no change in sex and gender reporting or analyses over time or between subspecialties. The vast majority of studies were industry-funded.
Conclusions
Despite extensive research demonstrating the importance of sex-specific analyses and the obligation to consider sex as a biological variable for access to NIH funding since 2016, there has been no significant change (p>0.05) in the quality of reporting or analysis of sex or gender in therapeutic trials in neurology. Given the private funding model of most RCTs, drug approval-level requirements may be more effective to correct these shortcomings.
Accuracy of code stroke activations: a tale of two comprehensive stroke centres
Introduction
- Ontario Stroke System operates on a hub-and-spoke model that centralizes acute stroke expertise at comprehensive stroke centres (CSC) which serve primary stroke centres (PSC) or non-designated centres (NDC)
- Code stroke activations involves rapid mobilization of health care resources
- The hyperacute stroke treatment window has recently been extended to at least 24 hours, leading to a surge in code strokes and out-of-protocol cases
Objective
1) Quantify the proportion of out-of-protocol code stroke activations in two large CSC in Toronto, Canada, and describe which criteria were not met
2) Compared use of thrombolysis or thrombectomy in those seen in- or out-of-criteria
2) Compared use of thrombolysis or thrombectomy in those seen in- or out-of-criteria
Methods
Cohort
- Patients aged 18 years or older who were seen as code strokes in the ER between January 1, 2022 – December 31, 2022
- CSC1: St Michael’s Hospital (SMH)
- CSC2: Sunnybrook Health Sciences Centre (SHSC)
- Includes those arriving by paramedics (bypass protocol) and those activated by ER team
- Inpatient code strokes
- Code strokes activated by another service
- Patients transfered from a PSC for thrombectomy
- Chart review was performed to determine if patients met FAST and ACT-FAST screening criteria
- Paramedic-activated strokes: data extracted from paramedic notes and stroke neurologist notes
- ER-activated strokes: data extracted based on the ER team’s notes/screening sheets (when available) and the stroke neurologist assessment.
Results
Table 1. Reasons for off-criteria code stroke activations
| CSC1 N = 436 |
CSC2 N = 674 |
|
| By pass protocol | n = 352 | n = 516 |
| Did not meet time- based criteria | 48 (13.6) | 88 (17.1) |
| Did not meet symptom-based criteria: had no facial weakness, motor weakness or speech difficulty | 9 (2.6) | 14 (2.7) |
| Exclusions as per paramedic protocol | ||
| CTAS 1 | 2 (0.6) | 9 (1.8) |
| Symptoms of the stroke resolved prior to paramedic arrival or assessment | 18 (5.1) | 3 (0.6) |
| Blood sugar <3 mmol/L | 1 (0.3) | 0 (0.0) |
| Seizure at onset of symptoms or observed by paramedics. | 6 (1.7) | 6 (1.2) |
| Glasgow Coma Scale <10 | 1 (0.3) | 11 (2.2) |
| Terminally ill or palliative care patient. | 0 (0.3) | 4 (0.8) |
| Duration of out of hospital transport will exceed two hours. | 1 (0.3) | 0 (0.0) |
| More than one contraindication | 1 (0.3) | 5 (1.0) |
| ED activated | n = 84 | n = 158 |
| Within 6 hours of symptom onset | 44 | 101 |
| Within 6-24 hours of symptom onset | 40 | 56 |
| Exclusions as per ED activation protocol | ||
| Time based exclusion (mismatch of last seen well between ED documentation and stroke team documentation) | 5 (6.0) | 25 (15.8) |
| Symptom based exclusion (mismatch between ED documentation of symptoms vs. stroke team documentation) | 22 (26.2) | 25 (15.8) |
| No symptoms in ED documentation | 6 (7.1) | 13 (8.2) |
Table 2. Receipt of treatment in patients seen as code stroke
| CSC1 (n = 352) | CSC2 (n=674) | |||||
| By-pass protocol* | Off criteria (n = 48) |
On Criteria (n = 304) |
P value | Off criteria (n = 88) |
On Criteria (n = 428) |
P value |
| Thrombolysis | 2 (4.2) | 65 (21.4) | 0.003 | 3 (3.4) | 96 (22.4) | <0.001 |
| Thrombectomy | 3 (6.3) | 33 (10.9) | 0.45 | 19 (21.6) | 44 (10.3) | 0.006 |
| Thrombolysis or thrombectomy | 4 (8.3) | 81 (26.6) | 0.006 | 19 (21.6) |
113 (26.4) |
0.42 |
| Thrombolysis and Thrombectomy | 1 (2.1) | 17 (5.6) | 0.49 | 3 (3.41) | 27 (6.3) | 0.45 |
| Discharge disposition | 0.91 | 0.27 | ||||
| Repatriated to another hospital | 21 (43.8) | 131 (43.1) | 47 (55.4) | 191 (44.6) | ||
| Yes, to Stroke Unit | 19 (39.6) | 127 (41.8) | 39 (44.3) | 215 (50.2) | ||
| Yes, but not for stroke | 8 (16.7) | 46 (15.1) | 2 (2.3) | 22 (5.1) | ||
| In those repatriated to other hospital | ||||||
| Median repatriation time (in hours) | 6.7 (3.2 – 11.0) | 5 (3-8) | 0.36 | 5.7 (3.4-7.8) | 4.5 (2.8-7.1) | 0.12 |
| ED activated | Off criteria (n = 32) |
On Criteria (n = 52) |
P value | Off criteria (n =56) |
On Criteria (n =102) |
P value |
| Thrombolysis | 0 (0.0) | 3 (5.8) | 0.28 | 2 (3.6) | 8 (7.8) | 0.50 |
| Thrombectomy | 0 (0.0) | 6 (11.5) | 0.08 | 1 (1.8) | 8 (7.8) | 0.16 |
| Thrombolysis or thrombectomy | 0 (0.0) | 7 (13.5) | 0.04 | 3 (5.4) | 13 (12.3) | 0.18 |
| Thrombolysis and Thrombectomy | 0 (0.0) | 2 (3.9) | 0.52 | 0 (0.0) | 3 (2.94) | 0.55 |
| Discharge disposition | 0.002 | 0.057 | ||||
| Not admitted | 18 (56.3) | 10 (19.2) | 13 (23.2) | 11 (10.8) | ||
| Yes, to Stroke Unit | 7 (21.9) | 26 (50.0) | 29 (51.8) | 70 (68.6) | ||
| Yes, but not for stroke | 7 (21.9) | 16 (30.8) | 14 (25.0) | 21 (20.6) | ||
Discussion
- One in five code stroke activations were out-of-criteria, most of these due to incorrect assessment of last seen normal time
- Out-of-protocol code strokes were less likely lead to acute revascularization treatment
Success with incrementally faster times to endovascular therapy (SWIFT-EVT): a systematic review and meta-analysis
Background
Previous research demonstrates that for acute ischemic stroke (AIS), rapid initiation of endovascular therapy (EVT) improves patient outcomes.1
A major systematic review and meta-analysis assessing data through 2014 (the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials, HERMES) demonstrated that particularly over the initial 6 hours of AIS onset, rapid performance of EVT markedly improves outcomes.2
A major systematic review and meta-analysis assessing data through 2014 (the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials, HERMES) demonstrated that particularly over the initial 6 hours of AIS onset, rapid performance of EVT markedly improves outcomes.2
Objective
This analysis aimed to provide updated metrics summarizing estimates for modified Rankin Scale (mRS) improvements accrued by streamlining time to EVT in the initial 6 hours of stroke onset.
Methods
•Electronic databases including National Library of Medicine (PubMed.gov), EMBASE, and GoogleScholar were searched for manuscripts from 2014 onward to avoid overlap with HERMES.
•The search strategy identified 14,092 records, 133 records reviewed in full text, identifying N=5 studies meeting eligibility criteria.
•Priori eligibility criteria for screening was: diagnosis (ischemic stroke), intervention (EVT), and endpoint of mRS 0-2.
•Eligible studies reported time-benefit slope with times from AIS onset (or time last seen normal) to EVT commencement; the predictor was onset-to-groin (OTG) time.
•Primary outcomes evaluated were 90-day functional independence (mRS 0-2), secondary endpoints included 90-day excellent function (mRS 0-1), and mortality.
•Executed random effects modeling to generate a pooled effect estimate for benefits accrued by each 60-minute incremental pre-EVT time savings over our study window of 0-360 minutes (6 hours).
•Review was registered with the UK’s National Institute for Health and Care Research international Prospective Register of Systematic Reviews (PROSPERO), registration number 483826.
•The search strategy identified 14,092 records, 133 records reviewed in full text, identifying N=5 studies meeting eligibility criteria.
•Priori eligibility criteria for screening was: diagnosis (ischemic stroke), intervention (EVT), and endpoint of mRS 0-2.
•Eligible studies reported time-benefit slope with times from AIS onset (or time last seen normal) to EVT commencement; the predictor was onset-to-groin (OTG) time.
•Primary outcomes evaluated were 90-day functional independence (mRS 0-2), secondary endpoints included 90-day excellent function (mRS 0-1), and mortality.
•Executed random effects modeling to generate a pooled effect estimate for benefits accrued by each 60-minute incremental pre-EVT time savings over our study window of 0-360 minutes (6 hours).
•Review was registered with the UK’s National Institute for Health and Care Research international Prospective Register of Systematic Reviews (PROSPERO), registration number 483826.
Results
Primary Endpoint:
•For each hour saved within the time frame of 0-270 minutes (4.5 hours), the odds of achieving functional independence (mRS 0-2) improve by 25% (OR 1.25, 95% CI 1.16-1.35, I2 40%).
•Within the later time frame of 271-360 minutes (6 hours), the odds of achieving functional independence improve by 22% (1.22, 95% CI 1.12-1.33, I2 58%).
Secondary Endpoint:
•For each hour saved within the time frame of 0-270 minutes, the odds of achieving mRS 0-1 improve by 34% (OR 1.34, 95% CI 1.19-1.51, I2 27%).
•Within the later time frame of 271-360 minutes the time savings benefit drops to 20% (OR 1.20, 95% CI 1.03-1.38, I2 60%).
•Three studies reported a time-savings and mortality relationship.
•For each hour saved within the time frame of 0-270 minutes (4.5 hours), the odds of achieving functional independence (mRS 0-2) improve by 25% (OR 1.25, 95% CI 1.16-1.35, I2 40%).
•Within the later time frame of 271-360 minutes (6 hours), the odds of achieving functional independence improve by 22% (1.22, 95% CI 1.12-1.33, I2 58%).
Secondary Endpoint:
•For each hour saved within the time frame of 0-270 minutes, the odds of achieving mRS 0-1 improve by 34% (OR 1.34, 95% CI 1.19-1.51, I2 27%).
•Within the later time frame of 271-360 minutes the time savings benefit drops to 20% (OR 1.20, 95% CI 1.03-1.38, I2 60%).
•Three studies reported a time-savings and mortality relationship.
Conclusion
•There was a 22-25% increase in the odds of achieving functional independence with each hour saved from onset to EVT.
•This data may be useful to inform patient-specific and systems planning decisions.
•Further studies should evaluate alternative endpoints to ensure patient treatment optimization and prompt patient selection for EVT.
•This data may be useful to inform patient-specific and systems planning decisions.
•Further studies should evaluate alternative endpoints to ensure patient treatment optimization and prompt patient selection for EVT.
Figure 1. PRISMA flow diagram demonstrating study selection for data included in the meta-analysis
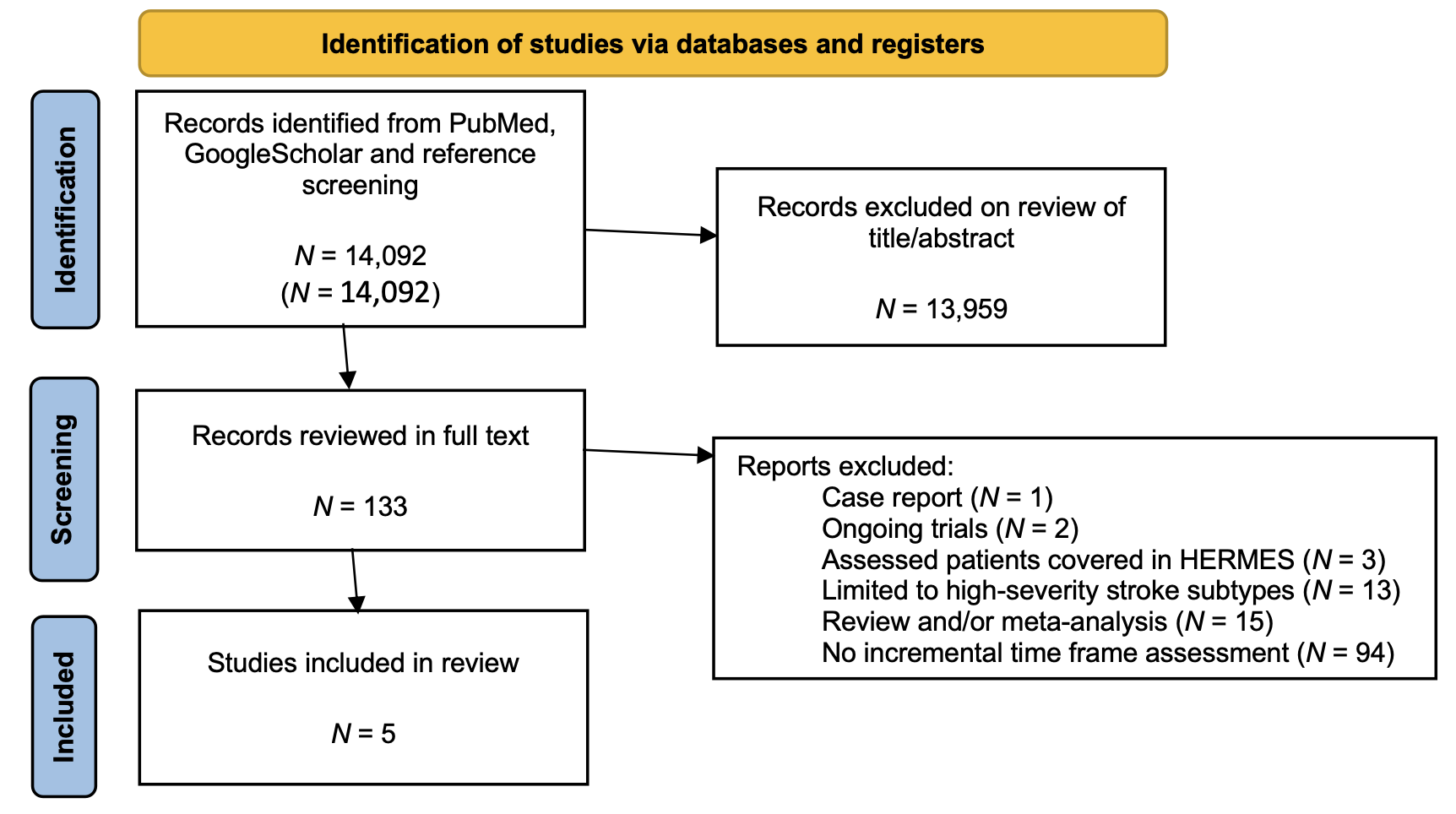
Figure 2. Forest plot for primary endpoint of each hour’s time savings and incremental gain in functional independence for 0-270’ time frame
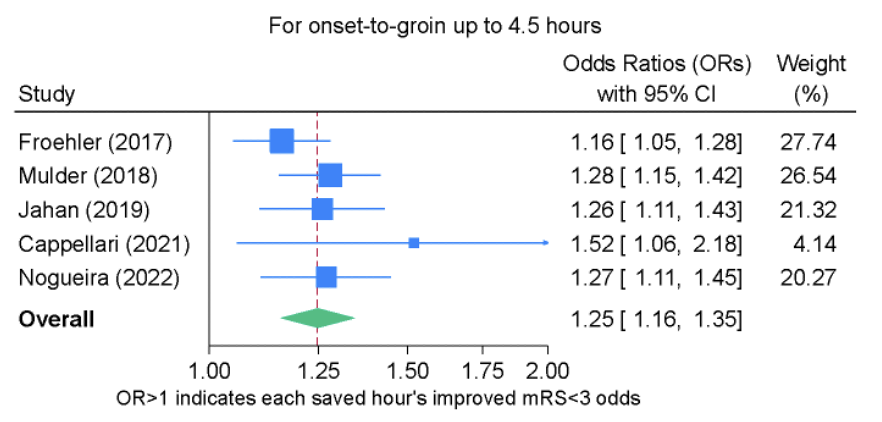
Figure 3. Forest plot for primary endpoint of each hour’s time savings and incremental gain in functional independence for 271-360’ time frame
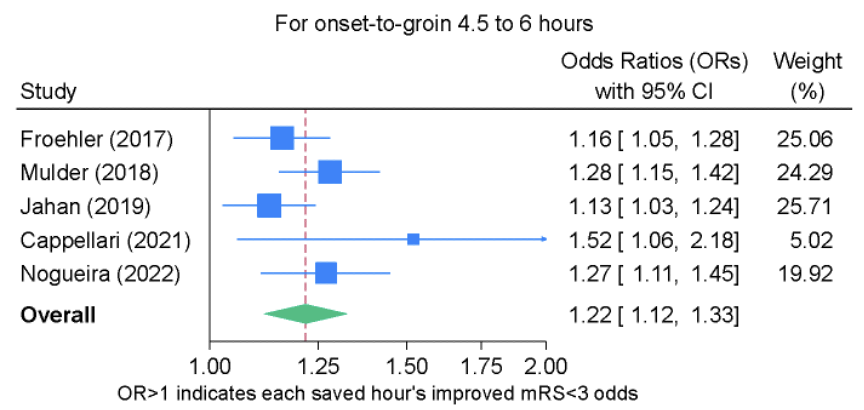
References
1. Warach S, Johnston SC. Endovascular Thrombectomy for Ischemic Stroke: The Second Quantum Leap in Stroke Systems of Care? JAMA 2016;316(12):1265-6. DOI: 10.1001/jama.2016.12266.
2. Saver JL, Goyal M, van der Lugt A, et al. Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. JAMA 2016;316(12):1279-88. DOI: 10.1001/jama.2016.13647.
2. Saver JL, Goyal M, van der Lugt A, et al. Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. JAMA 2016;316(12):1279-88. DOI: 10.1001/jama.2016.13647.
KNOW BRAIN EMBRACE CARE: A study investigating young adult stroke patients’ knowledge and behaviour around lifestyle
Background
- Neurological disorders affect 43.1% (3.4 billion) of the global population1.
- Stroke is the greatest global contributor of nervous system disability adjusted life-years (DALYs)1.
- Stroke prevalence, over the past 30 years, has increased by 86.1%1 with 12.2 million new stroke cases annually2,3.
- There is an emerging trend of rising stroke incidences (~40%) among the working population (≤65 years of age) over the past 10 years with approximately 15% among persons ≤50 years of age4.
Stroke & Risk Factors
- Stroke is linked to non-modifiable (e.g., age, genetics, sex, race) & modifiable risk factors (MRFs).
-
~90% of the population attributable stroke risk is associated with 10 MRFs (e.g., hypertension, hyperlipidemia, low physical activity, smoking, alcohol use, poor diet)5,6, which are lifestyle-associated & preventable7,8.
- Of the MRFs, hypertension is the largest (57.5%) & single attributable MRF globally that contributes to stroke1 & total stroke disability-adjusted life-years (DALYs)7.
-
MRFs can be targeted through risk factor modification, particularly Lifestyle Medicine (LSM)9,10.
- LSM: a clinical & evidence-based discipline that applies behavioural, motivational, environmental, & medical principles to address the complexity (MRFs) of chronic disease(s)11,12 (Figure 1).
Figure 1. LSM Pillars
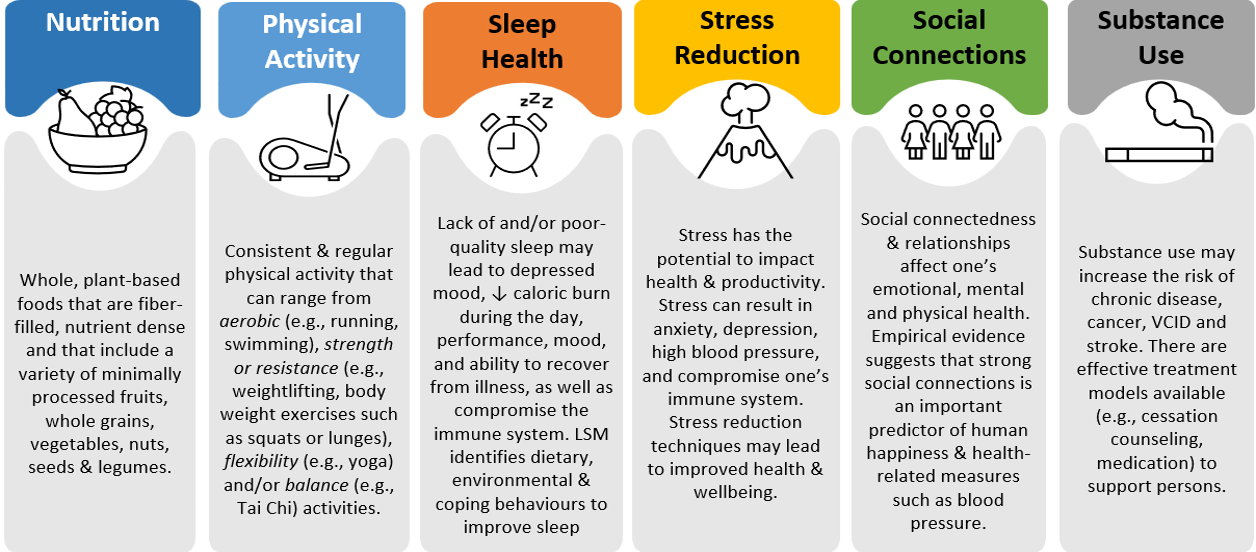
Current Gap & Study Aims
- Few studies investigated LSM-related knowledge & behaviours among younger adult stroke patients.
- No studies conducted in Canada investigating younger adult stroke patients’ LSM-related knowledge & behaviours as well as facilitators & barriers to support such adoption & engagement.
- Study Aims: To assess younger adult patients’ seen at the Stroke Prevention & Neurovascular Clinics at Toronto Western Hospital, University Health Network: 1) LSM-related knowledge & behaviours; and 2) facilitators & barriers in the adoption of healthy lifestyle habits with attention to gender differences.
Methods & Methodology
- A cross-sectional design was employed.
- Data were collected through an online, self-reported survey (using validated surveys) via REDCap following a routine Stroke Prevention or Neurovascular Clinic visit.
- Data were analyzed using descriptive & inferential statistics.
Findings
Sample:
Sample:
- N=103; 56.3% women, 60% White, Age: 47.5 ± 14.3, 54.5% had a prior stroke, 63.7% married & 58% had college/university level of education.
LSM-related Knowledge
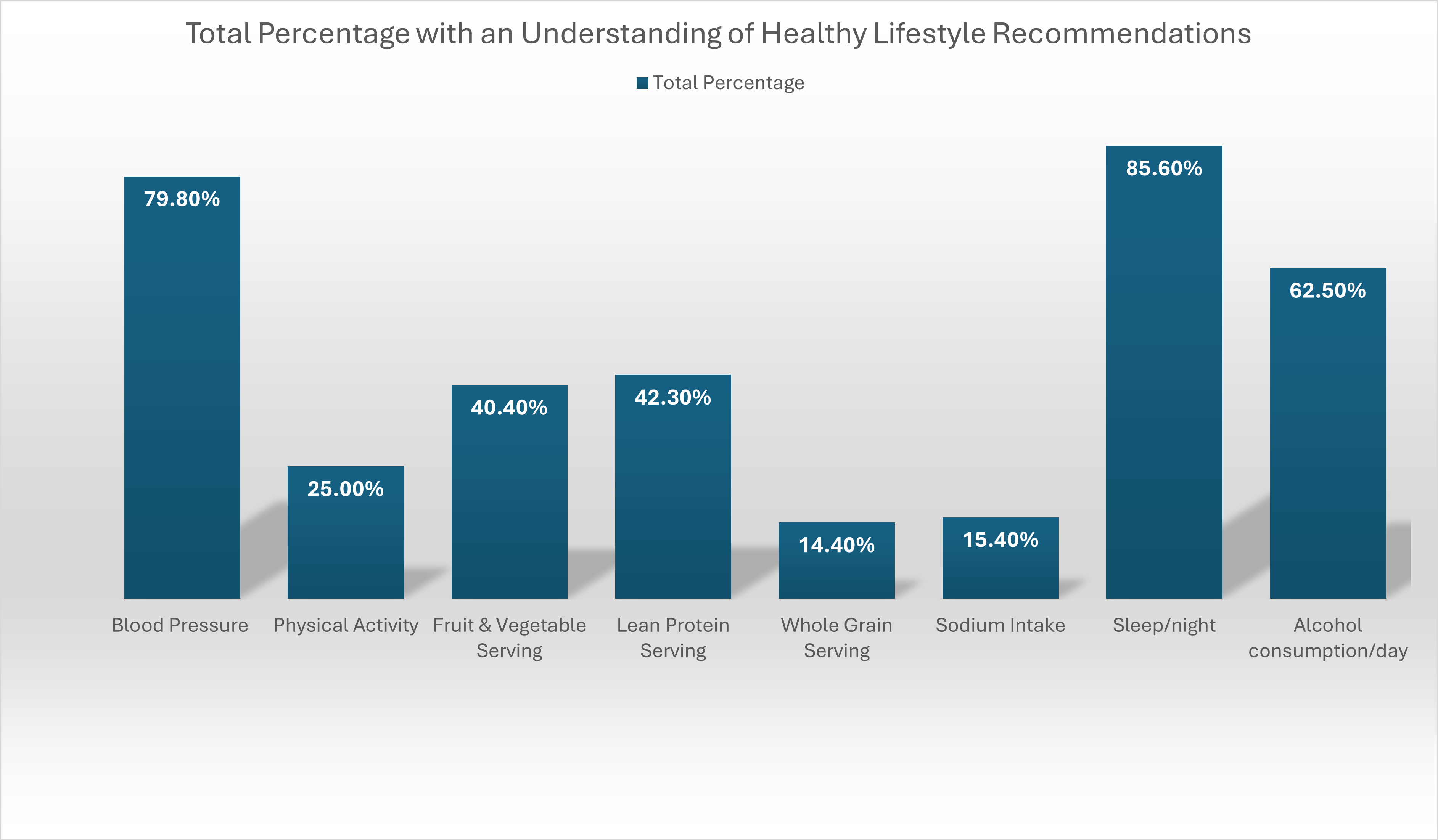
LSM-related Behaviours
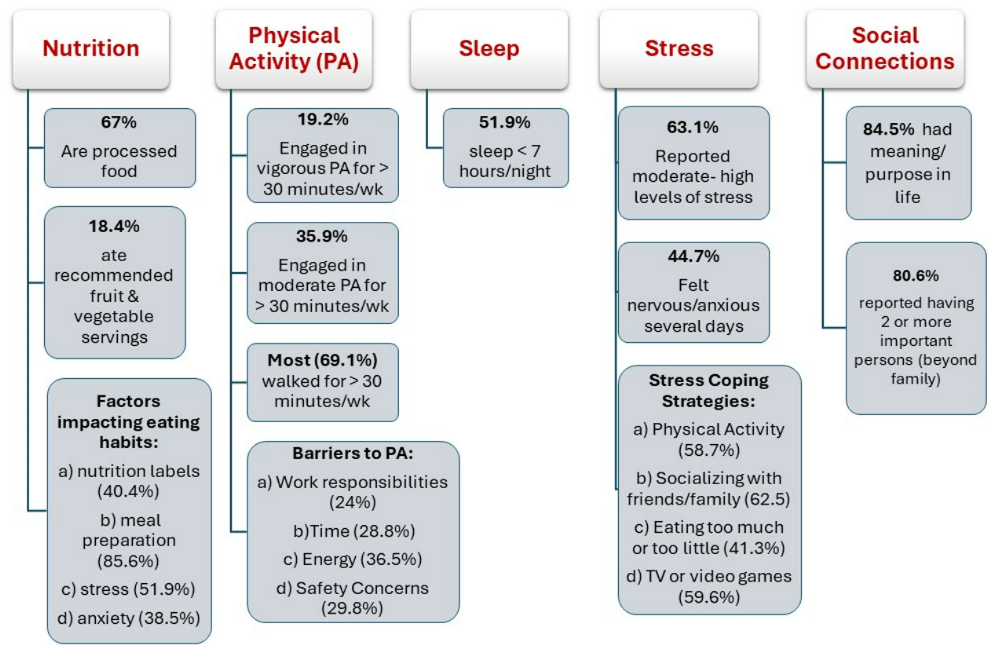
Gender Difference:
- Women had higher knowledge about fruit & vegetable serving (p= 0.002) and lean protein serving recommendations (p=0.026) compared to men.
- More women relied on packaged or fast food (p=0.023) & had a negative food relationship (p=0.021).
- Emotions (p= <0.001) impacted women’s eating habits (vs. men & non-binary person).
- More women coped with stress through journalling (p=0.021), counselling (p=0.014), socializing with friends & family (p=0.018) (vs. men & non-binary person).
Study Implications
- Findings provide valuable insight of younger adults’ current brain health & LSM-related knowledge, barriers & influencing factors to healthy lifestyle habits/status.
- A myriad of barriers exists that may hinder younger stroke patients from incorporating LSM recommendations in their daily lives.
- Findings will inform the development of patient-informed stroke prevention-related education & psychosocial interventions that address the identified gaps, barriers & influencing factors for healthy lifestyle adoption for brain health in relation to LSM concepts.
References
http://qrto.ai/u-PiBJJz
Funding: The Slamen-Fast New Initiative
http://qrto.ai/u-PiBJJz
Funding: The Slamen-Fast New Initiative
Exploring young adult stroke patients’ lived experience, healthy lifestyle habits, and recommendations for designing innovative brain care-related initiatives
Background
- Worldwide, stroke incidences among young adults of working age (≤65years) has increased significantly (by 40%) over the past decade1,2.
- Potential explanation to the rise in stroke incidence is the increase in modifiable risk factors such as hypertension, low physical activity, poor diet3.
- Such increase in stroke incidences has implications during the most dynamic and “active” period of the lives of young adults.
- Post-stroke, young adults experience psychological, physical & cognitive deficit as well as impaired quality of life, negative impact on their self-identity, role, relationships & occupational status2,4,5.
- Further, the current design & delivery of stroke services and care are focused on the priorities & needs of older adults (physical function and activities of daily living)6,7, failing to meet the differing & unique needs of this patient population8.
Aim
- To gain knowledge & a deeper understanding of young adult stroke patients’ experiences, lifestyle habits & support needs for brain care-related education & interventions.
Methods
- Design. A descriptive qualitative study was used. Participants who took part in the quantitative phase of a larger mixed methods study (n=103) that expressed an interest in taking part in the qualitative phase, were invited to take part in semi-structured focus groups.
- Data Collection Procedures. Data were collected through focus groups. Focus groups were conducted virtually, recorded & transcribed verbatim. Simultaneous data collection & analysis were conducted.
- Data Analysis. Data were analyzed using inductive thematic analysis outlined by Braun and Clarke's (2006) six-step process9: 1) familiarization with the data; 2) generation of initial codes; 3) searching for themes; 4) reviewing themes; 5) defining and naming themes; and 6) producing report. Trustworthiness of the qualitative data were maintained through: dependability, credibility, conformability & transferability10.
Findings
- Sample: N=12 (4 focus groups in total)
Demographic & Clinical Characteristics
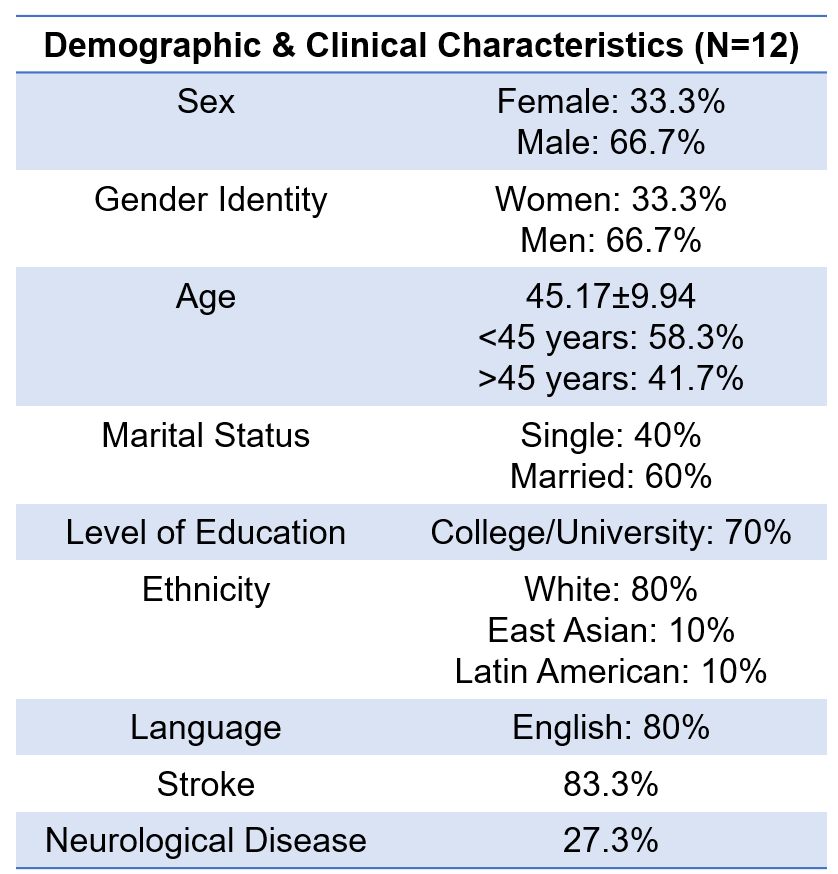
Six Emergent Themes
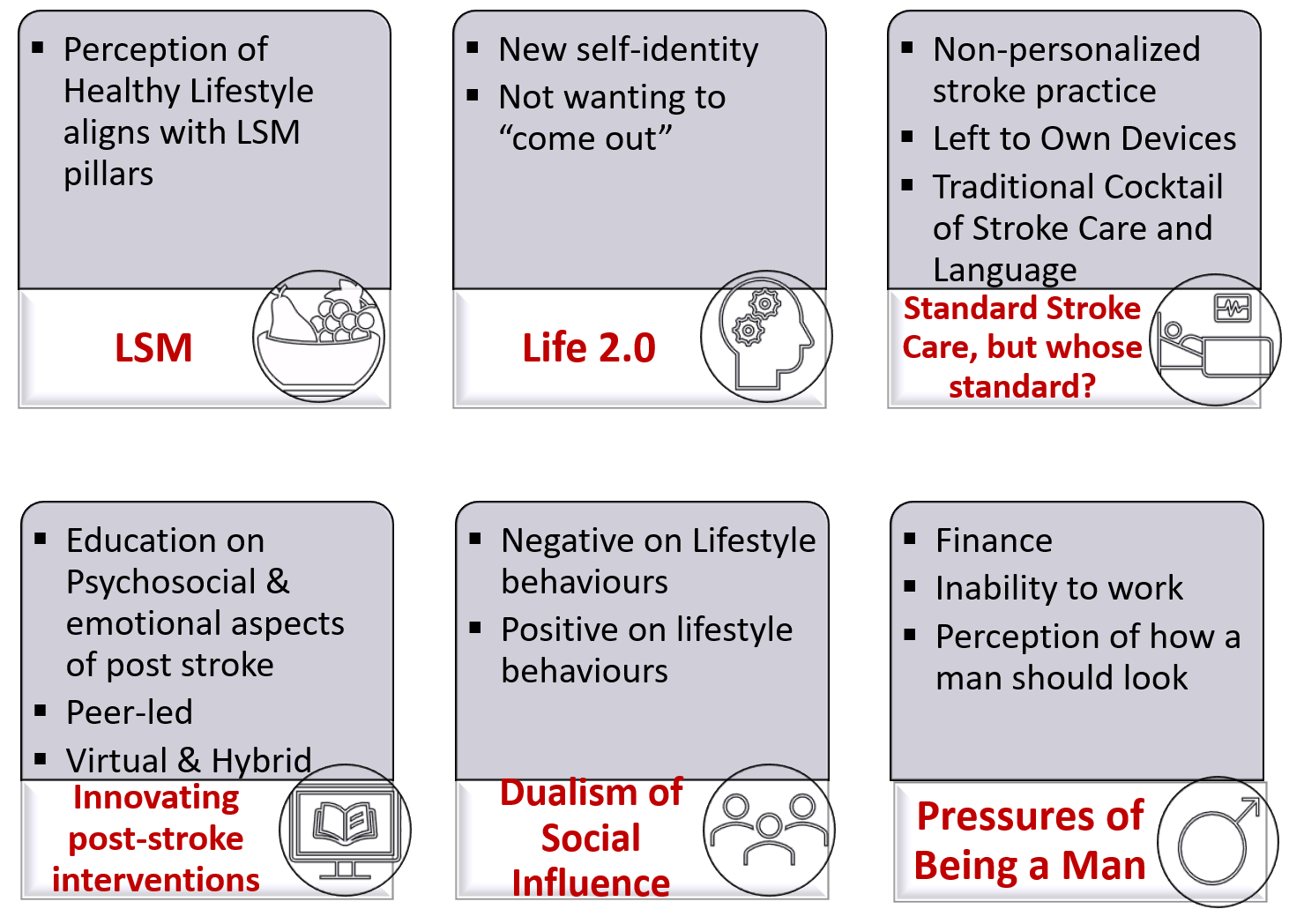
Summary of Themes
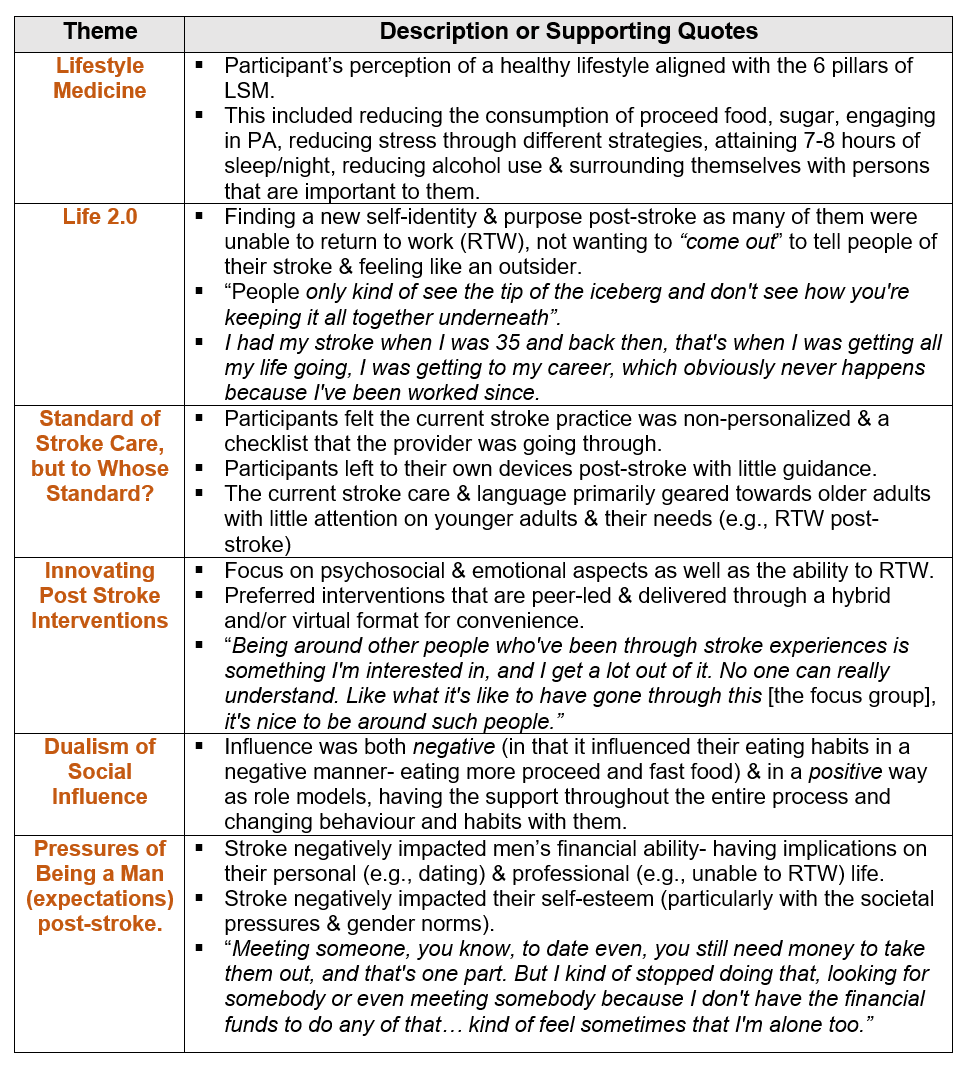
Significance
- Study findings are essential to: 1) Mobilize an understanding of young adult stroke patients’ lived experience; 2) Reconceptualize the current model of stroke care and services that is traditionally geared towards older adults; and 3) Inform the development of brain care-related education and interventions to meet the unique needs, priorities, and preferences of young adult stroke patients.
References
https://qr.link/uNTtK3
Funding: The Slamen-Fast New Initiative
https://qr.link/uNTtK3
Funding: The Slamen-Fast New Initiative
Endovascular therapy for cerebral venous thrombosis: an international survey






Preoperative corticosteroids reduce diagnostic accuracy for primary central nervous system lymphoma biopsies: a meta-analysis
INTRODUCTION
- Primary central nervous system lymphoma (PCNSL) is highly sensitive to corticosteroid induced cell arrest, apoptosis and shrinkage
- The impact of preoperative corticosteroids on the accuracy of PCNSL diagnosis using tissue obtained from biopsies remains debated
PURPOSE
- Determine the effect of preoperative corticosteroids on non-diagnostic biopsy rates for PCNSL in immunocompetent adults
METHODS
- Systematic review and meta-analysis of randomized control trials, longitudinal cohort and retrospective case-control studies
- Searched Ovid MEDLINE, Embase, Web of Science and Scopus databases inception until 31 December 2022
- Inclusion: 1) age ≥18 years, 2) immunocompetent, 3) undergoing diagnostic biopsy for suspected PCNSL, 4) histopathologic confirmation of de novo PCNSL diagnosis, 5) study described whether or not corticosteroid treatment was given before obtaining tissue
SEARCH RESULTS
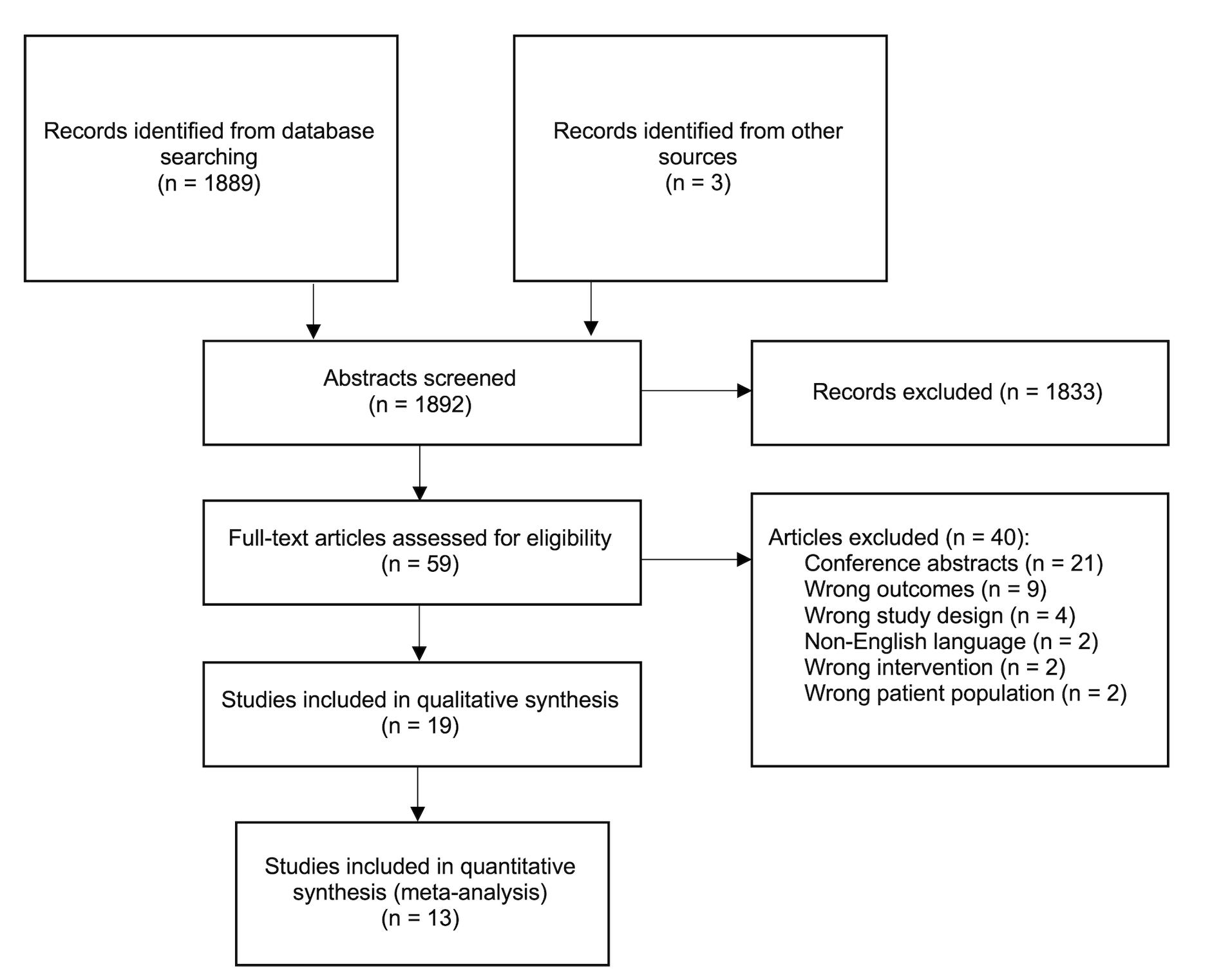
RESULTS
ALL BIOPSY TYPES
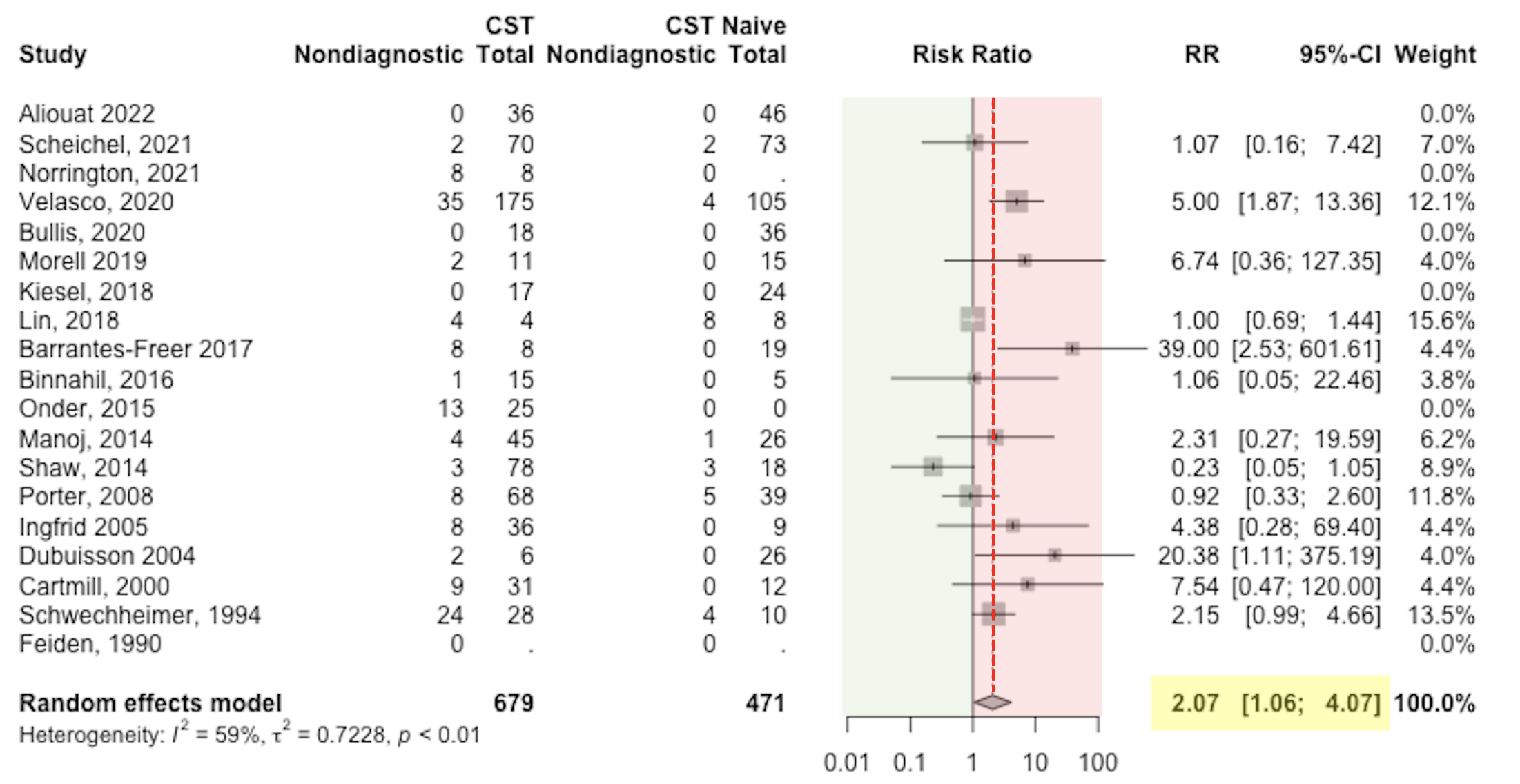
Preoperative corticosteroids (CST) conferred a significantly increased risk ratio (RR = 2.1 [95% CI: 1.1-4.1]) of non-diagnostic tissue in cases of suspected PCNSL.
DEMOGRAPHICS
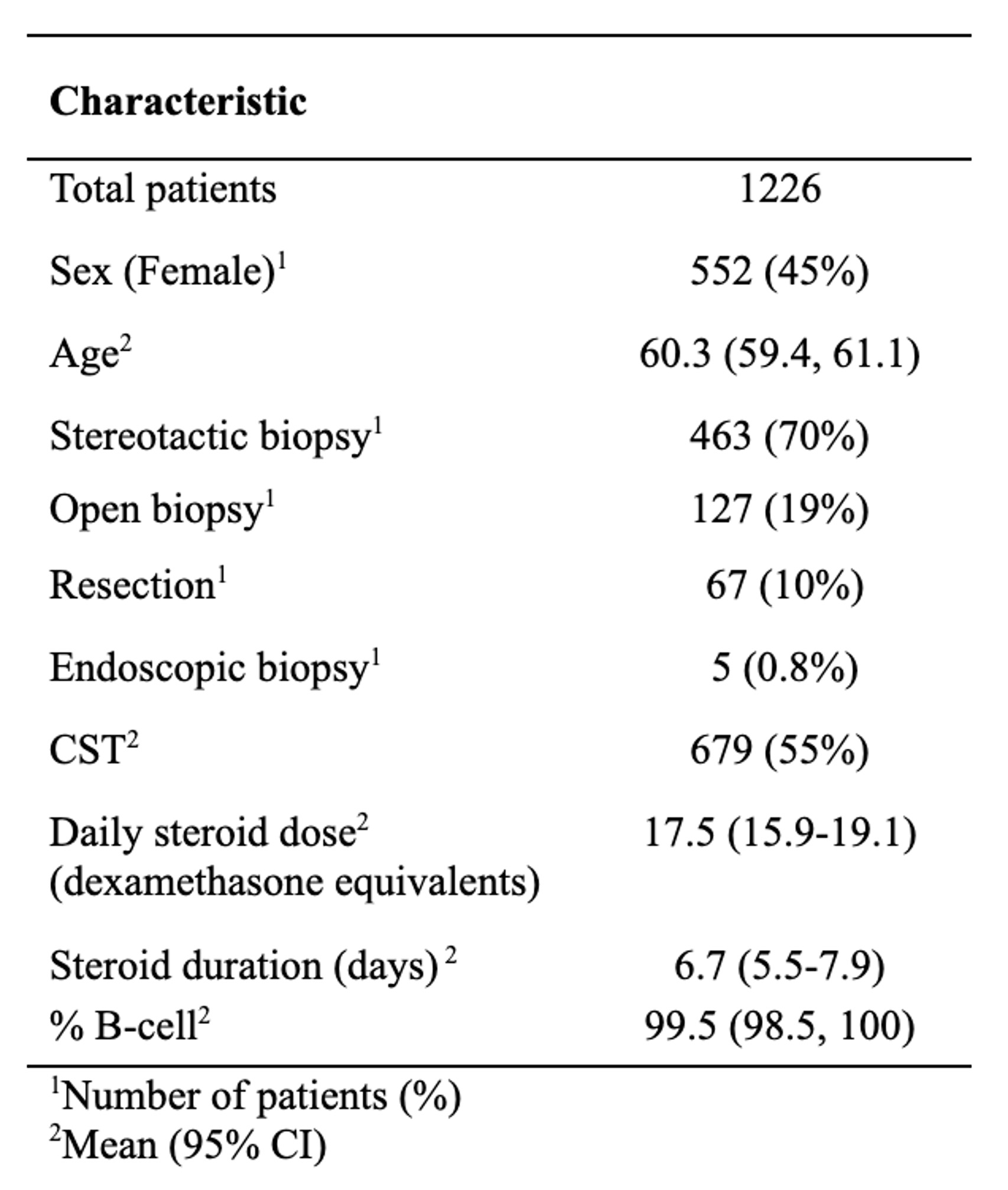
- Biopsy type specified for 662 patients
- 55% patients received preoperative steroids (dexamethasone 4mg q6h most common)
STEREOTACTIC BIOPSIES ONLY
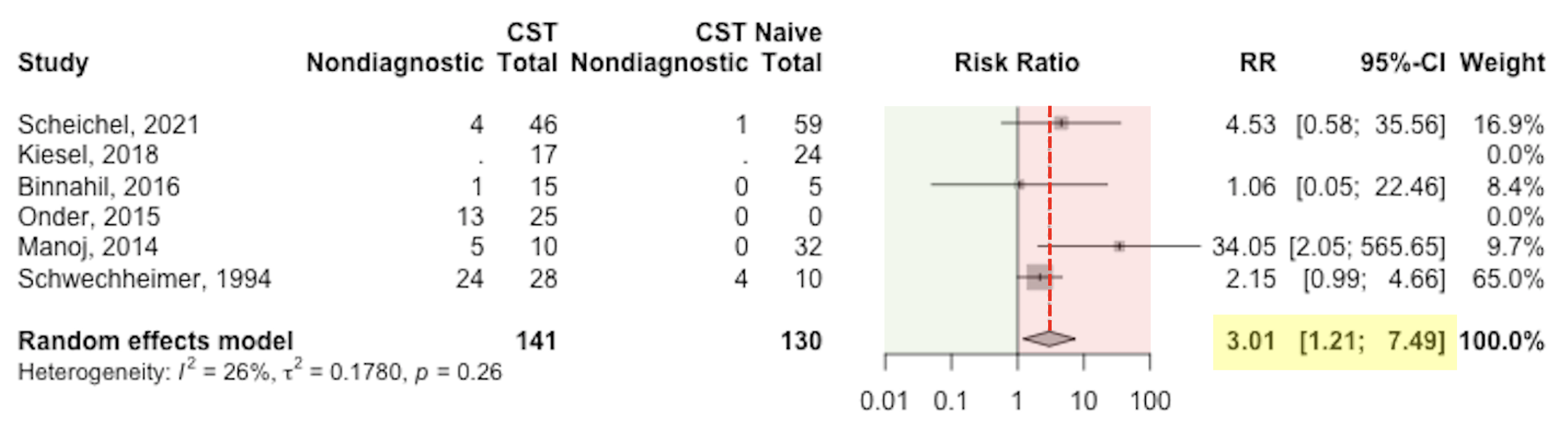
In subgroup analysis limited to stereotactic biopsies, patient pretreated with corticosteroids (CST) were three times more likely to have a non-diagnostic biopsy (RR = 3.0 [95% CI: 1.2-7.5]) in cases of suspected PCNSL.
IMPACT OF PREOPERATIVE CORTICOSTEROIDS
- If given preoperative corticosteroids: 19.3% patients had a non-diagnostic first biopsy
- If corticosteroid naïve: 5.7% patients had a non-diagnostic first biopsy
TAPERING CORTICOSTEROIDS?
- No association between mean cumulative steroid dose (p=0.18) or duration of steroids (p=0.44) and non-diagnostic biopsy rate
- No association between steroid taper duration and non-diagnostic biopsy rate (p=0.90)
CONCLUSIONS
-
Corticosteroids should be withheld, if clinically safe, prior to stereotactic biopsies in cases of suspected PCNSL.
- If corticosteroids are administered preoperatively, an open biopsy should be considered instead of stereotactic biopsy
The importance of transition clinics: A chart-review examining demographic, health, and social variables in young adults with epilepsy who were recently transitioned
Background
- Research has consistently shown that adolescents with a chronic illness transitioning from pediatric to adult care struggle through the transition period
- Research suggests that young adults tend to continue to struggle after transition
- Data looking specifically at the two-year period after young adults with epilepsy transition to adult care is limited
Methods
- We performed a retrospective chart review of 58 patients transferred from pediatric to adult care between 2017 and 2018, who had at least one appointment with their adult provider.
Demographics
|
n= 58 |
||
| Age at seizure start | 10.5 years (range:1.0-17.4) | |
| Age at first adult centre visit | 18.5 years (range: 17.7-19.7 | |
| Sex | Male | 31 (53.4%) |
| Female | 27 (46.6%) | |
| Seizure type | Focal | 27 (46.6%) |
| Generalized | 28 (48.3%) | |
| Focal and generalized | 2 (3.44%) | |
| Unknown | 1 (1.72%) | |
| Cognitive ability | Typical | 38 (64.4%) |
| Learning Disabilities | 13 (22.0%) | |
| Mild Intellectual Disorder | 5 (8.62%) | |
| Unknown | 2 (3.44%) | |
Results
Mental Health
- Of the 45 patients who filled out mental health questionnaires, 13 (28.9%) met the threshold for major depressive disorder and 25 (56.6%) of patients showed symptoms of anxiety.
- At one-year follow-up, 60% of these patients had similar or worsened depression, and 64% had similar or worsened anxiety scores
- Two patients openly reported self-harm and one patient was hospitalized after a suicide attempt
Follow-ups
- Twelve patients were temporarily lost to follow-up (on average for 1.35 years)
-
11 patients were permanently lost to follow-up
- 4 patients lost after 6 months, 5 patients lost after 12 months, and 2 lost at 24 months
Results (Cont'd)
Medication Compliance
-
23 (39.7%) patients admitted to medication non-compliance
- 15 of these patients had break-through seizures as a result
Other Social Demographics
- 10 patients dropped out of their studies
- 3 had significant substance abuse issues
- 2 patients were incarcerated
Conclusions
- There is a need for greater education and support to help these adolescents/young adults through their transition
- Specifically, patients seem to need more education on the importance of scheduling and attending follow-up visits, as well as the importance of consistently taking medication
- Additionally, finding suggest the importance of addressing mental health concerns when identified
References
- Andrade, D., et al., (2017). Epilepsia; 58(9), 1502 -1517.
- Camfield et al., (2017) Epilepsy Behav; 69: 170–176.
- Nabbout R et al. (2017)Epilepsy Behav; 69: 153–60.
- Thomson L et al., (2014) Dev Med Child Neurol; 56(5): 421–433.
Electrophysiological signatures of sedation in pediatric patients

Introduction
Following admission to the pediatric intensive care unit (PICU) for brain injury, CNS infection, or status epilepticus, sedation is often used for neuroprotection or seizure control. This period carries diagnostic uncertainty due to sedation masking physical exam findings. Continuous electroencephalogram (EEG) monitoring is an added evaluation method to observe background electrical activity and subclinical seizures. EEG can also be used to evaluate brain's ability to respond to stimuli1, such as an anesthetic agent (which PICU patients are routinely subjected to). Previous studies on adults measured the response to anesthesia using two principles: feedforward connectivity and anteriorization of alpha hubs.
Feedforward Connectivity / Phase Lag Index ( dPLIRS)2
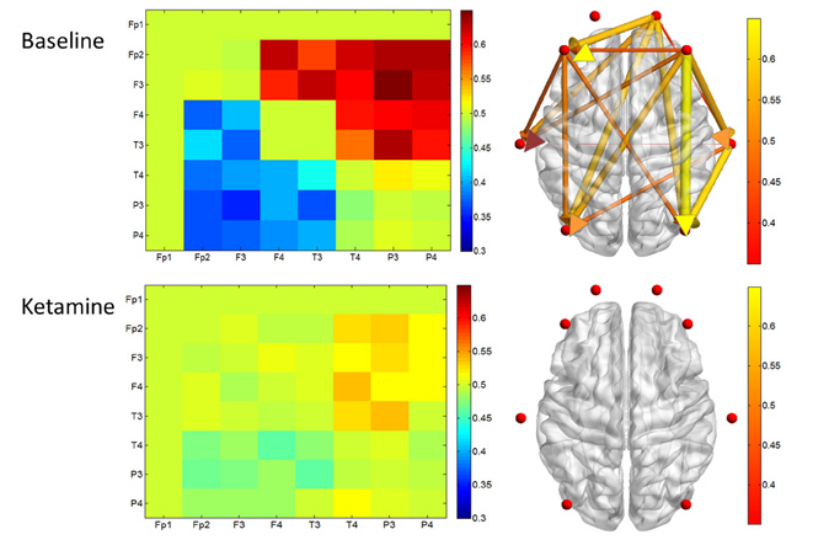
Network Hub Analysis (HubRS)3

ARI = HubRS + dPLIRS
When combined together, a value called Adaptive Reconfiguration Index (ARI) can be calculated and correlated with outcomes post injury. In a previous adult study, ARI had 100% accuracy in predicting recovery of consciousness at 3 month time point in 11 acute and chronic patients4. Factors predicting a positive outcome included higher ARI scores, distinct anterior shift of the alpha hub, and increased feedforward/decreased feedback connectivity. This current project is an exploratory study aimed at evaluating the effectiveness of translating this model into a pediatric population, with the hypothesis that the same markers of adaptive reconfiguration in response to anesthesia could be correlated with a higher potential for recovering consciousness.
Methods
This was a descriptive, observational pilot study to assess the feasibility of performing this method of EEG analysis on a larger scale. Primary questions were the following:
- Does network reconfiguration predict diagnosis/prognosis across all ages?
- Does network reconfiguration predict diagnosis/prognosis across all anesthetics?
Initially 20 cases were extracted with the following inclusion criteria:
- Admission to PICU at McMaster Children’s Hospital between June 30th 2014 to April 30th 2021
- Age from 1 month to 18 years
- Continuous EEG monitoring in place with and without receiving an anesthetic
Data collected:
Demographics/anasthetic: age, sex, injury etiology, weight, anasthetic (type, infusion rate, boluses)
EEG: strength and direction of functional connectivity using the weighted and directed phase lag index were extracted from 5-minute EEG epochs of EEG drug administration time and post sedation using 10-20 system with 21 channels with XLTEK / Natus system at 256 Hz
GCS: Glasgow Coma Scale (GSC) under anesthesia, GCS after sedation wean
Outcome: Glasgow Outcome Scale Extended (GOSE) three months after EEGEEG Epochs
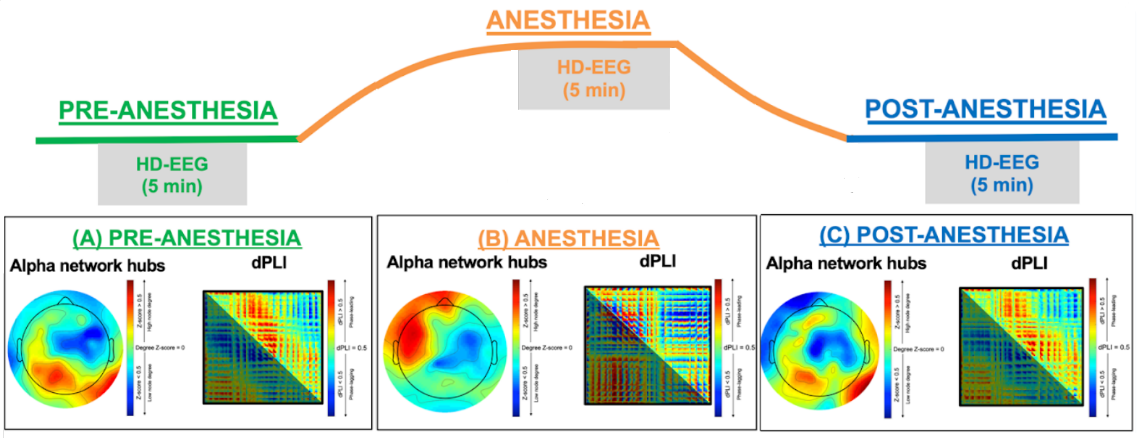
Results
Evaluation of 14 subjects (6 were excluded due to not having an overlap between anasthetic infusion and EEG timing) showed promise in children aged 5-18 undergoing sedation with midazolam, dexmedetomidine, and propofol. Further analysis of five subjects revealed a correlation between adaptive reconfiguration during anesthesia and both higher baseline Glasgow Coma Scale and Glasgow Outcome Scale-Extended scores post-treatment.
Table 1: Clinical and Demographic Characteristics

Results (continued)
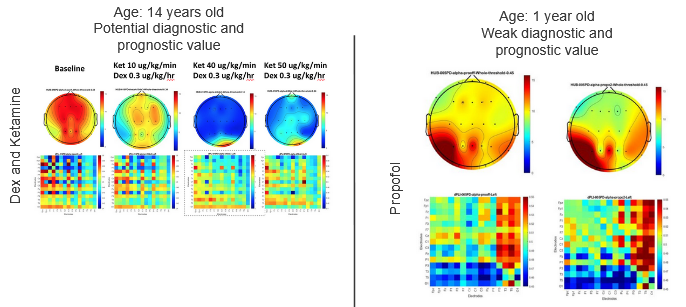
Model most accurate in age 5-18 years
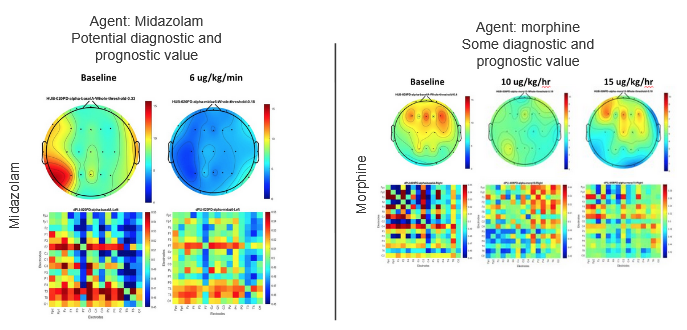
Model most accurate in dexmedetomidine, midazolam, propofol
Discussion
The initial stages of this pilot study offered promising outcomes, showing applicability of the model in a subset of the pediatric population, demonstrating potential of future use. While additional correlational analyses will be essential to assess the model's efficacy, prior to that, the current model needs to be refined for pediatric application. Future steps include the following:
- Modify inclusion criteria to only include appropriate age and anesthetic agents
- Expanding cohort to include 2 additional years of data collection
- Delineate optimal medication dose for ARI calculation
- Perform formal analysis of demographics and ability of model to predict recovery given above parameters
Cardiac screening in children with genetic epilepsy at risk for sudden unexpected death in epilepsy
Background
- People with epilepsy experience greater rates of sudden death than the general population, with the highest risk in genetic epilepsies.
- People with epilepsy experience greater rates of heart disease and sudden cardiac death.
- Many of the genes causally associated with epilepsy are expressed in both heart and brain tissue.
- Growing evidence implicates autonomic dysregulation, especially cardiorespiratory dysfunction, as a mechanism of sudden unexpeced death in epilepsy (SUDEP).
- Routine cardiac screening for epilepsy patients is rarely performed.
Objective: Describe the cardiac phenotype in people with epilepsy caused by variants in genes that are expressed in both the heart and the brain.
Methods
Cohort
Cohort
- Single center, retrospective chart review of patients with developmental epileptic encephalopathies.
- Clinical history, results of genetic investigations, anti-seizure medications, age, and cardiac evaluation data were extracted.
-
Inclusion:
- <18 years old
- clinical diagnosis of epilepsy
- identified genetic variant in a gene clinically evaluated to be causative of epilepsy
- the gene expressses protein in both the heart and the brain
-
Exclusion:
- diagnosed with clinically significant structural heart disease
- ECGs were independently read by a cardiologist electrophysiologist.
- ECG parameters examined included heart rate (HR), PR interval, QRS duration, P-wave axis, QRS axis, T-wave axis, QT interval, rate-corrected QT interval (QTc), QT dispersion, and QTc dispersion.
- For patients with multiple ECGs, the most recent ECG available was analyzed.
- Shapiro-Wilk test of normality
- Median and interquartile range
- Mann-Whitney U tests
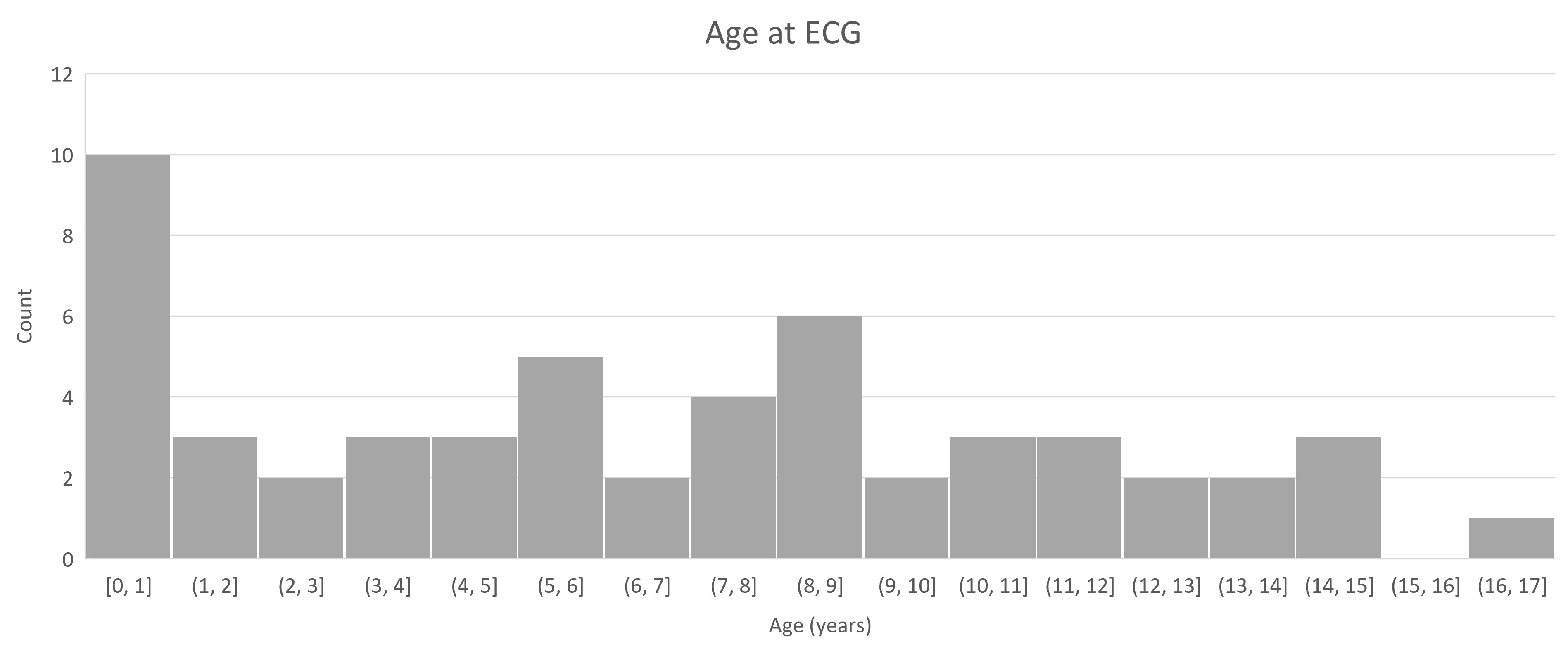
Cohort characteristics
| Variable | n (%), n=54 |
|---|---|
| Age (years) at most recent ECG, median (IQR) | 6.4 (2.7-10.4) |
| Female | 31 (57%) |
| Generalized Tonic-Clonic Seizures (GTCS) | 39 (72%) |
| Epilepsy presentation before 12 months | 45 (83%) |
| Genes SCN1A 15 (28%) SCN2A 4 (7%) KCNT1 3 (6%) CDKL5 8 (15%) SCN8A 4 (7%) CACNA1A 2 (4%) SLC2A1 7 (13%) STXBP1 3 (6%) PPP3CA 1 (2%) MECP2 4 (7%) KCNQ2 3 (6%) |
|
ECG parameter subgroup comparisons
|
SCN1A variant (n=15) |
Other gene variants (n=15) |
P value |
GTCS (n=39) |
No GTCS (n=15) |
P value | Epilepsy duration < 3 years (n=17) | Epilepsy duration ≥ 3 years (n=37) |
P value |
|
| Age at ECG (years) | 6.5 (4.65-7.85) | 6.1 (4.55-8.20) | 0.442 | 7.4 (3-10.2) | 5.3 (2.15-9.55) | 0.265 | 0.75 (0.3-1.8) | 8.7 (6.3-11.8) | <0.001 |
| Female, n (%) | 7 (46.7) | 10 (66.7) | 0.285 | 23 (59.0) | 8 (53.3) | 0.714 | 12 (70.6) | 19 (51.4) | 0.192 |
| Heart Rate | 105 (97-126) | 106 (88-113.5) | 0.209 | 106 (94.5-123.5) | 103 (93-118) | 0.249 | 122 (118-135) | 99 (88-106) | <0.001 |
| PR Interval | 120 (106-128) | 128 (115-133) | 0.110 | 122 (111-135) | 128 (120-131) | 0.246 | 118 (106-124) | 128 (120-136) | 0.005 |
| QRS interval | 72 (65-78) | 72 (67-81) | 0.273 | 72 (63-82) | 72 (64-79) | 0.393 | 62 (60-72) | 74 (66-82) | 0.012 |
| QTc interval | 392 (386.5-416.5) | 387 (374.5-411) | 0.155 | 404 (387.5-422) | 390 (378-410) | 0.056 | 417 (388-427) | 399 (382-418) | 0.118 |
| P-wave axis | 48 (40-59) | 45 (37.5-53.5) | 0.267 | 49 (39.5-60.5) | 44 (32.5-48) | 0.044 | 48 (39-58) | 45 (38-58) | 0.401 |
| QRS axis | 63 (47-82) | 78 (51-82) | 0.203 | 75 (60-88) | 61 (46-83) | 0.110 | 82 (56-99) | 70 (52-85) | 0.050 |
| T-wave axis | 28 (23.5-39.0) | 22 (12-43) | 0.247 | 38 (24-54) | 25 (16-35) | 0.014 | 35 (20-47) | 35 (22-49) | 0.285 |
| QTd | 0.05 (0.041-0.061) | 0.067 (0.035-0.081) | 0.347 | 0.05 (0.038-0.063) | 0.041 (0.038-0.052) | 0.151 | 0.052 (0.046-0.064) | 0.042 (0.036-0.060) | 0.046 |
| QTCd | 0.064 (0.035-0.076) | 0.048 (0.041-0.078) | 0.492 | 0.06 (0.044-0.077) | 0.055 (0.034-0.069) | 0.116 | 0.060 (0.044-0.068) | 0.058 (0.040-0.080) | 0.451 |
Clinical Evaluation
-
Among 54 patients with at least one ECG, 20 (37%) had a clinically identified abnormality.
- Common abnormalities included sinus bradychardia, sinus tachycardia, ventricular hypertrophy, and early repolarization.
- One patient had an incomplete RBBB of unclear significance.
- One patient had short QTc and early repolarization.
-
41 (76%) patients had a repeat ECG:
- 8 showed persistent abnormalities
- 7 resolution of abnormalities
- 7 a new abnormality
- Five patients with an abnormality did not receive a follow up ECG.
- Two patients each had histories of cardiac arrest, syncope, and sudden death in a family member.
- Most common ECG indication was for QTc monitoring on a ketogenic diet or following initiation of a new antiepileptic drug.
Conclusions
- Over 1/3 of our high-risk epilepsy cohort had history of cardiac events or abnormalities on cardiac testing.
- Cardiac phenotypes differed in patients who experienced GTCS - higher P wave and lower T wave axes - and patients with epilepsy for 3+ years - lower HR, greater PR and QRS intervals, and smaller QTd.
-
Further research is needed to determine the clinical significance of these findings and whether routine cardiac screening of high-risk epilepsy patients may be warranted.
- Most abnormalities were seen at older ages, suggesting an initial screen in infancy may be insufficient to capture abnormalities that develop over time.
Future Directions
Case-control comparisons
- General epilepsy population (excluding DEE/genetic epilepsies) - to investigate whether cardiac phenotypes differ for children with epilepsy caused by genetic epilepsies which put them at high risk for SUDEP
- Population averages of healthy, age-matched children - to investigate whether cardiac phenotypes differ for children with genetic epilepsies compared to the general population.
Refractory status dystonicus and hypotension after cardiac arrest in a child with AADC deficiency post gene therapy: a case report
Introduction
- Aromatic L-amino acid decarboxylase (AADC) deficiency:
- Presentation: Severe hypotonia, developmental delay, dystonia, autonomic symptoms.
- Management: supportive with dopamine agonists, SSRIs, and MAO-I
- Novel gene therapy: AAV2 vector to provide a functional copy of AADC
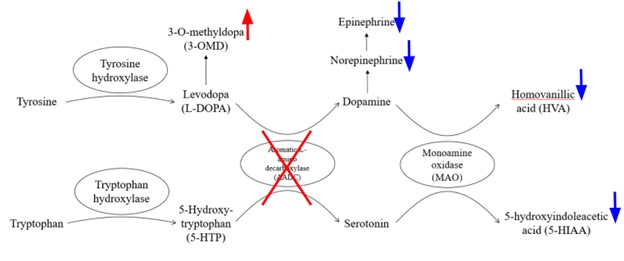
Figure 1. Biogenic amine synthesis pathway

Figure 2 Dopamine pathway map. Adapted from Dopamine Pathways, by OIST. CC by 4.0. https://tinyurl.com/y9px9pvh
Patient baseline post gene therapy
- 10yo female with AADC deficiency status-post intracranial rAAV2-hAADC gene therapy
- Baseline: Walks in standing frame, no pincer grip, jejunal-tube feeding, vocalizes yes-no


Figure 3. Movements before and after cardiac arrest.
Clinical Events
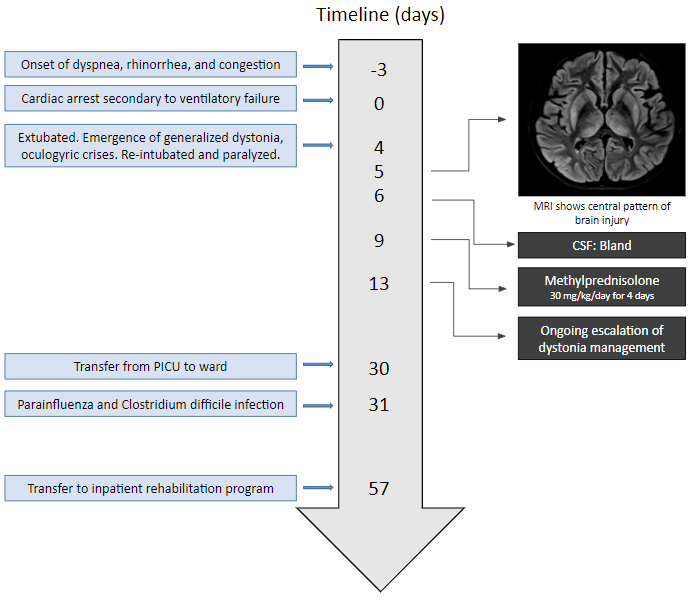
Figure 4. Timeline of clinical events
Examination
- Oculogyric crises and severe generalized dystonia impairing ventilation
- Refractory hypotension requiring 10 day epinephrine infusion
- 4 month followup: Inconsistent visual tracking. Cannot bring hand to mouth. Cannot maintain head upright or sit unsupported. No social smile.
- Moderate encephalopathy with no seizures
- Trihexyphenidyl, selegiline, clonidine, baclofen, and pyridoxine.
- Levodopa was ineffective. Dantrolene caused orolingual hyperkinetic movements.
| Baseline | Post gene therapy | Post cardiac arrest | ||
| Global developmental delay | Severe | Improved | Severe | |
| Hypotonia | Severe | Improved | Severe | |
| Dystonia | Generalized, severe | Improved | Generalized, severe | |
| Oculogyric crisis | Frequent | Resolved | Infrequent | |
| CSF studies | HVA nmol/L (ref) | 23 (450-1132) | Low normal | 27 (167-563) |
| 5HIAA nmol/L (ref) | 6 (179-711) | Low | 7 (67-189) | |
| 3OMD nmol/L (ref) | 1748 (<300) | 793 (<100) | ||
| Genetics DDC | c.714+4A>T (IVS6+4A>T) homozygous | |||
Table 1. CSF studies post cardiac arrest

Figure 5. Brain MRI images 4 days post arrest showing showign axial (A) T1, (B) FLAIR, (C and D) DWI destriction.
Synopsis
Brief in-house cardiac arrest leading to:
- Profound neurological injury
- Very low AADC activity
- Refractory status dystonicus
- Refractory hypotension with bradycardia
Discussion
Disproportionate injury and poor AADC activity may explained by:
- Possible atypical cerebrovascular physiology in AADC deficiency
- Serotonin plays key role in hypoxic response via S2-serotonergic receptors in endothelial vasculature
- Gene therapy does not target serotonergic neurons
- Possible selective vulnerability of gene therapy promoter
- Cytomegalovirus promoter used which has intrinsic hypoxia sensitivity
- Generalized dystonia requires prompt recognition and treatment
- Caution should be exercised with general anesthetics as patients have insufficient catecholamine response
- Poor serotonin production predisposes to hypotension and bradycardia
- Oculogyric crises and dystonic shaking may be confused for seizure
- Incidence of epilepsy in AADC deficiency: 4.5%
- Sleep disorders common in AADC deficiency
- Use melatonin early to help regular circadian rhythm
Exploring Alternative Deep Brain Stimulation Targets for Movement Disorder in Children – A Systematic Literature Review
Introduction
- Deep Brain Stimulation (DBS) has become increasingly prevalent in the management of paediatric movement disorders, with the globus pallidus interna (GPi) serving as the most utilized target.1
- However, limitations exist, including variable responses in genetic versus acquired forms of movement disorder2 and structural damage in the GPi would preclude its use as a target.

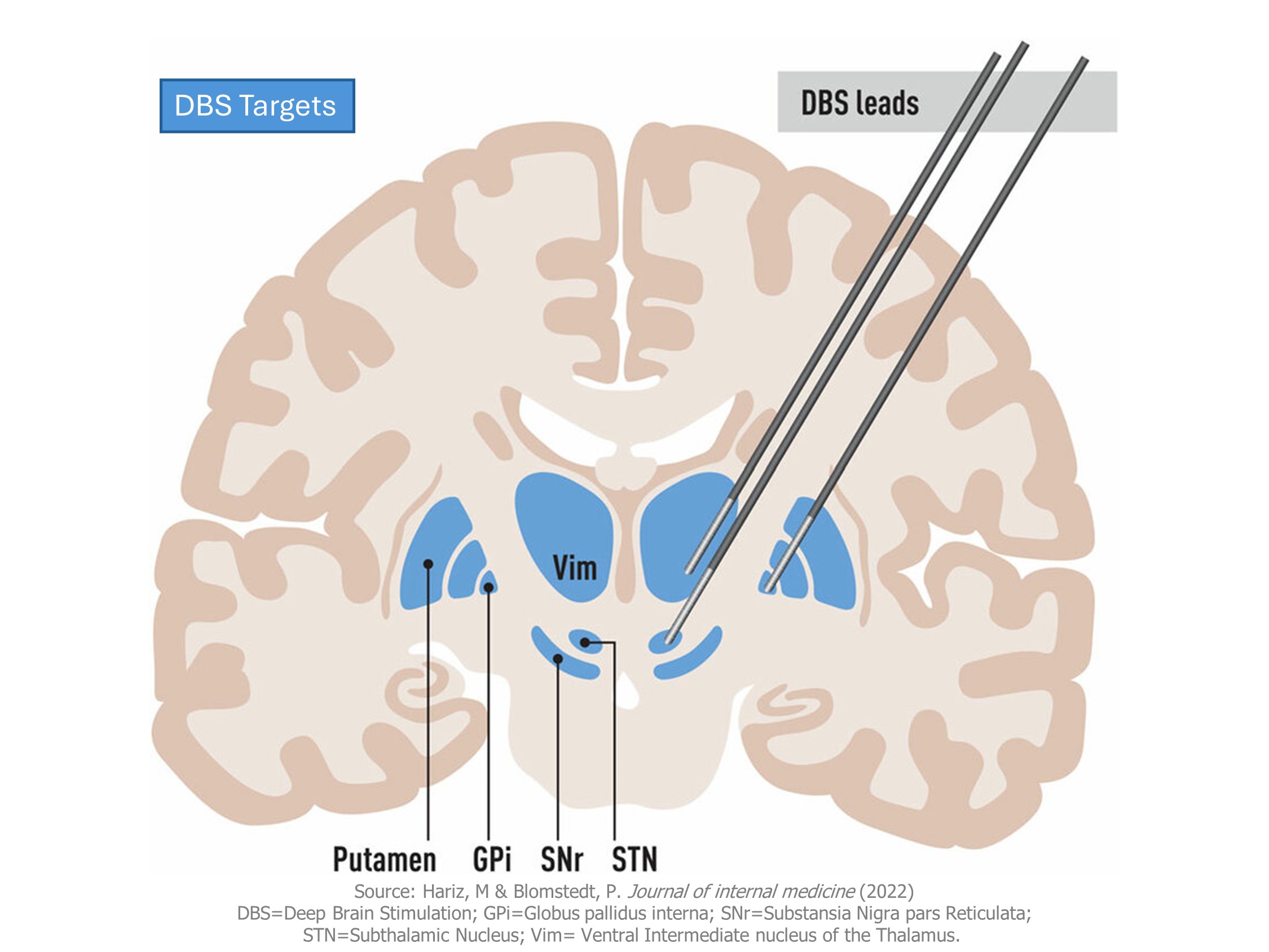
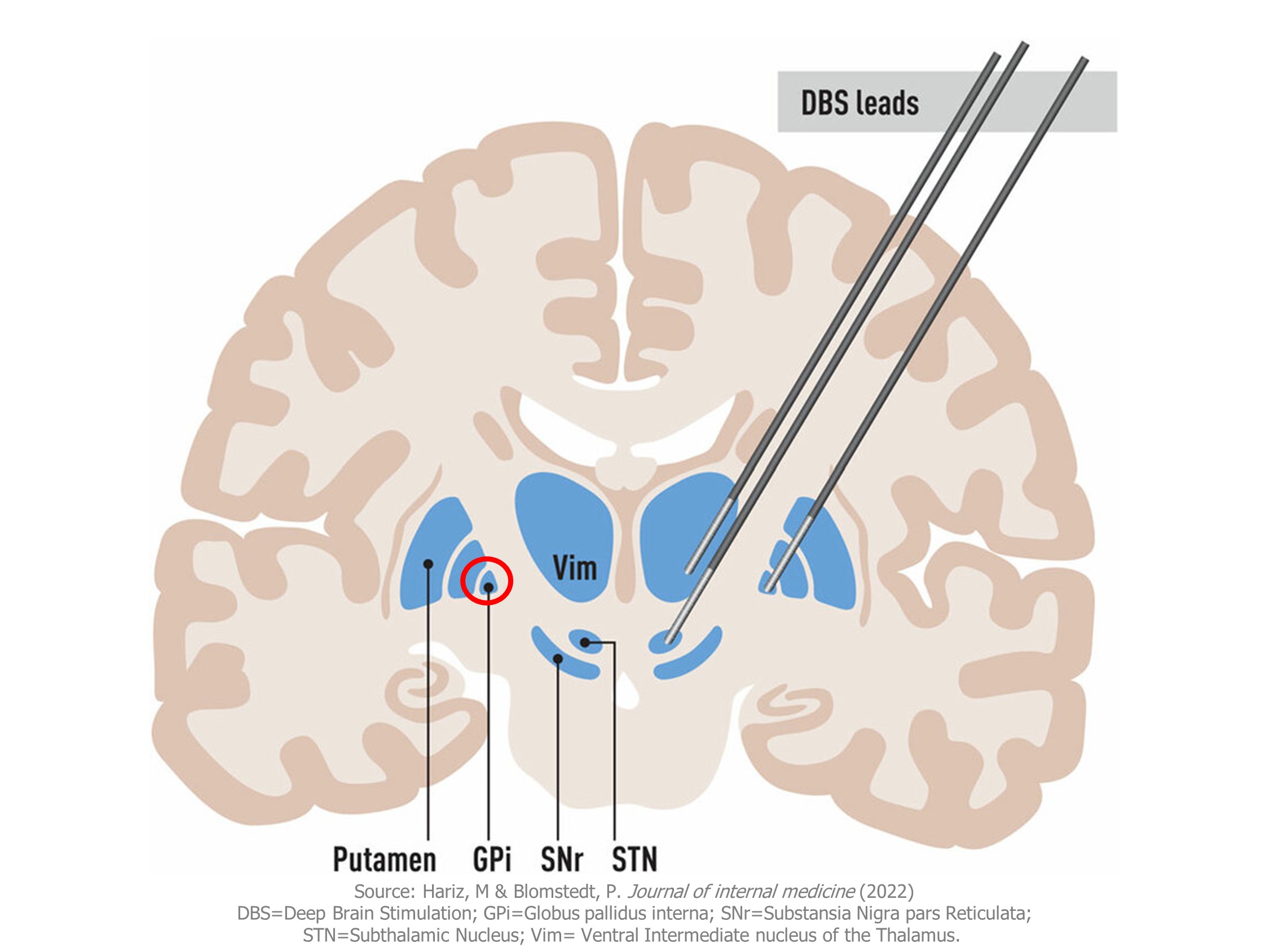

- Given these limitations, there is a pressing need to explore alternative targets. We investigated the application of non-GPi targets in paediatrics through a systematic review.
Methods
We conducted a systematic literature review and extracted individual participant data (IPD).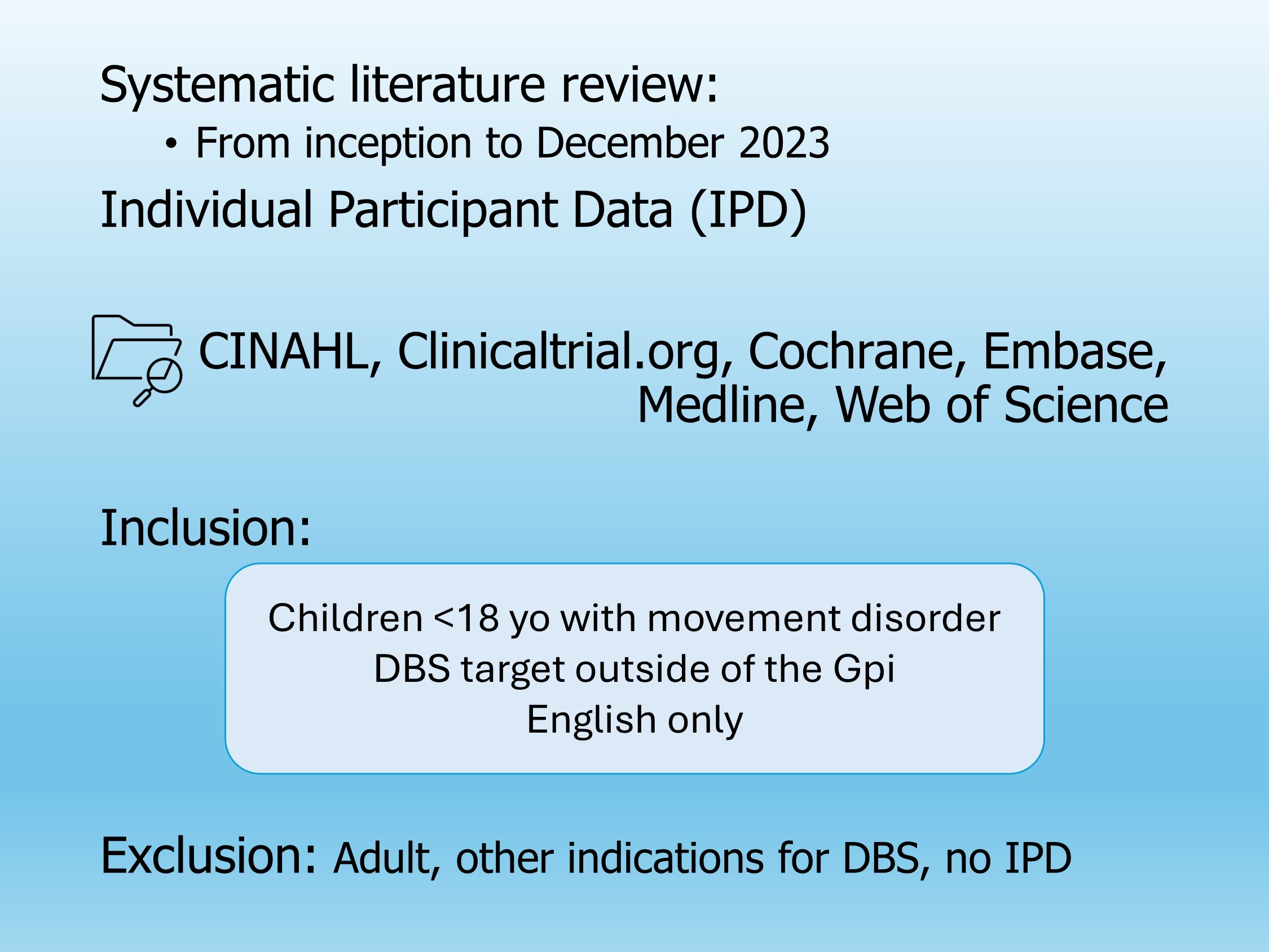
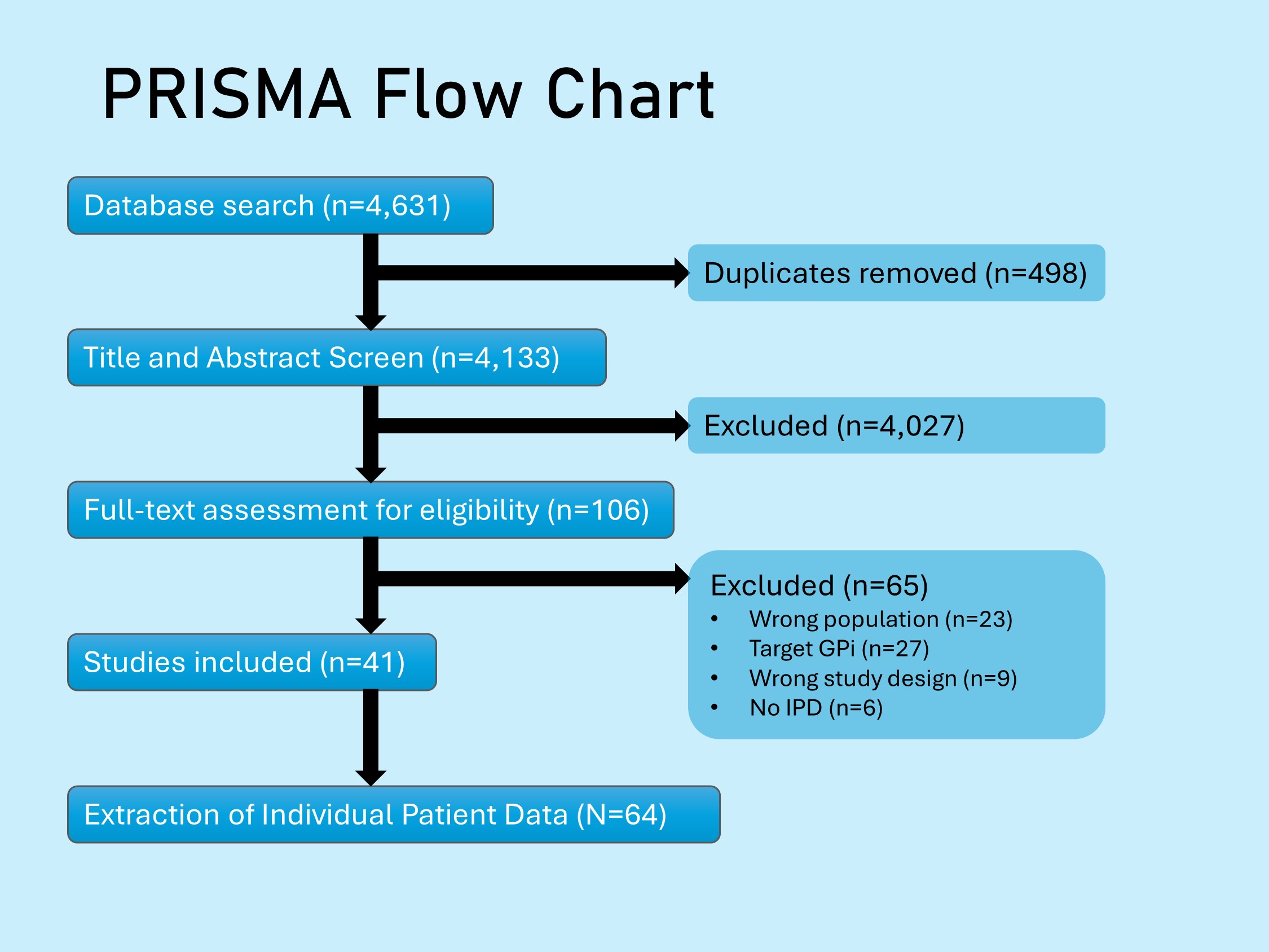
Results
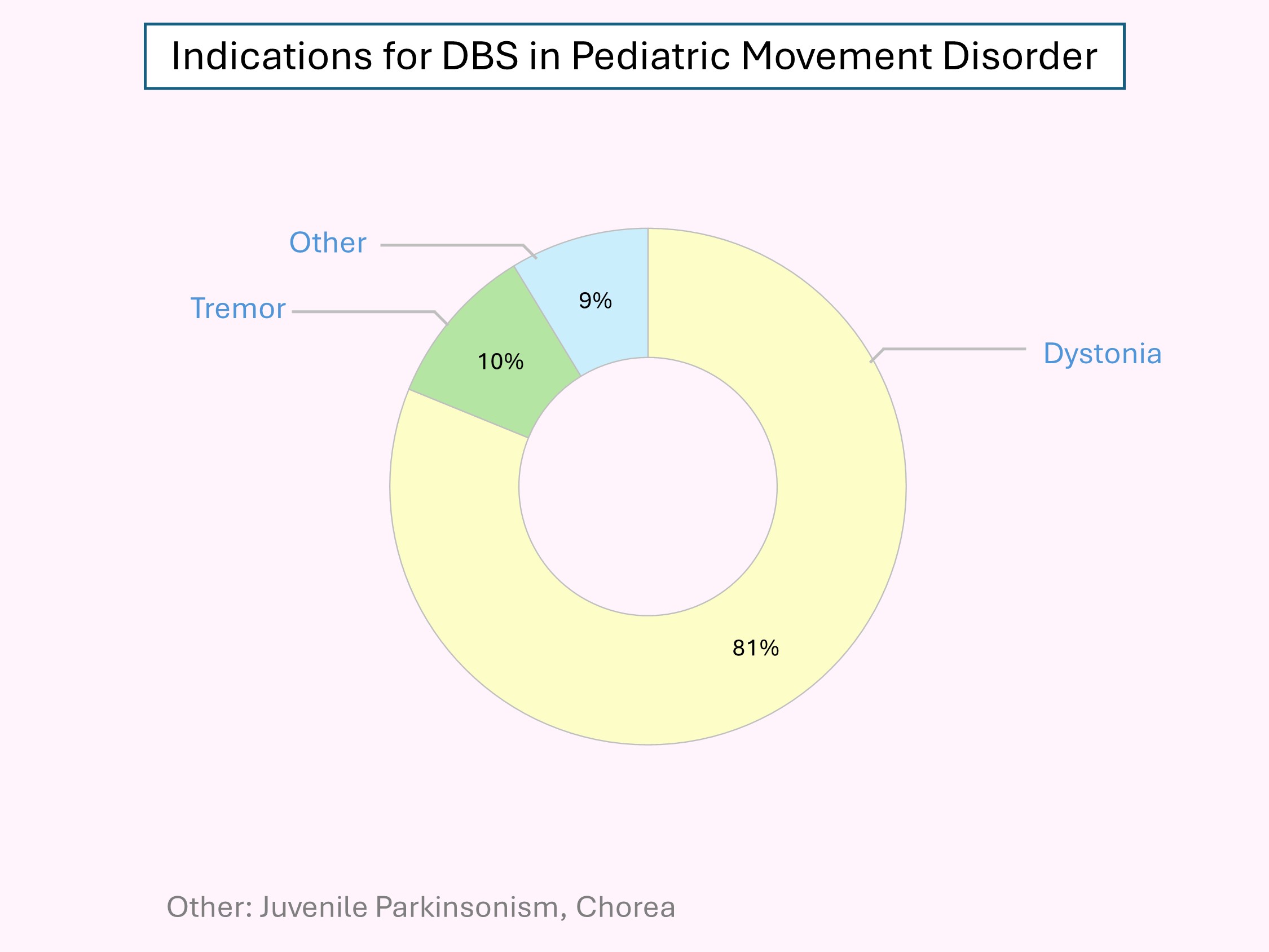
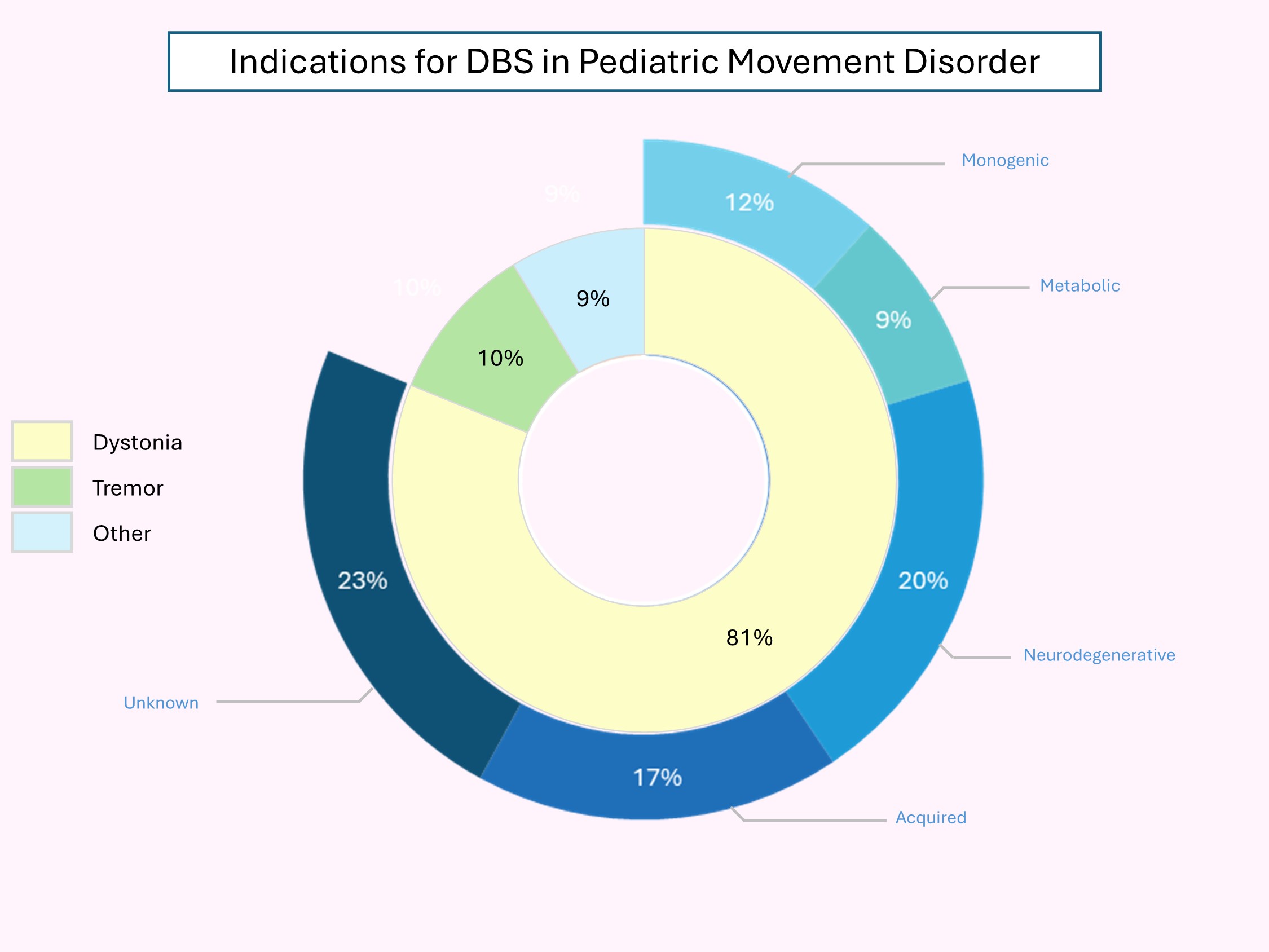

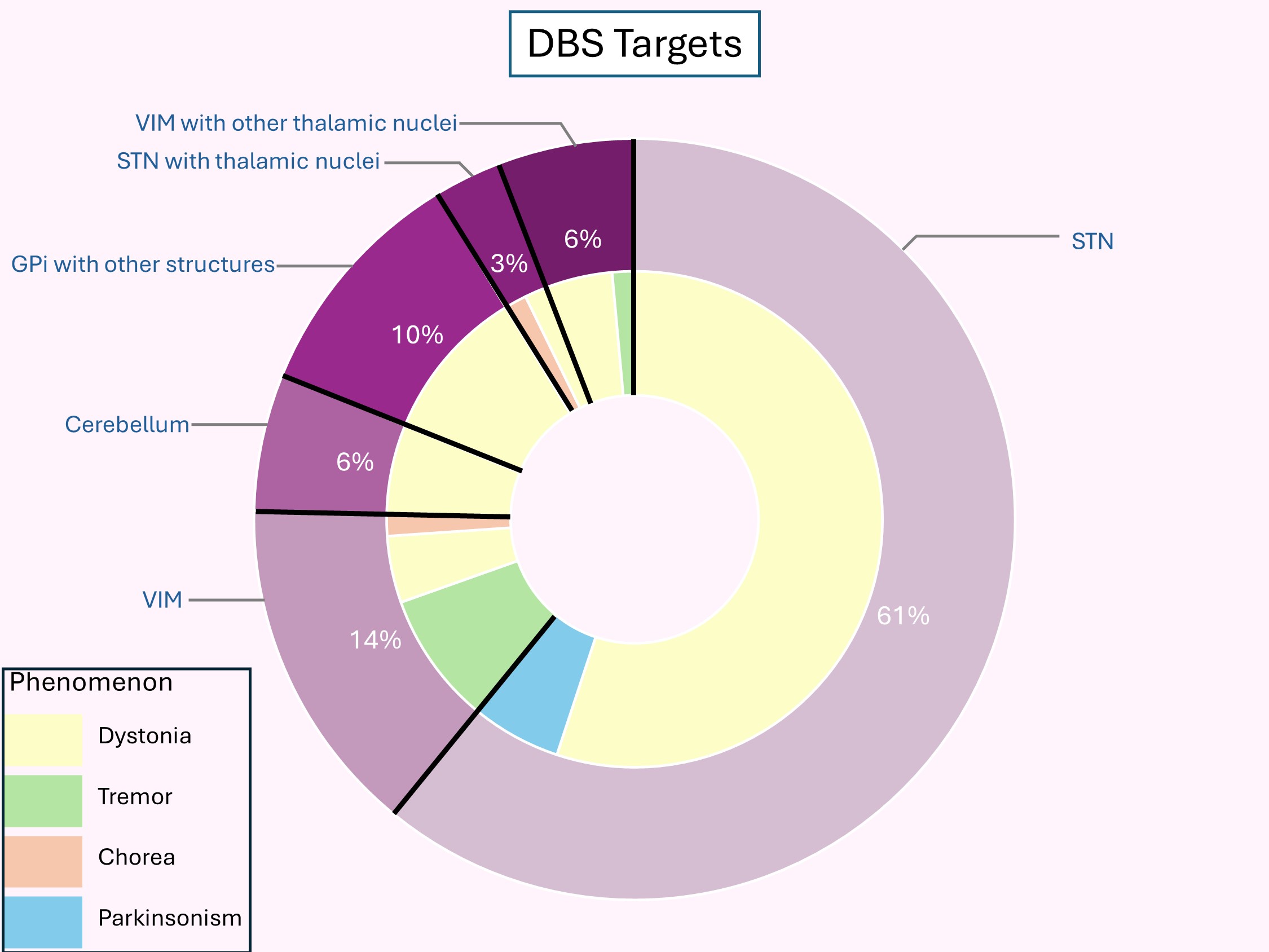
The STN was the most frequent DBS target, in which it was used to treat dystonia. The VIM nucleus was the second most employed target.
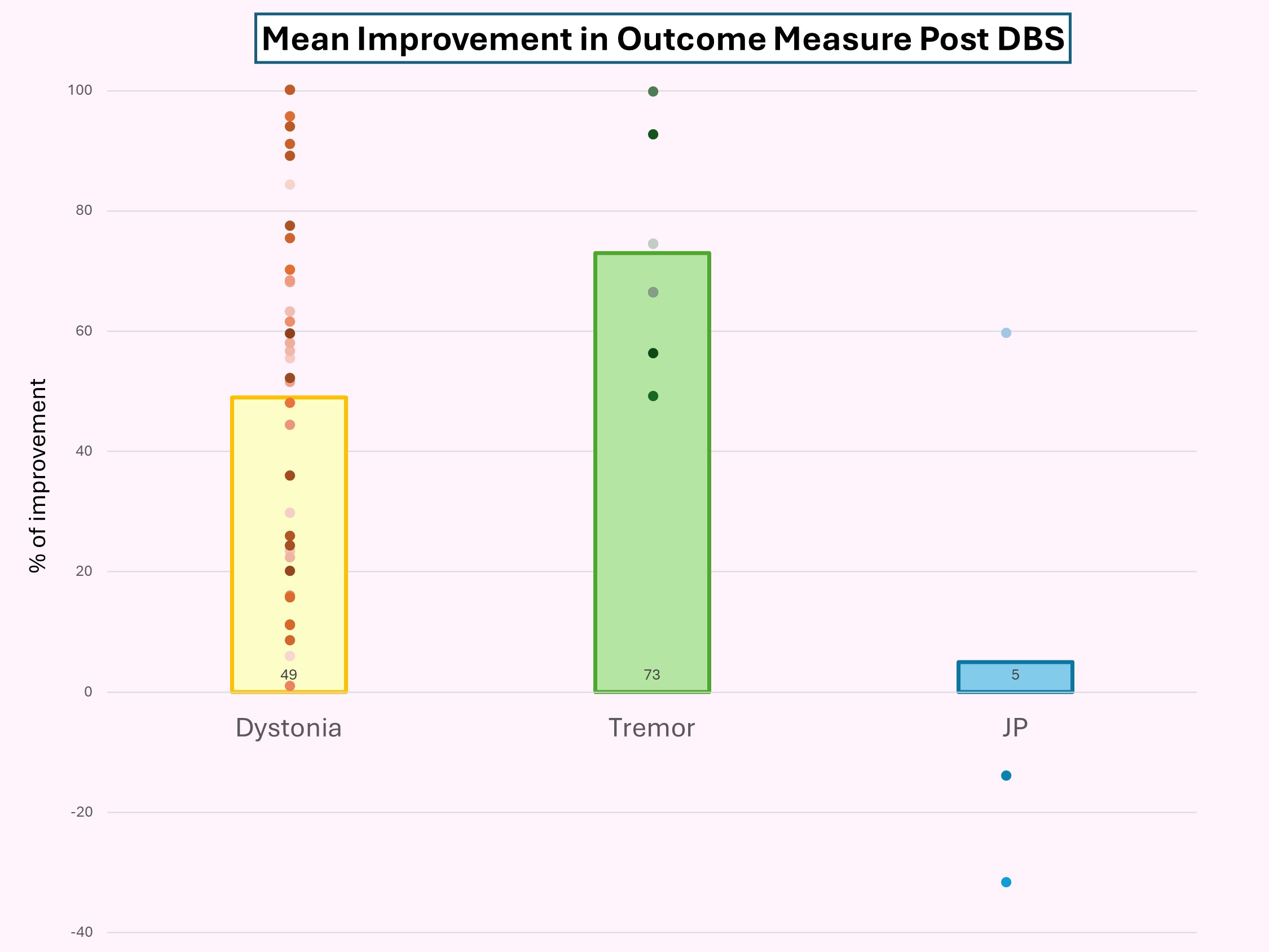
There are 8 dystonia, 1 tremor, and 3 chorea patients who reported subjective improvement after DBS.
Conclusion
The results of non-pallidal targets for dystonia are comparable to GPi-DBS and can potentially be used in children who are not candidates for GPi-DBS. To further validate their effectiveness and safety, larger multi-centre randomized studies are required.
LAUNCH: Longitudinal Analysis of oUtcomes in Neurocritical Care Health

Background
- Children with neurological insult carry the highest risk of death and disability in pediatric and neonatal intensive care units.
- Advances in critical care medicine have decreased mortality, but as a consequence, morbidity is more prevalent.
- There is limited longitudinal outcome data in the pediatric neurocritical care (NCC) population to inform treatment effects and innovation strategies to improve outcomes.
Aims
1. Extensively characterize a cohort of children with critical illness and CNS involvement using standardized outcome measures.
2. Use derived epidemiology to inform strategies for quality improvement studies and improved care guidelines.
1. Extensively characterize a cohort of children with critical illness and CNS involvement using standardized outcome measures.
2. Use derived epidemiology to inform strategies for quality improvement studies and improved care guidelines.
Primary Objective
Demonstrate the utility/benefit of tracking detailed measures of neurodevelopmental outcomes in neurologically complex pediatric patient populations
Secondary Outcome
Explore which patient characteristics increase the risk of poor neurodevelopmental outcomes
Demonstrate the utility/benefit of tracking detailed measures of neurodevelopmental outcomes in neurologically complex pediatric patient populations
Secondary Outcome
Explore which patient characteristics increase the risk of poor neurodevelopmental outcomes
Methods
Phase 1 (retrospective, complete)
Retrospective review of all 929 NCC consults (Alberta Children’s Hospital and Foothills Medical Center) from 2019-2023.

Methods
Phase 2 (prospective, in progress)
Prospectively review clinical records for comprehensive data including (but not limited to) imaging, electrophysiology, invasive ventilation and medications, in addition to development outcomes and quality of life (QoL) assessments
Phase 2 (prospective, in progress)
Prospectively review clinical records for comprehensive data including (but not limited to) imaging, electrophysiology, invasive ventilation and medications, in addition to development outcomes and quality of life (QoL) assessments
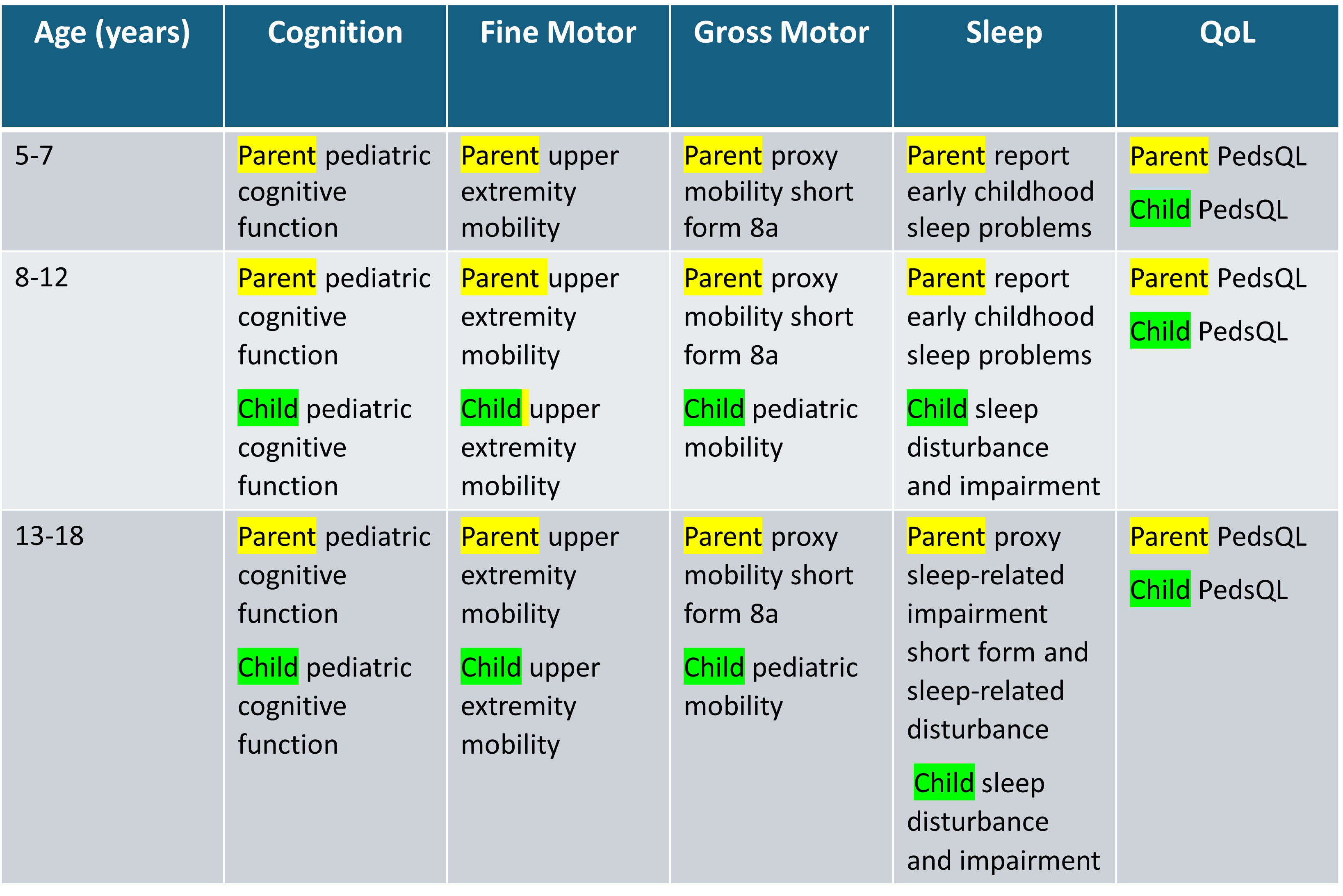
Table 1: Assessments for each domain and corresponding ages (>5 years).
Parental surveys highlighted in yellow, and patient surveys highlighted in green.
Cognitive, fine motor, gross motor and sleep scales all obtained from PROMIS
(Patient-Reported Outcomes Measurement Information System).
Parental surveys highlighted in yellow, and patient surveys highlighted in green.
Cognitive, fine motor, gross motor and sleep scales all obtained from PROMIS
(Patient-Reported Outcomes Measurement Information System).
Results
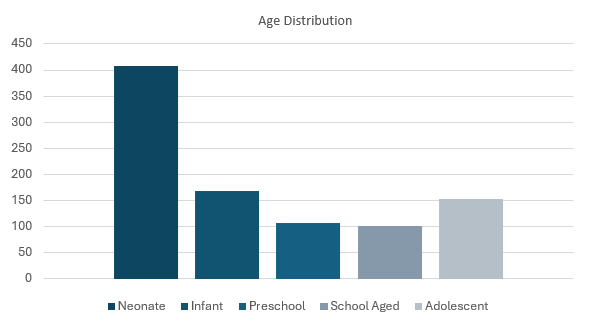
Results
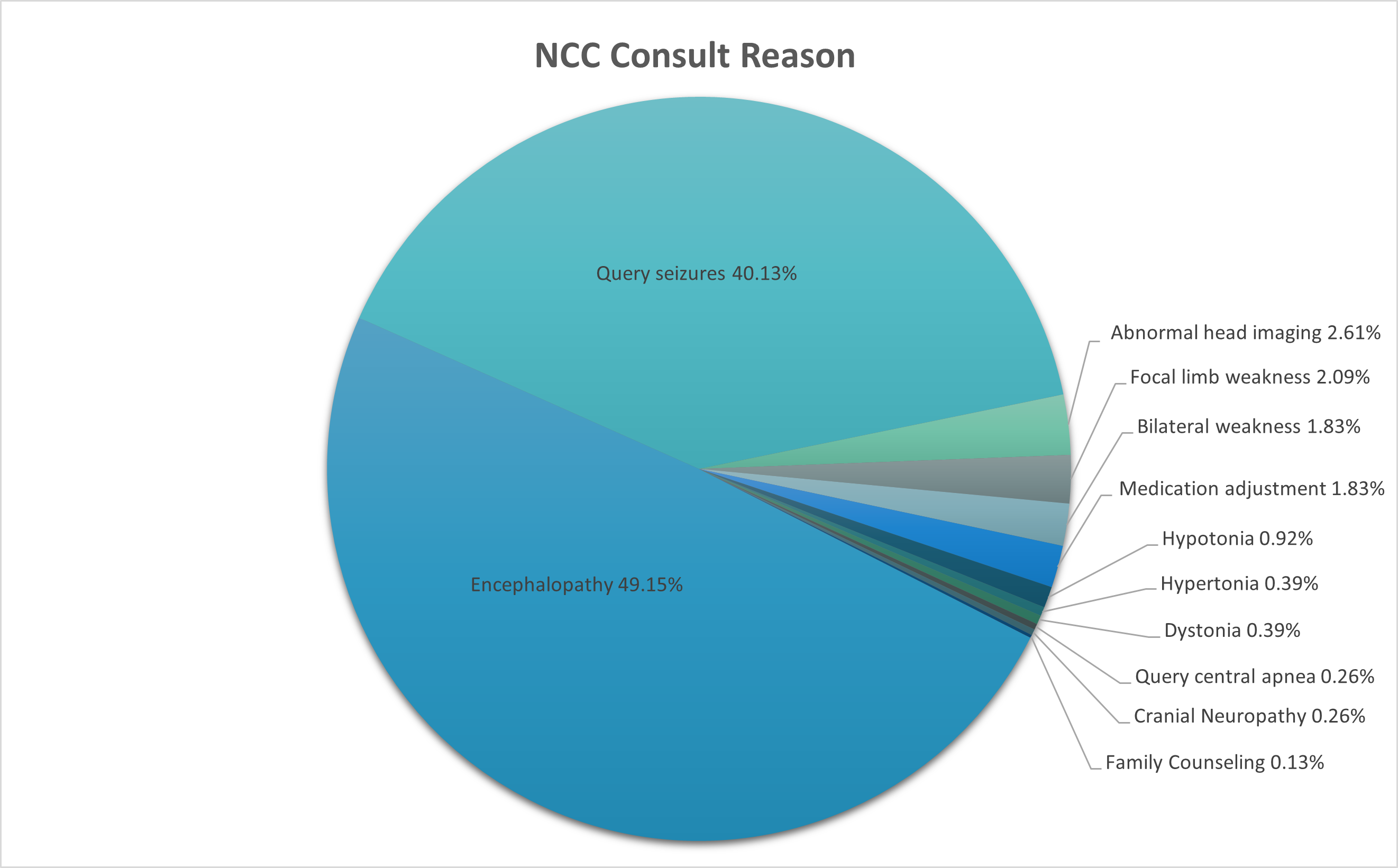
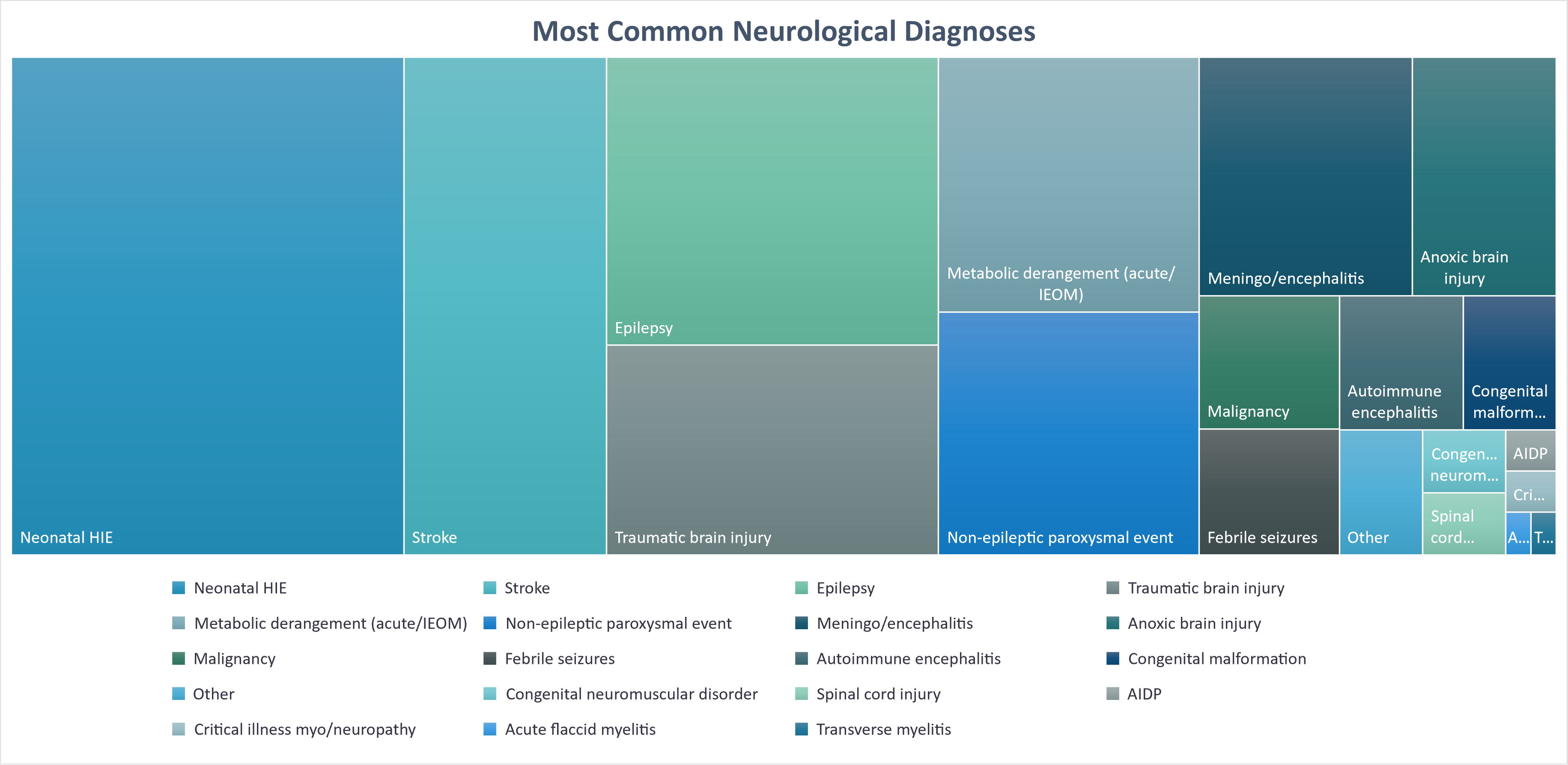
Conclusions
- Our database encapsulates the diversity of NCC patients, enabling cohort-specific studies (e.g., neonatal HIE and ECLS outcomes).
- Program evolution will facilitate high-powered research through large enrollment, comprehensive data capture and longitudinal outcomes.
- Engagement with staff and families will inform treatment and afford evidence-based counseling to families.
Decreased incidence of neuro-autoimmune disorders during COVID-19 pandemic restrictions
Introduction
- A growing body of evidence suggests infections may trigger autoimmunity
- Published data about the epidemiological effects of the COVID-19 pandemic on autoimmune disorders is sparse, and there is a lack of data surrounding recent incidence trends for neuro-autoimmune disorders within the pediatric population
Methods
- Retrospective study assessing incidence of pre-defined autoimmune disorders at the Children's Hospital of Eastern Ontario between October 2017-June 2023
- Queried patient charts in the electronic medical record system Epic to identify subjects diagnosed with a neuro-autoimmune disorder or type 1 diabetes (T1D), serving as a non-neurological autoimmune disorder for comparison
- Charts of patients with a possible neuro-autoimmune disorder were reviewed to check eligibility and identify disease onset; T1D subjects/data were directly extracted
Exclusion criteria: 1) patient had a known pre-existing neuro-autoimmune disorder or T1D; 2) was diagnosed with a disorder that was not autoimmune; or 3) diagnosis could not be confirmed by the treating physician or an expert reviewer
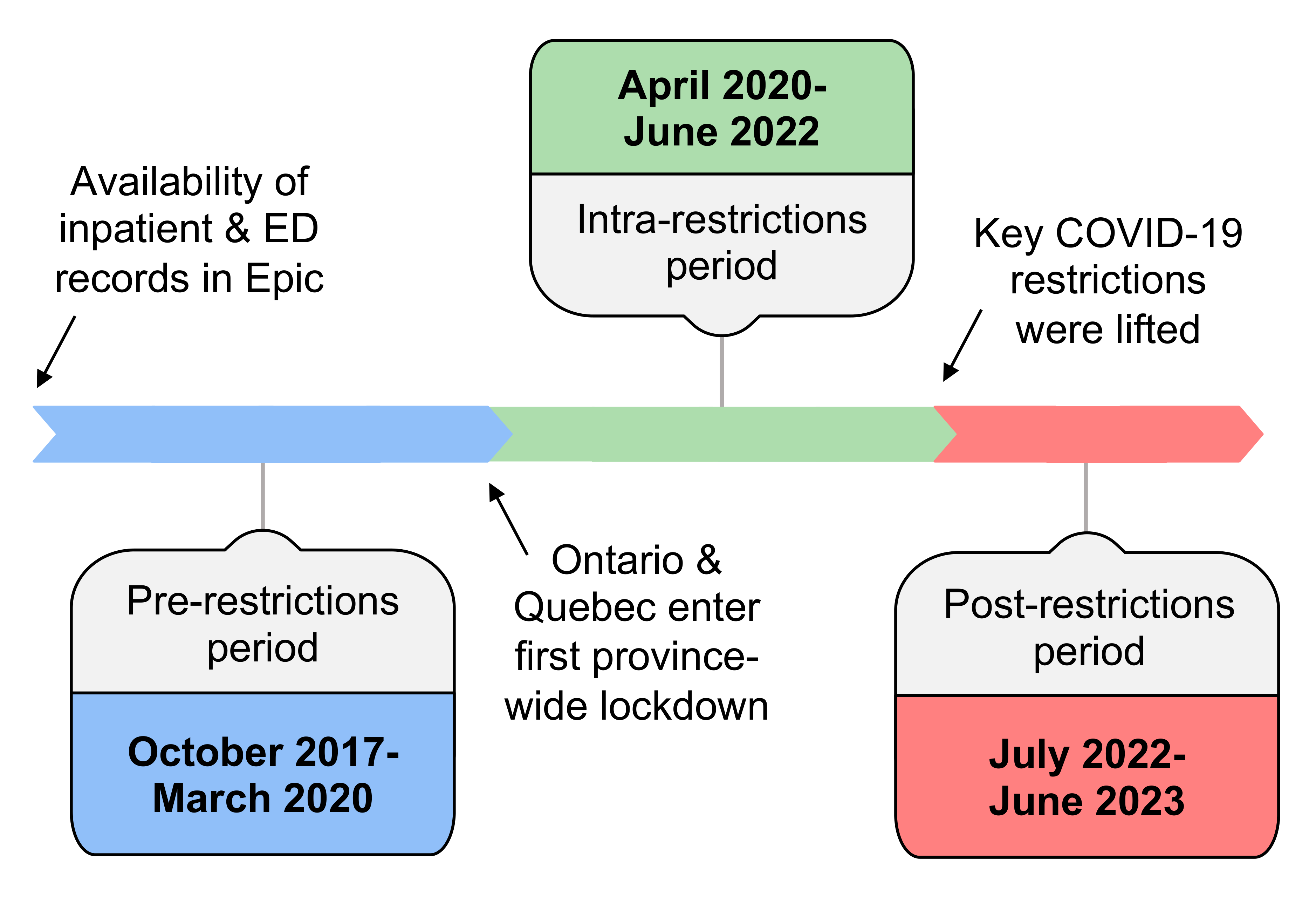
Results
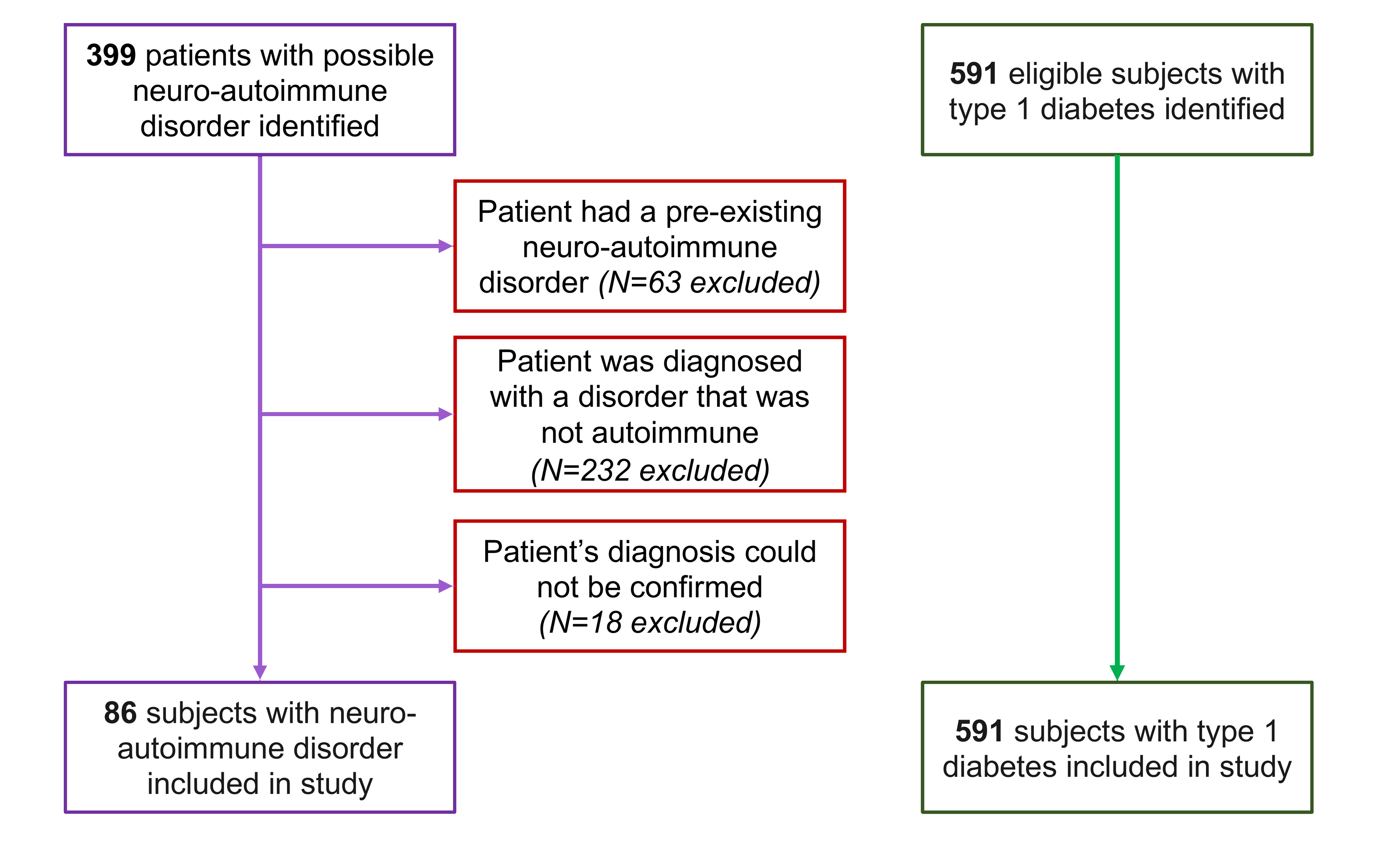
Figure 1: Screening of patient charts and inclusion of study subjects.
Incidence of Neuro-Autoimmune Disorders and Type 1 Diabetes
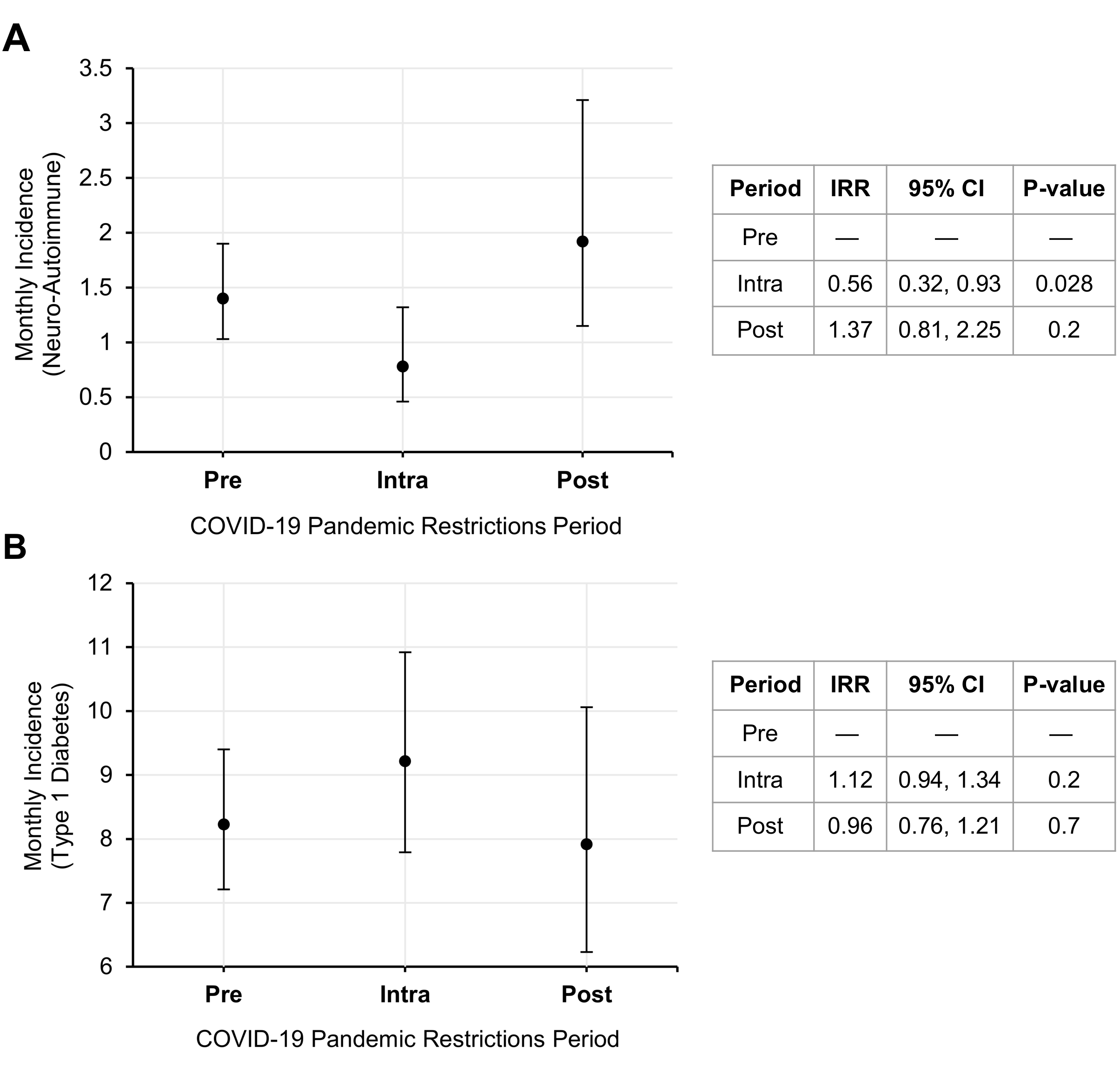
Figure 2: Monthly incidence rates (with standard deviation) of pediatric neuro-autoimmune disorders (A) and type 1 diabetes (B) during periods of COVID-19 pandemic restrictions. ‘Pre’ = pre-pandemic restrictions period (Oct 2017-Mar 2020), ‘Intra’ = intra-restrictions period (Apr 2020-Jun 2022), and ‘Post’ = post-restrictions period (Jul 2022-Jun 2023).
Results
Incidence of Neuro-Autoimmune Disorders by Diagnosis Category
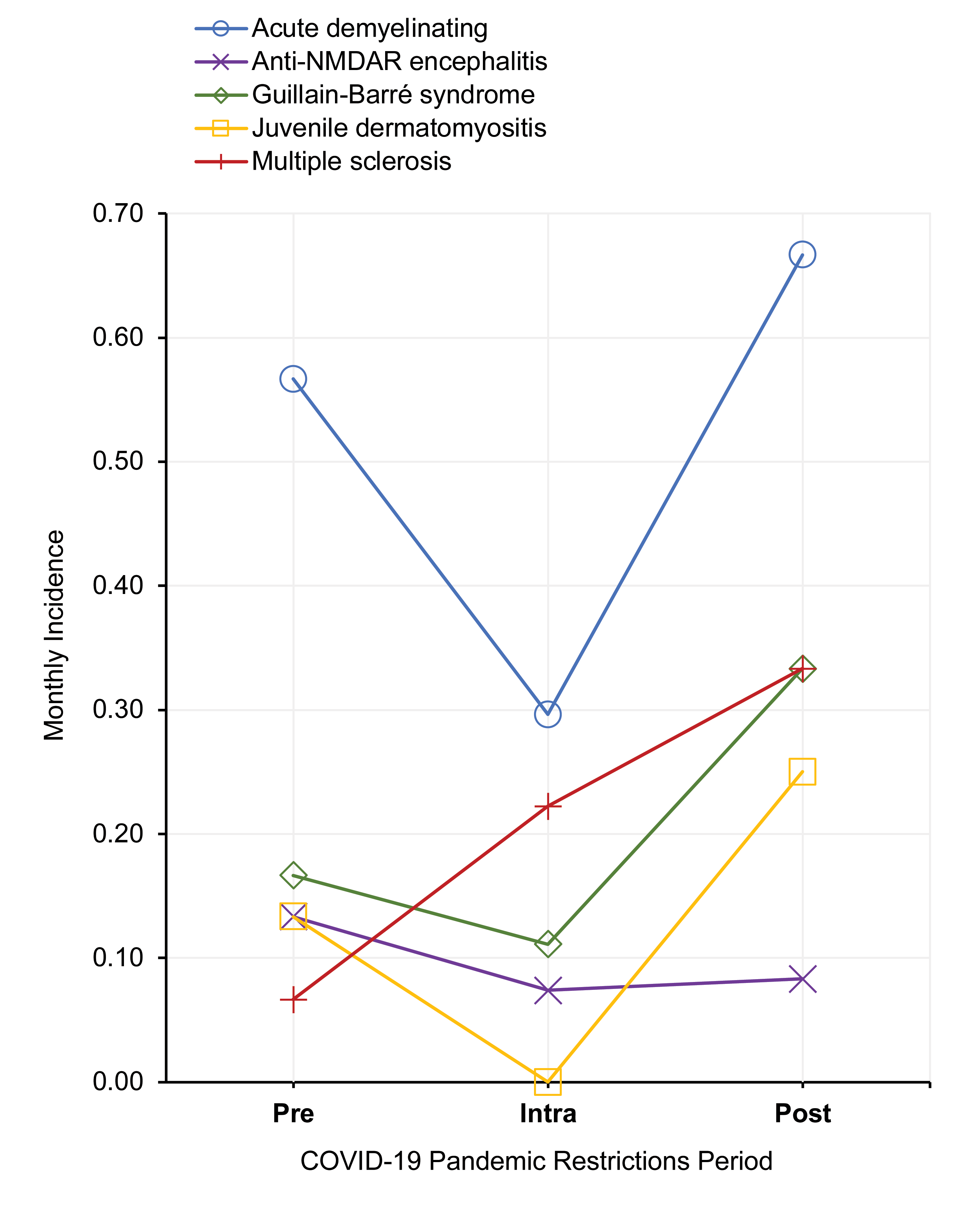
Figure 3: Monthly incidence rates of pediatric neuro-autoimmune disorders (by diagnosis category) during distinct periods of COVID-19 pandemic restrictions. ‘Pre’ = pre-pandemic restrictions period (Oct 2017-Mar 2020), ‘Intra’ = intra-restrictions period (Apr 2020-Jun 2022), and ‘Post’ = post-restrictions period (Jul 2022-Jun 2023). Diagnosis categories included were acute demyelinating disorders (N=33), anti-NMDAR encephalitis (N=7), Guillain-Barré syndrome (N=12), juvenile dermatomyositis (N=7), multiple sclerosis (N=12).
Conclusions
- Incidence of pediatric neuro-autoimmune disorders, but not T1D, decreased during the intra-restrictions period when compared to the pre-restrictions period, possibly attributable to a reduced transmission of infections triggering neuro-autoimmune disorders due to the implementation of public health restrictions
- Grouping subjects by specific diagnosis showed a trend towards decreased incidence during the intra-restrictions period vs. the pre-restrictions period for all groups except multiple sclerosis and T1D, which may reflect a difference in the mechanisms triggering disease manifestation

Next Steps
- Correlate incidence data with COVID-19 infection parameters and conduct an in-depth analysis of subject antecedent infections/vaccinations to clarify the roles these factors may play in influencing pediatric autoimmune disease incidence
- This will be crucial for improving our understanding of potentially modifiable environmental triggers for these diseases
Acknowledgements
- The authors would like to thank Matthew MacDonald, Data Warehouse Analyst at the CHEO Research Institute, for assistance with data extraction
Ethics & Funding
- This study was approved by and conducted in accordance with the regulations of the CHEO Research Institute Ethics Board, and was supported by the Data Warehouse Grant from the CHEO Research Institute
Three-year Longitudinal Health Related Quality of Life in Spinal Muscular Atrophy
Background
Spinal Muscular Atrophy (SMA) is a rare, genetic neuromuscular disorder, diagnosed in infancy or early childhood and is marked by motor neuron degeneration, causing progressive muscle weakness. SMA significantly impacts patients and their families due to its severe manifestations.
Objective
To investigate HRQoL changes in a longitudinal SMA cohort over three years.
Methods
The study exclusively examined HRQoL in pediatric patients aged 6 to 10 years who were diagnosed with SMA.
Patients were recruited through the Canadian Neuromuscular Disease Registry over two time points. The subjects were sent questionnaires for completion in 2017 (T1) and 2022 (T2). Ethics was obtained from Western REB.
HRQoL was evaluated using the PedsQL™ Measurement Model. This model is specifically designed for assessing health-related quality of life in children and adolescents with health conditions, focusing on general health (Generic module) and a neuromuscular disease-specific concerns (NMD module).
Patients were recruited through the Canadian Neuromuscular Disease Registry over two time points. The subjects were sent questionnaires for completion in 2017 (T1) and 2022 (T2). Ethics was obtained from Western REB.
HRQoL was evaluated using the PedsQL™ Measurement Model. This model is specifically designed for assessing health-related quality of life in children and adolescents with health conditions, focusing on general health (Generic module) and a neuromuscular disease-specific concerns (NMD module).
| Patient # | Δ Age | SMA Type | Ambulatory Status | Treatment | Scoliosis | Ventilation |
| 1 | 6 | 2 | Non-ambulatory | Yes | Yes | Non-invasive Bi-PAP |
| 103 | 5 | 3 | Ambulatory | Yes | No | None |
| 2 | 2 | 2 | Non-ambulatory | No | No | Non-invasive Bi-PAP |
| 32 | 1 | 2 | Non-ambulatory | Yes | Yes | None |
| 33 | 3 | 2 | Non-ambulatory | Yes | Yes | Non-invasive Bi-PAP |
| 74 | 6 | 2 | Non-ambulatory | Yes | Yes | None |
| 125 | 3 | 1 | Non-ambulatory | Yes | Yes | Non-invasive Bi-PAP |
| 58 | 4 | 3 | Ambulatory | Yes | No | None |
| Patient # | T1 Generic | T1 NMD | T2 Generic | T2 NMD | Δ Generic | Δ NMD |
| 1 | 45.83 | 58.00 | 52.29 | 55.00 | 6.46 | -3.00 |
| 103 | 39.79 | 67.00 | 78.23 | 81.00 | 38.44 | 14.00 |
| 2 | 53.33 | 78.13 | 66.88 | 72.92 | 13.54 | -5.21 |
| 32 | 51.96 | 81.25 | 37.29 | 66.00 | -14.67 | -15.25 |
| 33 | 52.19 | 77.00 | 51.56 | 83.00 | -0.63 | 6.00 |
| 74 | 54.58 | 56.52 | 67.92 | 78.00 | 13.33 | 21.48 |
| 125 | 46.88 | 32.35 | 52.71 | 80.00 | 5.83 | 47.65 |
| 58 | 52.71 | 38.24 | 67.71 | 83.00 | 15.00 | 44.76 |

Figure 1. Timepoint scores comparison over two timepoints
Acknowledgements: Canadian Neuromuscular Disease Registry
Results
Eight patients completed the HRQoL assessment at two timepoints:
Timepoint 1:
-
Age: 9.0 (SD = 1.73)
-
Generic: 49.66 (SD=5.05)
-
Neuromuscular: 61.06 (SD=18.37)
Timepoint 2:
-
Age: 12.75 (SD = 2.54)
-
Generic: 59.32 (SD=13.08)
-
Neuromuscular: 74.86 (SD=9.88)
Overall Change:
-
Age: +3.75 (SD= 2.54)
-
Generic: +9.66 (SD=15.16)
-
Neuromuscular: +13.80 (SD=23.03)
Conclusions
Between the two timepoints, HRQoL scores in SMA patients improved, suggesting a potential enhancement in quality of life over time. This improvement may indicate the positive impact of medical interventions as most children were on disease modifying treatment.
Anti-HMG Coenzyme A reductase antibody (anti-HMGCR) myopathy: case review of two pediatric patients from a single center

Background
Anti-HMG CoA reductase (anti-HMGCR) myopathy is considered a subtype of immune mediated necrotizing myopathy (IMNM). Patients present with proximal muscle weakness, pain and hyperCKemia. Pertinent imaging shows abnormal T2 and STIR hyperintense MRI signal in affected muscle, and necrotizing fibers on biopsy. Diagnosis is usually confirmed with positive anti-HMGCR antibodies.
Necrotizing anti-HMGCR myopathy is rare in children and not typically associated with statin use or malignancy, as in the adult population. Children often present with skin involvement and less commonly involve the cardiac and respiratory system. Due to the rarity there is often diagnostic delay which can result in a poor response to treatment, often requiring multiple drugs to achieve partial remission.
We present two patients identified at the Children’s Hospital of Eastern Ontario with anti-HMGCR myopathy.
Methods
Retrospective chart review (January 2009 to December 2023) was completed at the Children’s Hospital of Eastern Ontario in Ottawa, Canada. Two cases of anti-HMGCR myopathy were identified. Both patients consented to this study.
Necrotizing anti-HMGCR myopathy is rare in children and not typically associated with statin use or malignancy, as in the adult population. Children often present with skin involvement and less commonly involve the cardiac and respiratory system. Due to the rarity there is often diagnostic delay which can result in a poor response to treatment, often requiring multiple drugs to achieve partial remission.
We present two patients identified at the Children’s Hospital of Eastern Ontario with anti-HMGCR myopathy.
Methods
Retrospective chart review (January 2009 to December 2023) was completed at the Children’s Hospital of Eastern Ontario in Ottawa, Canada. Two cases of anti-HMGCR myopathy were identified. Both patients consented to this study.
Results
Patient A:
A previously healthy, developmentally normal 8 year old boy presented with 1-2 year history of progressive proximal muscle weakness. Initially noted to only be present during activity, however progressed to the point of impacting his ability to go up the stairs and ride a bike. No fatigability or pain, no recent illness or exposure to medication (including steroids and statins). No rash, dysphagia or respiratory concerns. Development, birth, and past medical history were unremarkable. Family history was non-contributory except for a 2nd degree relative with rheumatoid arthritis.
Physical exam: Weakness of neck flexors, as well as symmetric weakness of deltoid, gluteus medius and hip flexors (MRC scale 4- to 4+/5), with a positive Gower sign. The rest of his neurological exam was normal, including distal strength and deep tendon reflexes.
- Childhood Myositis Assessment Scale (CMAS): 33/52
- CK: 4, 923 U/L (normal < 205 U/L)
- Inflammatory markers and metabolic screening: Normal
- Echocardiogram, ECG and pulmonary function test: Normal
- Duchenne Muscular dystrophy (duplication/deletion analysis and gene sequencing): Negative
- Limb-Girdle muscular dystrophy panel: 1 variant of uncertain significance in TTN gene
- Muscle biopsy: Necrotizing muscle fibers and evidence of degeneration (regenerating fibers, split fibers and some centrally-located nuclei).
- Anti-myositis panel returned high positive for anti-HMGCR antibody, which was later found to be > 200 CU (normal <20 CU).
- Full body MRI revealed diffuse muscle atrophy and fatty infiltration in upper/lower extremities, predominantly: teres major muscles, gluteus minimus/intermedius.
Patient A-Coronal MRI short-tau inversion-recover (STIR): Notable for fluid signal intensity between middle and posterior heads of right deltoid
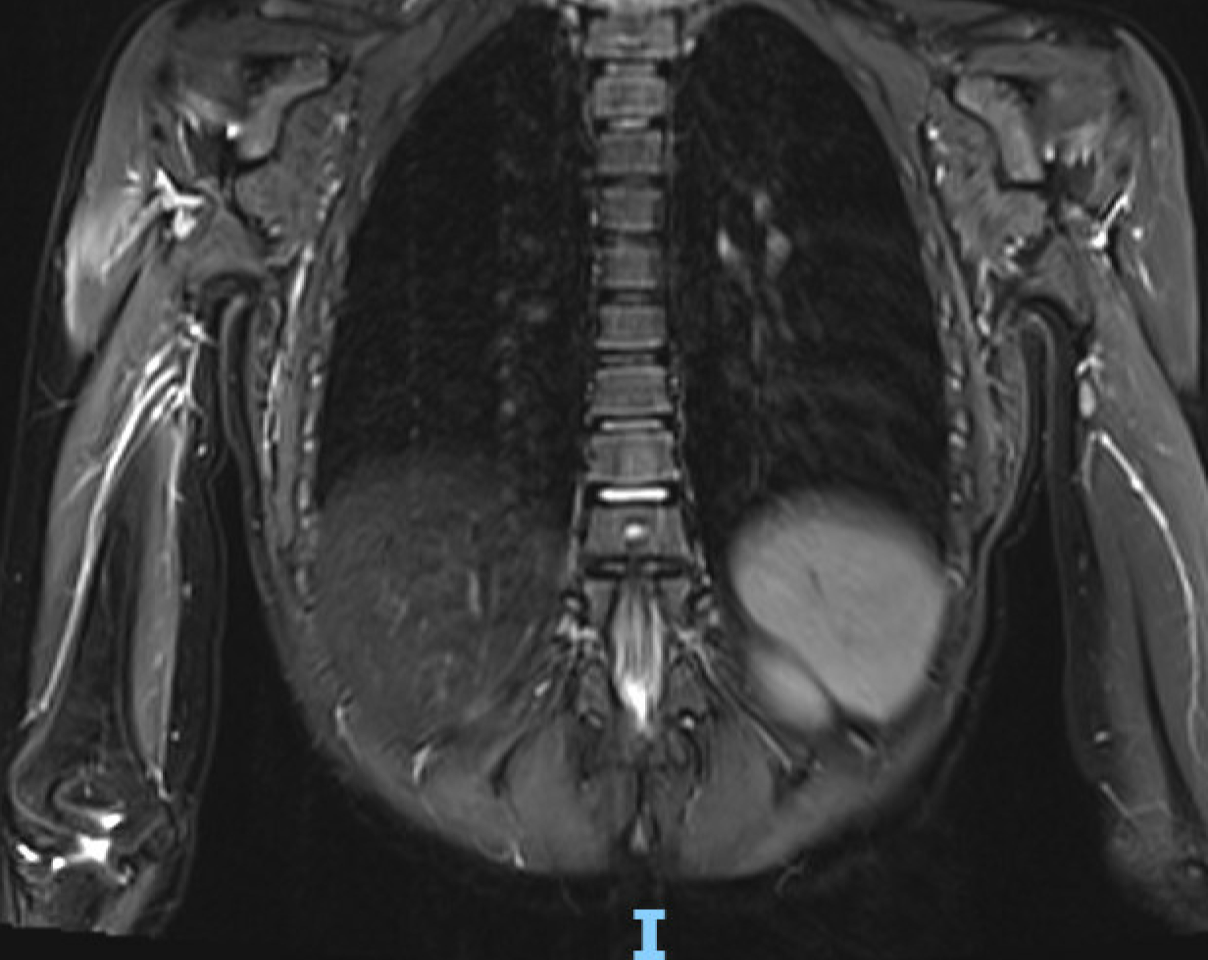
Patient B:
A previously healthy, developmentally normal 8 year old male presenting with a 1 month history of acute onset proximal weakness, after using some heavy weights, and erythematous pruritic rash of the knuckles, knees and elbows. He presented to hospital given ongoing weakness, such that he was unable to use his arms to feed himself and unable to stand from a sitting position or to go up the stairs. No fatigability, no recent illness or exposure to medication (including steroids and statins). No dysphagia or respiratory concerns. Development, birth and past medical history were unremarkable. Family history was non-contributory.
Physical exam: Weakness of neck flexors and symmetrical proximal weakness of upper/lower extremities (MRC 3 to 4+/5), distal strength of the upper extremities were affected (MRC 4/5), but not the lower extremities. The rest of his neurological exam was normal, including deep tendon reflexes.
Physical exam: Weakness of neck flexors and symmetrical proximal weakness of upper/lower extremities (MRC 3 to 4+/5), distal strength of the upper extremities were affected (MRC 4/5), but not the lower extremities. The rest of his neurological exam was normal, including deep tendon reflexes.
- CMAS: 13/52
- CK: 20,185 U/L (normal < 205 U/L)
- Inflammatory markers and metabolic screening: Normal
- Echocardiogram, ECG and pulmonary function test: Normal
- Muscle biopsy: necrotizing myopathy with regenerating myofibers and inflammation.
- MRI of the hips revealed patchy symmetric T2 hyperintense signal involving muscles of the pelvic girdle, anterior and posterior compartment of the thighs bilaterally.
- Anti-myositis panel returned positive for anti-HMGCR antibodies (>550 CU)
He was started on oral prednisone (1mg/kg) with improvement of the CK (9,940 U/L) after 4 weeks, but no functional change (CMAS 9/52). He was subsequently started on IVIG 2g/kg every 2 weeks x3 then monthly and methotrexate weekly, steroids were slowly tapered. He had rapid improvements of CK and strength on IVIG. After 7 months of IVIG, CK were 335 U/L and CMAS was 49/52. CK normalized after 1 year and methotrexate monotherapy was attempted. At last follow up, 20 months from presentation and 8 months off IVIG, CK were trending up (519 U/L) however he remains asymptomatic (CMAS 51/52).
Patient B-MRI and skin findings
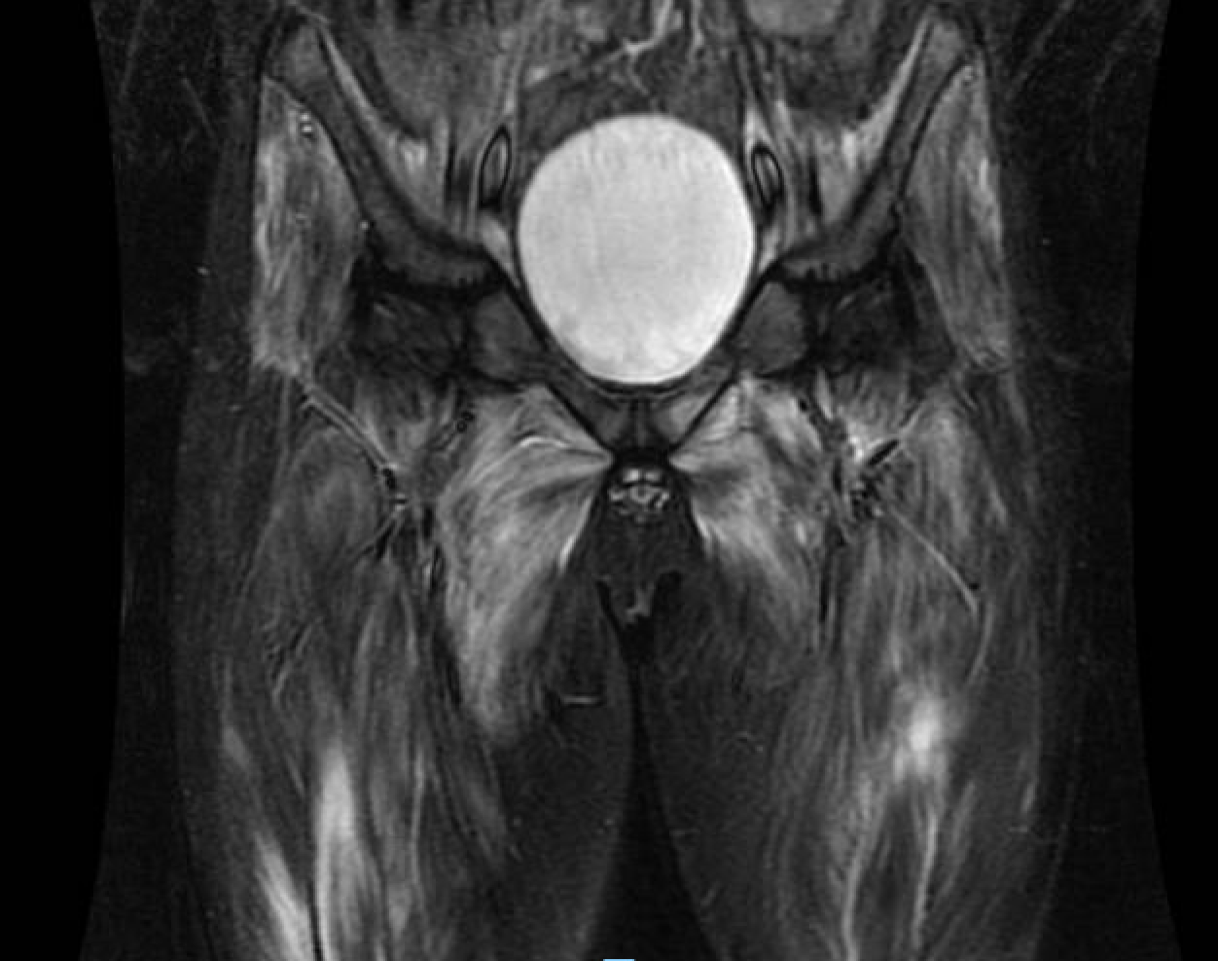


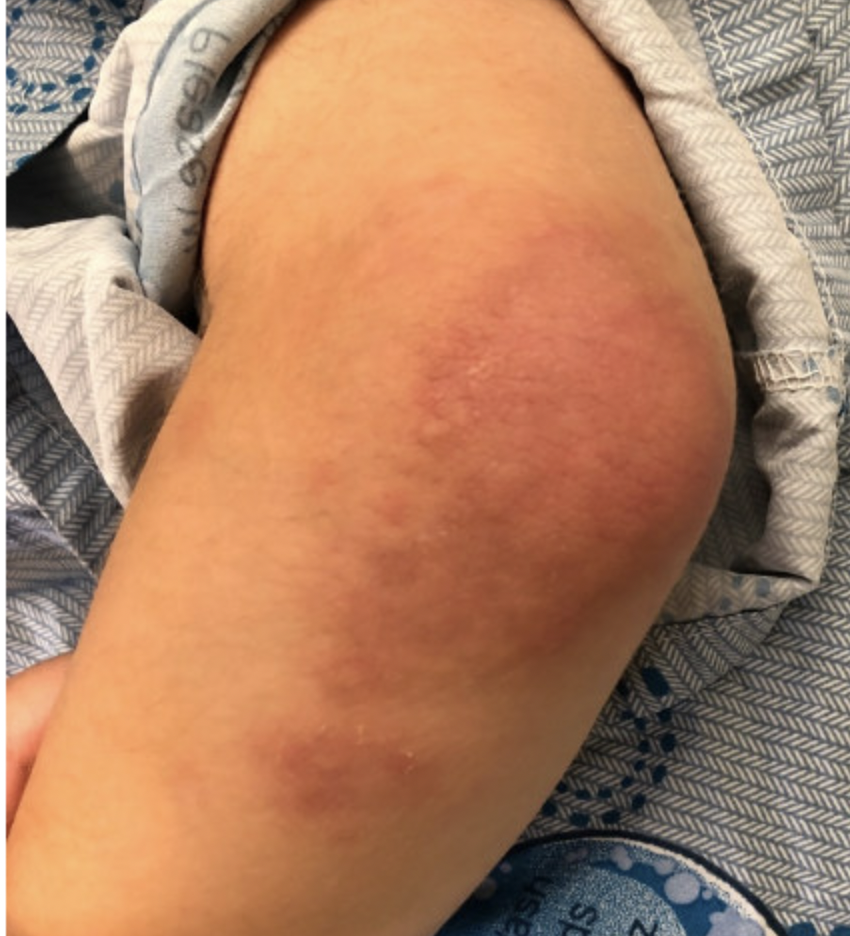

1-Coronal STIR MRI: Hyperintense signal within the anterior compartment of the thigh muscle consistent with muscle edema.
2,3,4- Diffuse confluent erythematous macules over extensor surface of knees (2-3) and elbows (4)
5-Erythematous macular lesions over several MCPs and PIPs of both hands. DIPs are spared. No associated keratosis/hypertrophy.
2,3,4- Diffuse confluent erythematous macules over extensor surface of knees (2-3) and elbows (4)
5-Erythematous macular lesions over several MCPs and PIPs of both hands. DIPs are spared. No associated keratosis/hypertrophy.
Conclusion
Anti-HMGCR antibody myopathy requires prompt diagnosis to obviate muscle necrosis and long-term complications. Delay in therapy can lead to poor response to treatment and permanent muscle damage. We present two patients with very different presentations – one with chronic and the other with acute onset, but both with proximal muscle weakness. Necrotizing myopathy secondary to anti-HMGCR antibodies should be considered in all patients with elevated CK and proximal weakness as this is a treatable condition. Offending agents should of course be discontinued, however these are less commonly found in the pediatric population.
Ambient air pollution and emergency department presentations for pediatric primary headache and seizure disorders in Calgary, Canada

BACKGROUND
Climate change, vehicular traffic, and fossil fuel combustion threaten the health of children globally through direct and indirect mechanisms, such as the exacerbation of ambient air pollution.1,2
Children are more vulnerable to environmental health threats due to: 1) proportionately increased air intake and metabolic rates, and 2) immature physiologic defense mechanisms2,3
Increased ambient air pollutant concentrations are associated with emergency department (ED) visits for episodic and paroxysmal neurologic conditions in adults in the Toronto region of Canada.4,5
The possibility of an association between air pollution and paroxysmal neurologic conditions in children in the Calgary region merits exploration.
Children are more vulnerable to environmental health threats due to: 1) proportionately increased air intake and metabolic rates, and 2) immature physiologic defense mechanisms2,3
Increased ambient air pollutant concentrations are associated with emergency department (ED) visits for episodic and paroxysmal neurologic conditions in adults in the Toronto region of Canada.4,5
The possibility of an association between air pollution and paroxysmal neurologic conditions in children in the Calgary region merits exploration.
OBJECTIVES & AIMS
To determine whether increased ambient air pollutant concentrations are positively associated with the daily count of pediatric ED presentations for headaches and seizures in Calgary, Alberta. It was hypothesized that fine particulate matter (PM2.5) concentrations and the Air Quality Health Index (AQHI) will be positively associated with this outcome.
METHODS
A time-stratified, aggregated exposure, case-crossover ecological study design was employed. Emergency department (ED) cases with seizure- and headache-related diagnoses, aged 1-17 years, and presenting between January 1, 2012-December 31, 2021 to 4 different hospitals in Calgary were identified using diagnostic codes from the National Ambulatory Care Reporting System (REB23-1012). Air pollutant and meteorological data were obtained from Environment and Climate Change Canada, and the National Air Pollution Surveillance program.
Quasi-Poisson regression modeling, incorporating ambient air pollutants, calendrical clusters and meteorological covariates, estimated mean ED visit counts relative to concentrations in air pollutants.
Quasi-Poisson regression modeling, incorporating ambient air pollutants, calendrical clusters and meteorological covariates, estimated mean ED visit counts relative to concentrations in air pollutants.
RESULTS
Descriptive Analysis
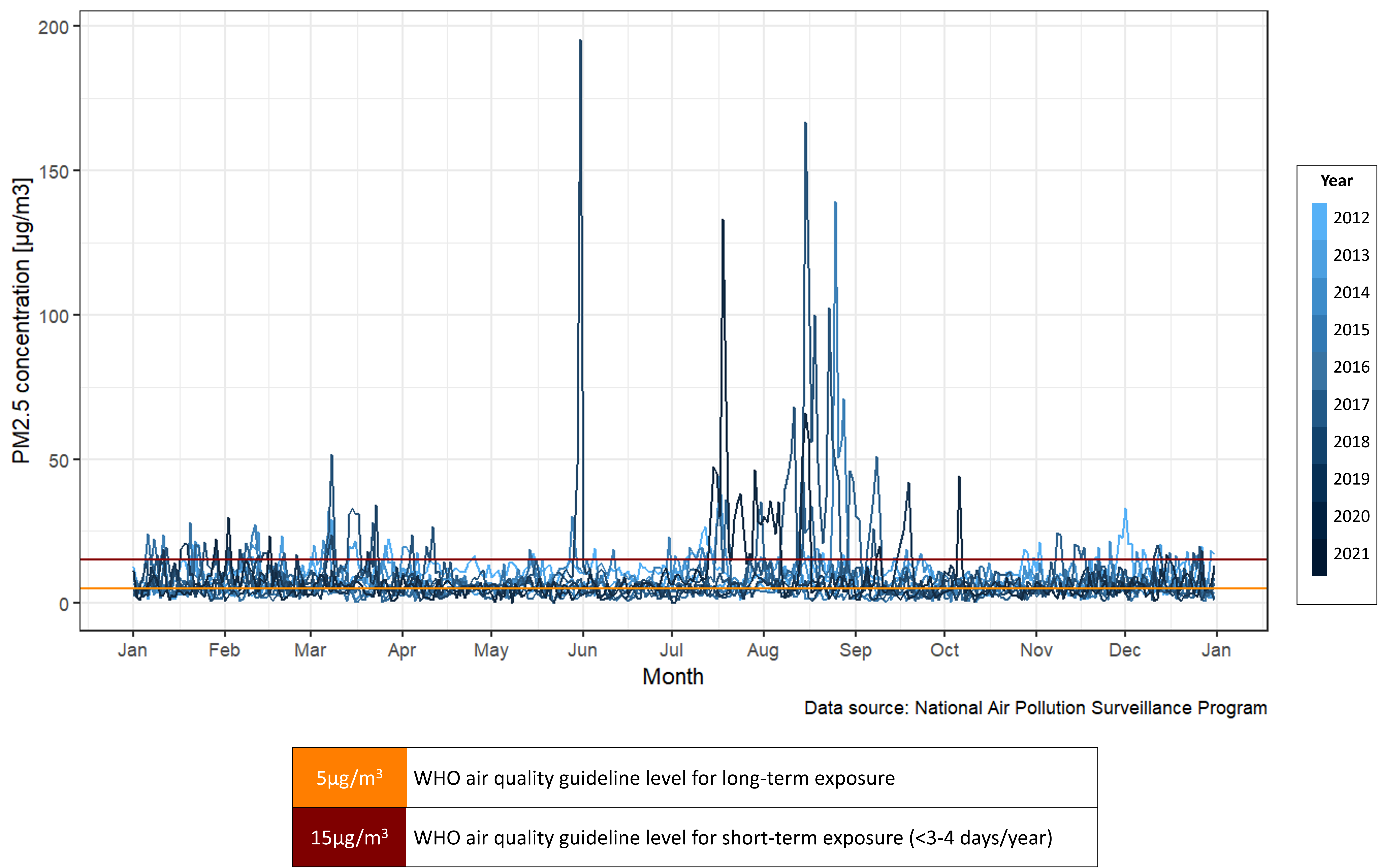
Figure 1. Measured concentrations of ambient fine particulate matter (PM2.5) as 24-hour mean values in Calgary, Canada from 2012 to 2021.
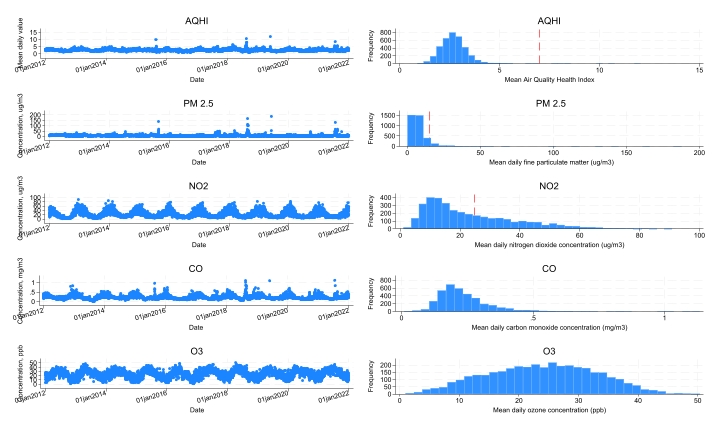
Fig 2. Daily means and frequency distributions of pollutant and AQHI values in the Calgary region, 2012-2021. Red lines indicate boundary for levels exceeding WHO Air Quality Guidelines for protecting public health.
Measured values of PM2.5 (0.23-187.58 ug/m3) and AQHI (0.89-12.05) fluctuated considerably. Case counts varied between 0-15 per day (median=4). Demographic characteristics of cases (n=16449) are summarized in Table 1.
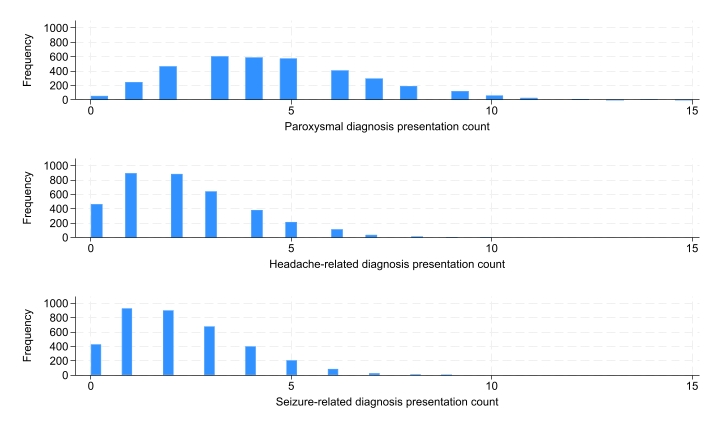
Figure 3. ED count frequency distributions by combined paroxysmal, seizure-related and headache-related disorders.
Positive, statistically significant associations were found in both unadjusted (with a nested calendar structure) and adjusted (temperature, humidity, pressure, with a nested calendar structure) quasi-Poisson regression models. Combined counts increased with a one-unit increase in AQHI (1-day lag and 7-day lag), and a 10ug/m3 increase in PM2.5 (7-day lag only). Seizure-related counts increased with PM2.5 (7-day lag only) and headache-related counts increased with AQHI (1-day lag only).
Exploratory analysis found positive associations between NO2 (1-day lag) with combined and headache-related counts, and between CO (7-day lag) and combined counts.
Table 1. Demographic characteristics of included ED cases.
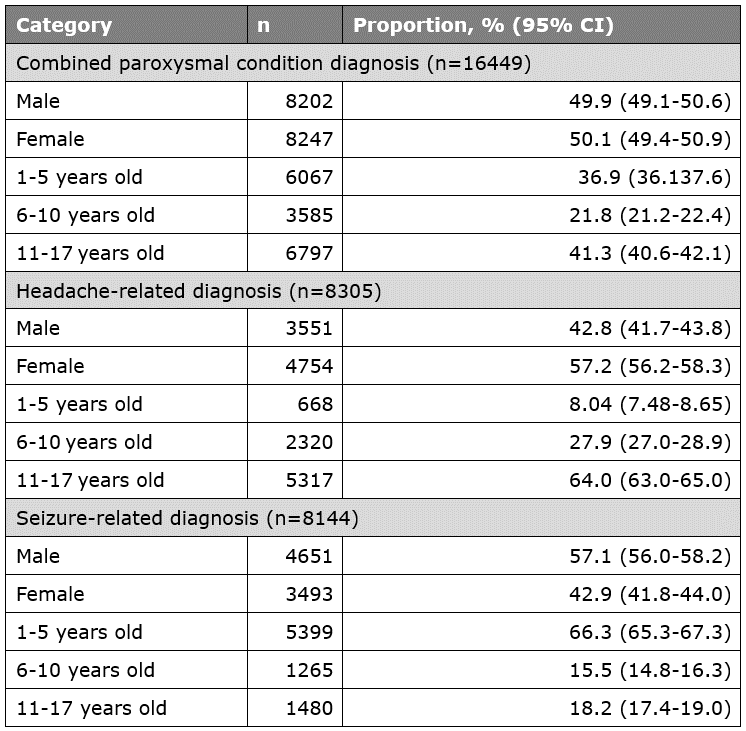
Regression Analyses
Table 2. Results of fully-adjusted quasi-Poisson regression analyses.
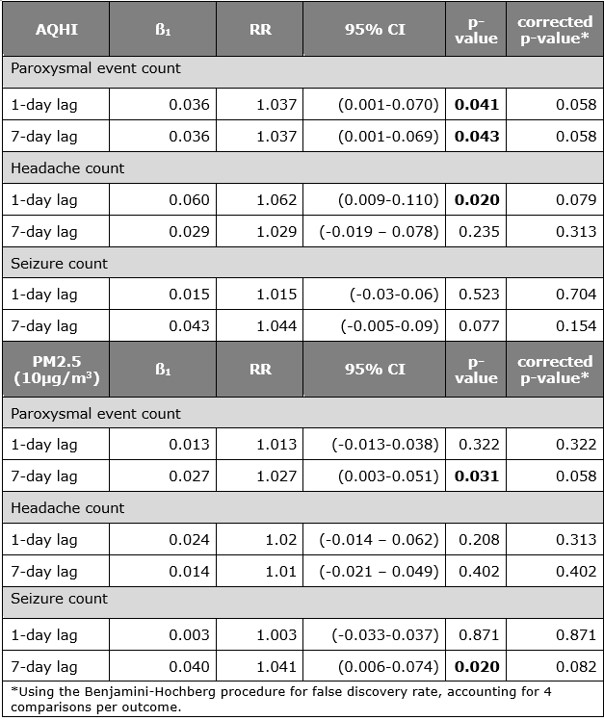
DISCUSSION
The a priori hypotheses were supported by results of this analysis, though statistical significance was lost after correction for multiple comparisons.
Limitations of the study design include potential misclassification of exposure (e.g., related to travel) and outcome (i.e., administrative data usage) as well as selection bias (e.g., urgent care visits not captured). Limitations of the analysis included vulnerabilities to Type I error (mitigated by BH procedure) and Type II error related to a limited sample size.
Future directions will include supervised machine learning to best discriminate key combinations of time lags and pollutants impacting child neurological health, without compromising the dataset’s power.
Limitations of the study design include potential misclassification of exposure (e.g., related to travel) and outcome (i.e., administrative data usage) as well as selection bias (e.g., urgent care visits not captured). Limitations of the analysis included vulnerabilities to Type I error (mitigated by BH procedure) and Type II error related to a limited sample size.
Future directions will include supervised machine learning to best discriminate key combinations of time lags and pollutants impacting child neurological health, without compromising the dataset’s power.
Trofinetide for the Treatment of Rett Syndrome: Long-Term Safety and Efficacy Results From the Open-Label LILAC and LILAC-2 Studies
BACKGROUND
- Rett syndrome (RTT) is a rare, neurodevelopmental disorder that primarily affects females1 and is characterized by a broad set of core symptoms, including irregular breathing, partial or complete loss of acquired spoken language and hand function skills, development of hand stereotypies, gait abnormalities, nighttime behaviors, eye gaze, and seizures2
- Trofinetide, a synthetic analog of glycine-proline-glutamate, became the first FDA-approved treatment for RTT (indicated in adults and pediatric patients aged ≥2 years) on the basis of the results of the 12-week, randomized, placebo-controlled, phase 3 LAVENDER study (NCT04181723)3,4
- RTT is a chronic disorder that requires lifelong treatment5; hence, it is important to investigate the long-term efficacy and safety of trofinetide in patients with RTT
Objective
- To evaluate the long-term safety and efficacy of trofinetide in girls and women with RTT
METHODS
Study design
-
LILAC (NCT04279314) was an open-label extension study of trofinetide in females aged 5–21 years who were previously treated in the LAVENDER study
- The study consisted of a 40-week treatment period and a 30-day safety follow-up period for participants who did not enter LILAC-2
- LILAC-2 (NCT04776746) was a 32-month, open-label extension study of trofinetide in females aged 5–22 years following completion of the LAVENDER and LILAC studies
- In LILAC and LILAC-2, trofinetide was administered following weight-based dosing twice daily (morning and evening, at least 8 hours apart), orally or by gastrostomy tube: 6 g (30 mL), 8 g (40 mL), 10 g (50 mL), and 12 g (60 mL) for body weights of 12–20 kg, >20–35 kg, >35–50 kg, and >50 kg, respectively
Safety assessments
- Adverse events (AEs) in LILAC included treatment-emergent AEs during LILAC and events that began during LAVENDER and were still ongoing at the baseline visit of LILAC
- AEs in LILAC-2 included treatment-emergent AEs during LILAC-2 and events that began during LAVENDER and LILAC and were still ongoing at the baseline visit of LILAC-2
-
Efficacy was assessed during LILAC and LILAC-2 using the Rett Syndrome Behaviour Questionnaire (RSBQ) total score and the Clinical Global Impression–Improvement (CGI-I) score
- RSBQ is a 45-item, caregiver-completed scale (items are grouped into 8 symptom domain subscales) that assesses a wide range of core RTT symptoms6
- CGI-I is a clinician rating of illness improvement or worsening relative to the baseline visit using a 7-point scale with RTT-specific anchors7
RESULTS
Demographics and baseline characteristics
- In the LILAC study, 154 participants were enrolled and treated with open-label trofinetide following the double-blind treatment of trofinetide (n=69) or placebo (n=85) received in LAVENDER
- The LILAC-2 study consisted of 77 participants who were treated with open-label trofinetide and had completed LAVENDER (placebo n=36 and trofinetide n=41) and LILAC
- The mean ages (standard deviation [SD]) in the LILAC and LILAC-2 populations were 11.0 (4.6) and 12.0 (4.4) years, respectively, and the majority were aged between 5 and 11 years (Table 1 in slideshow)
Safety
- The most common AEs in the respective populations of LILAC and LILAC-2 were diarrhea (74.7% and 53.2%), vomiting (28.6% and 19.5%), and COVID-19 (11.0% and 27.3%) (Table 2 in slideshow)
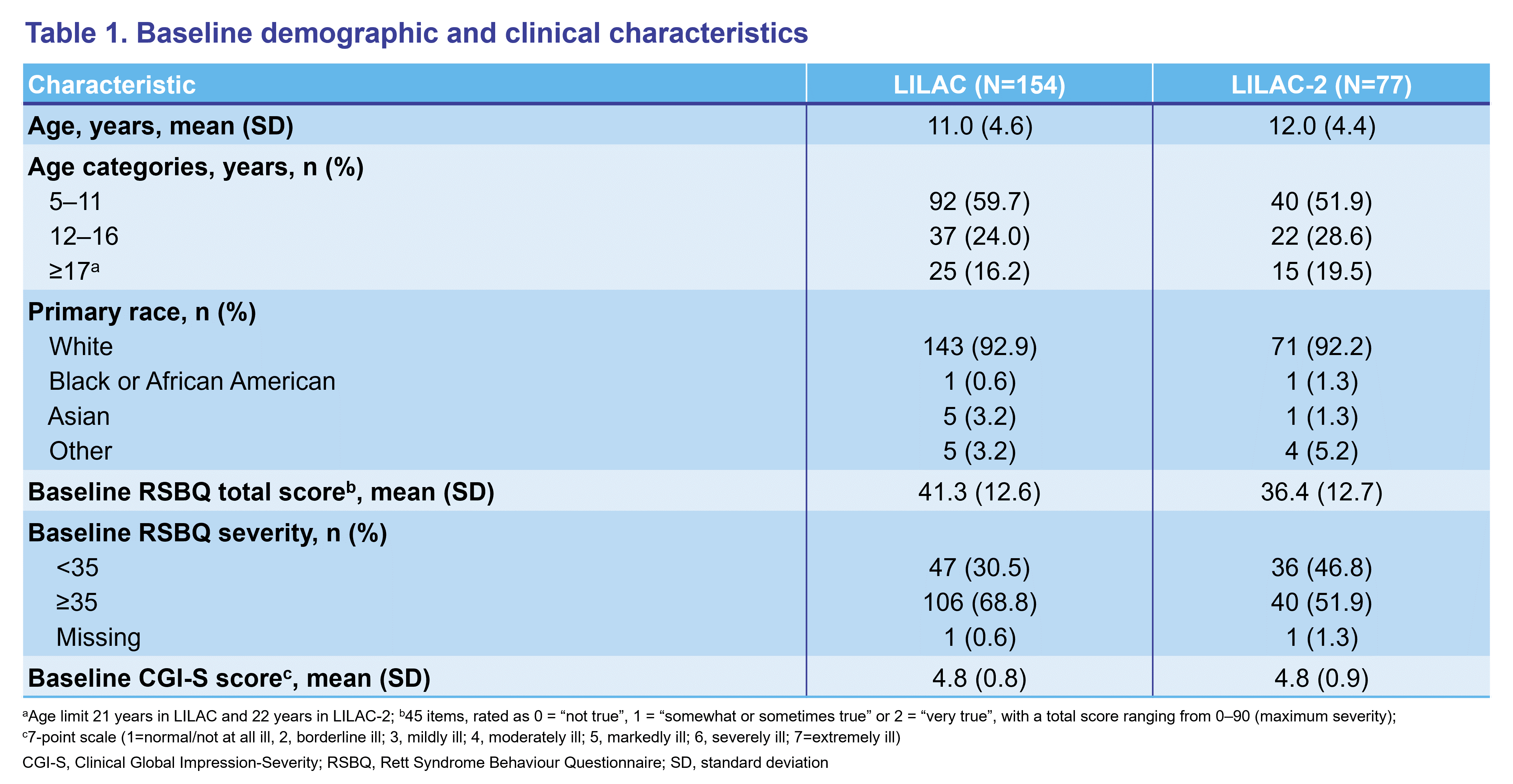
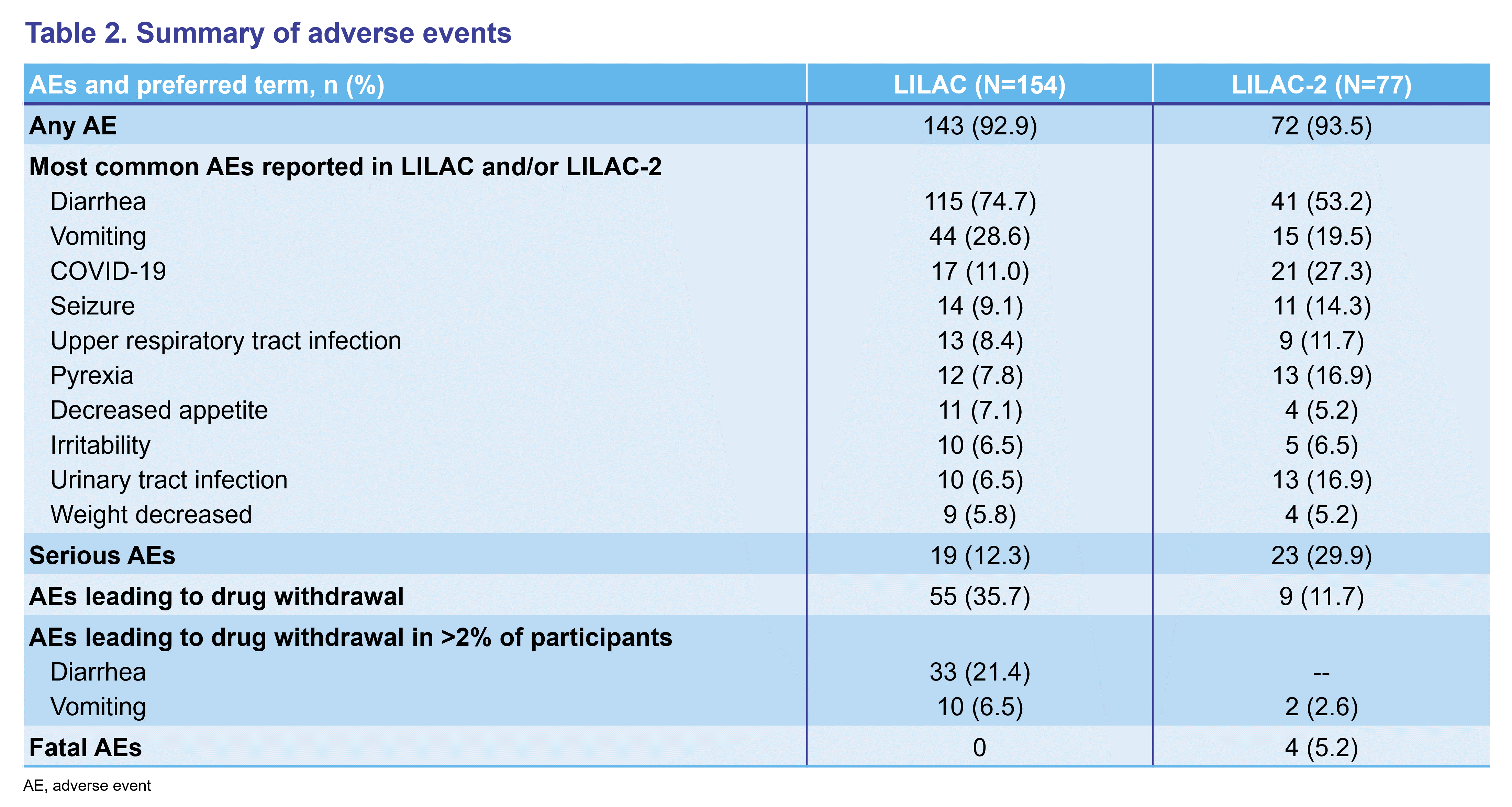
-
Overall, 70 (46.0%) and 16 (20.8%) participants discontinued treatment during LILAC and LILAC-2, respectively
-
AEs leading to study drug discontinuation or termination of study participation were reported in 55 (35.7%) participants in LILAC and 9 (11.7%) participants in LILAC-2
- Diarrhea (21.4%) and vomiting (2.6%) were the most common AEs leading to discontinuation in LILAC and LILAC-2, respectively
-
AEs leading to study drug discontinuation or termination of study participation were reported in 55 (35.7%) participants in LILAC and 9 (11.7%) participants in LILAC-2
-
Four participants died during the LILAC-2 study
- Cause of death was reported as cardiac arrest (n=1), gastric ulcer hemorrhage (n=1), sudden unexplained death in epilepsy (n=1), and vomiting and aspiration (n=1) following surgical placement of gastrostomy tube
- Deaths were not considered related to study drug by the investigator or sponsor
Efficacy
-
In LILAC, treatment with trofinetide for 40 weeks resulted in improved RSBQ and CGI-I scores
- The mean (standard error [SE]) change in the RSBQ from the LAVENDER baseline to Week 40 in the LILAC study was −7.3 (1.6) and −7.0 (1.6) for participants treated with trofinetide and placebo in LAVENDER, respectively, and was −7.1 (1.1) in the LILAC total group (Figure 1A)
- Mean (SE) CGI-I scores compared with the LILAC baseline at Week 40 were 3.1 (0.1) and 3.2 (0.1) for patients treated with trofinetide and placebo in LAVENDER, respectively, and the score in the LILAC total group was 3.1 (0.1) (Figure 1B)
-
In LILAC-2, treatment with trofinetide for up to 32 months resulted in continued improvement in RSBQ scores and sustained improvement in CGI-I scores
- The mean (SE) change in the RSBQ from the LAVENDER baseline to Week 104 in the LILAC-2 study was −9.8 (3.4) and −13.8 (3.6) in participants treated with trofinetide and placebo in LAVENDER, respectively, and was −11.8 (2.5) in the LILAC-2 total group (Figure 1A)
- The mean (SE) CGI-I score relative to LILAC baseline at Week 12 was 3.2 (0.1) and 3.0 (0.2) for participants treated with trofinetide and placebo in LAVENDER, respectively; the score in the LILAC-2 total group was 3.1 (0.1) (Figure 1B)
Figure 1. RSBQ (A) and CGI-I (B) scores in LILAC and LILAC-2
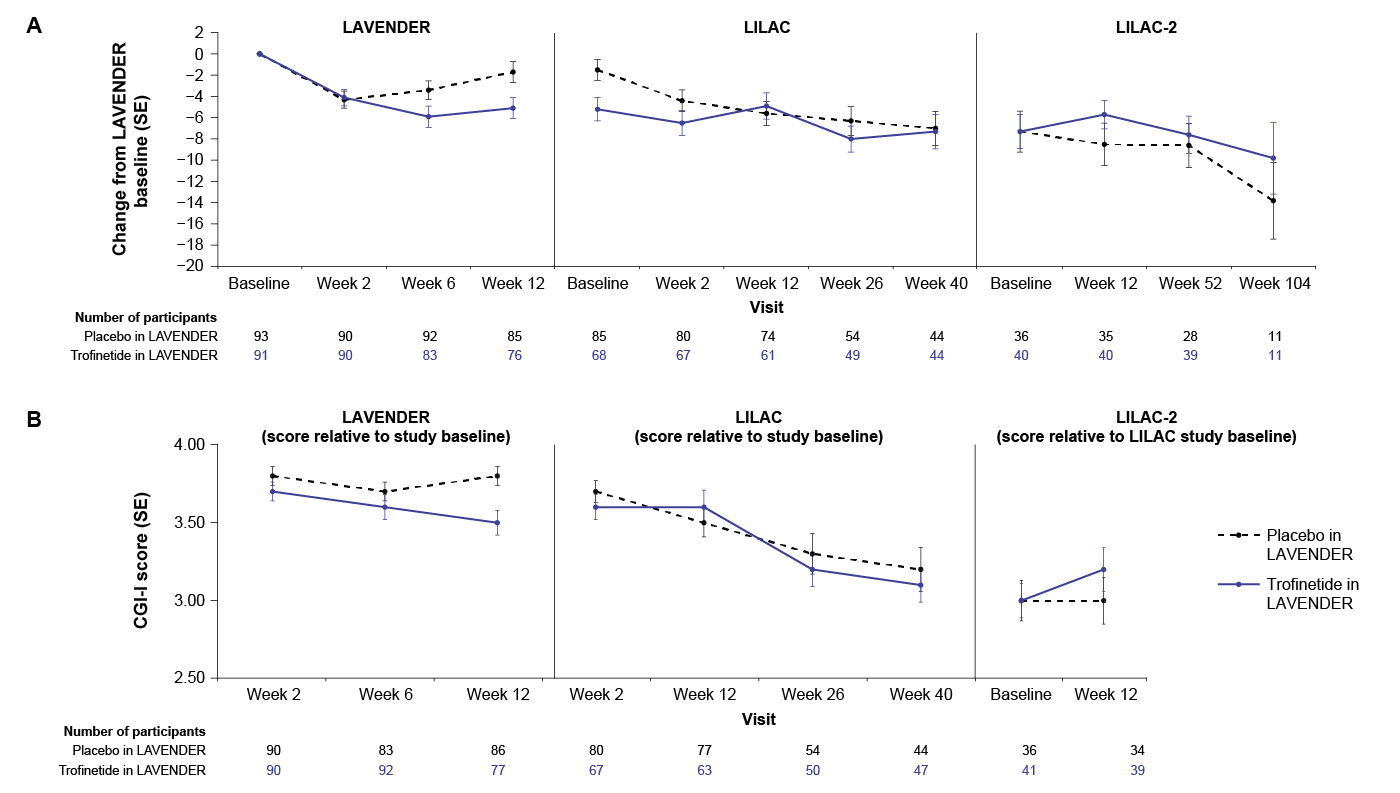
CONCLUSIONS
- Symptoms of RTT continued to improve in LAVENDER study participants following open-label trofinetide treatment for 40 weeks in LILAC and up to 32 months in LILAC-2
- No new safety concerns were reported in LILAC and LILAC-2, and the safety profile of trofinetide in the LILAC studies was consistent with LAVENDER
Key Messages:
- Child and adolescent WE is underrecognized and should be considered in patients at risk of thiamine deficiency for ≥2 weeks
- In pediatrics, deficient intake, malabsorption and altered thiamine metabolism are the main non-alcohol-related causes of WE
- Thiamine IV 200-500mg TID (initially) is safe, so when risk factors for thiamine deficiency are present, treat without hesitation before giving carbohydrates
Introduction:
- The incidence of pediatric WE is estimated to be similar to that of adults1
- Only 16% of pediatric Wernicke’s Encephalopathy (WE) present the classic triad of acute encephalopathy, oculomotor dysfunction, and ataxia2
- The main causes are decreased intake (anorexia nervosa, psychiatric illnesses, autism, parenteral nutrition), malabsorption (gastrointestinal surgery, colitis, food allergy), and altered thiamine metabolism (leukemia, SLC19A3 mutation) as opposed to alcohol related WE, which is rare1
- Giving prolonged carbohydrates before thiamine can precipitate WE by accumulation of toxic metabolites from catabolic enzymes that need vitamin B1 in order to function properly
- No treatment guidelines exist for pediatric WE
Methodology:
Figure 1: Rapid Review Flow Diagram

Results:

Vagal nerve stimulation in three cases of continuous spike-wave during slow wave sleep
Key Messages:
- Approximately 70% of Continuous Spike and Wave during slow wave Sleep (CSWS) cases are refractory to ≥3 AED, and only 5% are eligible for surgery.
- We report 3 cases of vagus nerve stimulation in children with CSWS who were pharmaco-resistant and not surgical candidates (only 1 previous case report)
- VNS reduced or eliminated the epileptiform discharges on EEG, improved cognitive outcomes, and decreased seizure frequency in all cases.
Introduction:
- Continuous Spike and Wave during Sleep (CSWS), previously Electrical status epilepticus in sleep (ESES) is know known as Developmental Epileptic Encephalopathy with Spike Wave Activation In Sleep (DEE-SWAS)
- CSWS can be idiopathic, or manifest from structural or organic brain lesions, of which unilateral polymicrogyria is most frequent1
- CSWS onset is typically between ages 4 to 7.
-
The clinical evolution often follows a three stage progression2:
- Infrequent nocturnal motor focal seizures, and non-REM sleep potentiation of spiking or slow spike-waves in primarily centro-temporal and frontal regions
- Worsening seizures clinically and on EEG, and neuropsychological regression
- Spontaneous resolution by puberty
- Early therapy lowers the risk of long term poor cognitive outcomes and the longer duration (rather than intensity) of CSWS is associated with poorer cognitive outcomes3
- Typically, anti-epileptic drug(s) (AED) are first-line
- Neurosurgery and steroids are second-line, but both demonstrate superior efficacy in CSWS4
- Options for refractory cases are inconclusive, but include IVIg, ketogenic diet, vagus nerve stimulation, cannabinoids and hemispherectomy or multiple subpial transections
Methodology
- Retrospective clinical chart review
- All patients were followed by Dr. Wendy Stewart prior to VNS and post VNS therapy
- Patients and families were contacted and consented to share de-identified clinical data
Case Series:
| Characteristics | Case 1 | Case 2 | Case 3 |
| Age (years) | 24 | 16 | 13 |
| Sex at birth | F | M | M |
| Pre-existing neurodevelopmental disorder | No | ASD and developmental delay, chromosome 15q duplication syndrome | ASD |
| Age (years) at CSWS diagnosis | 5 | 4 | 5 |
| Onset of VNS therapy (age in years) | 10 | 6 | 8 |
| Other treatment | Valproate Clobazam Clonazepam Keppra Lacosamide Steroids IVIG |
Tegretol Trileptal Valproic acid Clobazam Topamax Ethosuximide Lacosamide Fycompa Vigabatrin Family did not want steroids due to behavioural concerns |
Clobazam Valproic acid Lamotrigine Clonazepam Keppra Topamax Steroids IVIG |
| EEG findings after VNS therapy |
- Almost no epileptiform discharge in the awake state - Ongoing brief discharges in sleep - Seizures captured in overnight EEG - focal from right hemisphere |
- Marked reduction in discharges within 17 months of VNS insertion and within 2 years continued improvement |
- Resolved CSWS within 6 months - still had abnormalities but markedly less frequent. - Pages with 1-2 discharges and some longer runs |
| Clinical seizure post VNS | Infrequent seizures some clusters. Initially no medication but lacosamide started | Decreased seizures over time and eventually they stopped then recurred when he was a teenager | Very infrequent seizures |
| Subjective cognitive outcomes | Language improved and she was more socially engaged. She was able to complete school on a special learning plan | Increased vocabulary | Remains nonverbal but is able to understand what is happening around him. Has been able to learn at school |
Case 1 Prior to VNS Therapy
Case 1 Post VNS Therapy
Discussion:
- Desynchronization activity of VNS on thalamic projections could potentially disrupt aberrant thalamic reverberating circuits found in CSWS5
- VNS had positive outcomes in lowering seizure frequency in CSWS in one case report found in the literature5. A handful of cases also mentioned the use of VNS in CSWS, but did not elaborate on outcomes6,7
- No adverse side effects have been reported from VNS therapy in CSWS, including our three cases
- The results support VNS as an option to reduce or eliminate the epileptiform discharges and decrease clinical seizure frequency for children with CSWS who are pharmaco-resistant and not surgical candidates
References:

Developing a Brief Clinical Dataset for Duchenne Muscular Dystrophy

Key Messages:
- We have created the first ICF Brief Core Sets for DMD (ambulatory and non-ambulatory)
- The CNDR registry is being updated with outcomes measures that best align with the ICF brief core set for DMD to fill the gaps identified in the activities and participation and environemntal factors domains
- In comparing ambulatory and non-ambulatory, the biggest difference was in the body function domain whereas the environmental factors were similar
- This work will improve post-marketing surveillance for the CNDR registry and inform the design of upcoming clinical trials for DMD
Introduction:
- Canadian Neuromuscular Disease Registry (CNDR) is a pan-neuromuscular disease registry that collects prospective data from 38 clinics across Canada.
- CNDR is undergoing a dataset update for its Duchenne Muscular Dystrophy (DMD) registry containing data of approximately 534 patients.
- The International Classification of Functioning, Disability and Health (ICF) is an international standard with 1400+ categories describing health and disability in the domains of body functions, activity & participation, environmental factors, and body structure1.
- Goal: Update the CNDR registry to reflect the lived experiences of those affected by DMD using an ICF wholistic dataset
Methodology:

Results:
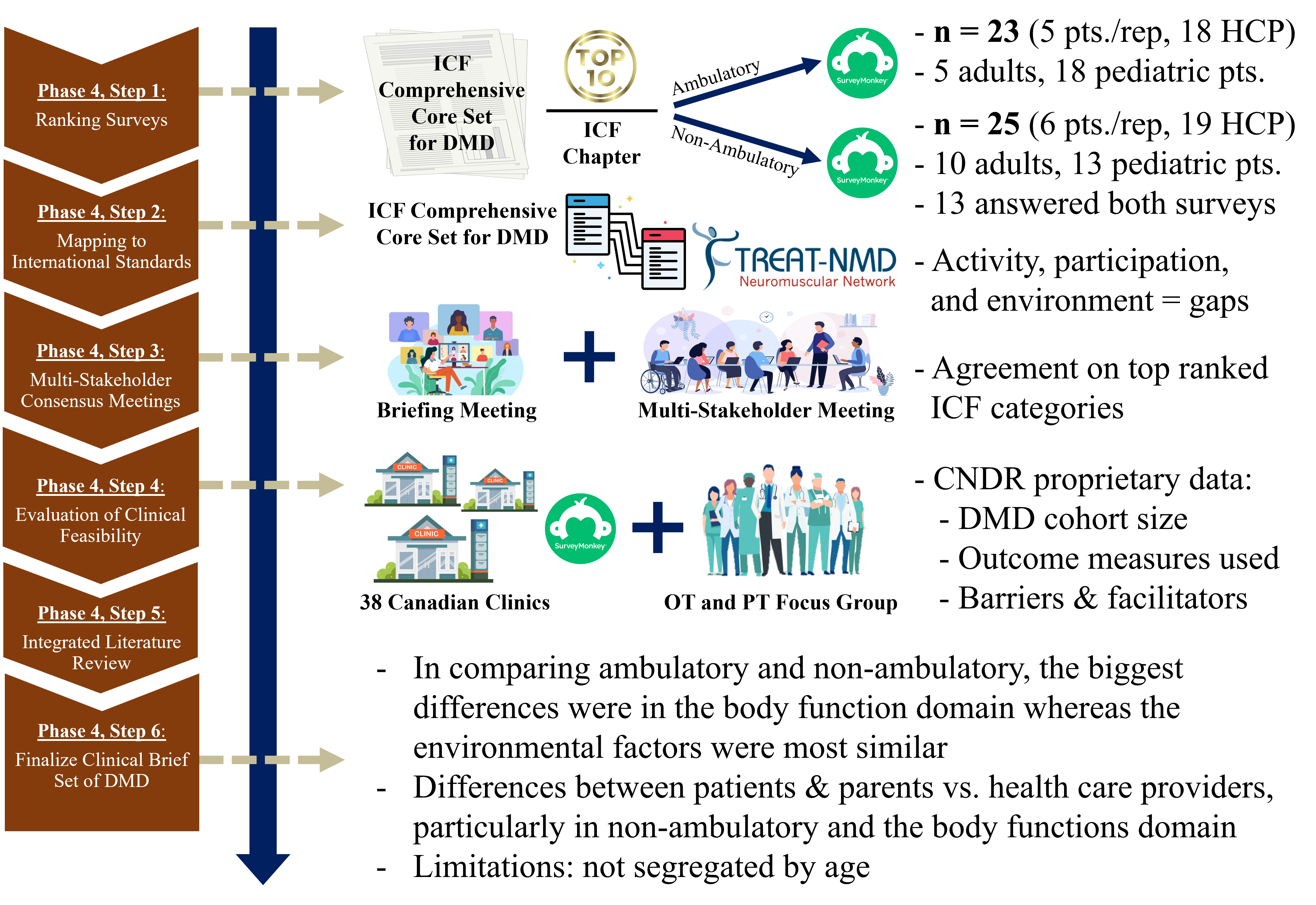
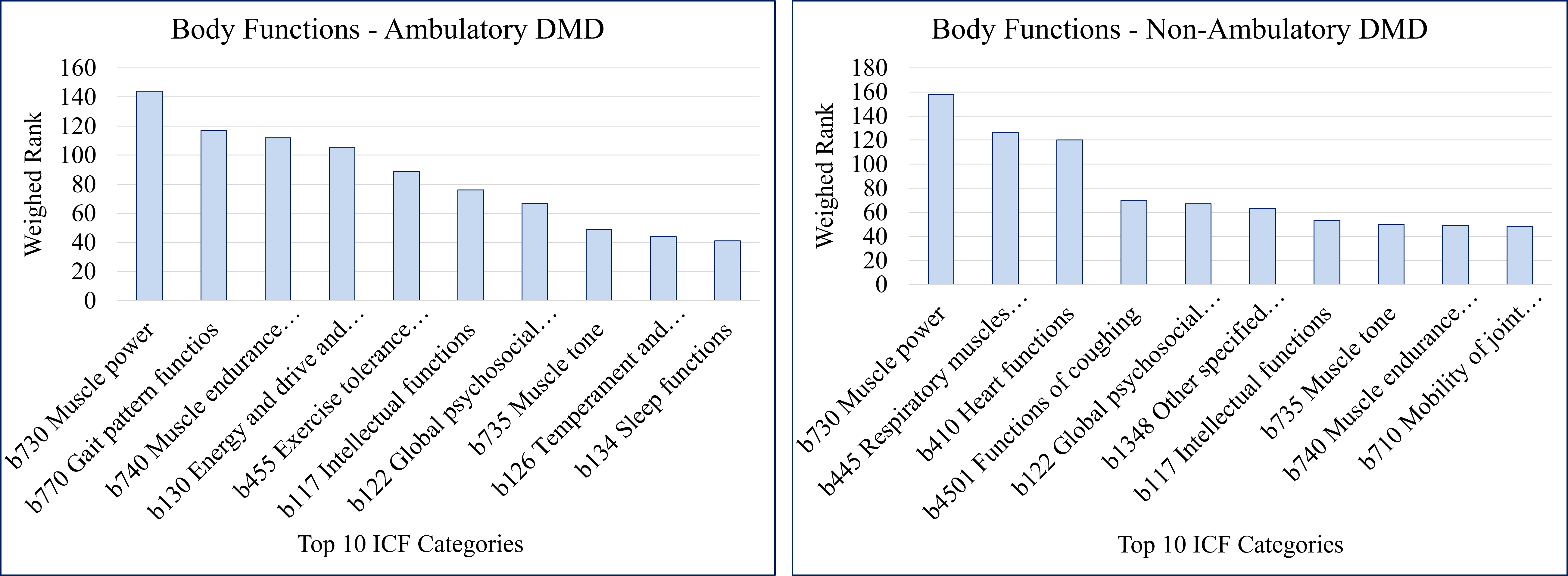
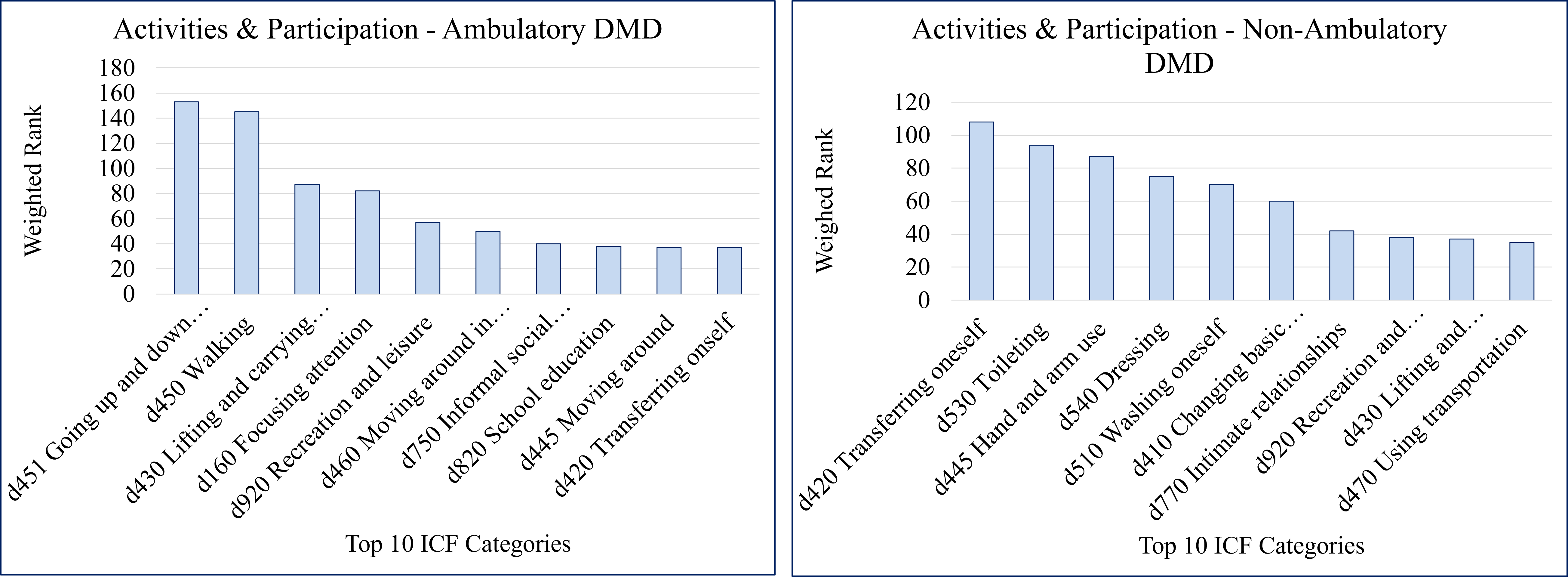
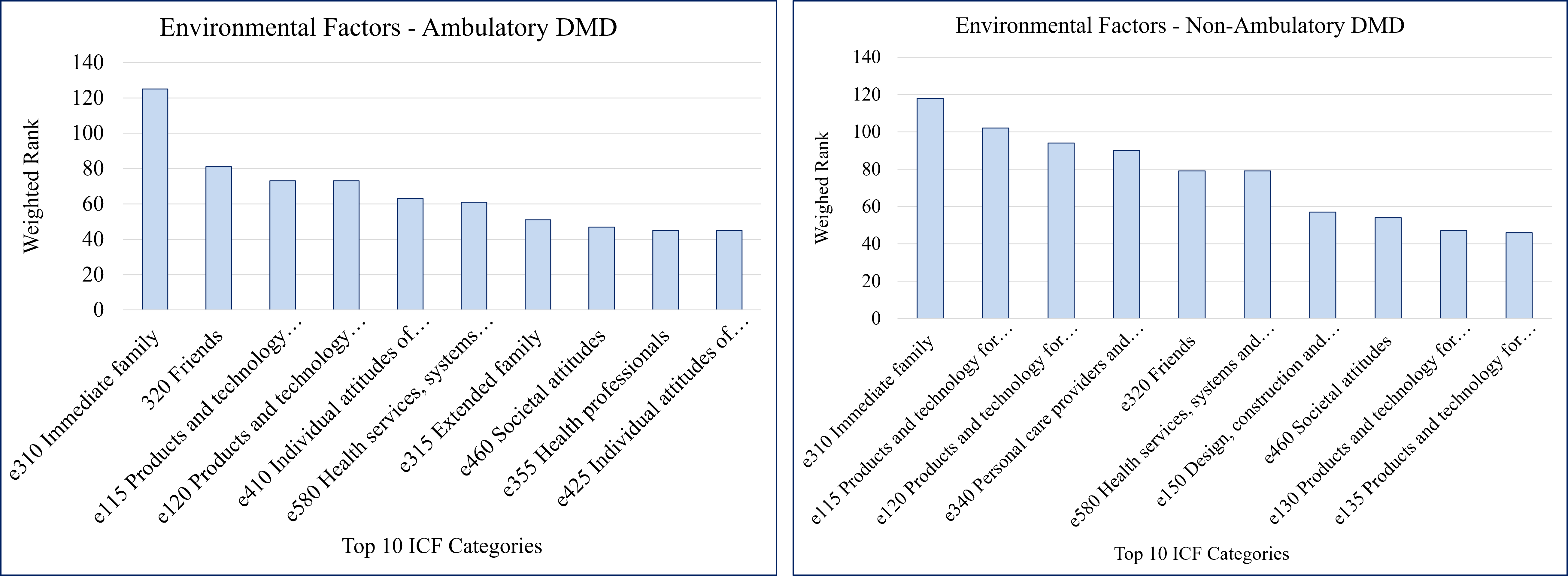
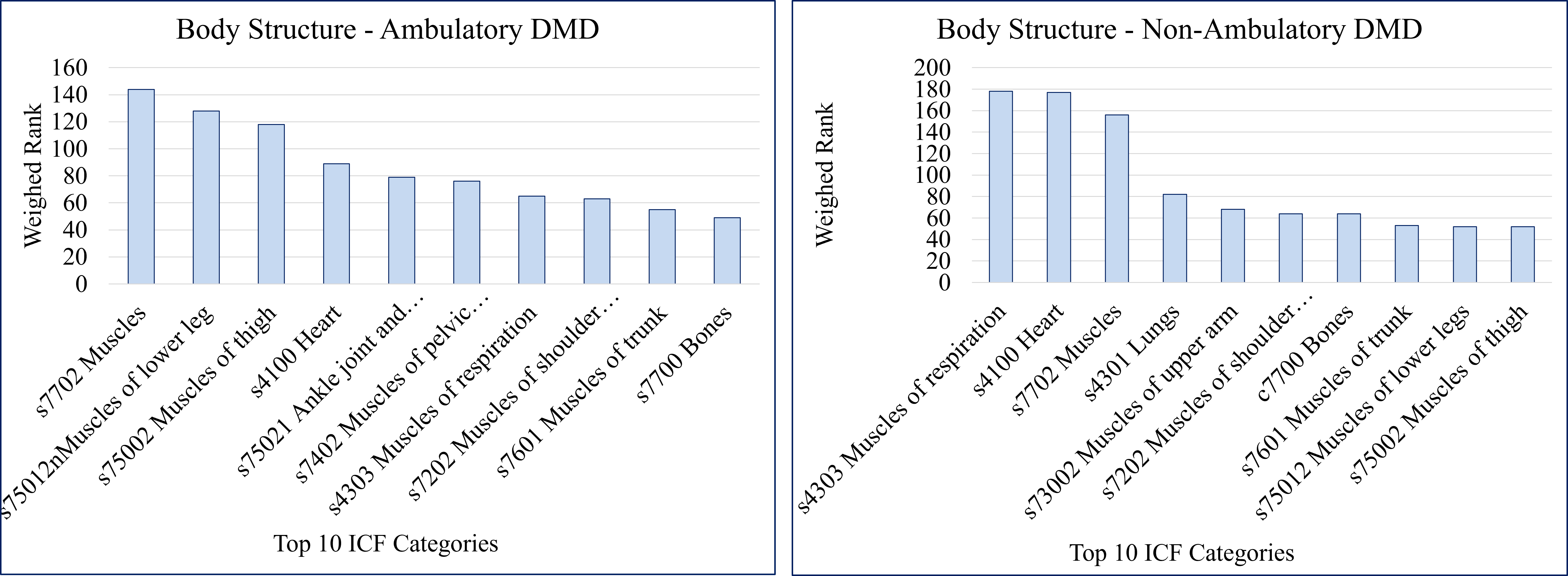
Erid Morden shares the relevance of a wholistic dataset for DMD:

Next Steps:
- Last consensus conference to approve final DMD ICF Core Set prior to publication
- Continue engagement of site investigators, patient and parent partners, and industry to identify and build consensus on feasible outcome measures to fill the data collection priority gaps
- Pilot expanded registry dataset for CNDR
- Knowledge translation via Defeat Duchenne Canada, Muscular Dystrophy Canada, and the Neuromuscular Disease Network 4 Canada

Survey of caregivers of individuals with NBIAs to identify relevant quality of life outcomes

Background
- Neurodegeneration with brain iron accumulation (NBIA) is a rare group of disorders characterized radiologically by abnormal accumulation of iron in the basal ganglia.
- NBIA disorders typically present as progressive childhood onset neurodegeneration consisting of developmental delay, dystonia, spasticity, optic atrophy and epilepsy.
- Care currently consists of multidisciplinary symptom management
- Similar to other rare diseases, there exist challenges in management from both the caregiver and healthcare provider perspectives
Introduction
- Caring for a family member with an NBIA disorder is intensive but the degree and spectrum of challenges is currently unknown
- There are little available resources and supports available to caregivers of children with NBIA disorders.
- Our study employed a caregiver survey to identify factors related to the health of children with NBIA disorders that are impacting caregiver well-being and quality of life.
- Understanding these challenges can lead to better care for the patients, better support systems for families, and better educational resource development for healthcare providers.
Methods
- A review of literature was completed to create the survey to create questions related to quality of life in chronic diseases and neurological diseases.
- The survey was created and administered using the digital platform, RareConnect.
- The survey was piloted with the Parent and Family Advisory Committee at the CHEO RI.
- The survey revised and then administered to 30 caregivers of Canadian patients with NBIA.
- Data was analyzed quantitatively using Likert plot analysis and qualitatively using thematic analysis to extract caregiver challenges
- A summary of demographic information of NBIA patients is shown in Table 1.
Table 1: Demographic information of NBIA Caregivers
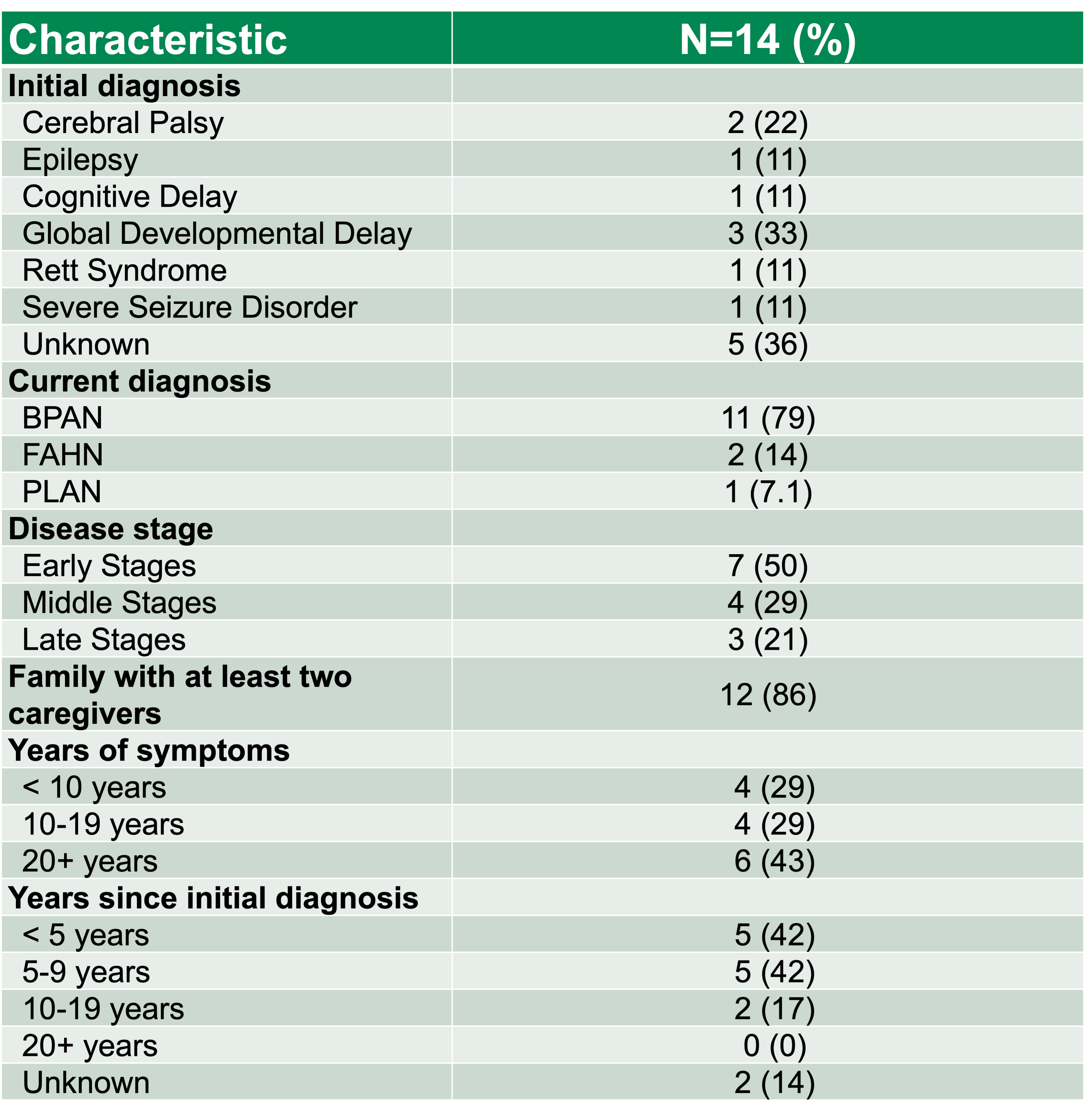
Results
Diagnosis
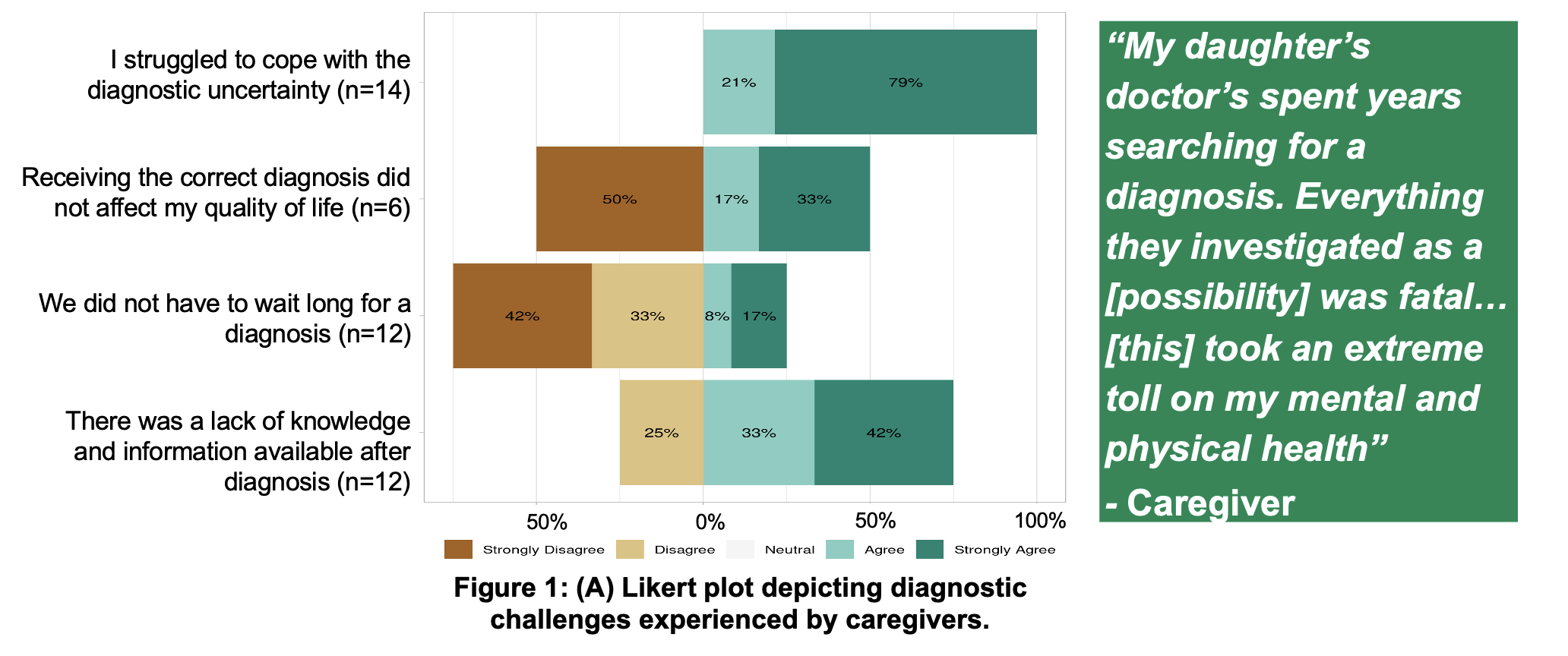
Symptom Management
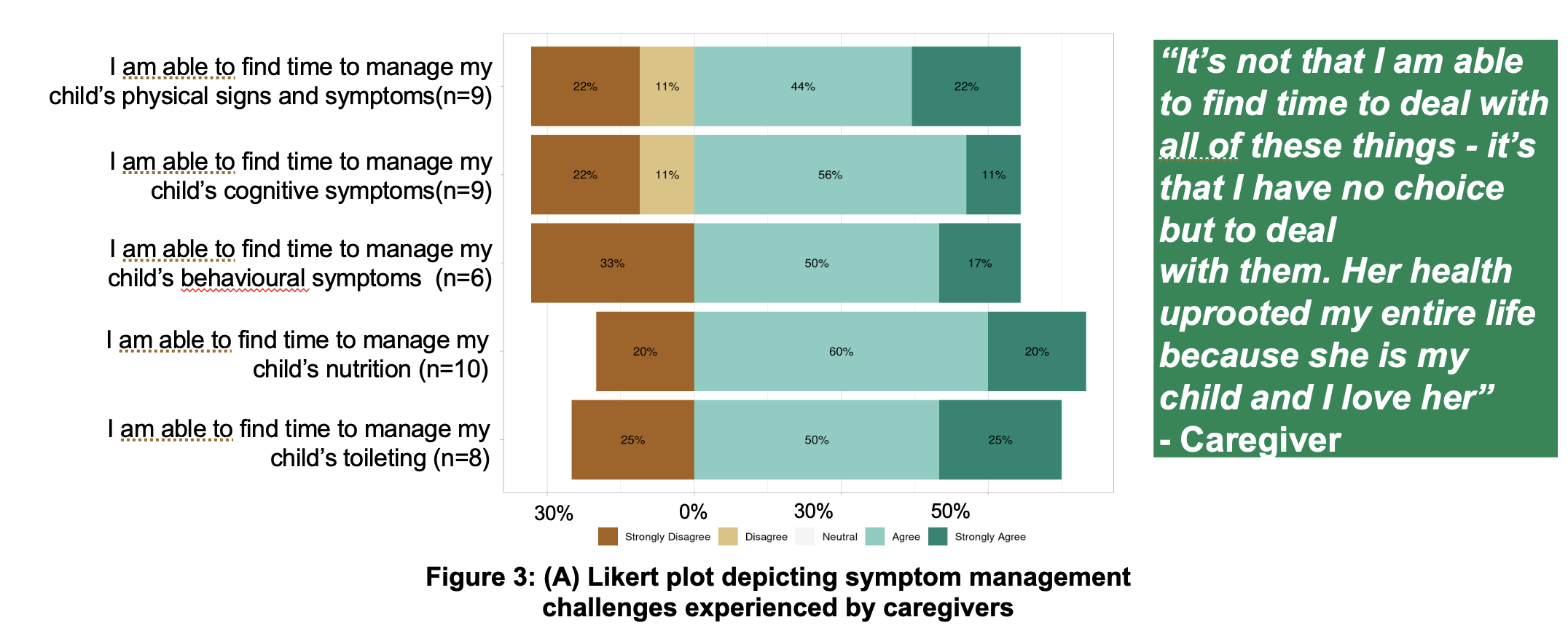
Resources and Support
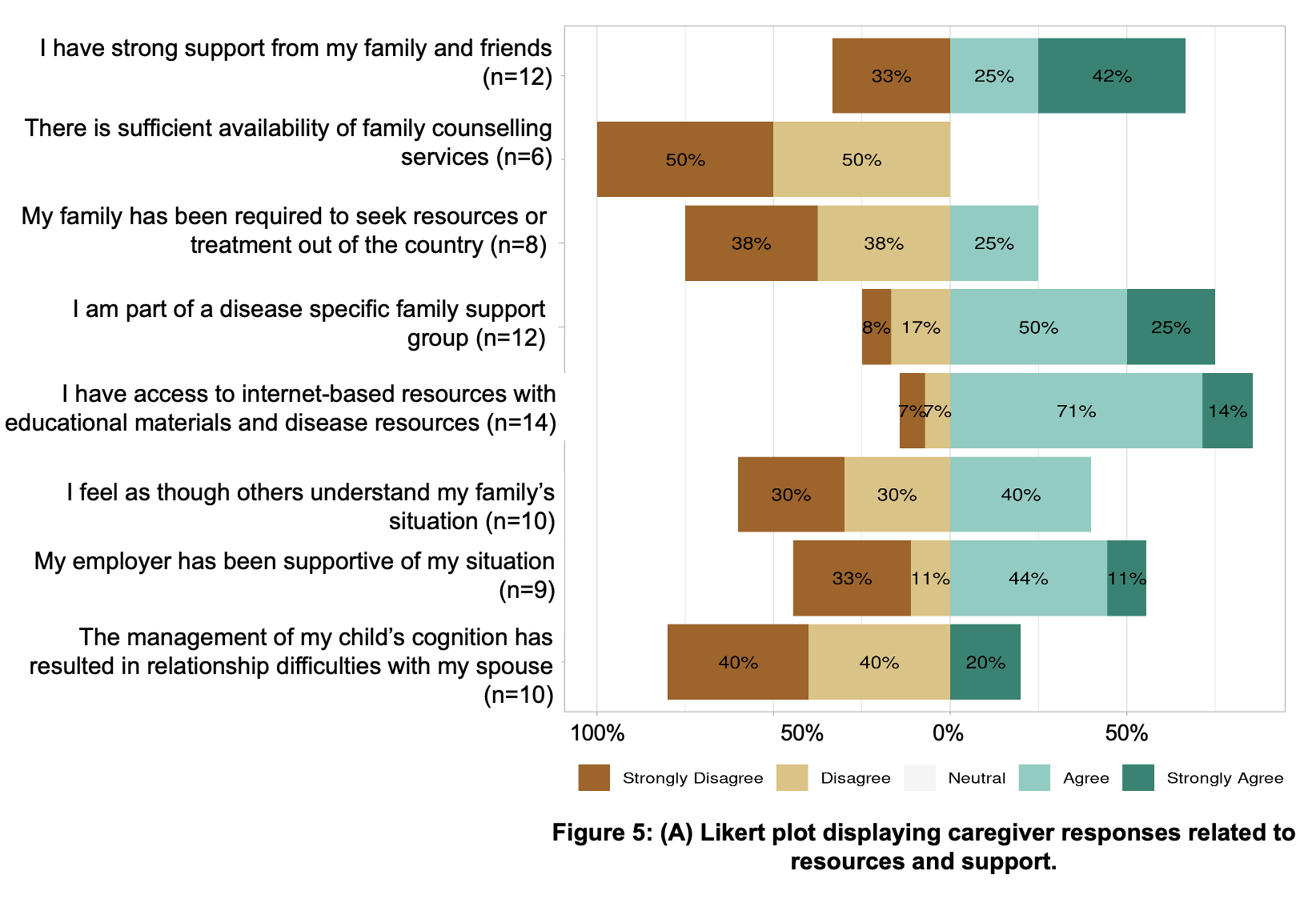
Healthcare Provider and Communication
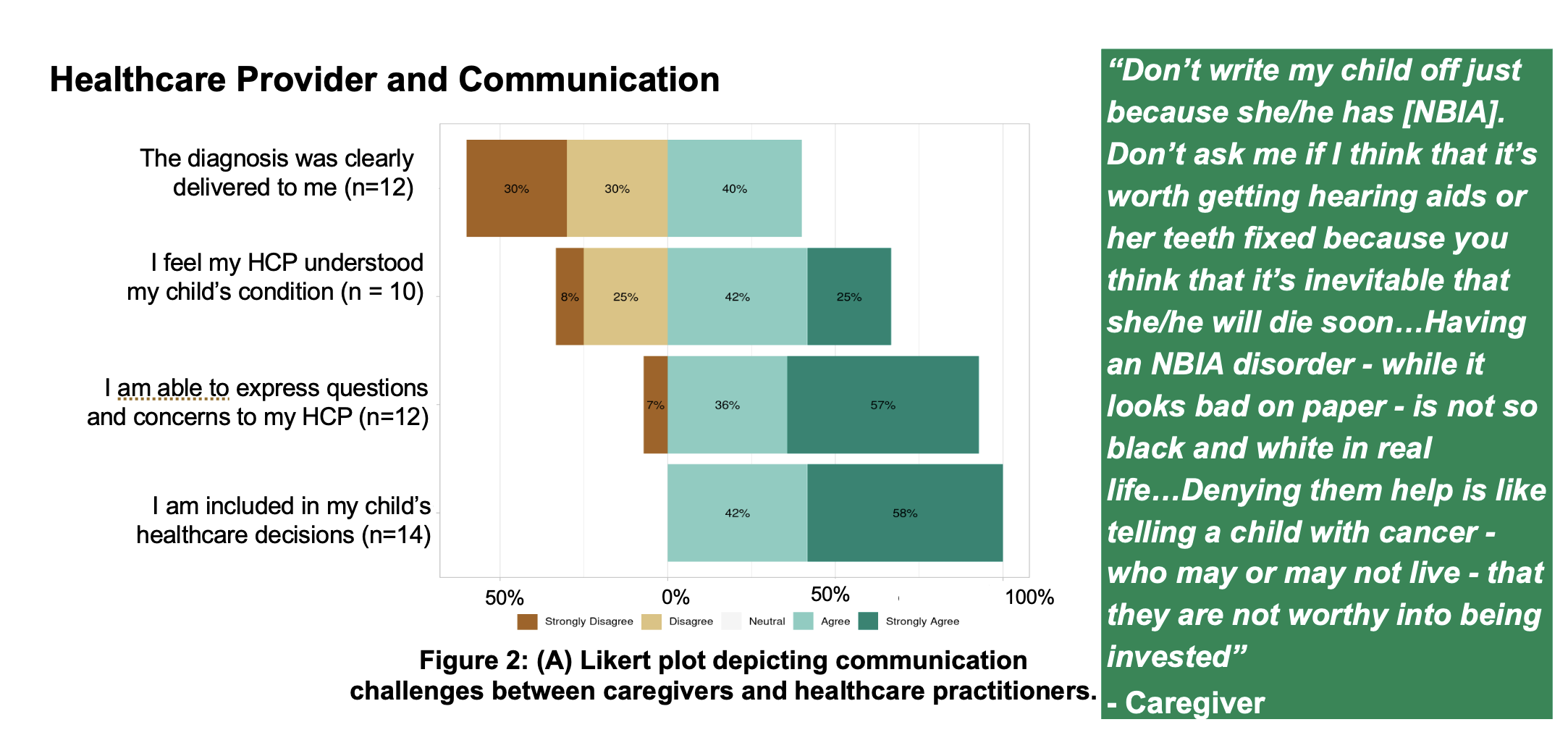
Clinical Experience

Factors Affecting Caregiver QOL
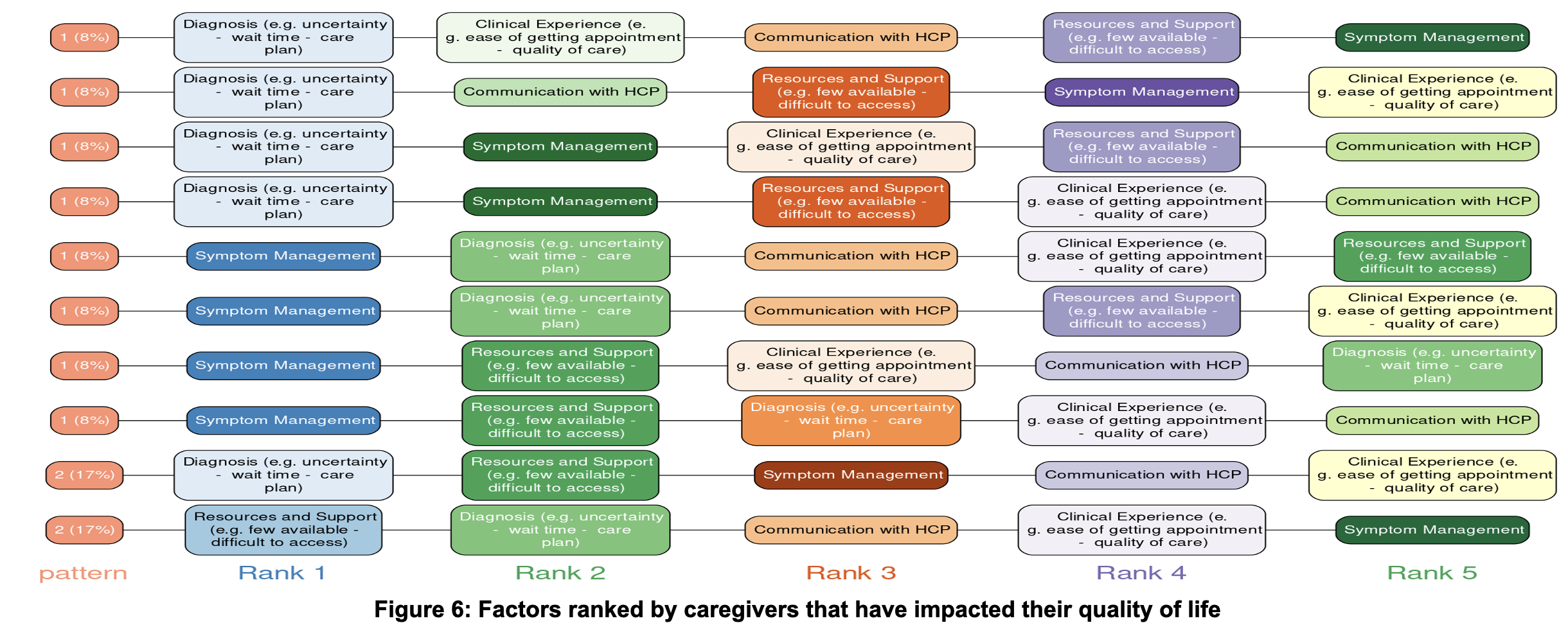
Conclusion
The results of the survey were extremely informative in advocating for increased support of caregivers (financially and informatively) through the development of NBIA management guidelines for physicians and families and direct the structure of future Canadian NBIA family conferences.
Prevalence, type, and risk factors of intracranial hemorrhage in term neonates: a systematic review and meta-analysis

Introduction
Background
- ICH in the newborn poses significant potential challenges to subsequent development
- In preterm neonates, germinal matrix hemorrhage is the most common cause, prevalence varying from 20 to 59% 1
- In term neonates, the prevalence and etiology of ICH has not been well elucidated3,4
- The rate of detection of ICH is influenced by the modality used for imaging and multiple risk factors that contribute
Objectives
The objective was to assess the prevalence of examine risk factors associated with ICH in term neonates
Specific questions:
Specific questions:
- What is the prevalence of ICH in asymptomatic and symptomatic term neonates?
- What are the types of ICH in term neonates?
- Is there any change in prevalence depending on the method of detection, that is, MRI, CT or USG?
- What are the risk factors associated with ICH in term neonates?
Methods
Search Strategy
- PUBMED and EMBASE
- Used variations on the terms “intracranial hemorrhage” and “term neonate”.
- Term neonates - born at a gestational age of 37+ weeks
- Subdivided based on method of delivery
- Subdivided into asymptomatic versus symptomatic
- Cohort studies, case-control studies, case series
-
Excluded studies:
- Examined only a specific type of hemorrhage or did not describe ICH
- Examined only one risk factor
- Sample size <20
- Not in English or full text not accessible/available
Results
Studies included
Modalities for Detection
- A total of 1233 studies were identified
-
20 studies were included the final analysis
- 11 studies included asymptomatic patients
- 7 studies included symptomatic patients
- 2 studies included both
| Group | Prevalence (%) | 95% C.I |
| Overall | 9.3 | 4.9-14.9 |
| Asymptomatic | 5.8 | 2.5-10.2 |
| Symptomatic | 29.3 | 15.3-44.8 |
Modalities for Detection
- Overall, CT > MRI > USG
-
Research shows CT and MRI are similar regarding extra-axial hemorrhages
- MRI is better at detecting ICH in symptomatic neonates
- MRI is also better at detecting intraparenchymal hemorrhages
-
USG is better at detecting ICH in asymptomatic versus symptomatic neonates
- Prior studies have shown USG sensitivity is 85.7-93% and specificity is 97.9-98% in detecting hemorrhages in children <2 18, 19
- USG is inadequate for visualizing hemorrhages along the cerebral convexities or in the posterior fossa 20, 21
| Modality | Asymptomatic vs Symptomatic | # of Studies | Total # of Studies | Total Prevalence (%) |
| USG | Asymptomatic Symptomatic |
7 1 |
8 | 1.8 |
| CT | Both Symptomatic |
1 1 |
2 | 32.2 |
| MRI | Asymptomatic Symptomatic |
2 3 |
5 | 22.2 |
| Multiple | Both Symptomatic |
1 4 |
5 | - |
| Total Prevalence (%) | |
| USG - Asymptomatic | 1.8 |
| CT + MRI- Asymptomatic | 19.7 |
| CT + MRI - Symptomatic | 29.3 |
Types of hemorrhage
| Type of hemorrhage | Proportion (%) | 95% CI |
| Extraaxial hemorrhage | 30 | 8 - 44 |
| Germinal matrix hemorrhage | 24 | 4 - 38 |
| Intraparenchymal hemorrhage | 21 | 3 - 35 |
| Intraventricular hemorrhage | 14 | 1 - 29 |
| Subarachnoid hemorrhage | 7 | 0 - 18 |
| Multiple hemorrhage | 4 | 0 - 13 |
-
Extra-axial hemorrhage
- Most common
- Subdural hemorrhage > extradural hemorrhage
- Contrasts to ICH in pre-term neonates - most common is germinal matrix hemorrhage 13.
-
Subdural hemorrhage
- More frequently demonstrated with MRI (26-46% 15)
- Unclear clinical significance of SDH in asymptomatic neonates
- Zamora et al - no major difference in neurodevelopmental outcomes in symptomatic neonates vs controls
-
The short term prognosis of neonates with SDH also remains favorable.
- Whitby et al - 9 neonates with SDH did not require neurosurgical intervention, all had complete resolution of hematomas at 4 weeks 16
- Birth related SDH can involve both the supratentorial and infratentorial compartments 17
- Epidural hemorrhage is rare, likely because the middle meningeal artery is not yet adherent to the bone
-
Germinal matrix hemorrhage and intraparenchymal hemorrhages
- Althought the germinal matrix almost completely involutes by 36-37 weeks, results from our study indicate that GMH is still substantial at 23.59%
-
Significance of GMH and IVH is not well understood, possible increased risk of CP
Risk factors
- Only risk factor for ICH amenable to analysis was mode of delivery
-
Rate of ICH was 6x more when delivered using vacuum extraction24
- Similar increase with forceps assisted delivery (OR 3.4) 23
-
Multiple possible mechanisms as the cause of SDH n term neonates
- Compression of the skull during passage through the birth canal or an instrumental delivery mechanical stresses tearing of the tentorium, falx, or bridging veins 25, 26
-
C/S associated with a lower risk of ICH
- Likely because it eliminates mechanical stresss
-
Disorders of coagulation or platelets
- Risk with Hemophilia A or B is 40-60x higher 30
- 50-82% of neonates with vitamin K deficiency will present with ICH31
- Can occur secondary to autoimmune or alloimmune thrombocytopenia
- ECMO and associated anticoagulation can predisopse neonates to ICH 34, 35
- Low APGAR score and/or need for rescucitation 30, 36
- Labour complications or prolonged labour 30, 36
- Metabolic acidosis 30, 36
- Congenital brain tumours 30, 36
-
Vascular anomalies
- Mutations in COL4A1 or COL4A2, which encode for alpha1 and alpha2 subunits of type IV collagen 36, 37
Conclusions
Conclusions
-
The overall prevalence of ICH in term neonates is 9.3%
- Much more commonly (almost 5x) detected in symptomatic neonates
-
Overall, CT had the highest rate of detection
- MRI is better at detecting intraparenchymal hemorrhage and ICH in symptomatic neonates
-
The only risk factor that could be analyzed is method of delivery
- Highest risk with instrumental deliveries, lowest risk with C/S
- Other risk factors could not be statistically analyzed
-
Heterogeneity in studies, noted by the high I2 statistic
- Likely due to multiple factors - ie. symptomatic vs asymptomatic
- Mode of detection also varied, adding to diversity
- Studies were conducted over years, technological improvements likely influenced rate of detection
- Improvements in maternal/perinatal care could decrease the occurrence of ICH
- Only mode of delivery included in analysis, although several other risk factors
Acetazolamide use for myoclonus: case report of 2 patients with progressive myoclonus epilepsy and literature review
BACKGROUND
- Cortical myoclonus are brief muscle jerks caused by abnormal cortical activity. They can occur spontaneously or triggered by somatosensory stimuli or by voluntary movement.
- Acetazolamide (ACZ) is an inhibitor of the carbonic anhydrase protein which ultimately results in a low intracellular pH, causing acidification.
- Current evidence shows that a seizure focus tends to be alkaline, thus the change in pH induced by ACZ is postulated to explain some of the anti-seizure effects.
METHODS
CASE 1
22-year-old female, diagnosed with PME secondary to a KCNC1 variant. Her symptoms started at 10 years of age with bilateral tonic clonic seizures (BTCS). She later developed progressive ataxia and myoclonus, involving face and limbs, which worsened with stimulus and menses. Perampanel, Clonazepam and Levetiracetam helped with some seizures, however, myoclonus was still limiting. At the age of 19, ACZ 250 mg BID was started for 2 weeks around her menses which led to significant improvement of myoclonus, resulting in better ambulation, balance and speech. These improvements were sustained 2.5 years later.
CASE 2
67-year-old male, previous history of diabetes, sleep apnea and hypothyroidism presented with BTCS at the age of 53 along with cortical myoclonus (Figure 2), dementia and ataxia, leading to diagnosis of PME with an likely pathogenic IRF2BPL variant. His myoclonus was worse in the morning or with anxiety, ranging from 4 to 10 per hour, compromising his ability to perform independent activities of daily living and requiring a walker on a regular basis. Improvement of myoclonus occurred with ACZ 250 mg BID which was sustained after 2 years, although balance and cognition continued to deteriorate as part of his condition.
Figure 2. Drawing of spiral from Case 2 showing tremor and myoclonus.
CONCLUSION
Previous literature outlines 4 cases of action myoclonus that responded to ACZ. Our study adds 2 patients to the current literature. Hence, we conclude that the use of ACZ should be considered in the treatment of myoclonus, especially in cases with cortical involvement and hormonal fluctuations.
RESULTS & DISCUSSION

Table 1. Summary of ACZ Uses in Literature and Our Two Cases. Acetazolamide (ACZ), Progressive myoclonic epilepsy (PME), Bilateral tonic clonic seizures (BTCS), Computerized Tomography (CT scan), Clonazepam (CLZ), Valproate (VPA), Phenobarbitone (PB), Phenytoin (PNT), Levetiracetam (LEV), Lamotrigine (LMT), Perampanel (PER), Progressive Myoclonic Epilepsy (PME), Bilateral Tonic-Clonic seizures (BTCS), Electroencephalography (EEG), Not Available (NA).
Spike source localizations between the three non-REM sleep stages: resemblances to wakefulness and distinctions from REM sleep
Introduction
Sleep-wake states (SWS) affect the expression of interictal epileptiform discharges (“spikes”), which affects resultant source localization calculations used in epilepsy evaluation. We hypothesize that spike localizations from non-REM (NREM) sleep 1-3 are most concordant with one another. In this study, we chose 3-way concordance and hypothesized that REM should be the least 3-way concordant in any combination of 3 SWS in all 5 SWS.
Methods
We assessed the localization of epileptic generators during various sleep stages, including N1, N2, N3, rapid eye movement (REM) sleep, and wakefulness (W). The initial analysis involved the computation of the F-statistic parameter using Standardized low-resolution brain electromagnetic tomography (sLORETA) within Curry 8 software. The F-statistic represents the statistical probability of epileptic generator presence within specific voxels. A threshold was set to determine voxels likely to contain epileptic sources, defined as those with an F-statistic greater than 50% of the maximum F-statistic observed. This process was iterated for each stage of SWS, resulting in distinct source localizations for each stage. Source localization was quantified as a percentage of cortical grey matter voxels, calculated by dividing the total number of involved voxels by the total number of voxels in the brain model. Subsequent analysis involved the comparison of source localizations across different SWS, aiming to identify areas of agreement or disagreement regarding the presence of epileptic sources. A 3-way concordance analysis was conducted to identify voxels consistently identified as epileptic sources across all three SWS. Voxel concordance was assessed among various combinations of sleep stages, including N1-N2-N3, N1-N2-W, N1-N3-W, N2-N3-W, REM-N1-N2, REM-N1-N3, REM-N2-N3, REM-N1-W, REM-N2-W, and REM-N3-W. Concordances were categorized based on the presence or absence of specific sleep stages for comparative purposes.
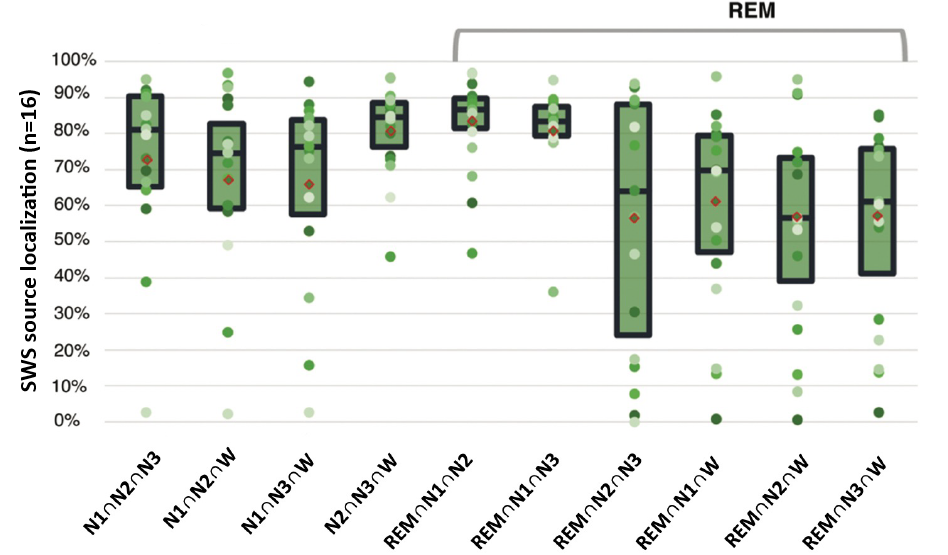
Figure 1: Sleep-wake states (SWS) source localization (n=16)
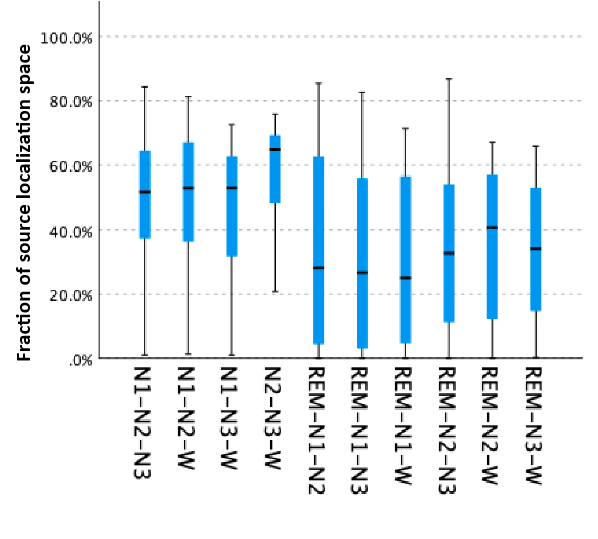
Figure 2: Independent-Samples Kruskal-Wallis test in different combination of SWS in 3-way concordance
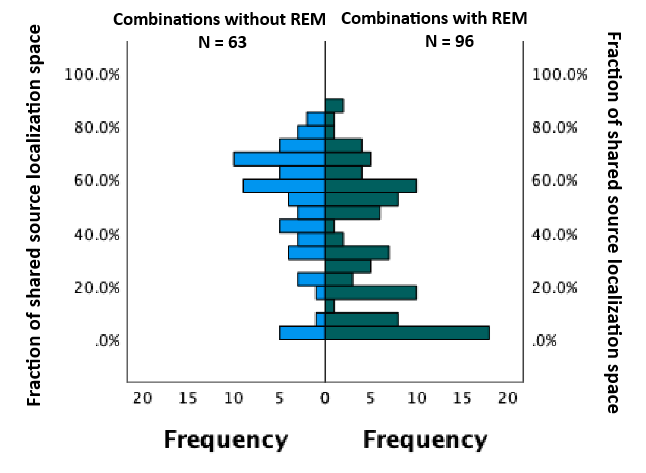
Figure 3: Independent-Samples Mann-Whitney U test of 3-way concordances without REM vs. with REM, as fractions of shared source localization space
Results
We calculated concordances for 16 patients and it did not differ for N1-3 or W (Figure 1). However, concordances with REM were lower than those without REM as a fraction of source localization space (median 32.1% vs. 56.1%, p<0.001) (Figure 2) and cortical grey matter (median 20.4% vs. 27.3%, p=0.003). To assess the impact of REM sleep, we compared 3-way concordance (fraction of shared localization space) between combinations without REM sleep and those with REM sleep to find that combinations with REM sleep were significantly less 3-way concordant (p<0.001, Figure 3).
Conclusion
As expected, source localizations from spikes in N1, N2, and N3 did not significantly differ from one another because these three states are constituent members of NREM sleep. Surprisingly, however, source localizations derived from awake spikes – not a constituent of NREM sleep – also did not differ. In contrast, REM was most different by reproducibly exhibiting the least three-way concordance. These findings reinforce the unique localizing ability of REM sleep.
Parkinson’s disease tremor can show entrainment and distractibility with tapping test
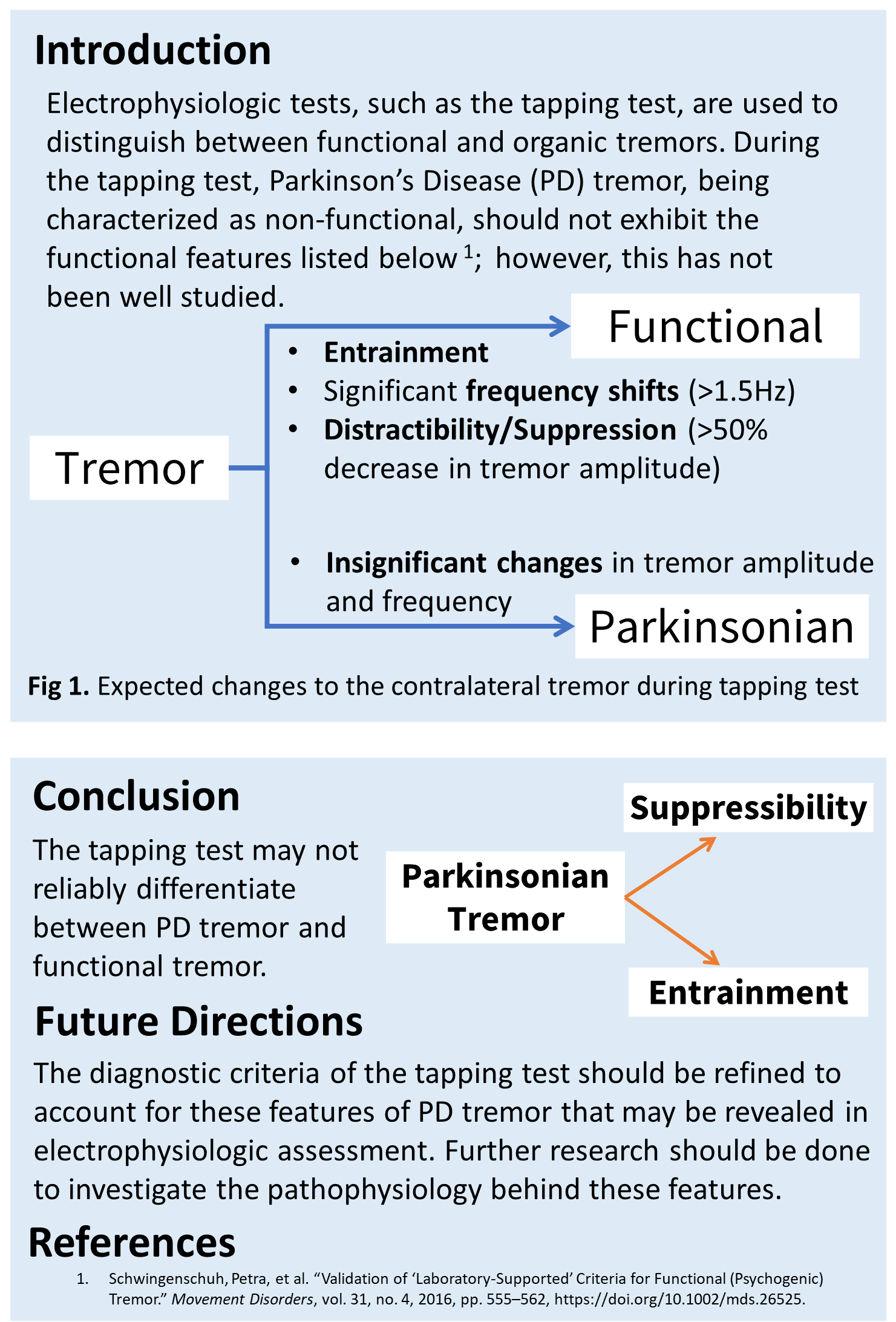
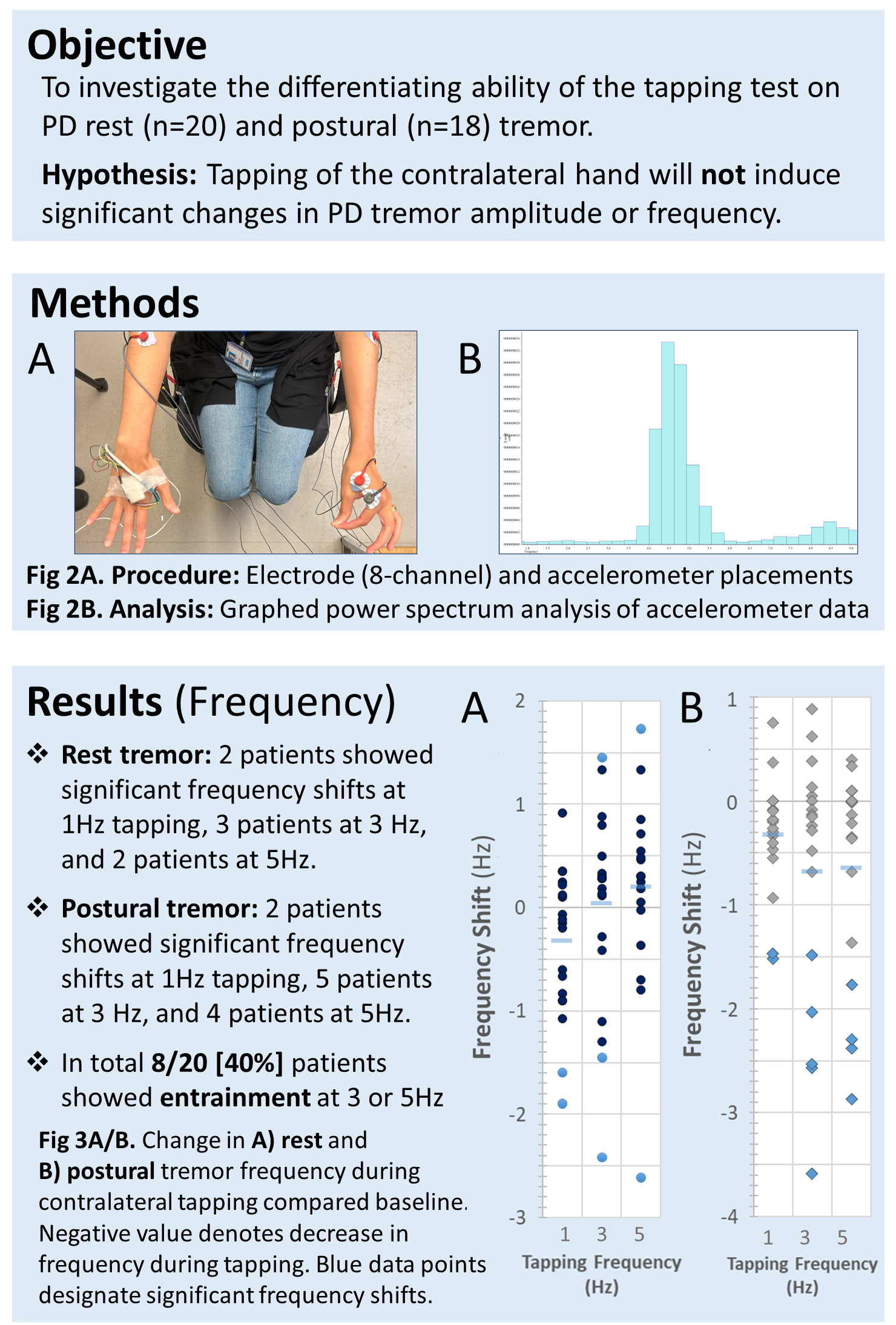
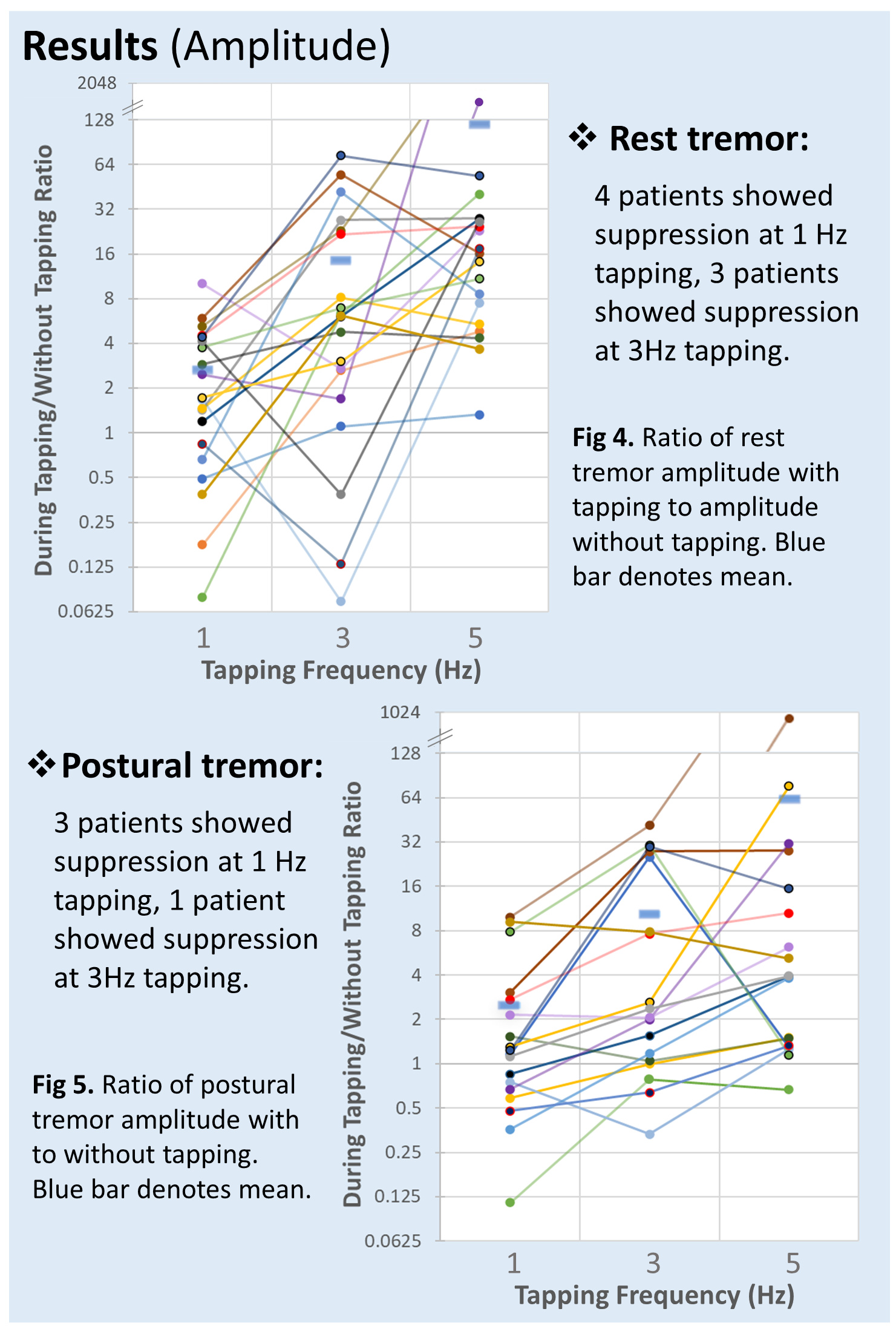
Utility of amyotrophic lateral sclerosis functional rating scale (ALSFRS) bulbar subscores for predicting need for gastrostomy tube
Introduction
- ALSFRS is a validated and gold-standard rating instrument to track functional disability and progression of limb, bulbar, and respiratory symptoms in ALS
- The utility of ALSFRS in predicting clinical interventions such as gastrostomy tube (G-tube) insertion is unknown
- We aimed to evaluate the utility of ALSFRS bulbar subscores in predicting G-tube insertion
- We hypothesized that a transition in the swallowing subscore from 3 to 2 would significantly increase likelihood of G-tube insertion
| ALSFRS subscore | Swallowing | Speech | Salivation |
| 4 | Normal | Normal | Normal |
| 3 | Early eating problems; occasional choking | Detectable speech disturbance | Slight but definite excess of saliva in mouth; may have nighttime drooling |
| 2 | Dietary consistency changes | Intelligible with repeating | Moderately excessive saliva; may have minimal drooling |
| 1 | Needs supplemental tube feedings | Speech combined with nonvocal communications | Marked excess of saliva with some drooling |
| 0 | Nothing by mouth, exclusively parenteral or enteral feeding | Loss of useful speech | Marked drooling; requires constant tissue or handkerchief |
Materials and Methods
- Retrospective study using the Pooled Resource Open-Access ALS Clinical Trials Database (PRO-ACT) approved by the University of Calgary Conjoint Heath Research Ethics Board (REB23-1715)
- Primary outcome, G-tube insertion, was defined as date on which ALSFRS swallowing subscore transitioned to 1 or less
- Survival analyses were used to estimate median time to and cumulative probability of the outcome within 91 days from baseline and following ALSFRS bulbar subscore transitions
- Individuals who did not meet the outcome were censored at last ALSFRS
- Kaplan-Meier failure curves and 95% confidence intervals (CIs) were used to compare groups
Results
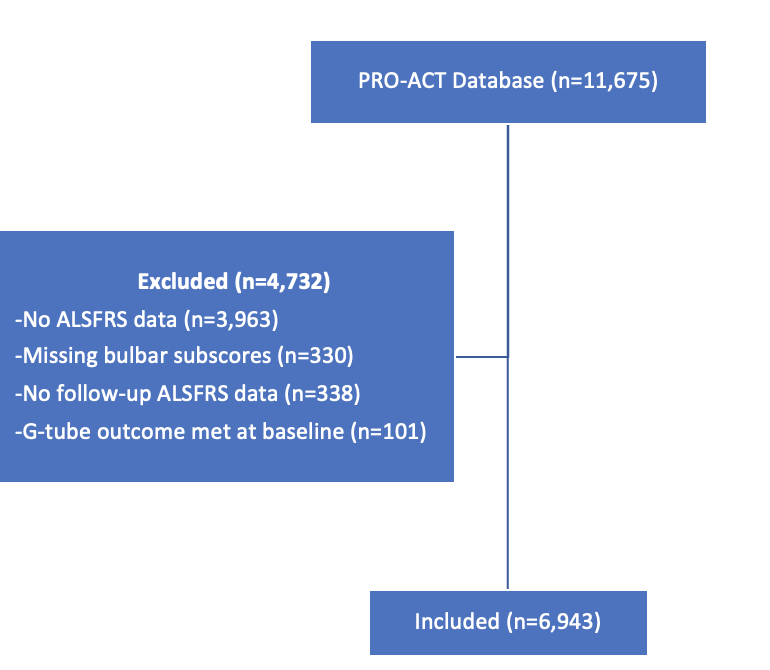
Figure 1. Flowchart describing exclusion of participants
Mean age of cohort was 55.7, 63.2% were males, and 19.3% had bulbar onset.
Mean age of cohort was 55.7, 63.2% were males, and 19.3% had bulbar onset.
Table 1. Time to G-tube outcome by baseline ALSFRS bulbar subscores
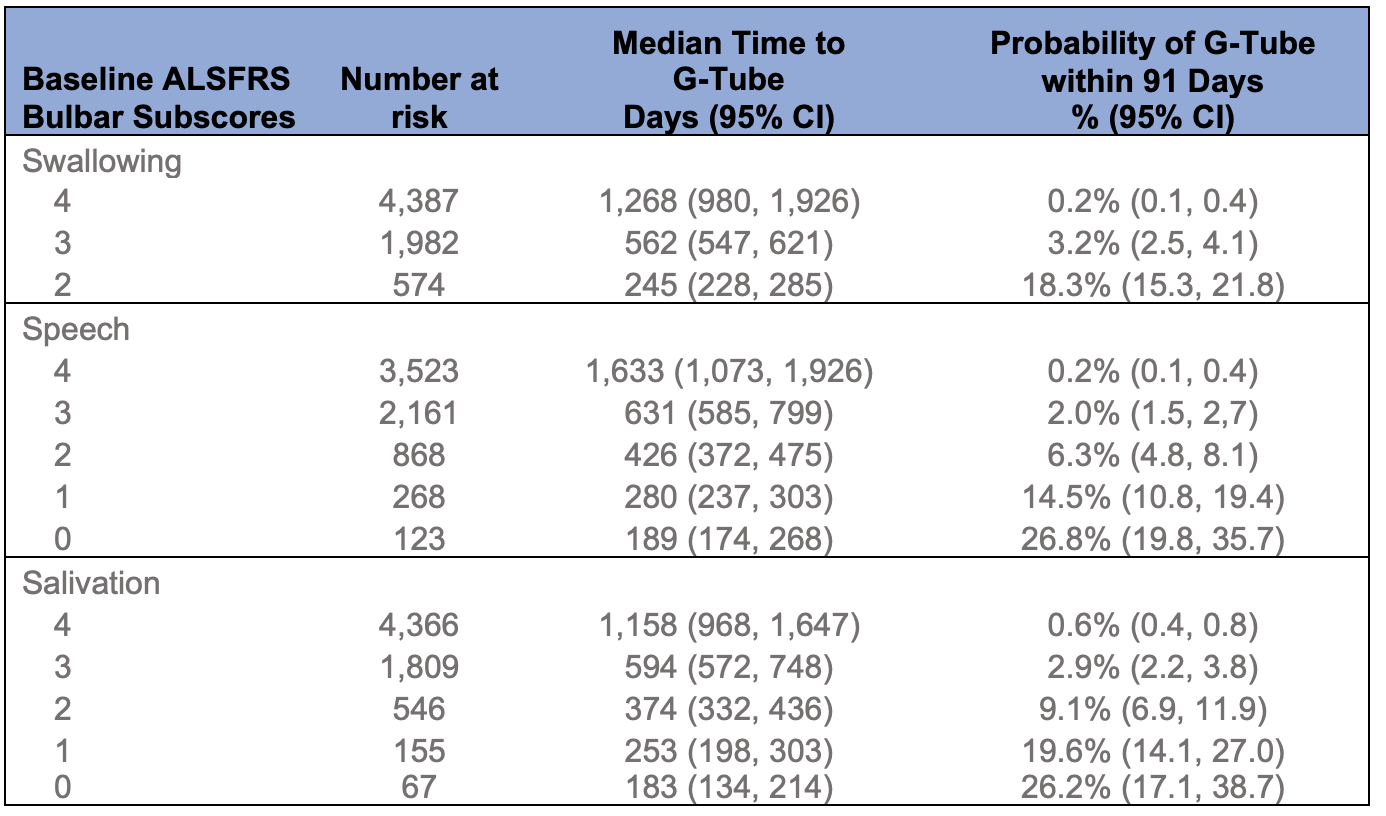
Table 2. Time to G-tube outcome after ALSFRS bulbar subscore transitions
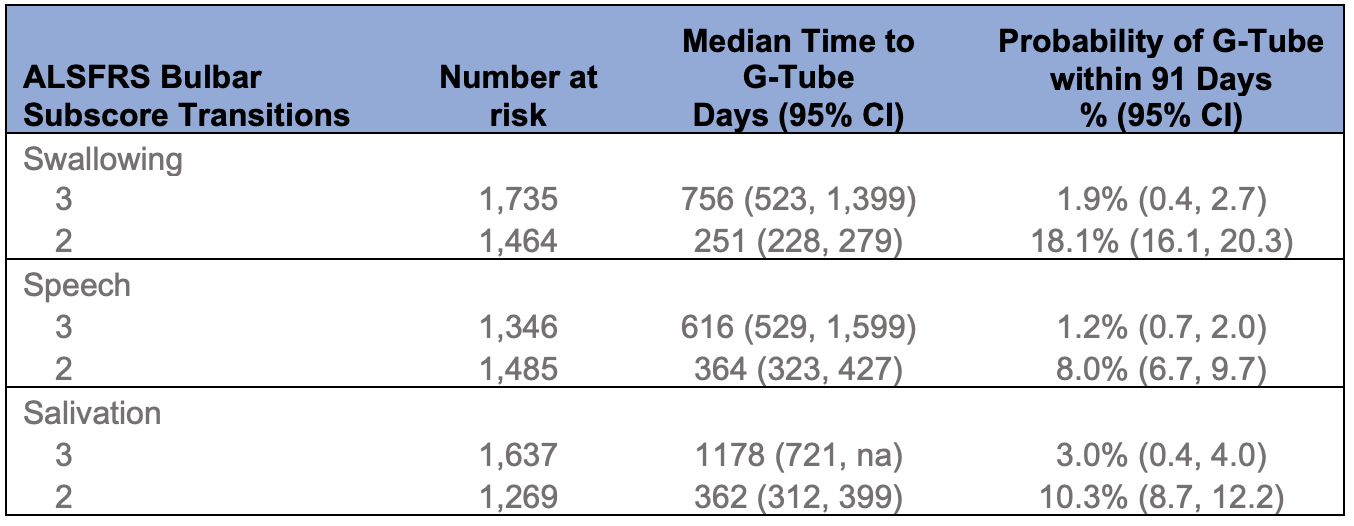
na = not available. The upper bound of the 95% confidence interval could not be estimated.
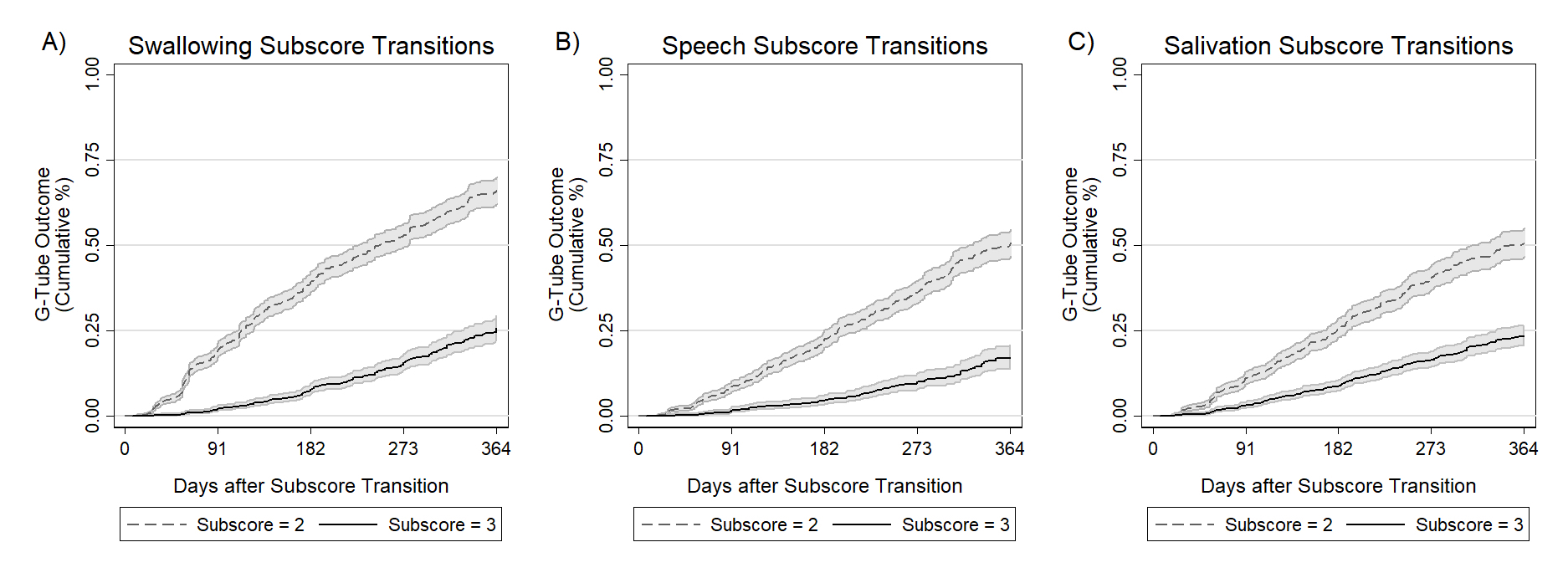
Figure 2. Kaplan-Meier failure curves showing the cumulative percentage of participants meeting the G-tube outcome after subscore transitions to 2 and 3 for each of A) swallowing, B) speech, and C) salivation subscores. Lower subscores indicate worse functional status. 95% confidence intervals are shown in grey.
Conclusions
- Time to G-tube decreases and 91-day risk increases with decreasing bulbar subscores
- Transition from 3 to 2 is an important inflexion point in bulbar subscores as seen by time to outcome from transition and % reaching outcome within 91 days
- Closer clinical monitoring around this inflexion point may be helpful
- ALSFRS could be added to other clinical parameters positively associated with gastrostomy tube insertion such as body mass index, and tracheostomy tube insertion2,3
References 1. Vergonjeanne M, Fayemendy P, Marin B, Penoty M, Lautrette G, Sourisseau H, et al. Predictive factors for gastrostomy at time of diagnosis and impact on survival in patients with amyotrophic lateral sclerosis. Clin Nutr. 2020 Oct;39(10):3112–8. 2. Albert SM, Murphy PL, Del Bene M, Rowland LP, Mitsumoto H. Incidence and predictors of PEG placement in ALS/MND. J Neurol Sci. 2001 Oct;191(1–2):115–9.
Long-term safety and efficacy of zilucoplan in myasthenia gravis: Additional interim analyses of RAISE-XT
Introduction
- Zilucoplan, a complement C5 inhibitor, showed significant MG-specific improvement in patients with AChR Ab+ gMG in the randomised, double-blind, placebo-controlled, Phase 3 RAISE study (NCT04115293)1
- Long-term data from RAISE-XT (NCT04225871), an ongoing OLE, will enhance our understanding of the safety and efficacy of zilucoplan in adults with gMG
- Here, we evaluate the safety and efficacy of zilucoplan up to 96 weeks in RAISE-XT
- RAISE-XT, a Phase 3, multicentre, OLE study, included patients who participated in the double-blind Phase 2 (NCT03315130) and Phase 3 (NCT04115293) zilucoplan studies
- Patients self-administered daily subcutaneous zilucoplan 0.3 mg/kg injections
- Primary outcome was incidence of TEAEs and secondary outcomes included change from baseline in MG-ADL score
Results
- RAISE-XT included a broad, mild-to-severe gMG population (Table 1)
- At data cut-off (11 May 2023), median (range) exposure to zilucoplan was 1.8 (0.11–5.1) years
- TEAEs occurred in 191 (95.5%) patients; the most common TEAE was COVID-19 (Table 2)
-
Mean CFB in MG-ADL score (Figure 1):
- Increased rapidly at Week 1 in those who switched from placebo to zilucoplan
- Continued to improve through to Week 24 and was sustained to Week 96 for pooled zilucoplan patients
- Similar improvements were observed for QMG, MGC, MG-QoL 15r and Neuro-QoL fatigue scores
- MG-ADL responder rates were high and sustained through to Week 96 (Figure 2)
- MSE responder rates increased rapidly and continued to improve through to Week 96 (Figure 2)
- Complete complement inhibition was maintained during RAISE-XT, including in those patients who received zilucoplan with IVIg and PLEX concomitantly (Figure 3)
Table 1 Patient demographics and baseline disease characteristics
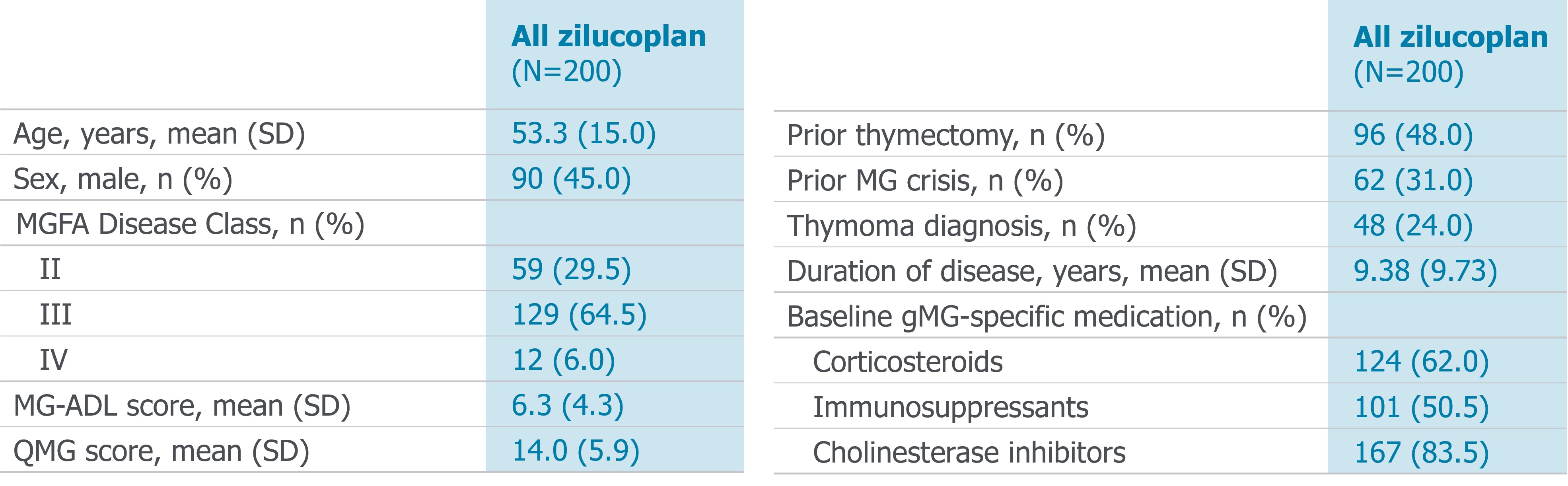
Table 2 Overview of TEAEs
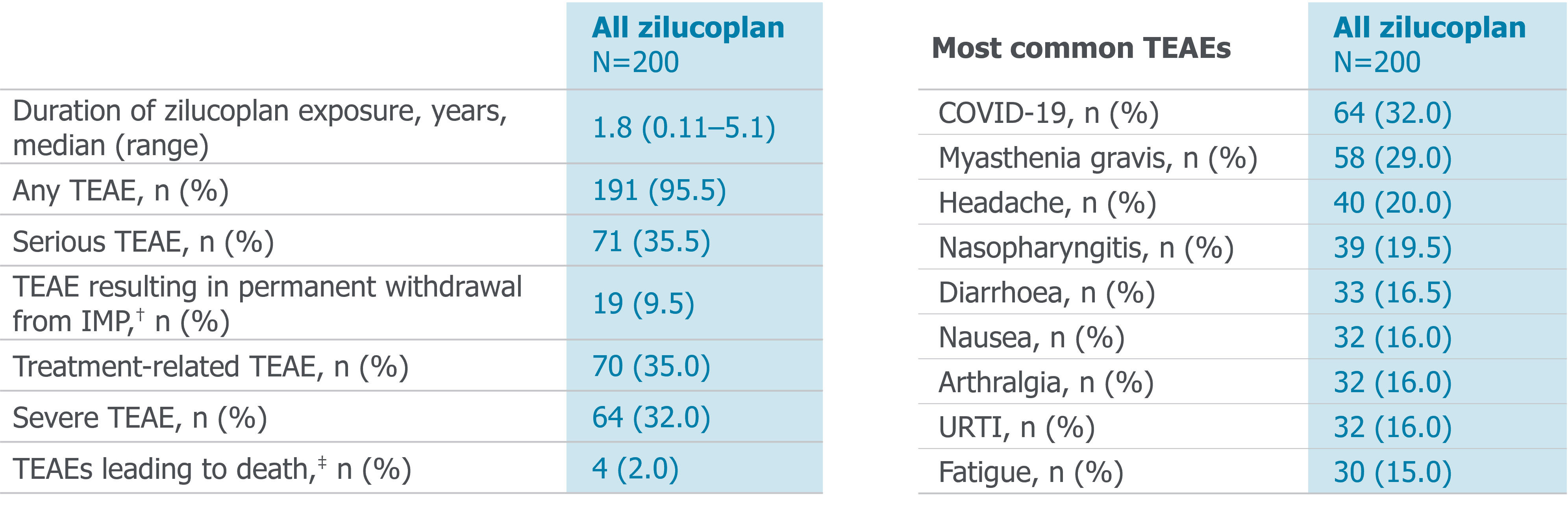
†Includes all deaths. ‡No deaths were considered treatment related. TEAEs leading to death included cardiac arrest (n=2) and accidental head injury (n=1) in the zilucoplan 0.3 mg/kg / 0.3 mg/kg group, and death from an unknown cause (n=1) in the placebo / zilucoplan 0.3 mg/kg group. Most common TEAEs occurring in ≥15% of patients overall are reported only.
Figure 1 Change from baseline in MG-ADL score to Week 96
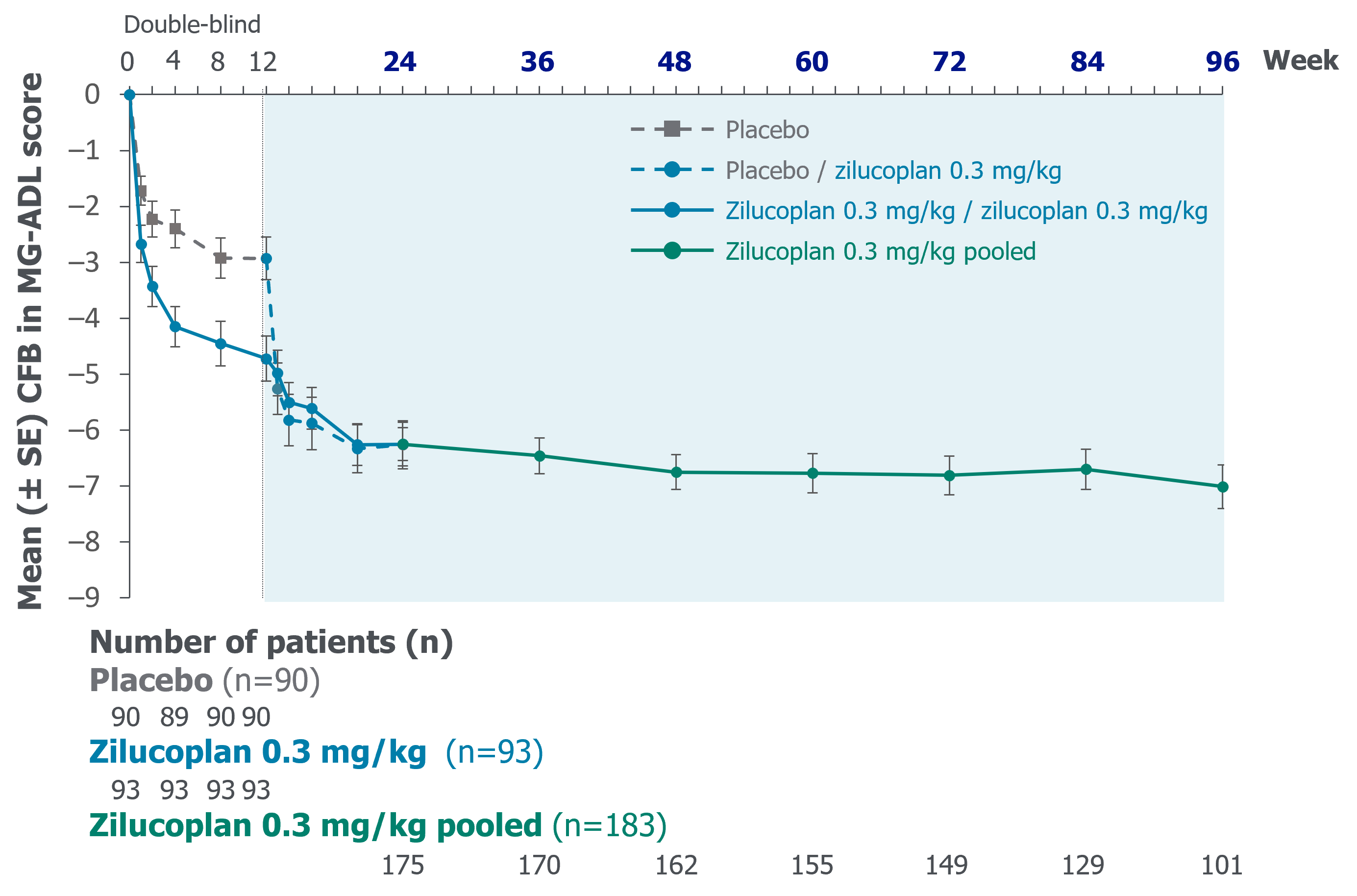
Summary and conclusions
Zilucoplan had a favourable safety profile and was well tolerated in the long term
There was a rapid improvement in symptoms, which was sustained through to Week 96
Complete complement inhibition was maintained after rescue therapy (IVIg or PLEX) during zilucoplan treatment, confirming that zilucoplan can be used concomitantly with IVIg or PLEX without the need for supplemental dosing
Zilucoplan had a favourable safety profile and was well tolerated in the long term
There was a rapid improvement in symptoms, which was sustained through to Week 96
Complete complement inhibition was maintained after rescue therapy (IVIg or PLEX) during zilucoplan treatment, confirming that zilucoplan can be used concomitantly with IVIg or PLEX without the need for supplemental dosing
Figure 2 MG-ADL and MSE responder rates to Week 96
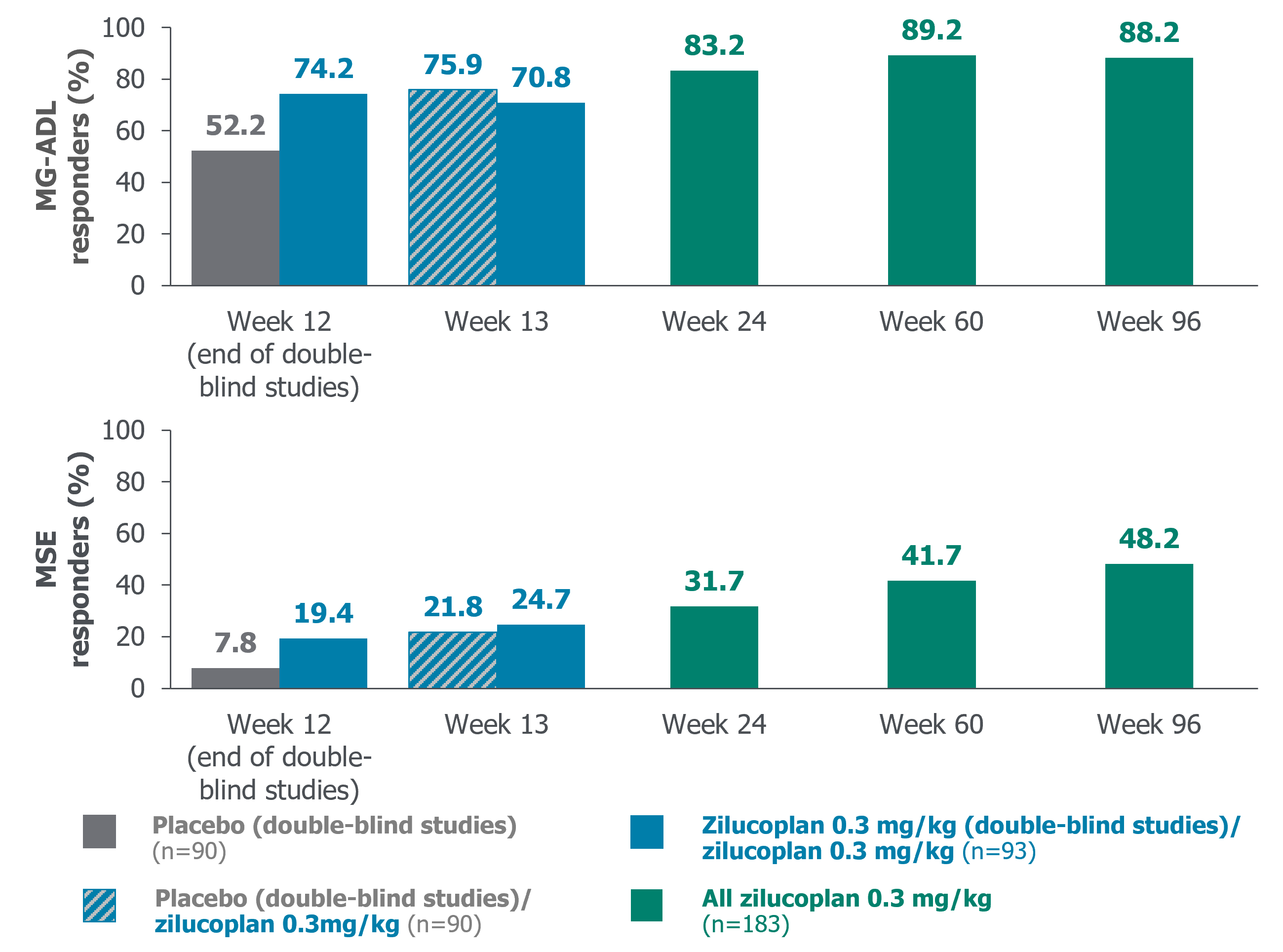
MG-ADL response: ≥3-point improvement from baseline in patients who have not received rescue therapy.
MSE response: Total MG-ADL score of 0 or 1 in patients who have not received rescue therapy.
MSE response: Total MG-ADL score of 0 or 1 in patients who have not received rescue therapy.
Figure 3 Complement inhibition during concomitant use of zilucoplan with IVIg and PLEX
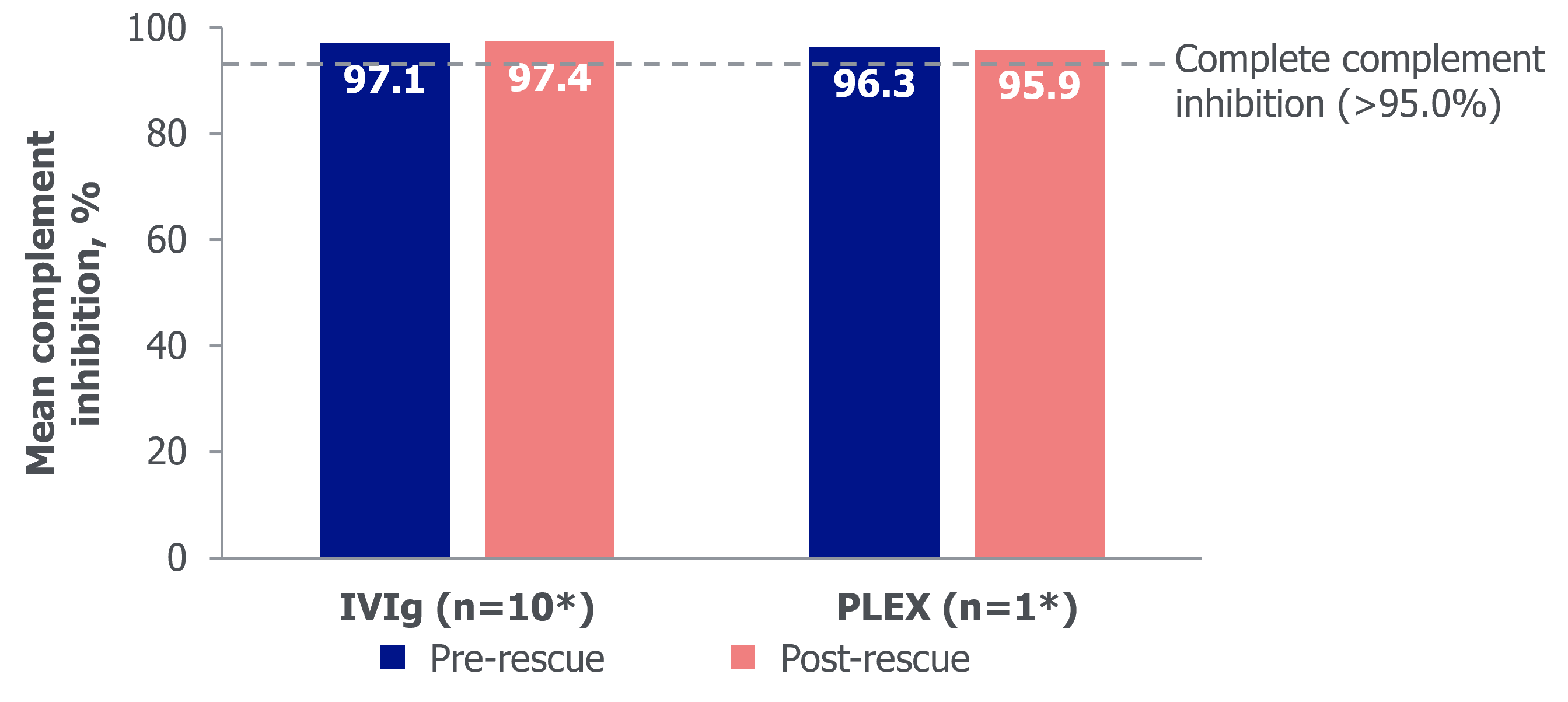
*Events with available data. Complement activity was measured by sRBC lysis assay, with post-administration measurement taken up to 1 day after rescue treatment. Data cut-off: 8 September 2022.
Corticosteroid dose tapering in patients with generalised myasthenia gravis on zilucoplan: Interim analysis of RAISE-XT
Introduction
- In the randomised, double-blind, placebo-controlled, 12-week, Phase 3 RAISE study (NCT04115293), the macrocyclic peptide complement C5 inhibitor zilucoplan significantly improved MG-specific outcomes in patients with AChR Ab+ gMG, with a favourable safety profile1
- Patients and physicians generally aim to reduce corticosteroid use where possible due to safety risks associated with long-term use2
- Per protocol, corticosteroid dose was kept stable in the Phase 2 study (NCT03315130), the RAISE study and during the first 12 weeks of the ongoing OLE study, RAISE-XT (NCT04225871)1,3
-
After the first 12 weeks of zilucoplan treatment in RAISE-XT, corticosteroid dose could be changed at the investigator’s discretion
- Here we evaluate changes in corticosteroid dose during RAISE-XT
Methods
-
RAISE-XT enrolled adult patients who completed either the Phase 2 or the RAISE study where they received either zilucoplan or placebo
- In RAISE-XT, patients self-administered SC zilucoplan 0.3 mg/kg daily
- The primary endpoint was the incidence of TEAEs
-
In this post hoc analysis, we assessed the proportion of patients who discontinued, reduced or increased their corticosteroid dose relative to the double-blind study baseline up to Week 120 (interim data cut-off date: 11 November 2023)
- Only patients receiving a corticosteroid at baseline were included in the analysis of patients who discontinued or reduced corticosteroids
- Patients who increased or started corticosteroids were evaluated as a proportion of the overall population
- Mean CFB in corticosteroid dose and MG-ADL score at Week 60 and Week 120 (Extension Weeks 48 and 108 of RAISE-XT, respectively) were evaluated for each category
Results
- Overall, 200 patients entered RAISE-XT (Table 1)
- At Week 120, of patients who were on corticosteroids at baseline and had data available, 33/54 (61.1%) had reduced the dose or discontinued corticosteroids (mean dose reduction: 15.5 mg) (Figures 1 and 2)
- Overall, 7/156 (4.5%) patients at Week 60 and 8/86 (9.3%) patients at Week 120 increased or started corticosteroids relative to double-blind baseline, with a mean dose increase of 13.2 mg and 11.6 mg, respectively
- Mean CFB in MG-ADL score was −6.6 (SD 3.6) in patients who discontinued or reduced their corticosteroid dose at Week 120 (Figure 1)
- Mean CFB in MG-ADL score was similar in patients who increased or started corticosteroids: −5.9 (SD 5.8) and −7.4 (SD 4.6) at Week 60 and Week 120, respectively
-
In the RAISE-XT overall population, TEAEs occurred in 194/200 (97.0%) patients
- The most frequently reported TEAEs were COVID-19 (71 [35.5%] patients) and MG (59 [29.5%] patients)
- 81/200 (40.5%) patients experienced a serious TEAE
- There was no meaningful difference in infection rates between patients who reduced their corticosteroid dose and those who did not (Table 2)
Table 1 Demographics and baseline disease characteristics
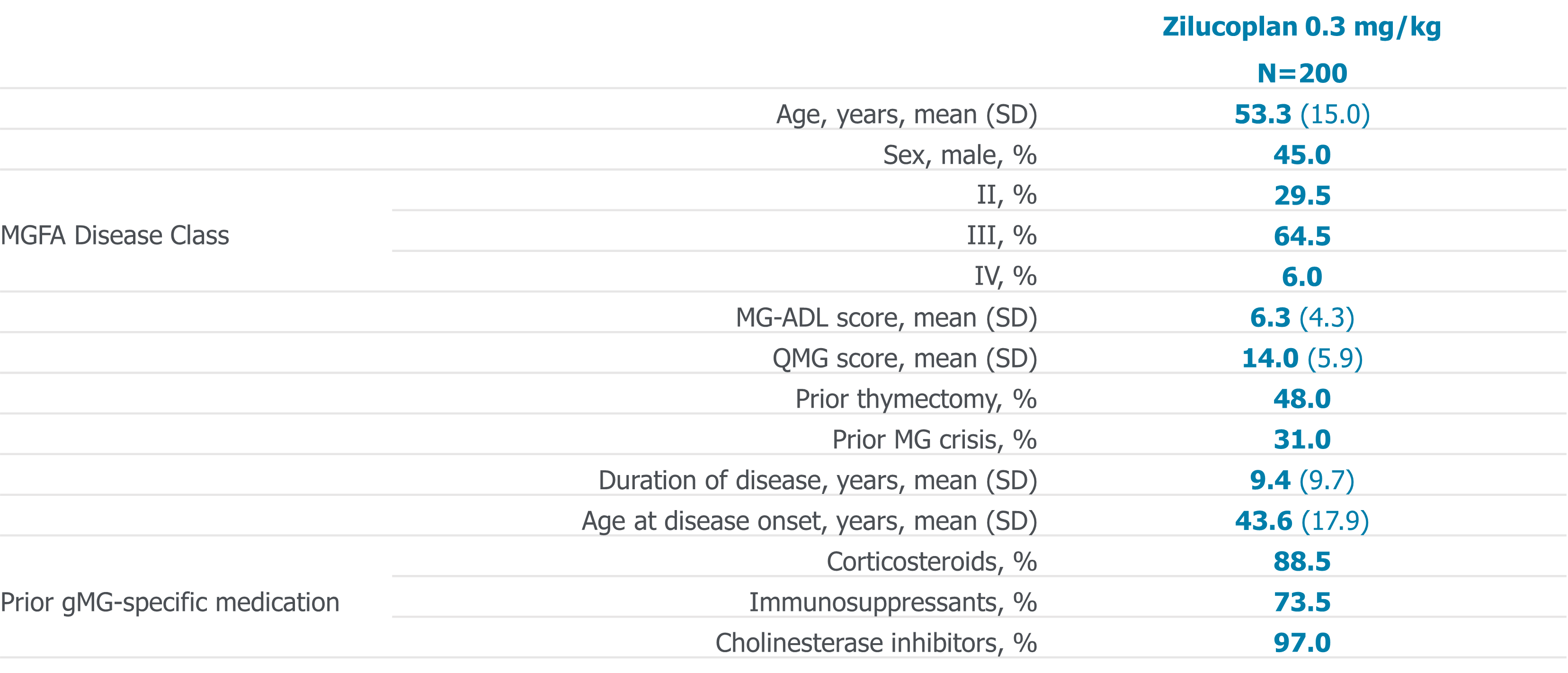
Figure 1 Proportions of patients in RAISE-XT who discontinued or reduced their corticosteroid dose*
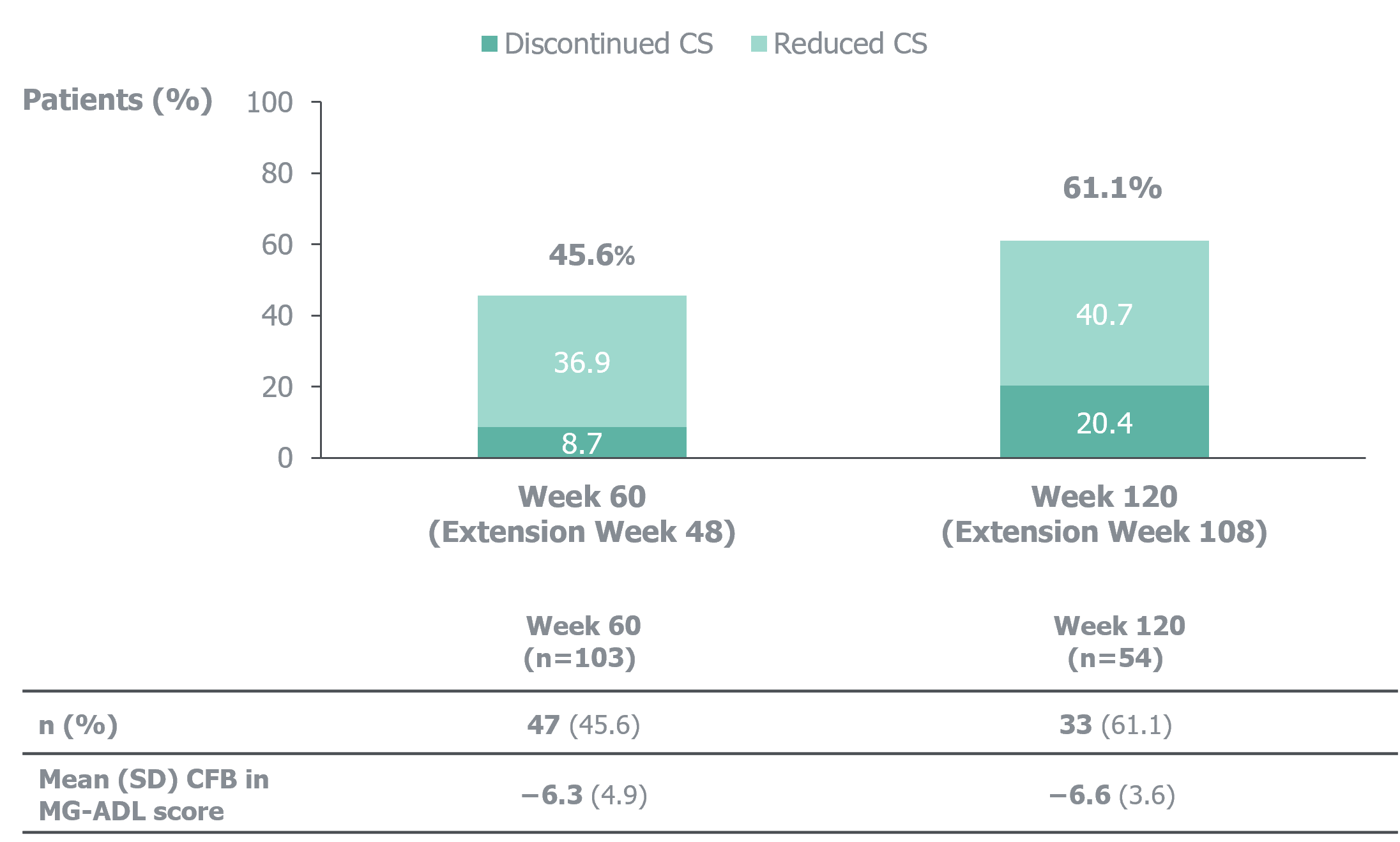
Corticosteroid dose remained stable prior to Week 24 (i.e., Extension Week 12 of RAISE-XT).
*Analysed in patients with >0 mg corticosteroid dose at baseline in the double-blind study.
*Analysed in patients with >0 mg corticosteroid dose at baseline in the double-blind study.
Summary and conclusions
This post hoc analysis investigated changes in concomitant corticosteroid dose among patients receiving zilucoplan in RAISE-XT
More than 60% of patients had reduced their dose or discontinued corticosteroids at Week 120 of zilucoplan treatment
Mean reductions from baseline in MG-ADL up to Week 120 were similar in patients who discontinued, decreased or increased their corticosteroid dose
Sustained efficacy with zilucoplan treatment for up to 120 weeks allows for tapering or discontinuation of concomitant corticosteroids, beneficial for managing the safety risks associated with long-term corticosteroid use
This post hoc analysis investigated changes in concomitant corticosteroid dose among patients receiving zilucoplan in RAISE-XT
More than 60% of patients had reduced their dose or discontinued corticosteroids at Week 120 of zilucoplan treatment
Mean reductions from baseline in MG-ADL up to Week 120 were similar in patients who discontinued, decreased or increased their corticosteroid dose
Sustained efficacy with zilucoplan treatment for up to 120 weeks allows for tapering or discontinuation of concomitant corticosteroids, beneficial for managing the safety risks associated with long-term corticosteroid use
Figure 2 Corticosteroid dose change in patients who discontinued or reduced their corticosteroid dose*
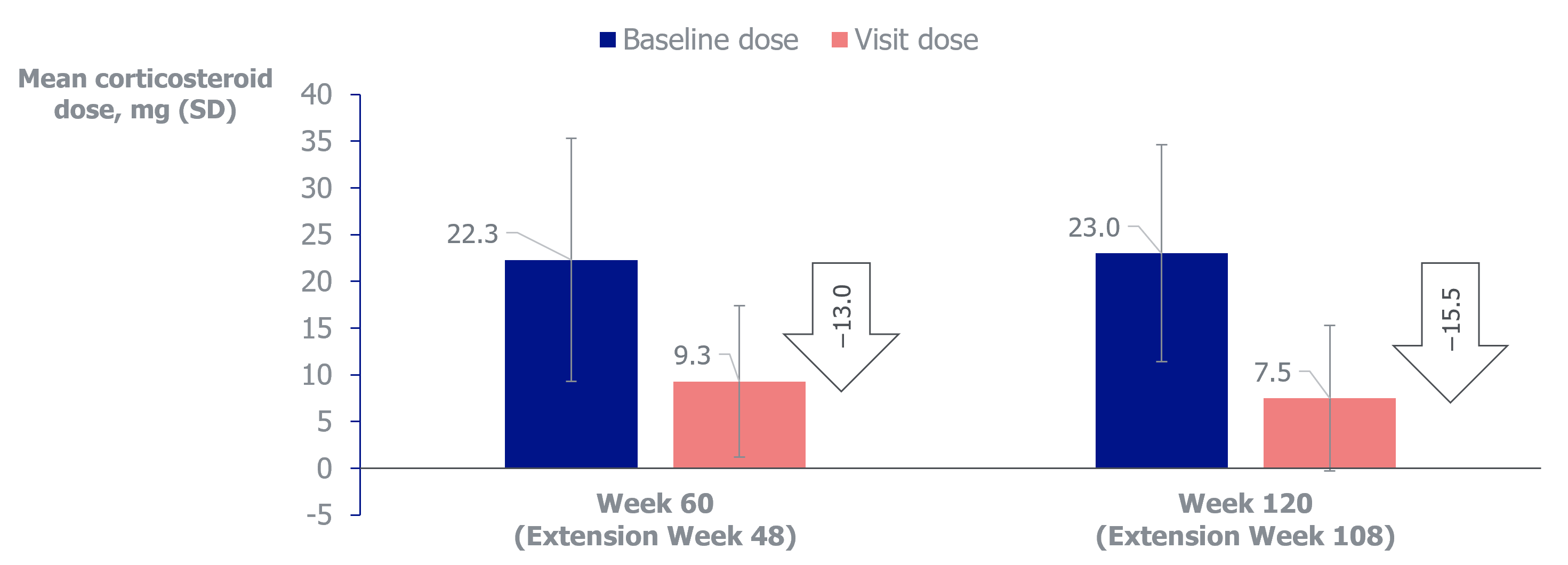
The daily corticosteroid dose was defined as the total prednisone-equivalent daily dose, summed across multiple corticosteroids taken. Corticosteroid dose remained stable prior to Week 24 (i.e., Extension Week 12). n=103 at Week 60 and n=54 at Week 120. *Analysed in patients with >0 mg corticosteroid dose at baseline in the double-blind study.
Table 2 Infection rates for corticosteroid dose cohorts
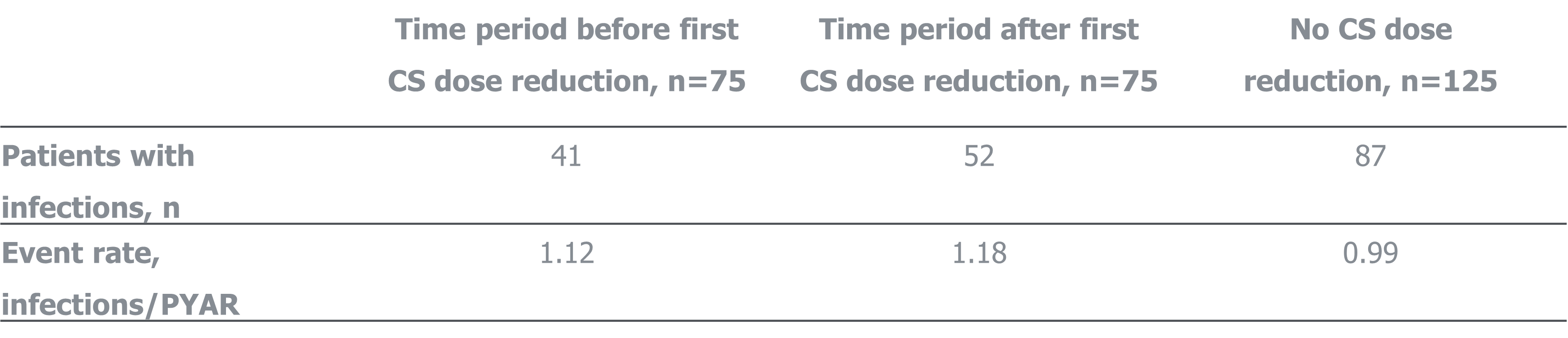
mITT population.
Real-World Reduction in Oral Corticosteroid Utilization Following Efgartigimod Initiation in Patients With Generalized Myasthenia Gravis


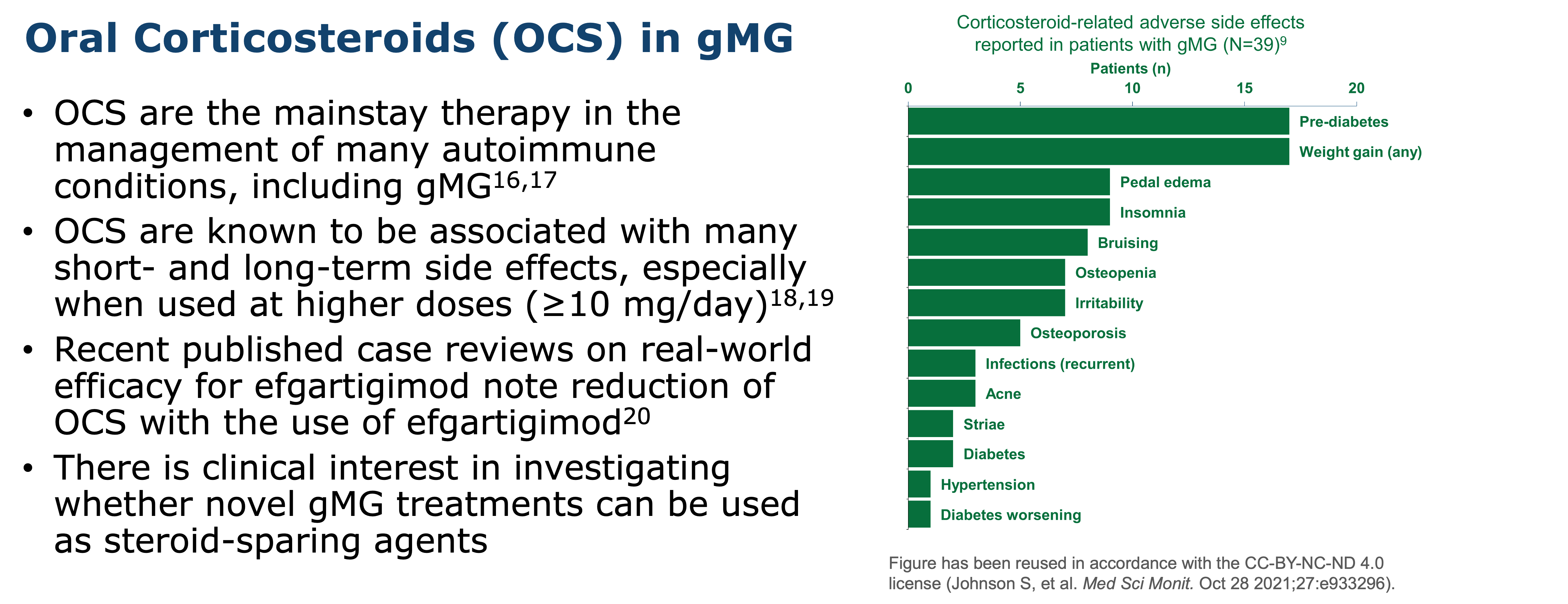
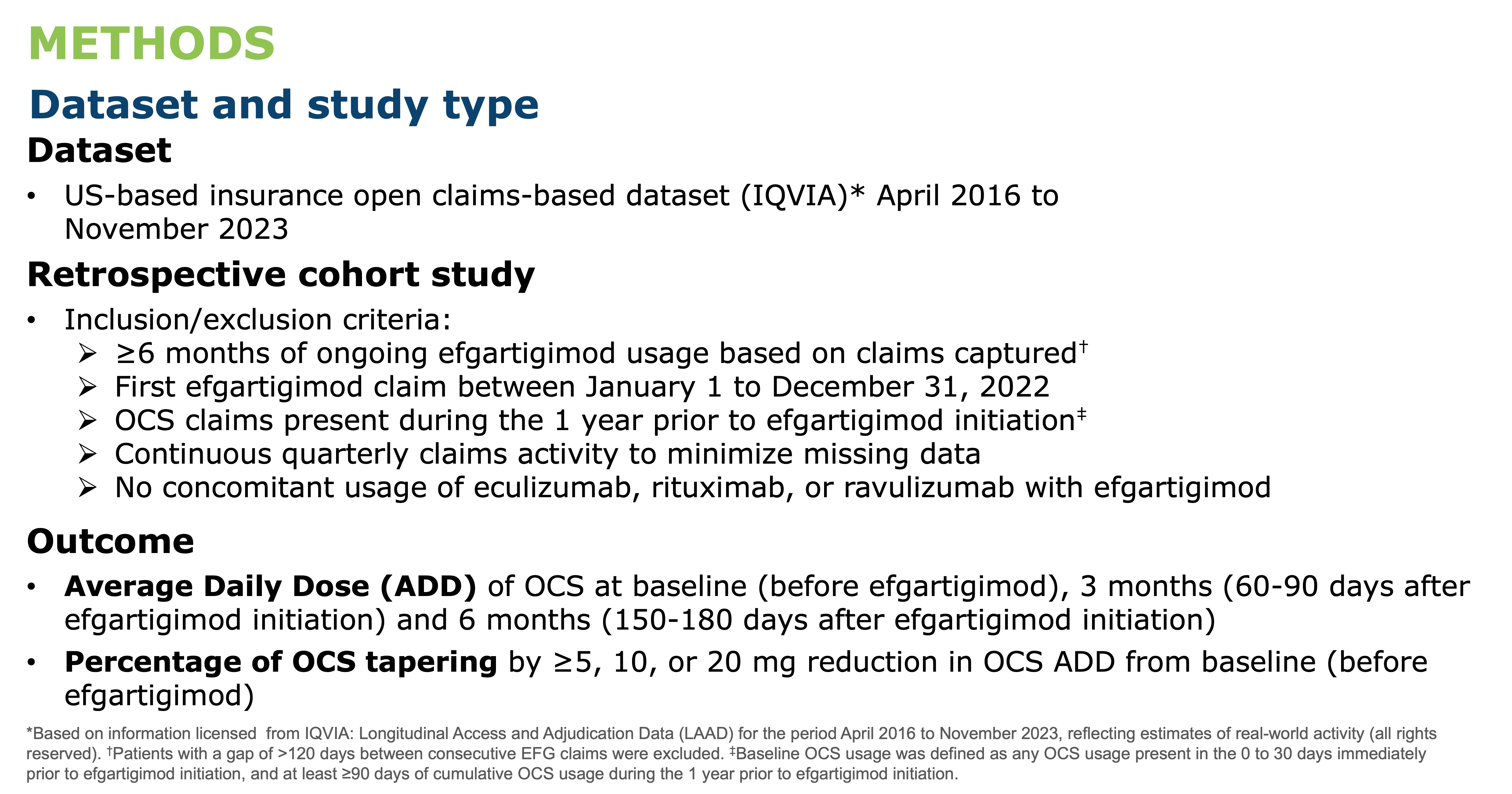
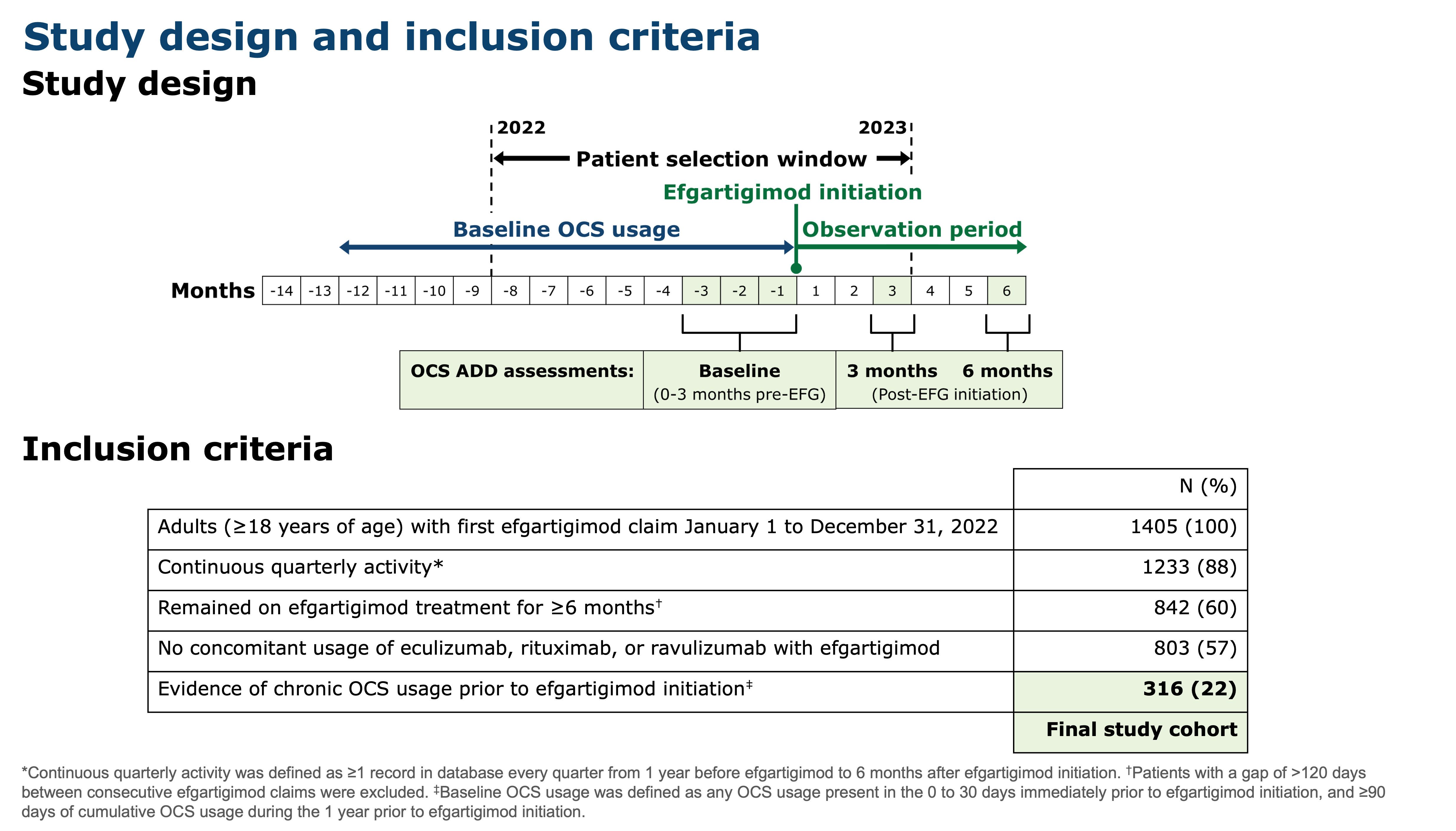
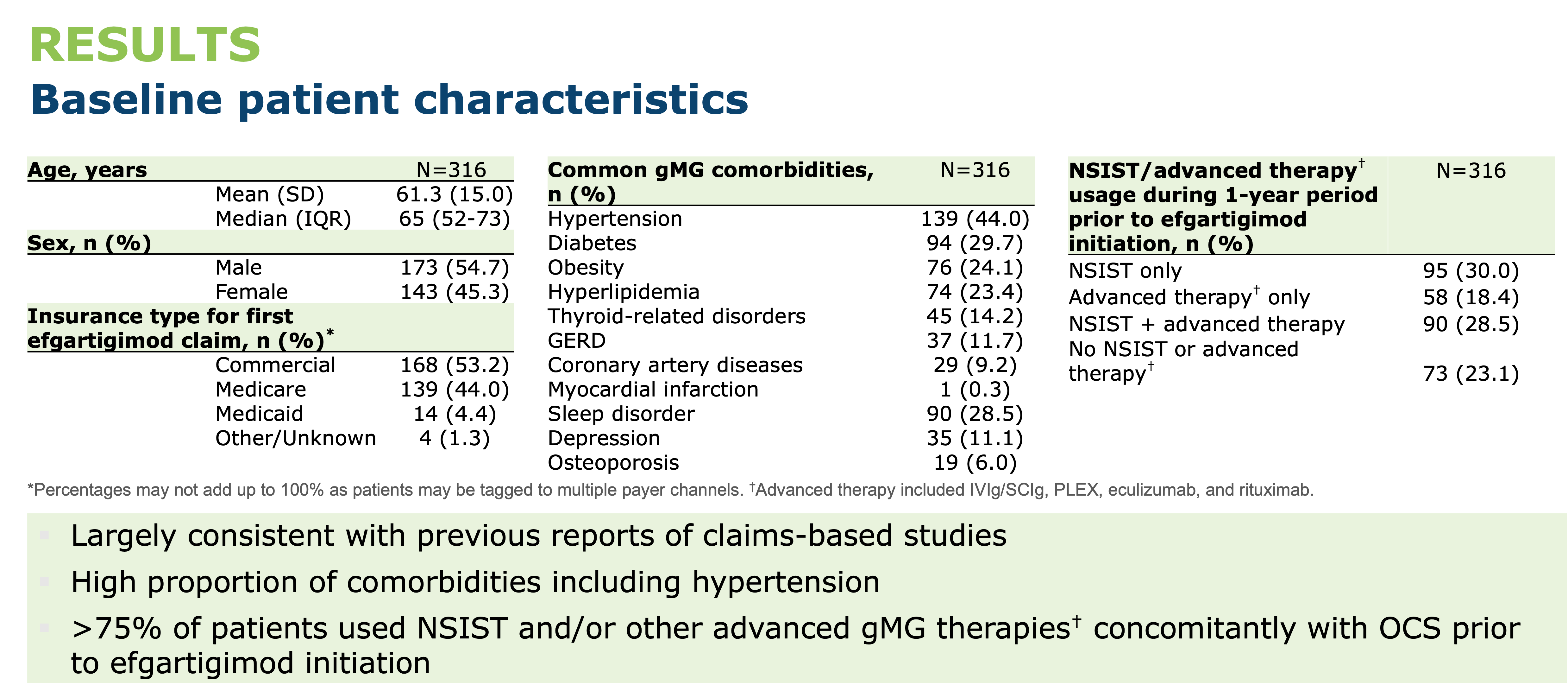
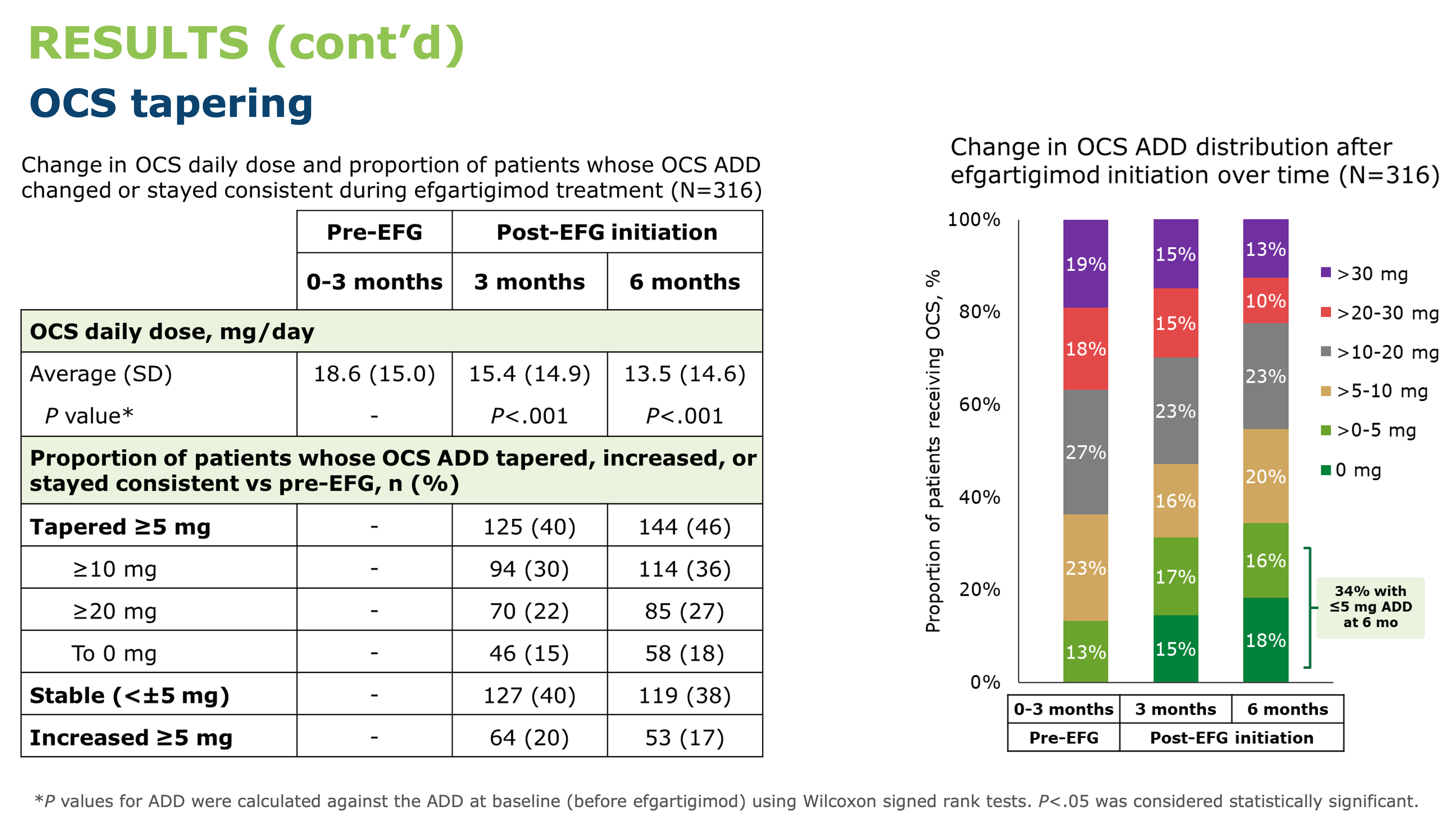
Neuromuscular neurologists’ experience in recognizing, diagnosing, and treating Long-chain fatty acid disorders (LC-FAOD): a national survey
Background
•LC-FAOD diagnoses may be missed in neuromuscular (NM) clinics due to its rarity and absence from common NM genetic panels.
•The Canadian Neuromuscular Disease Registry (CNDR) collects real-world patient data and includes a network of clinician-investigators.
•The objective of this study was to inform future registry work by evaluating diagnosis pathways for LC-FAOD patients and estimating the number followed at Canadian NM clinics.
•The Canadian Neuromuscular Disease Registry (CNDR) collects real-world patient data and includes a network of clinician-investigators.
•The objective of this study was to inform future registry work by evaluating diagnosis pathways for LC-FAOD patients and estimating the number followed at Canadian NM clinics.
Methods
•A questionnaire was developed with an expert committee and circulated to 111 CNDR-affiliated NM neurologists across the country.
Fig. 1 – 12 neurologists in 5 provinces completed the survey, a response rate of 10.8%. There were no survey respondents from any other provinces.
•8 respondents were adult-treating practitioners, 3 pediatric, and 1 treating both adult and pediatric
•11 respondents (91.7%) had been practicing medicine for >10 years.
•11 respondents (91.7%) had been practicing medicine for >10 years.
Results
•Agreement trends existed between definition of, and tests to evaluate, rhabdomyolysis.
•All 12 indicated they would perform further investigations for a patient with rhabdomyolysis with no obvious trigger after either a single episode (n=4) or 2-3 episodes (n=8).
•All 12 indicated they would perform further investigations for a patient with rhabdomyolysis with no obvious trigger after either a single episode (n=4) or 2-3 episodes (n=8).
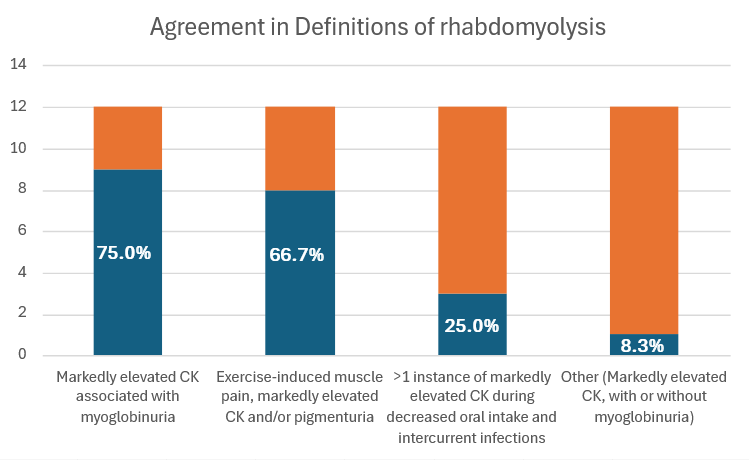
Fig. 2 – Clinician agreement on possible definitions of rhabdomyolysis.
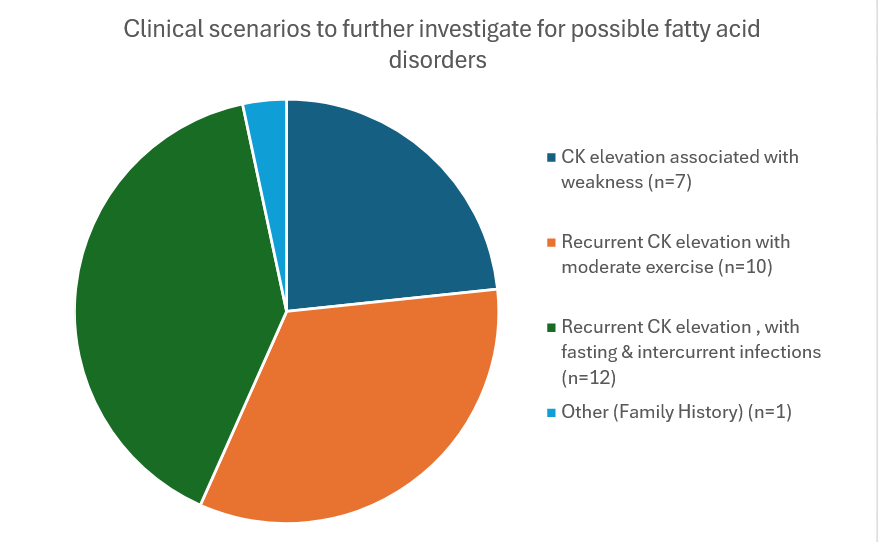
Fig. 3 – Clinician identification of scenarios warranting further investigation for possible fatty acid disorders
Results
Table 1. Clinician selection of clinical features and tests to evaluate for rhabdomyolysis

•4 clinics routinely follow LC-FAOD patients.
•9 respondents had diagnosed a patient with LC-FAOD.
•In the last 1-2 years, respondents followed an estimated 91 patients with LC-FAOD (mean=7.5 per clinic).
•9 respondents had diagnosed a patient with LC-FAOD.
•In the last 1-2 years, respondents followed an estimated 91 patients with LC-FAOD (mean=7.5 per clinic).
Table 2. Estimated # of patients followed by respondents diagnosed in the last 1-2 years with the listed diseases.
Note: 1 clinician diagnosed 30 patients with Mitochondrial myopathies; all other respondents diagnosed 5 or fewer patients within the past 1-2 yearsResults
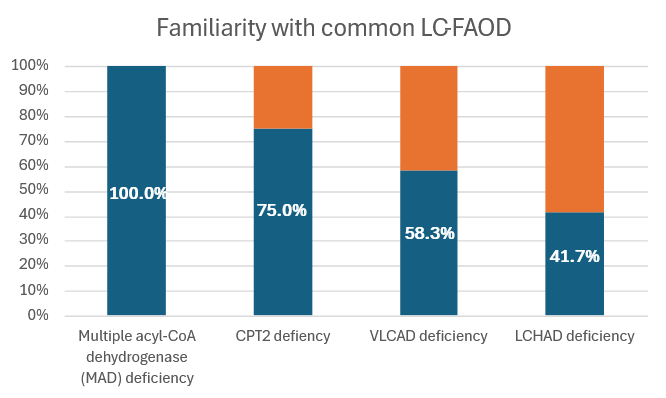
Fig. 4 – Clinician familiarity with common LC-FAOD
•All respondents were familiar with CPT2 deficiency
•N=5 were familiar with all four diseases.
•Of the remaining 7 respondents:
oN=3 selected only CPT2 deficiency
oN=2 selected only CPT & VLCAD deficiency
oN=2 selected CPT2, VLCAD, & LCHAD deficiency
•N=5 were familiar with all four diseases.
•Of the remaining 7 respondents:
oN=3 selected only CPT2 deficiency
oN=2 selected only CPT & VLCAD deficiency
oN=2 selected CPT2, VLCAD, & LCHAD deficiency
Fig. 5 – Clinician preferences for continuing education
•83.3% never received continuing education on LC-FAOD, though 75% indicated interest in expert-led webinars.
Conclusion
•Low sample size limits conclusions.
•Results suggest LC-FAOD may be under-diagnosed or not routinely followed by NM specialists, limiting viability of an LC-FAOD registry. Practitioners may be interested in LC-FAOD-specific education.
•Future work: Collaboration with metabolic geneticists on education initiatives to raise awareness.
•Results suggest LC-FAOD may be under-diagnosed or not routinely followed by NM specialists, limiting viability of an LC-FAOD registry. Practitioners may be interested in LC-FAOD-specific education.
•Future work: Collaboration with metabolic geneticists on education initiatives to raise awareness.
ACKNOWLEDGEMENTS: Funding for this study was provided by Ultragenyx Pharmaceutical
Achievement of Minimal Symptom Expression in Acetylcholine Receptor Antibody-Positive Participants Treated With Efgartigimod in ADAPT/ADAPT+
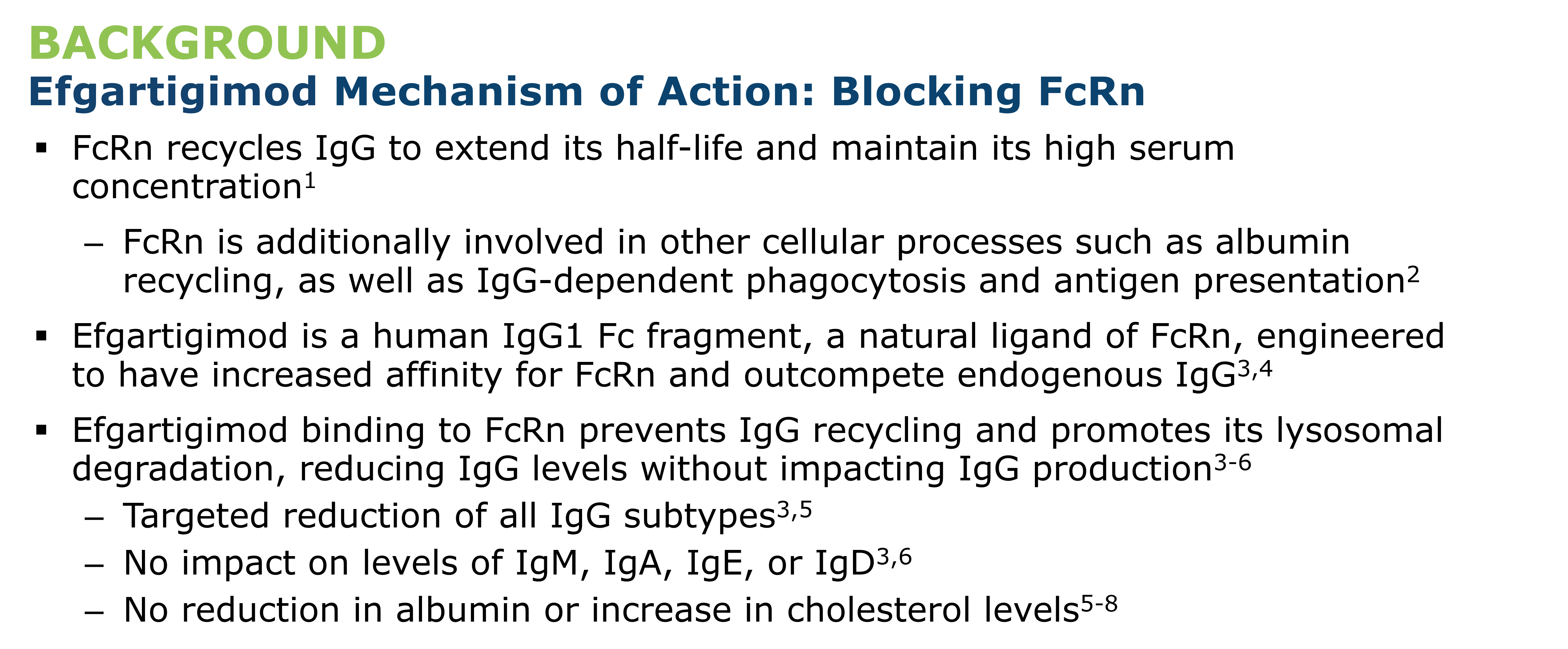

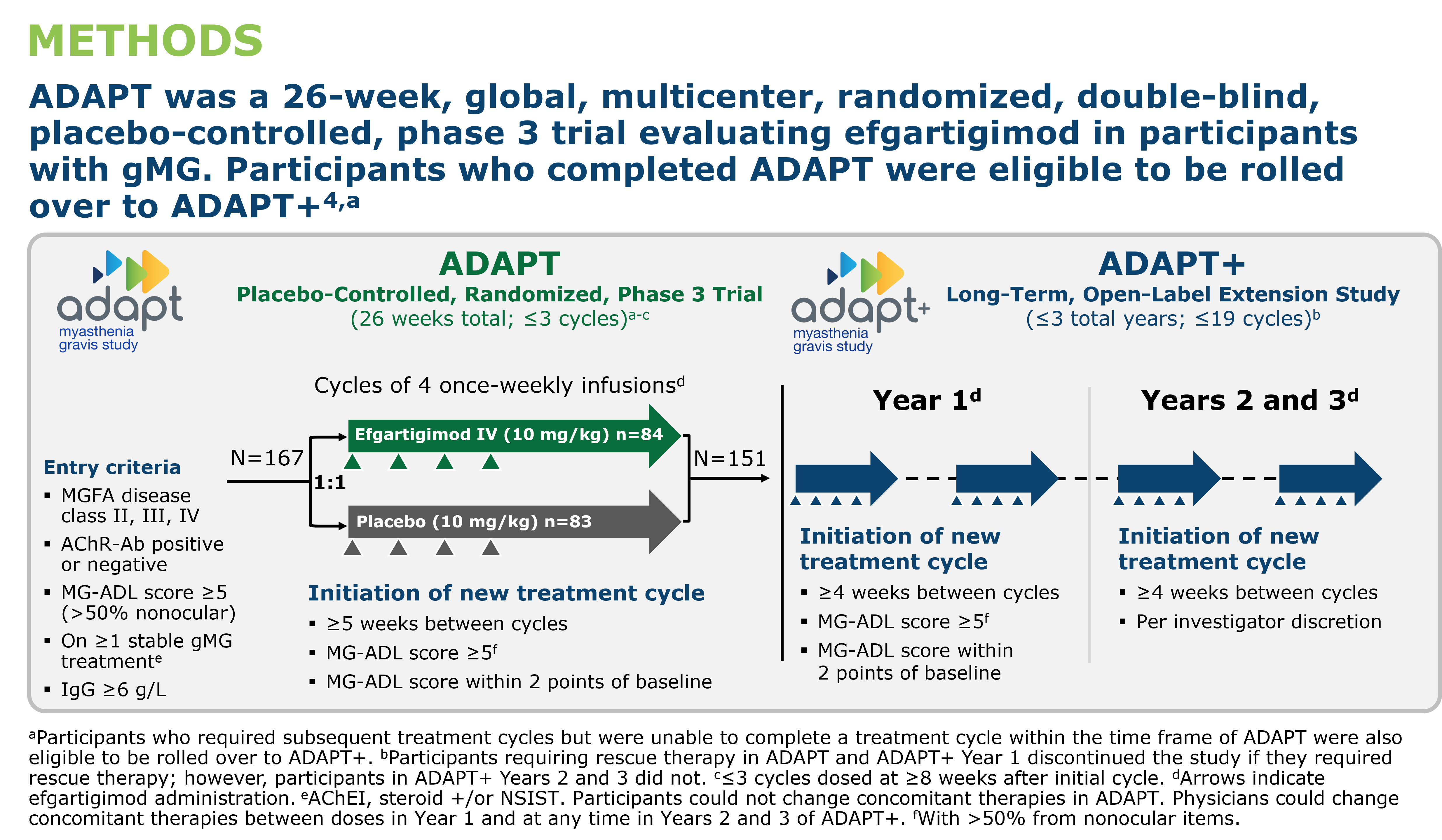
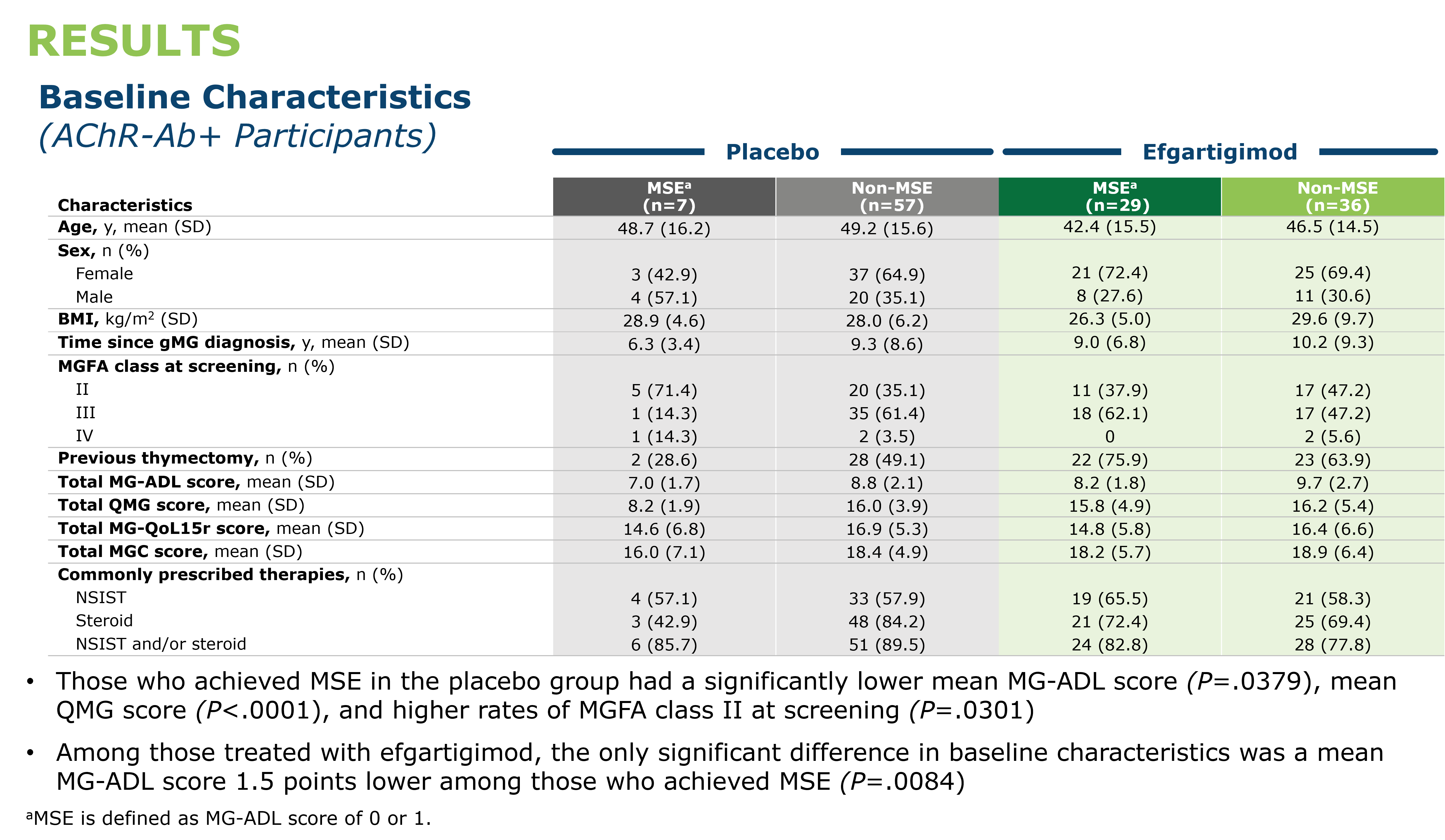
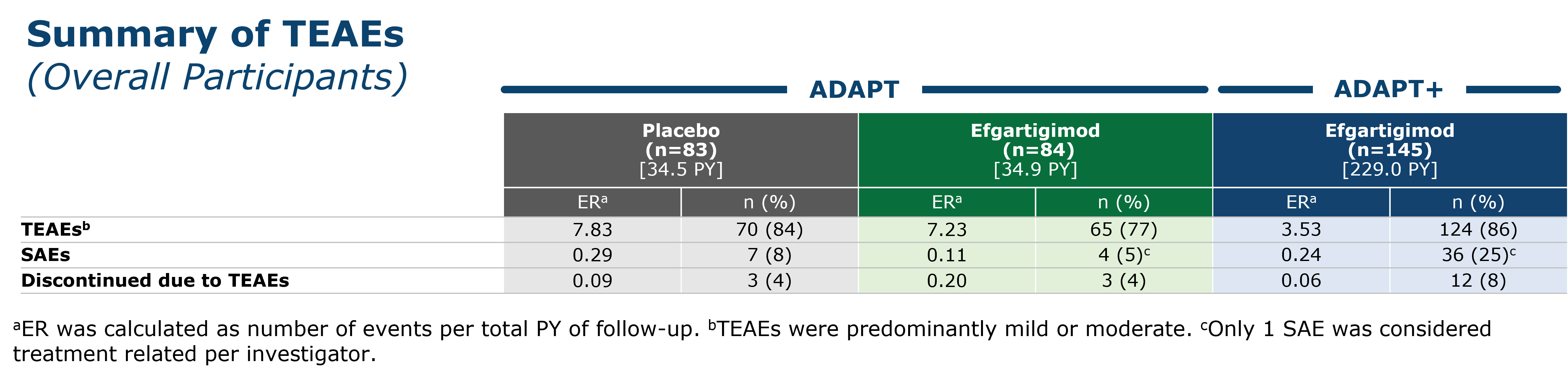
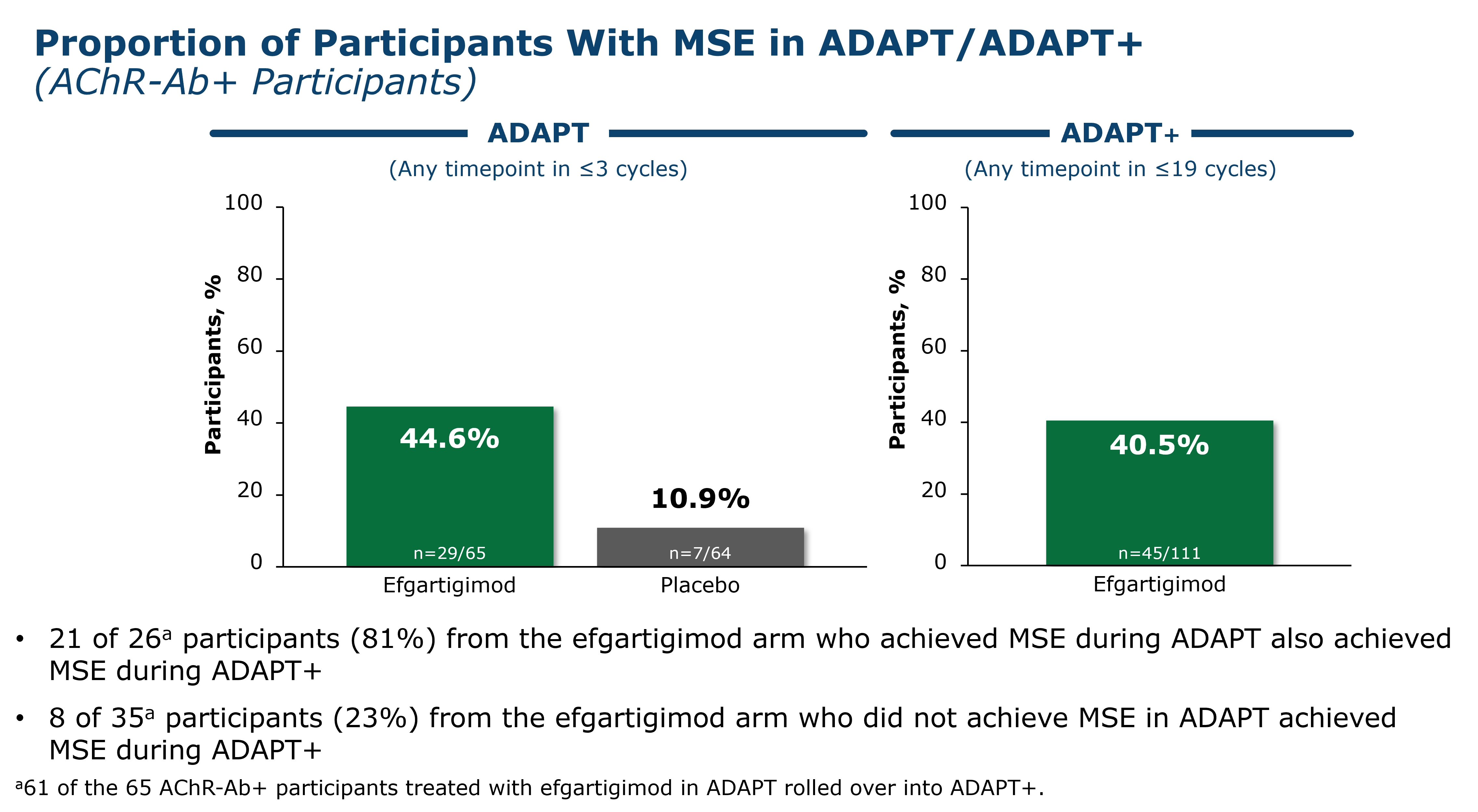

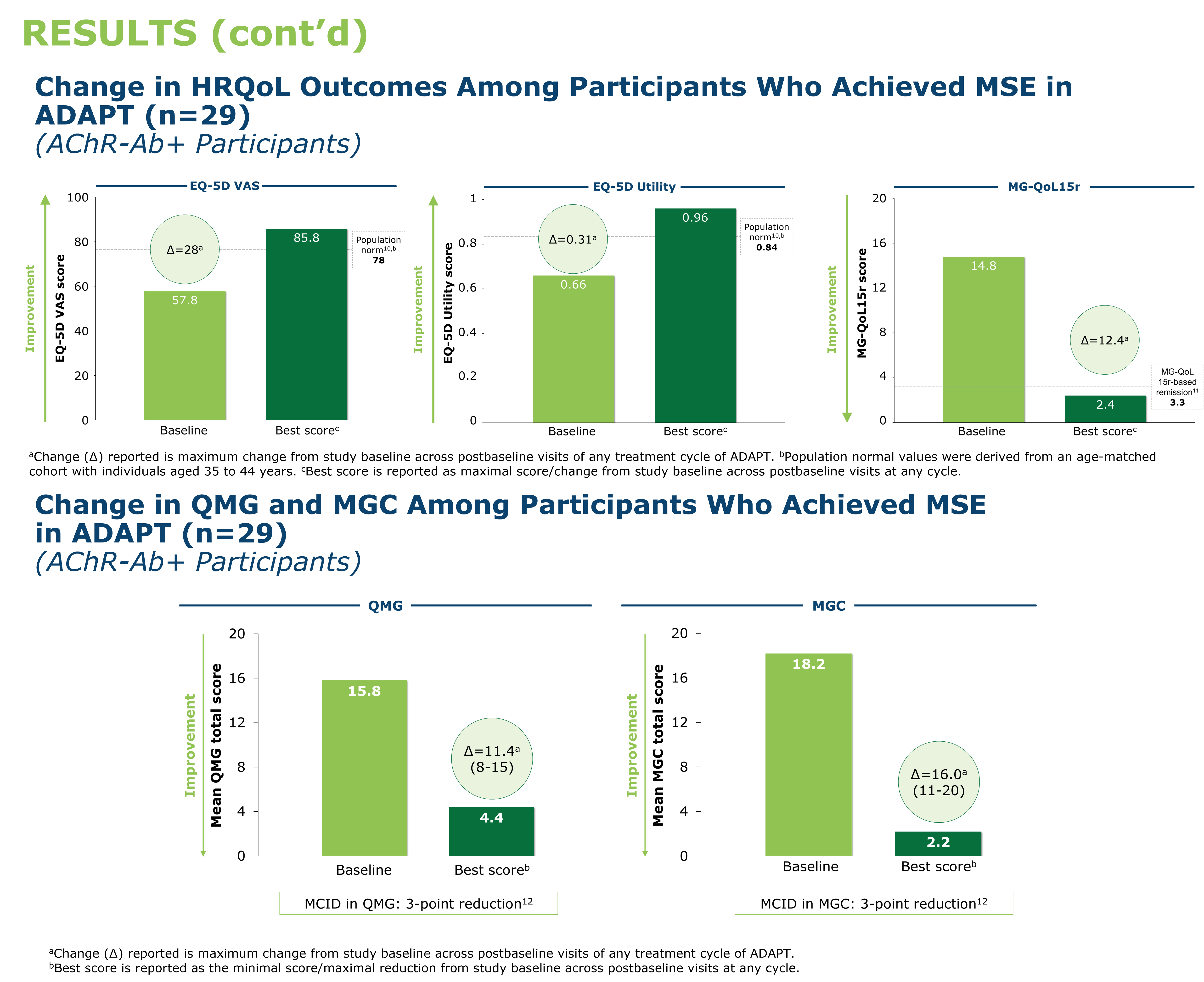
Provider and patient perspectives on outcome measure use in clinical care for chronic inflammatory neuropathy

BACKGROUND
-
Chronic Inflammatory Neuropathies (CIN) are disabling autoimmune neuromuscular disorders.
-
A set of outcome measures are recommended for trials in CIN, yet they are not widely used in routine clinical care.
-
Patient and provider feedback is key in the successful implementation of a team-based outcome measure program that adds value and avoids unnecessary burden.
Project goals:
-
Compare the patient and provider perspectives on the utility of using outcome measures in clinical settings.
-
Identify barriers to outcome measure use and areas of improvement in clinical settings.
METHODS
1. A set of nine outcome measures were administered in routine practice for CIN patients over one year. The panel included patient-reported and functional outcome measures.
2. Five providers (two neurologists, one nurse, two research assistants) and 25 participants with a diagnosis of CIN completed an online questionnaire on their experience. The questionnaire included scales and free-text fields.
RESULTS
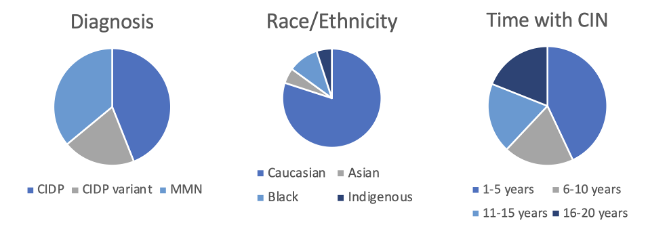
CIN participant demographics: 25 participants (mean age = 59.9 years; 10 females).
Comparing patient and provider perspectives on the utility of outcome measures:

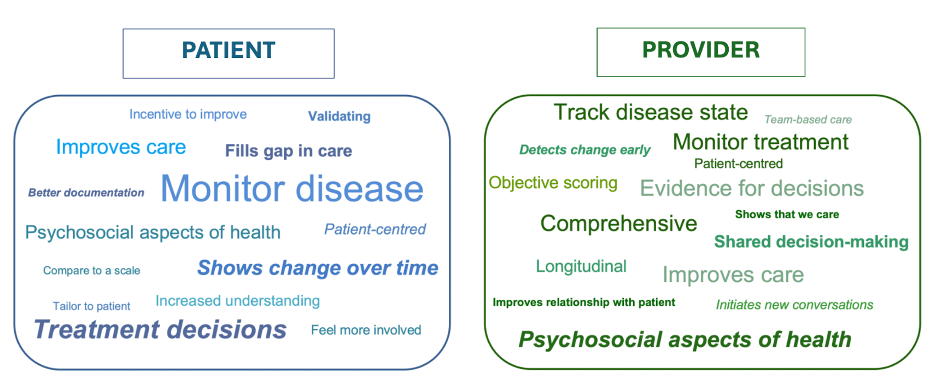
Word clouds representing entries from free-text fields related to outcome measure use.


CONCLUSIONS
-
CIN patients and providers recognize the value of integrating outcome measures into routine care.
-
Outcome measurement should be adapted to meet patient and provider preferences.
-
Providers emphasized integration into EMRs and streamlining processes.

Introduction
- CMT
- AD / AR / X (D/R) / de novo
- 1 / 2 / 4 / DI
- Penetrance ~complete with some variability
- Asymptomatic CMT1A patients described after discovery from severe neurotoxic effects of chemotherapy (i.e., vincristine)1,2 or development of CIDP.3
- Carvalho et al. described 17 patients with CMT1A with an average median motor CV of 16.7 m/s with a range of 5 to 26.5 m/s.4
- Birouk et al. studied 119 CMT1A patients and found an average median motor CV of 20.2 m/s with a range of 7 to 33 m/s.5
- No studies described asymptomatic patients with normal NCSs
- This is the first report to document normal (or near normal) non-demyelinating NCSs in an adult man with genetically confirmed CMT1A
- AD / AR / X (D/R) / de novo
- 1 / 2 / 4 / DI
- Penetrance ~complete with some variability
- Asymptomatic CMT1A patients described after discovery from severe neurotoxic effects of chemotherapy (i.e., vincristine)1,2 or development of CIDP.3
- Carvalho et al. described 17 patients with CMT1A with an average median motor CV of 16.7 m/s with a range of 5 to 26.5 m/s.4
- Birouk et al. studied 119 CMT1A patients and found an average median motor CV of 20.2 m/s with a range of 7 to 33 m/s.5
- No studies described asymptomatic patients with normal NCSs
- This is the first report to document normal (or near normal) non-demyelinating NCSs in an adult man with genetically confirmed CMT1A
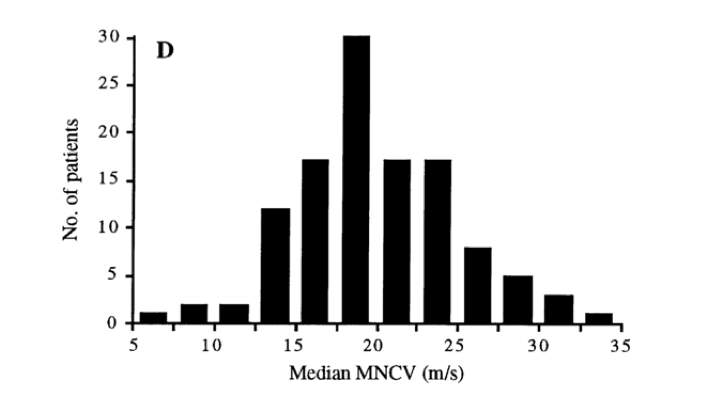
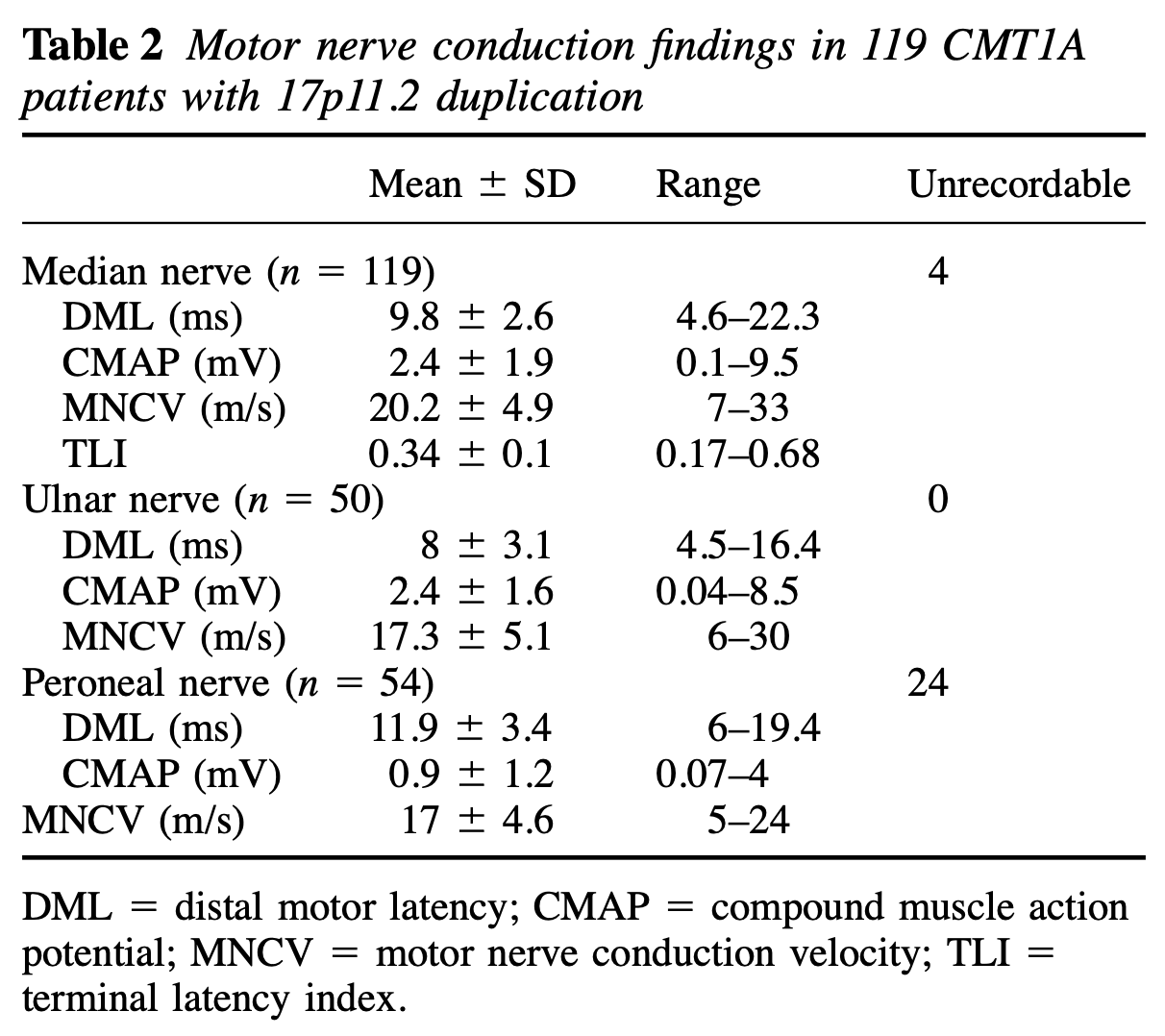
Figure 1. Distribution of median motor CVs in 119 CMT1A patients.
Case Report
A 42-year-old man was found to have CNV gains in 17q22.3 on microarray testing as part of a work-up for his son's delayed speech. Confirmation was obtained via direct duplication/deletion analysis (via LHSC).
He was neurologically intact:
- No S/G sensory loss;
- MRC 5/5 diffusely (including DF);
- MSRs +2 x all sites;
- Gait/coordination/station N
A 42-year-old man was found to have CNV gains in 17q22.3 on microarray testing as part of a work-up for his son's delayed speech. Confirmation was obtained via direct duplication/deletion analysis (via LHSC).
He was neurologically intact:
- No S/G sensory loss;
- MRC 5/5 diffusely (including DF);
- MSRs +2 x all sites;
- Gait/coordination/station N
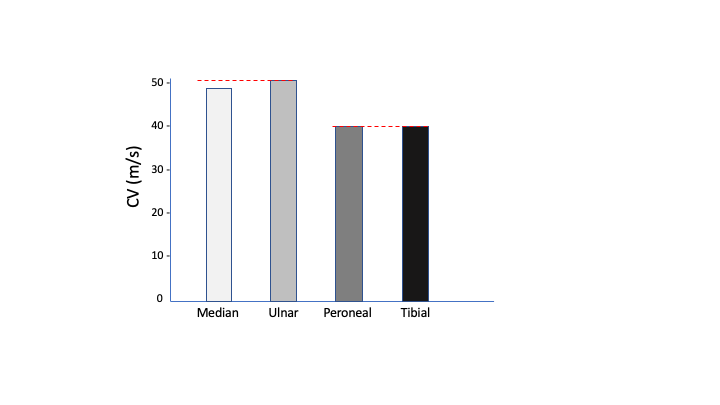
Figure 2. Nerve conduction data.
Conclusions
It can be assumed that phenotypic variability is predicated on genotypic variability.
This same variability appears to extend into the non-demyelinating range
Discovery of which genes afford this "protection" may serve as therapeutic targets.
Blood sent to S. Zuchner --> no results to date.
It can be assumed that phenotypic variability is predicated on genotypic variability.
This same variability appears to extend into the non-demyelinating range
Discovery of which genes afford this "protection" may serve as therapeutic targets.
Blood sent to S. Zuchner --> no results to date.
References
1. Jariwal R, Shoua B, Sabetian K, Natarajan P, Cobos E. Unmasking a Case of Asymptomatic Charcot-Marie-Tooth Disease (CMT1A) With Vincristine. J Investig Med High Impact Case Rep. 2018 Feb 26;6:2324709618758349. doi: 10.1177/2324709618758349. PMID: 29511693; PMCID: PMC5833168.
2. Holloway MP, DeNardo BD, Phornphutkul C, Nguyen K, Davis C, Jackson C, Richendrfer H, Creton R, Altura RA. An asymptomatic mutation complicating severe chemotherapy-induced peripheral neuropathy (CIPN): a case for personalised medicine and a zebrafish model of CIPN. NPJ Genom Med. 2016 Jun 8;1:16016. doi: 10.1038/npjgenmed.2016.16. PMID: 29263815; PMCID: PMC5685301.
3.Rajabally Y, Vital A, Ferrer X, Vital C, Julien J, Latour P, Vandenberghe A, Lagueny A. Chronic inflammatory demyelinating polyneuropathy caused by HIV infection in a patient with asymptomatic CMT 1A. J Peripher Nerv Syst. 2000 Sep;5(3):158-62. doi: 10.1046/j.1529-8027.2000.00014.x. PMID: 11442172.
4. Carvalho AA, Vital A, Ferrer X, Latour P, Lagueny A, Brechenmacher C, Vital C. Charcot-Marie-Tooth disease type 1A: clinicopathological correlations in 24 patients. J Peripher Nerv Syst. 2005 Mar;10(1):85-92. doi: 10.1111/j.1085-9489.2005.10112.x. PMID: 15703022.
5. Birouk N, Gouider R, Le Guern E, Gugenheim M, Tardieu S, Maisonobe T, Le Forestier N, Agid Y, Brice A, Bouche P. Charcot-Marie-Tooth disease type 1A with 17p11.2 duplication. Clinical and electrophysiological phenotype study and factors influencing disease severity in 119 cases. Brain. 1997 May;120 ( Pt 5):813-23. doi: 10.1093/brain/120.5.813. PMID: 9183252.
2. Holloway MP, DeNardo BD, Phornphutkul C, Nguyen K, Davis C, Jackson C, Richendrfer H, Creton R, Altura RA. An asymptomatic mutation complicating severe chemotherapy-induced peripheral neuropathy (CIPN): a case for personalised medicine and a zebrafish model of CIPN. NPJ Genom Med. 2016 Jun 8;1:16016. doi: 10.1038/npjgenmed.2016.16. PMID: 29263815; PMCID: PMC5685301.
3.Rajabally Y, Vital A, Ferrer X, Vital C, Julien J, Latour P, Vandenberghe A, Lagueny A. Chronic inflammatory demyelinating polyneuropathy caused by HIV infection in a patient with asymptomatic CMT 1A. J Peripher Nerv Syst. 2000 Sep;5(3):158-62. doi: 10.1046/j.1529-8027.2000.00014.x. PMID: 11442172.
4. Carvalho AA, Vital A, Ferrer X, Latour P, Lagueny A, Brechenmacher C, Vital C. Charcot-Marie-Tooth disease type 1A: clinicopathological correlations in 24 patients. J Peripher Nerv Syst. 2005 Mar;10(1):85-92. doi: 10.1111/j.1085-9489.2005.10112.x. PMID: 15703022.
5. Birouk N, Gouider R, Le Guern E, Gugenheim M, Tardieu S, Maisonobe T, Le Forestier N, Agid Y, Brice A, Bouche P. Charcot-Marie-Tooth disease type 1A with 17p11.2 duplication. Clinical and electrophysiological phenotype study and factors influencing disease severity in 119 cases. Brain. 1997 May;120 ( Pt 5):813-23. doi: 10.1093/brain/120.5.813. PMID: 9183252.
Deductive Syllogism:
A. Genes are assumed to be the cause of genetic and phenotypic variability in CMT1A
- GENES (G) CAUSE VARIABILITY IN CMT1A (V) -
- G --> V
B. This genetically confirmed patient with PMP22 duplication does not meet criteria for dysmyelination.
- PHENOTYPE (P) HAS ++VARIABILITY
- V --> P
C. Genes must be responsible for this patient's phenotype.
- GENES CAUSE THE PHENOTYPE
- G --> P
A. Genes are assumed to be the cause of genetic and phenotypic variability in CMT1A
- GENES (G) CAUSE VARIABILITY IN CMT1A (V) -
- G --> V
B. This genetically confirmed patient with PMP22 duplication does not meet criteria for dysmyelination.
- PHENOTYPE (P) HAS ++VARIABILITY
- V --> P
C. Genes must be responsible for this patient's phenotype.
- GENES CAUSE THE PHENOTYPE
- G --> P
Introduction:
Chronic inflammatory demyelinating polyradiculoneuropathies (CIDP) is a rare, acquired polyneuropathy, especially in children, affecting the peripheral nervous system. It most commonly presents in a symmetric, proximal and distal, sensorimotor fashion (1). Immunosuppression and immunomanipulation are treatment modalities.
We present a case of a 14 year old male with severe progressive CIDP who became refractory to steroid and IVIg but responded to Rituximab.
Case presentation (Method and Result):
A 14-year-old male with a history of asymmetric quadriparesis upper worse than lower was diagnosed with CIDP. He had an initial partial response to IVIG and prednisone but then rapidly became refractory with progressive weakness and not even response to weekly IVIG and prednisone. Rituximab, and methotrexate were therefore started, the methotrexate was changed to Cellcept after 8 weeks. Within 12 weeks of starting Rituximab, his strength improved from quadriplegia to walker-assisted gait. By 22 weeks he achieved independent ambulation. His JAMAR hand grip increased from 0 to 30 kg. His worst recordable median conduction velocity (CV) improved from a nadir (MRC 0/5) of 14% of normal to 52% at full recovery (MRC 5/5).
Discussion:
Pediatric CIDP is rare and refractory cases even more so. There are limited published studies. The optimal treatment for pediatric CIDP is not well established. Currently the treatment is borrowed from the management of adult CIDP, which include corticosteroids, IVIG and plasmapheresis as first-line (2). There is no consensus treatment evidence if the first line options failed. A study conducted over 13 years enrolled ten patients who were refractory to IVIG and steroids, four responded to PLEx. Six children did not respond to the first-line treatment and additional immunosuppressants, of these, four received cyclosporine and achieved successful disease control, while two were given a combination of steroids and azathioprine; one achieved complete remission and the other, partial remission (3). One case report supports the use of rituximab in pediatric refractory CIDP, while another found no definitive benefit (4) (5).
Our case showed significant improvement from quadroparesis to be independent with normal neurological exam, in our estimation is the rituximab which played the major part of the improvement.
Conclusion:
This case highlights several important clinical points.
Chronic inflammatory demyelinating polyradiculoneuropathies (CIDP) is a rare, acquired polyneuropathy, especially in children, affecting the peripheral nervous system. It most commonly presents in a symmetric, proximal and distal, sensorimotor fashion (1). Immunosuppression and immunomanipulation are treatment modalities.
We present a case of a 14 year old male with severe progressive CIDP who became refractory to steroid and IVIg but responded to Rituximab.
Case presentation (Method and Result):
A 14-year-old male with a history of asymmetric quadriparesis upper worse than lower was diagnosed with CIDP. He had an initial partial response to IVIG and prednisone but then rapidly became refractory with progressive weakness and not even response to weekly IVIG and prednisone. Rituximab, and methotrexate were therefore started, the methotrexate was changed to Cellcept after 8 weeks. Within 12 weeks of starting Rituximab, his strength improved from quadriplegia to walker-assisted gait. By 22 weeks he achieved independent ambulation. His JAMAR hand grip increased from 0 to 30 kg. His worst recordable median conduction velocity (CV) improved from a nadir (MRC 0/5) of 14% of normal to 52% at full recovery (MRC 5/5).
Discussion:
Pediatric CIDP is rare and refractory cases even more so. There are limited published studies. The optimal treatment for pediatric CIDP is not well established. Currently the treatment is borrowed from the management of adult CIDP, which include corticosteroids, IVIG and plasmapheresis as first-line (2). There is no consensus treatment evidence if the first line options failed. A study conducted over 13 years enrolled ten patients who were refractory to IVIG and steroids, four responded to PLEx. Six children did not respond to the first-line treatment and additional immunosuppressants, of these, four received cyclosporine and achieved successful disease control, while two were given a combination of steroids and azathioprine; one achieved complete remission and the other, partial remission (3). One case report supports the use of rituximab in pediatric refractory CIDP, while another found no definitive benefit (4) (5).
Our case showed significant improvement from quadroparesis to be independent with normal neurological exam, in our estimation is the rituximab which played the major part of the improvement.
Conclusion:
This case highlights several important clinical points.
- Dramatic improvement is possible in cases of quadriplegic CIDP.
- Strength recovery is not linearly related to m/sCV recovery.
- Therapeutic principle of proportionality: aggressive disease requires aggressive therapy/polytherapy.
- Rituximab, by temporal analysis, appears to be responsible for the balance of the response.
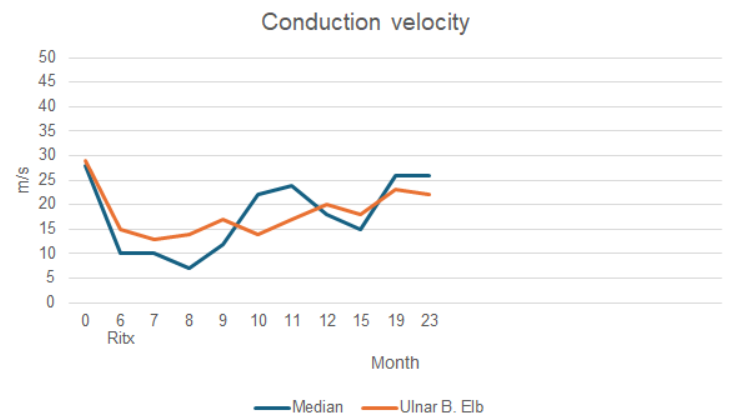
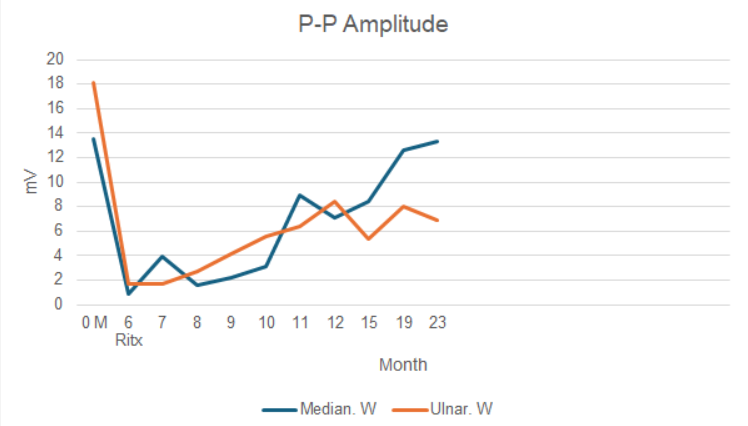
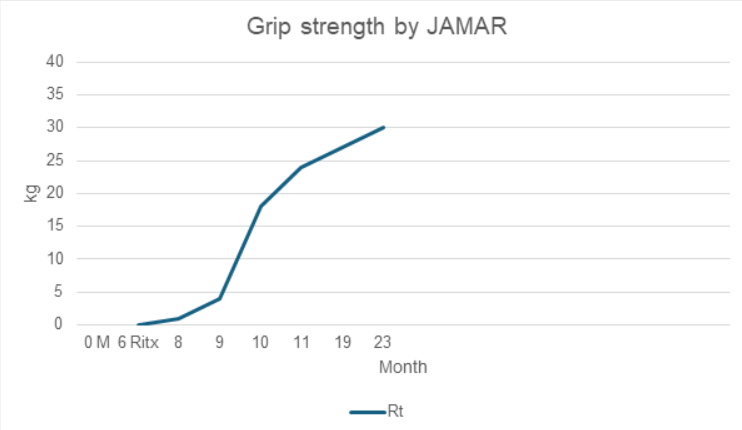
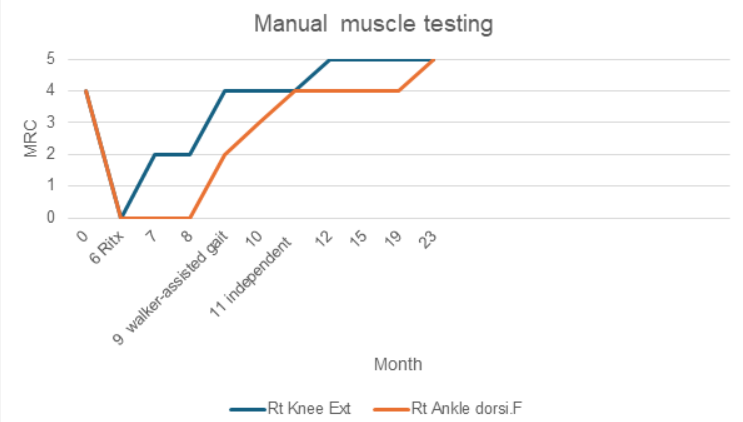
References
- Gogia B, Rocha Cabrero F, Khan Suheb MZ, et al. Chronic Inflammatory Demyelinating Polyradiculoneuropathy. [Updated 2023 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563249/
- Łukawska M, Potulska-Chromik A, Lipowska M, Hoffman-Zacharska D, Olchowik B, Figlerowicz M, Kanabus K, Rosiak E, Kostera-Pruszczyk A. Pediatric CIDP: Diagnosis and Management. A Single-Center Experience. Front Neurol. 2021 Jul 2;12:667378. doi: 10.3389/fneur.2021.667378. Erratum in: Front Neurol. 2022 Jan 21;12:784144. PMID: 34276534; PMCID: PMC8284159.
- Kim W, Shim YK, Choi SA, Kim SY, Kim H, Lim BC, Hwang H, Choi J, Kim KJ, Chae JH. Chronic inflammatory demyelinating polyneuropathy: Plasmapheresis or cyclosporine can be good treatment options in refractory cases. Neuromuscul Disord. 2019 Sep;29(9):684-692. doi: 10.1016/j.nmd.2019.06.010. Epub 2019 Jun 19. PMID: 31473049.
- D'Amico A, Catteruccia M, De Benedetti F, Vivarelli M, Colucci M, Cascioli S, Bertini E. Rituximab in a childhood-onset idiopathic refractory chronic inflammatory demyelinating polyneuropathy. Eur J Paediatr Neurol. 2012 May;16(3):301-3. doi: 10.1016/j.ejpn.2011.08.002. Epub 2011 Sep 7. PMID: 21903431.
- Desai J, Ramos-Platt L, Mitchell WG. Treatment of pediatric chronic inflammatory demyelinating polyneuropathy: Challenges, controversies and questions. Ann Indian Acad Neurol. 2015 Jul-Sep;18(3):327-30. doi: 10.4103/0972-2327.160065. PMID: 26425012; PMCID: PMC4564469.

BACKGROUND
Late onset Pompe disease (LOPD), rare autosomal recessive lysosomal storage disease, resulting from mutation in alpha glucosidase enzyme (GAA) can present even in 6th decade of life[1] Slowly progressive limb girdle pattern of weakness (LGPW), with auxiliary features such as ptosis, enlarged tongue, axial rigidity, facial diplegia, variable degree of respiratory weakness is not uncommon[2]. Hypertrophic and electrical cardiac abnormalities are well described in LOPD. [3]
Enzymatic replacement therapy (ERT) has been shown to be beneficail even in advanced cases. Early initiation of ERT after diagnosis is reccomended.
Here we present a case of LOPD presenting with proximal shoudler and hip girdle weakness as well as diastolic dysfunction and a restrictive left ventricular fillling pattern.
Late onset Pompe disease (LOPD), rare autosomal recessive lysosomal storage disease, resulting from mutation in alpha glucosidase enzyme (GAA) can present even in 6th decade of life[1] Slowly progressive limb girdle pattern of weakness (LGPW), with auxiliary features such as ptosis, enlarged tongue, axial rigidity, facial diplegia, variable degree of respiratory weakness is not uncommon[2]. Hypertrophic and electrical cardiac abnormalities are well described in LOPD. [3]
Enzymatic replacement therapy (ERT) has been shown to be beneficail even in advanced cases. Early initiation of ERT after diagnosis is reccomended.
Here we present a case of LOPD presenting with proximal shoudler and hip girdle weakness as well as diastolic dysfunction and a restrictive left ventricular fillling pattern.
[1] Hagemans ML, Winkel LP, Hop WC, Reuser AJ, Van Doorn PA,
Van der Ploeg AT. Disease severity in children and adults with Pompe disease related to age and disease duration. Neurology.
2005;64(12):2139-41
Van der Ploeg AT. Disease severity in children and adults with Pompe disease related to age and disease duration. Neurology.
2005;64(12):2139-41
[2] Tarnopolsky M, Katzberg H, Petrof BJ, Sirrs S, Sarnat HB, Myers K, Dupré N, Dodig D, Genge A, Venance SL, Korngut L, Raiman J, Khan A. Pompe Disease: Diagnosis and Management. Evidence-Based Guidelines from a Canadian Expert Panel. Can J Neurol Sci. 2016 Jul;43(4):472-85. doi: 10.1017/cjn.2016.37. Epub 2016 Apr 8. PMID: 27055517.
[3] Schüller A, Wenninger S, Strigl-Pill N, Schoser B. Toward deconstructing the phenotype of late-onset Pompe disease. Am J Med Genet C Semin Med Genet. 2012 Feb 15;160C(1):80-8. doi: 10.1002/ajmg.c.31322. Epub 2012 Jan 17. PMID: 22253010.
CASE PRESENTATION
We present a case of 67-year-old male presenting to EMG lab with lumbosacral radicular symptoms, parasthesias in feet. History of reduced ejection fraction (EF) with cardiomyopathy of undetermined etiology, developed in his 50s. Regular follow up with cardiology. History of NSTEMI at 60. Fatigability with ambulation, stairs, at times with sit to stand transfers for years prioir to presentation (exact timeline unclear). At times unstead during recreational walks. No falls history. No history of dysphagia, ptosis, constitutional symptoms. Developmental history not contributory.
ALLERGIES:
None
MEDICATION HISTORY:
Vitamin D 1000 units daily
Pantoprazole 40 mg daily
Atorvastatin 40 mg daily
Candesartan 16 mg daily
PAST MEDICAL HISTORY:
Hypertension
Increase cholesterol
History of cardiac surgery–coronary artery bypass , NSTEMI
SOCIAL HISTORY:
Non-smoker. Consumes approximately 6 alcoholic beverages per week. Rretired, he used to work in construction as well as as a driver.
FAMILY HISTORY
Adopted. No children
We present a case of 67-year-old male presenting to EMG lab with lumbosacral radicular symptoms, parasthesias in feet. History of reduced ejection fraction (EF) with cardiomyopathy of undetermined etiology, developed in his 50s. Regular follow up with cardiology. History of NSTEMI at 60. Fatigability with ambulation, stairs, at times with sit to stand transfers for years prioir to presentation (exact timeline unclear). At times unstead during recreational walks. No falls history. No history of dysphagia, ptosis, constitutional symptoms. Developmental history not contributory.
ALLERGIES:
None
MEDICATION HISTORY:
Vitamin D 1000 units daily
Pantoprazole 40 mg daily
Atorvastatin 40 mg daily
Candesartan 16 mg daily
PAST MEDICAL HISTORY:
Hypertension
Increase cholesterol
History of cardiac surgery–coronary artery bypass , NSTEMI
SOCIAL HISTORY:
Non-smoker. Consumes approximately 6 alcoholic beverages per week. Rretired, he used to work in construction as well as as a driver.
FAMILY HISTORY
Adopted. No children
PHYSICAL EXAMINATION:
MOTOR EXAM:
Head flexion and extension were 5/5. Bilateral: shoulder shrug : 5/5, shoulder AB duction 4/5, shoulder external rotation : -4/5 ,elbow flexion : 4/5 , elbow extension, wrist flexion and extension as well as grip strength all 5/5.Lower limbs:-4/5 hip flexion on the right side and 4/5 on the left. Hip extension was 4/5 bilaterally. Hip AB duction, AB duction,knee flexion and extension all : 5/5. Dorsiflexion and plantar flexion:5/5.
Atrophy :deltoids,arms, quads.
Gait : Hyperlordotic
CNS 2-12: mild L ptosis, no dysarthia, no macroglosia,no facial weakness
MOTOR EXAM:
Head flexion and extension were 5/5. Bilateral: shoulder shrug : 5/5, shoulder AB duction 4/5, shoulder external rotation : -4/5 ,elbow flexion : 4/5 , elbow extension, wrist flexion and extension as well as grip strength all 5/5.Lower limbs:-4/5 hip flexion on the right side and 4/5 on the left. Hip extension was 4/5 bilaterally. Hip AB duction, AB duction,knee flexion and extension all : 5/5. Dorsiflexion and plantar flexion:5/5.
Atrophy :deltoids,arms, quads.
Gait : Hyperlordotic
CNS 2-12: mild L ptosis, no dysarthia, no macroglosia,no facial weakness
RESULTS
EMG: L5 radiculopathy, with unexpected myopathic units in hip/pelvic/ shoulder girdle muscles with active denervation and muscle irritability. CK, CRP, SPEP, ANA, LFTs, HMG-CoA reductase,Myositis Ab panel: normal. GAA enzymatic activity=0.96µmol/L/hr (low), genetics: pathogenic variants in GAA gene: c.-32-13T>G and c.1194+3G>C (reclassified from VUS during diagnostic workup). ECHO: severe diastolic dysfunction, restrictive left ventricular filling,dilated LV, EF : 35-40%. PFTs: normal.
EMG: L5 radiculopathy, with unexpected myopathic units in hip/pelvic/ shoulder girdle muscles with active denervation and muscle irritability. CK, CRP, SPEP, ANA, LFTs, HMG-CoA reductase,Myositis Ab panel: normal. GAA enzymatic activity=0.96µmol/L/hr (low), genetics: pathogenic variants in GAA gene: c.-32-13T>G and c.1194+3G>C (reclassified from VUS during diagnostic workup). ECHO: severe diastolic dysfunction, restrictive left ventricular filling,dilated LV, EF : 35-40%. PFTs: normal.
Sequence Analysis and Deletion/Duplication Testing
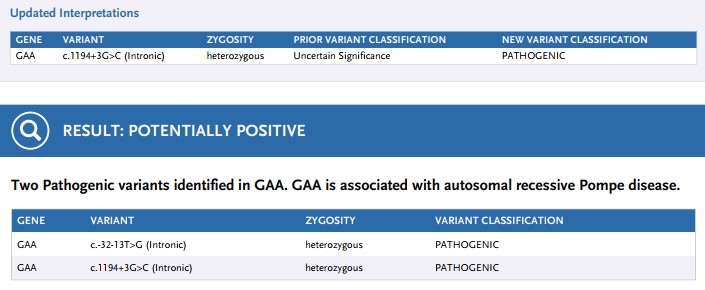
GAA, Intron 1, c.-32-13T>G (Intronic), heterozygous, PATHOGENIC
- Well documented variant
- Loss of the initiator methionine
- Does not directly change the encoded amino acid sequence of the GAA protein.
-
Affects a nucleotide within the consensus splice site, aberrant splicing
EMG
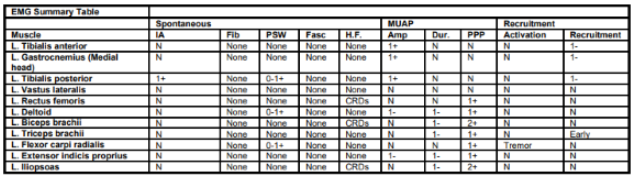
CONCLUSION
The patient was diagnosed with LOPD and started on a-Glucosidase replacement therapy ( 20mg/kg). Six months into therapy, improvment in proximal shoudler/hip girdle was achived. Improvement in EF followed on routine cardiac monitoring. Patient did not present nor develop pulmonary compromise. Muscle biopsy was not pursued in view of genetic and enzymatic testing results.
LOPD remains a differential for LGPW especially in older patient population with cardiopulmonary features. Nevertheless, it remains a diagnostic challange due to its phenotypical variability.
Combinations of skeletal muscle involvement with variable degrees of cardiopulmonary compromise are not uncommon. Isolated respiratory failure cases have also been reported. The slowly progressive muslce weakness may also mimic a scapuloperoneal pattern of involvement, further clouding the diagnostic process. CK levles may remain normal to mildly elevated in LOPD. Age-appropriate adjunct comorbidities may confound the extraskeletal findings in LOPD.
In summary, including LOPD in the differential of LGPW presentation.GAA enzymatic activity followed by genetic testing remains readily available, can confirm diagnosis, preventing delay of approved therapy in LOPD that allows for preventing organ damage and signifficant diasbility.
The patient was diagnosed with LOPD and started on a-Glucosidase replacement therapy ( 20mg/kg). Six months into therapy, improvment in proximal shoudler/hip girdle was achived. Improvement in EF followed on routine cardiac monitoring. Patient did not present nor develop pulmonary compromise. Muscle biopsy was not pursued in view of genetic and enzymatic testing results.
LOPD remains a differential for LGPW especially in older patient population with cardiopulmonary features. Nevertheless, it remains a diagnostic challange due to its phenotypical variability.
Combinations of skeletal muscle involvement with variable degrees of cardiopulmonary compromise are not uncommon. Isolated respiratory failure cases have also been reported. The slowly progressive muslce weakness may also mimic a scapuloperoneal pattern of involvement, further clouding the diagnostic process. CK levles may remain normal to mildly elevated in LOPD. Age-appropriate adjunct comorbidities may confound the extraskeletal findings in LOPD.
In summary, including LOPD in the differential of LGPW presentation.GAA enzymatic activity followed by genetic testing remains readily available, can confirm diagnosis, preventing delay of approved therapy in LOPD that allows for preventing organ damage and signifficant diasbility.
Understanding Treatment Barriers and Adherence Among People Living with Amyotrophic Lateral Sclerosis
Background
§Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disease with only three approved treatments in North America: Riluzole, edaravone, tofersen.
§Please note, in March 2024, the results of the PHOENIX Phase 3 trial were released showing that sodium phenylbutyrate (PB) and taurursodiol/ursodoxicoltaurine (TURSO) failed to meet its primary endpoint in ALS. Thus, PB and TURSO is being removed from the market.
§Poor treatment adherence reduces clinical effectiveness which can adversely impact disease progression and mortality rates (Introna et al., 2018).
§Understanding barriers and adherence to treatment in real world clinical practice is essential to address these issues.
§The objective of the current study was to perform a scoping review to identify knowledge gaps on the incidence of non-adherence and barriers to ALS treatment in clinical practice using real world data (RWD).
Methods
§This scoping review was conducted in February 2024 before the results of the PHOENIX trial were released and as such, PB and TURSO was included in the search terms.
§The scoping review proposed the following two questions and search terms:
| Q1. To describe the incidence of non-adherence to ALS drugs in the real world |
| Example Search Terms |
| 1. Treatment and adherence and amyotrophic lateral sclerosis* |
| 2. Treatment and compliance and amyotrophic lateral sclerosis* |
| 3. Treatment and amyotrophic lateral sclerosis* |
| 4. Treatment and ALS and adherence and real-world data* |
| 5. Treatment and ALS and compliance and real-world data* |
| Q2. What are the known barriers associated with low adherence to ALS treatments in the real world? |
| Example Search Terms |
| 1. Barriers and treatment and adherence and amyotrophic lateral sclerosis* |
| 2. Barriers and treatment and compliance and amyotrophic lateral sclerosis* |
| 3. Barriers and treatment and amyotrophic lateral sclerosis* |
| 4. Treatment and ALS and barriers and real-world data* |
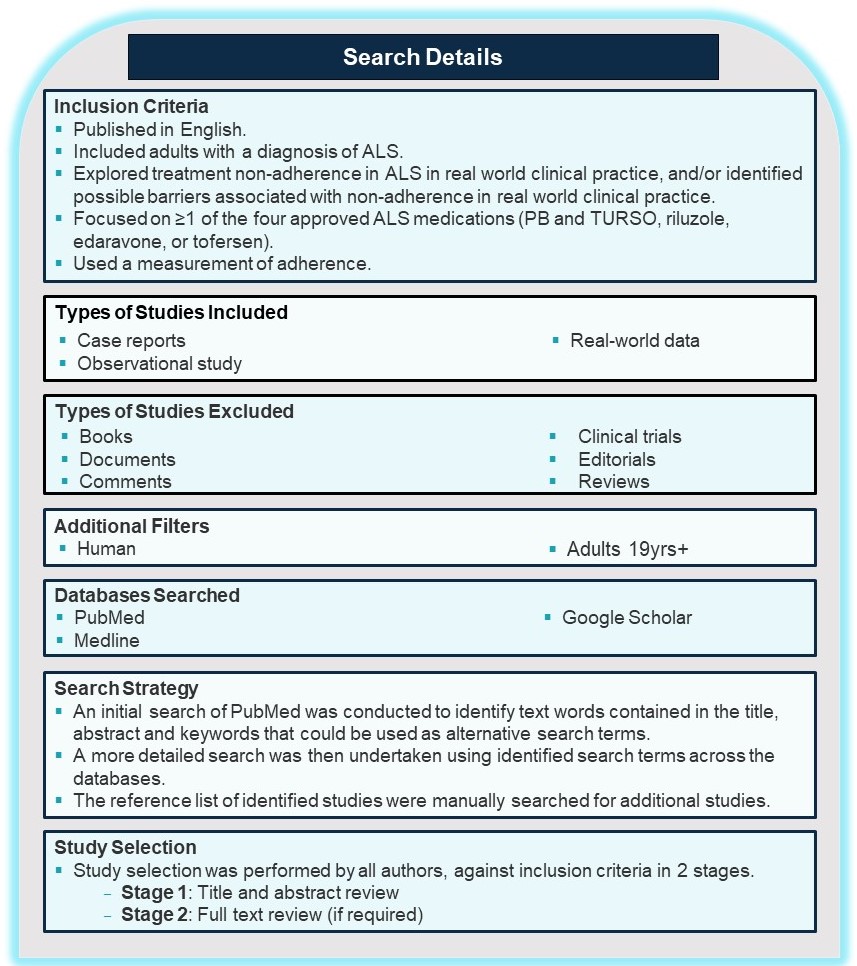
Results
§A total of 10 studies were retrieved that met the inclusion criteria for Q1 (Figure 1).
§5 studies were conducted in Italy, 3 in the USA, 1 in Portugal, and 1 in Japan.
§7 assessed riluzole and 3 assessed edaravone. No studies assessed PB and
TURSO or tofersen.
§No studies met the inclusion criteria for Q2 (Barriers as the primary outcome) (Figure 2).
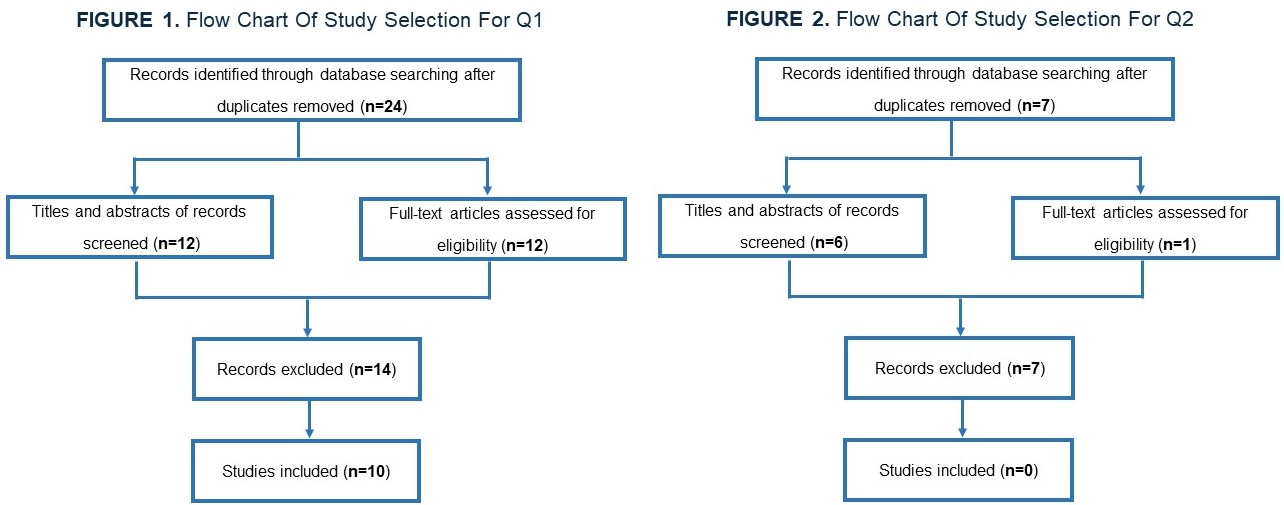
Discussion and Conclusion
§Available studies primarily focused on riluzole and estimates for non-adherence/non-persistence were highly variable, e.g., Chio et al., 2002 reported low levels of adherence at 4.2%; whilst Geronimo et al., 2022 and Gilbert et al., 2019 reported moderate levels of adherence at 17%-54% and 52%, respectively.
§Other studies reported very high discontinuation rates between 37%-59.9% (Okada et al., 2019; Vu et al., 2020).
§Persistence measurement is likely confounded by stage of disease and measurement differences making it challenging to interpret the magnitude of the problem with existing data.
§Similarly, reported barriers to adherence were highly variable – mostly focused on adverse health events that may or may not have been related to the ALS treatment.
§These findings demonstrate a clear need for further study to determine the extent to which negative patient outcomes could be delayed with improved drug use.
§Finally, there is a clear need for guidance to help standardize measurement approaches for non-adherence in the ALS population and identify direct causes.
Contact info: Genevieve Matte, MDCM, FRCP - Genevieve.matte.med@ssss.gouv.qc.ca
A 65 year-old male with subacute asymmetric, proximal more than distal upper extremity weakness with associated paresthesias and pain

CASE PRESENTATION
- ID: 65M RHD 6 week history of progressive upper extremity and neck weakness with associated paresthesias, burning pain, and headache; preceded by febrile illness with associated arthralgias 2 months prior
- PMHx: Asthma, psoriasis, osteoarthritis, and chronic dysphagia of unknown etiology
- Medications: Vitamin D
- Social Hx: Remote extensive smoking history, consumes approximately one alcoholic drink daily; visiting partner in Vancouver, Canada for the past month. Permanent address in Halifax, Nova Scotia and worked as a carpenter at outdoor summer festivals in Ontario
- FHx: ALS in his father and esophageal cancer in his mother and sister
-
O/E: head drop and asymmetric, proximal more than distal upper extremity weakness affecting L>R
- Strength testing (R/L): rhomboids 2/2, infraspinatus 2/2, supraspinatus 2/1, deltoids 1/1, biceps 1/1, triceps 3/2, pronator teres 4-/3, extensor carpi radialis 4/4-, abductor pollicis brevis 4/4-, flexor pollicis longus 4/4, abductor digiti minimi 4/4-, and first dorsal interossei 4/4. Intact in the lower extremities.Reflexes were absent in the upper extremities, except for left triceps which was 1+. Reflexes in the lower extremities were preserved and symmetric, with no clonus and downgoing plantar responses
- Diminished bilateral sensation to pin-prick in the distribution of C8 -T1 and patchy areas of reduced sensation in dermatomes C5-C7
- Coordination, and gait were normal
INVESTIGATIONS
- Positive for Borrelia burgdorferi IgG and IgM antibodies
- Normal/negative autoimmune, hematologic, and metabolic work-up.
- CSF: lymphocytic pleocytosis (197 cells/µL, 98% lymphocytes; reference range 0-5 cells/μL), elevated protein (2.31g/L; reference range 0.15-0.45g/L), and normal glucose. Flow cytometry polyclonal pattern consistent with a reactive process. CSF to serum antibody index was consistent with intrathecal B. burgdorferi antibody production.
- EMG/NCS indicative of preganglionic localization and polyradiculopathy; evidence of active denervation at L C6-C7 paraspinals and possible increased insertional activity at L C5 paraspinal
MRI of the cervical spine and brachial plexus.
MRI of the brachial plexus without contrast. Coronal T-2 Dixon fat-suppressed image of the bilateral brachial plexus identified mild diffuse, smooth thickening and enhancement with T2 hyper-intensity noted along the nerve roots, trunks, divisions, and cords of the bilateral brachial plexus.
FDG-PET Scan
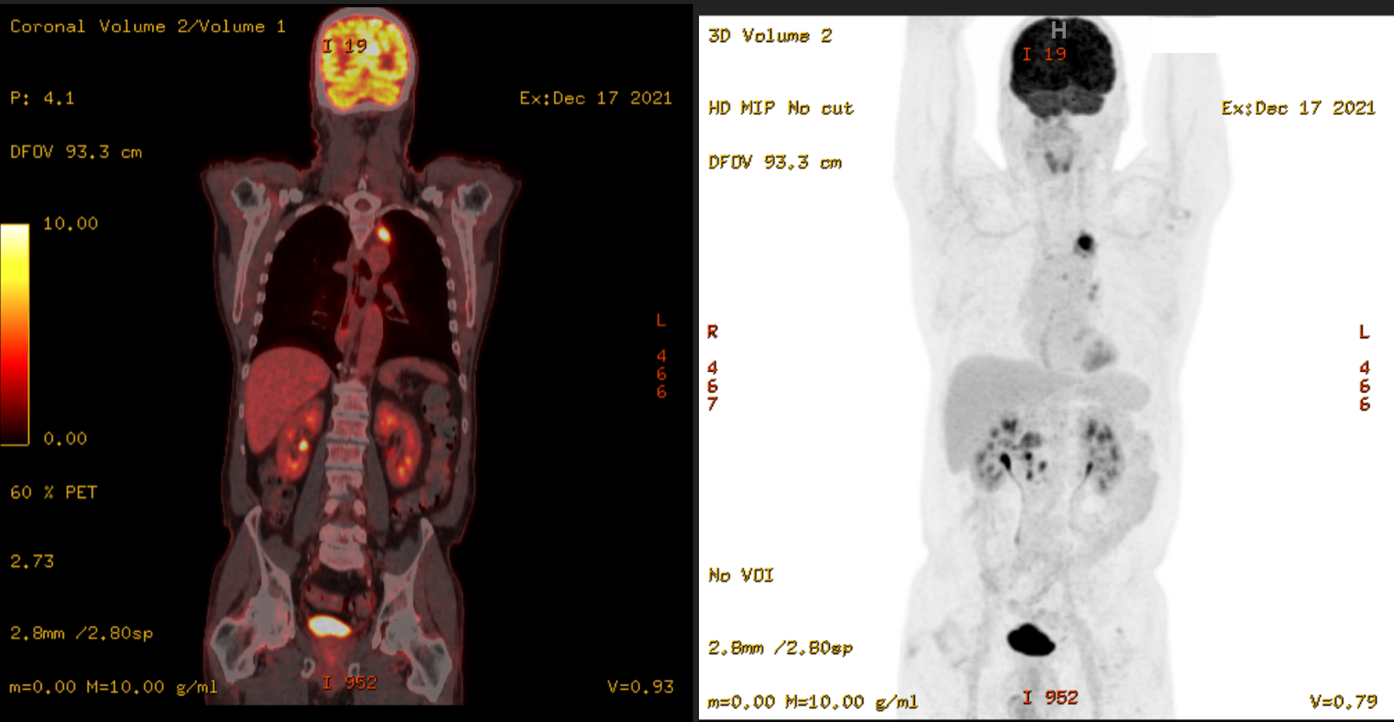
Positron emission tomography identified diffuse increased uptake in lymph nodes above and below the diaphragm. Reassuringly, there was no increased uptake in the affected nerve roots.
Computed tomography of the chest, abdomen, and pelvis.
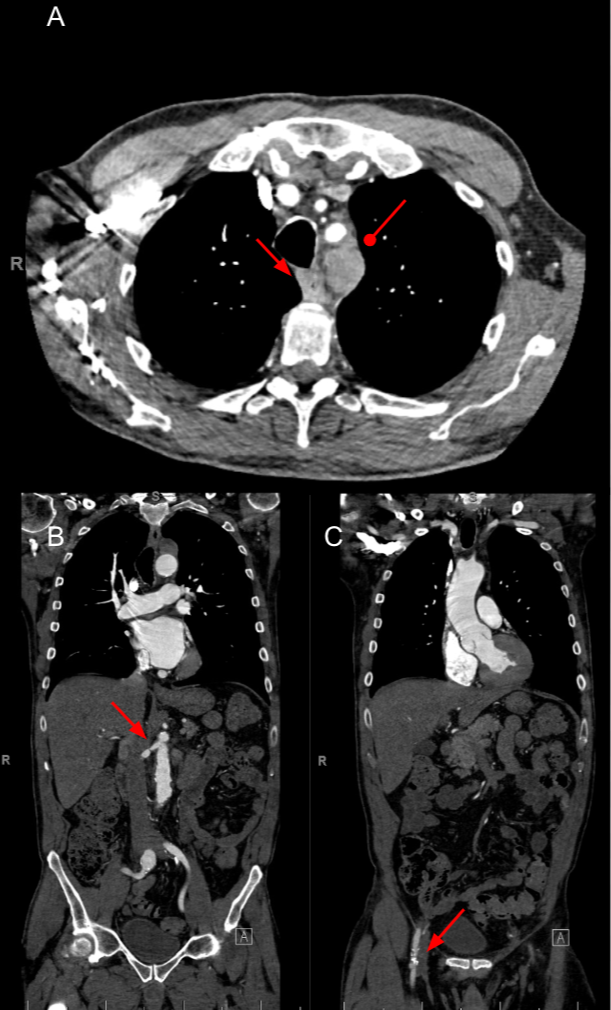
CT angiogram of the chest (A, B, C), abdomen and pelvis (B,C) identifying a number of unexpected findings highlighted by arrowheads. A. Esophageal thickening (arrowhead) and a necrotic superior mediastinal lymph node (round arrowhead) were noted on CTA of the chest. B. An intimal flap was noted in the right renal artery with suspected surrounding hematoma. C. An aneurysm in the right common iliac artery. Gastroenterology, respirology, and vascular surgery were consulted. EGD was consistent with achalasia. Vascular surgery suspected that the intimal flap and aneurysm were a byproduct of uncontrolled hypertension. Respirology performed a fine needle biopsy that was non-diagnostic for malignancy versus a duplication cyst.
MANAGEMENT
- Initially started on oral doxycycline; following resulted CSF findings, transitioned to ceftriaxone for 2 weeks followed by oral doxycycline for an additional 2 weeks.
- Exhibited gradual improvement in strength and repeat NCS/EMG completed one month post-treatment remained consistent with a polyradiculopathy, showing mixed denervation to left infraspinatus (C5/6) and biceps (C5/6) and active denervation of left paravertebral C5 muscles. Normalization of left triceps (C7) and paravertebral C7 muscles on EMG.
- Hypertension and presumed related aneurysms were managed medically under guidance of vascular surgery
DISCUSSION
Neuroborreliosis affects approximately 10-15% of people with untreated Lyme disease and typically declares itself 2-18 weeks after infection(1). How the spirochete crosses the blood brain barrier is unknown. Immunohistochemistry has identified direct spirochetal infiltration of the leptomeninges, nerve roots, and dorsal root ganglia with preservation of the CNS parenchyma(2). Damage to nervous tissue is secondary to inflammation(3).
North American neuroborreliosis often manifests with cranial nerve palsy, meningitis, and/or radiculoneuritis. Cranial neuropathy affects approximately half of patients(4). Facial nerve involvement is the most common and up to a quarter will have bilateral involvement(6).
Meningitis is lymphocytic and characterized by severe headache, not typically associated with meningismus or fever(4). Radiculoneuritis is seen in a third of patients and often accompanied by cranial nerve palsy(4). Intraparenchymal involvement of the brain or spinal cord is rare and seen more commonly with European neuroborreliosis(5).
Without treatment, symptom resolution typically occurs over months. However, patients are at risk of developing late Lyme disease characterized by chronic meningitis, progressive encephalitis, myelitis, and/or encephalomyelitis(5). Both early and late neuroborreliosis can be effectively managed with a 2-3 week course of doxycycline, ceftriaxone, cefotaxime, or penicillin G(4).
There are case reports identifying a possible link between B. burgdorferi and vascular aneurysms, similar to what is seen with Treponema pallidum(6). Lymphadenopathy is also a well-established hallmark of infection with B. burgdorferi. The relationship between Lyme disease and lymphoma is less clear. There is a link between cutaneous B-cell lymphoma and acrodermatitis chronica atrophicans, which is a manifestation of late European neuroborreliosis(7). An increased risk of mantle cell lymphoma has also been identified in patients with Lyme disease(8).
The case that we have described provides an excellent example of North American neuroborreliosis, and also highlights some of the rare manifestations of systemic Lyme disease.
Pharmacological prophylaxis for chronic migraine: A systematic review and network meta-analysis of randomized controlled trials

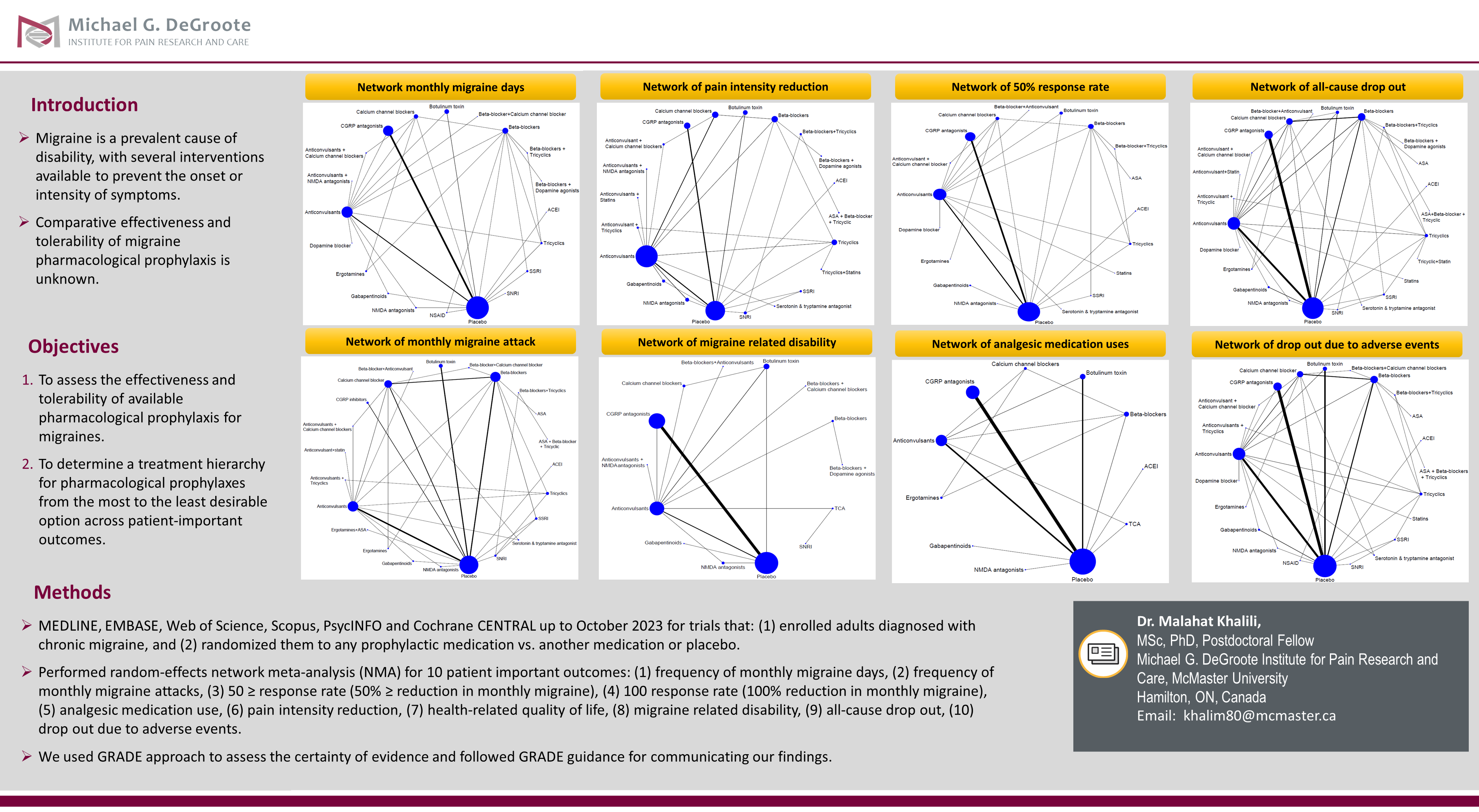
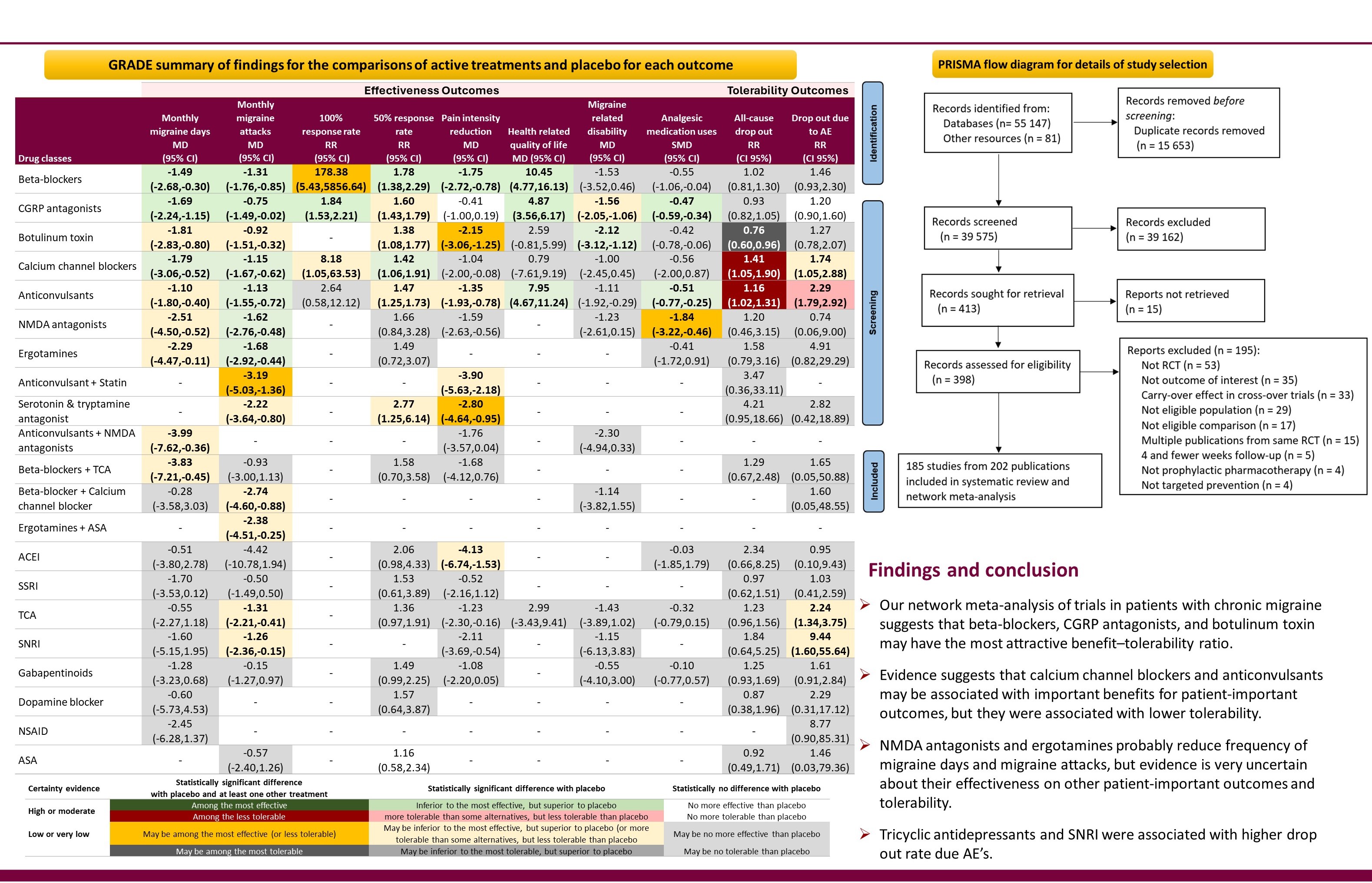
Malignant transformation of a spinal dermoid cyst into carcinosarcoma
Introduction
- Spinal dermoid cysts are benign, congenital lesions of ectodermal origin, often associated with spinal dysraphism. They can be asymptomatic or present with profound neurologic sequelae relating to mass effect or rupture.
- Malignant transformation of a spinal dermoid cyst is an exceptionally rare phenomenon, with transformation into carcinosarcoma not previously reported.
Case presentation
A 41-year-old male presented with 5 months of progressive leg weakness and back pain.
- He had a remote history of a L2-S1 laminectomy at age 15 for a congenital dermal sinus tract (Figure 1a,b) with a residual intradual, extramedullary cystic lesion at L1. The lesion remained stable on serial imaging for the next 26 years.
- MRI at presentation showed new enlargement and enhancement of the previously stable lesion and arachnoid adhesions of the cauda equina (Figure 3a)
- The patient underwent a T12-L1 laminectomy and resection of the intradural lesion. Intraoperative appearance of cystic contents and subsequent pathology were consistent with a dermoid cyst (Figure1c).
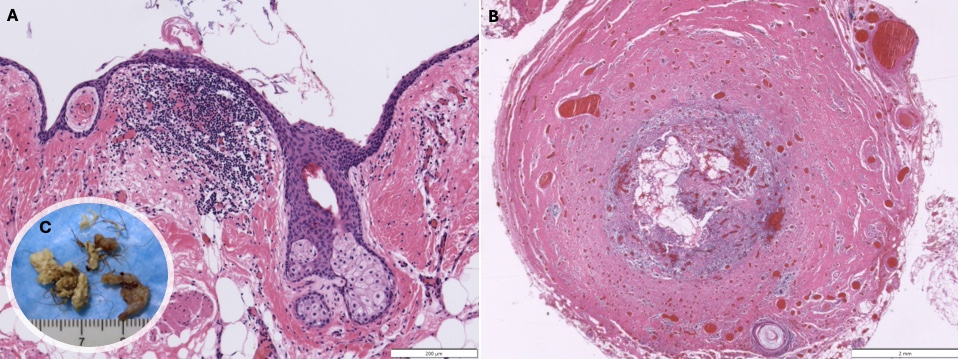
Post-operative course
- CSF: Protein 1.51, Glucose 4, TNCC 6; cultures (bacterial, fungal, TB), crypto antigen, viral PCRs, TB PCR, flow cytometry and cytology (repeated x 3) negative
- CT Chest/abdo/pelvis: calcified granulomas in lungs and adrenal gland
- BAL: negative cultures. Immunology and Infectious serology: negative
- The patient re-presented 2 weeks post-op with diplopia and headache due to acute hydrocephalus, thought to be due to chemical meningitis from ruptured cyst contents (Figure 2a).
-
Despite ventriculoperitoneal shunt implantation, dexamethasone, and supportive care, the patient declined over the next 2 months with progressive, widespread disease (Figure 3)
-> multiple cranial neuropathies, flaccid quadraplegia and neuromuscular respiratory failure
->florid arachnoiditis of the cauda equina, diffuse leptomeningeal enhancement of the brain and spine, and new intramedullary lesions
- CSF: Protein 1.51, Glucose 4, TNCC 6; cultures (bacterial, fungal, TB), crypto antigen, viral PCRs, TB PCR, flow cytometry and cytology (repeated x 3) negative
- CT Chest/abdo/pelvis: calcified granulomas in lungs and adrenal gland
- BAL: negative cultures. Immunology and Infectious serology: negative
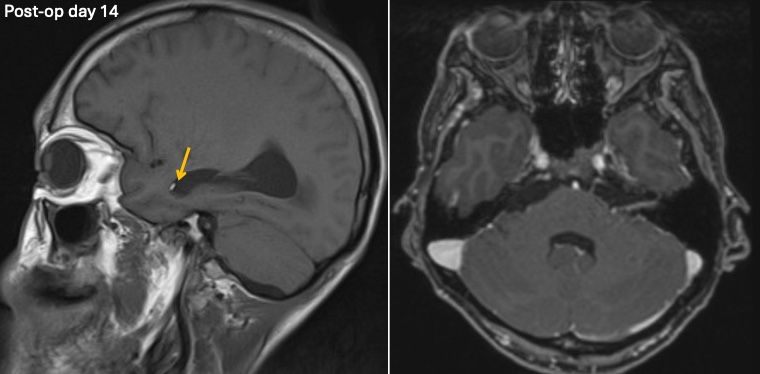
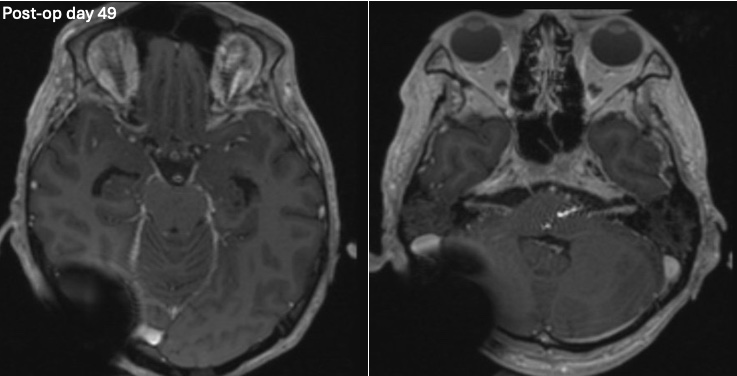

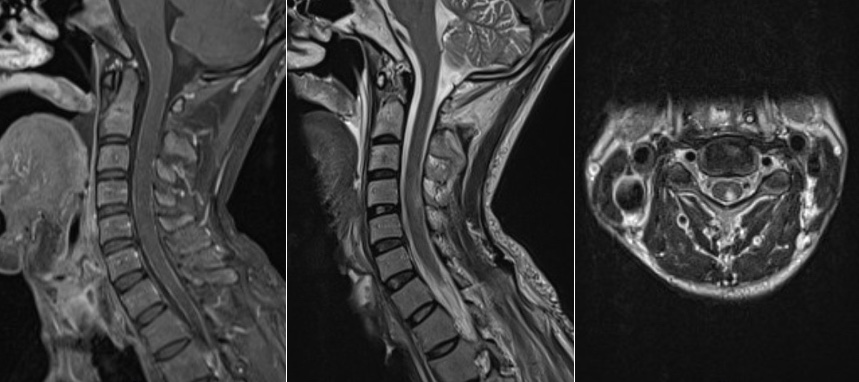

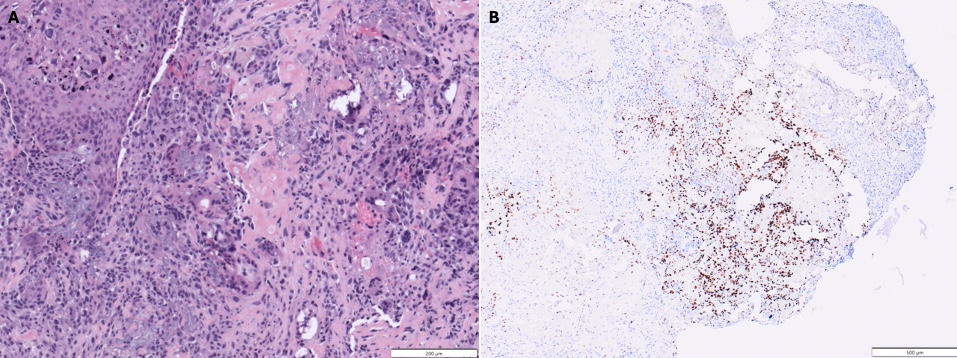
- A repeat spinal leptomeningeal biopsy (Figure 4) revealed presence of both carcinomatous and sarcomatous components, consistent with a diagnosis of invasive carcinosarcoma (Figure 5). The initial lesion was reexamined and sent for molecular testing; SATB2 immunoreactivity was supportive of (but not specific for) osteoblastic lineage in the immature cells (Figure 5b). Targeted next-generation sequencing (NGS) showed a TP53 point mutation (R273C).
- There were no curative treatment options. The patient was palliated and died 85 days after admission. Autopsy was not perormed.
Discussion
- To the authors knowledge, this is the first report of malignant transformation of a spinal dermoid cyst into carcinosarcoma
- The incidence of and risk factors for malignant degeneration of spinal dermoid cysts are unknown due to its rarity; in ovarian dermoid cysts, malignant degeneration occurs in <2% of dermoids, with risk factors that include rapid growth and adherence to adjacent structures.
- Red flags for a diagnosis of malignancy in this case include the rapid growth of the lesion after 26 years of stability, and progressive clinical course out of keeping with the self-limiting natural history of chemical meningitis. Extrapolating from the ovarian dermoid literature, the severity of the arachnoid adhesions could also be considered a red-flag.
- Repeat biopsy and re-examination of previous samples with molecular testing ultimately confirmed the diagnosis. In this case, there were no viable treatment options by that point.
Conclusion
- In patients with benign spinal dermoid cysts, malignant transformation should be considered in the differential diagnosis when there is rapidly progressive radiologic and clinical decline
- False negatives can occur with tumour pathology. Repeat sampling and/or re-examination of previous samples should be considered early if there is a high index of suspicion of an alternative diagnosis.
Development of a Streamlined Multi-Disciplinary Care Pathway for Compression Neuropathies: Reducing Wait Times and Complexity

Background
Care for compression neuropathies such as carpal tunnel syndrome (CTS) and ulnar neuropathy is often fragmented, uncoordinated, and slow. Patients may go through multiple steps (e.g., neurology consultation, nerve testing, ultrasound, surgical opinion, surgery) with a wait in between each step.
We used a Value-Based Health Care (VBHC) model to create a multidisciplinary clinic (family practice, neurology, physiatry, research, and plastic surgery) to create a novel care pathway.
Objectives
1. Develop a streamlined multi-disciplinary care pathway for CTS and ulnar neuropathy
2. Choose and implement patient reported outcomes measures
3. Pilot implementation of the care pathway
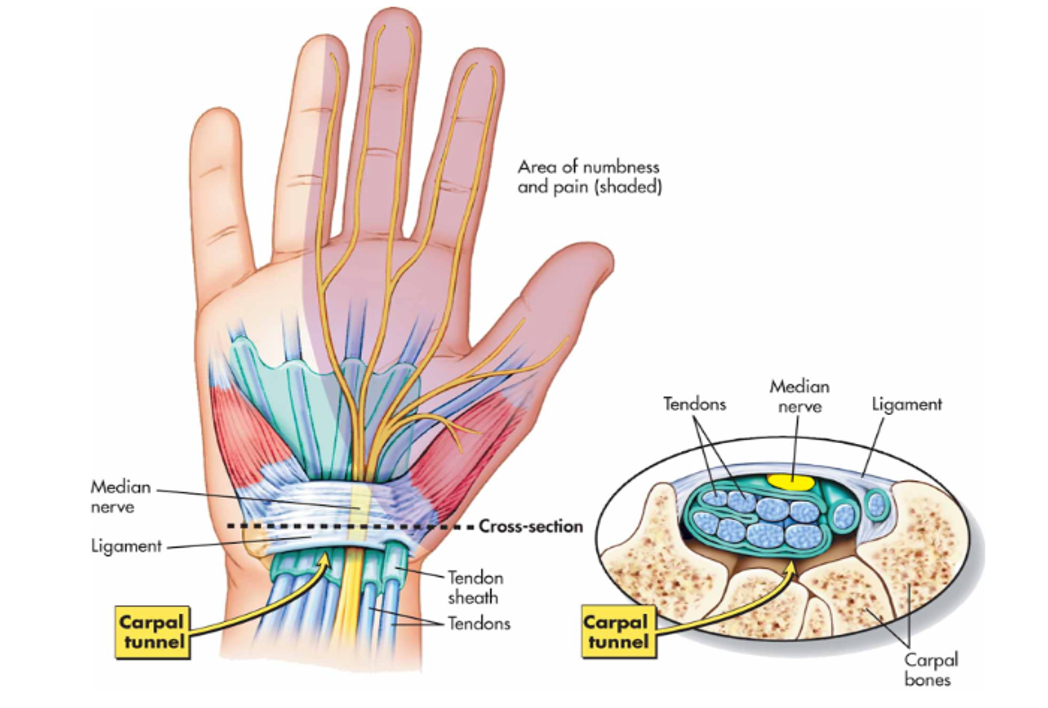
Figure 1. Anatomy of Carpal Tunnel
Methods
1. A working group with representation from specialists, family physicians, patient advocate, clerks, EMG technology, research, and administration was established, with support from Doctors of BC/Shared Care Project Manager.
2. Activities included process mapping, patient journey mapping, Pathways referral, website and resource development, and evaluation
3. Outcome measures were evaluated
4. Pilot Phase: Patient Reported Outcome Measures (PROMs) were collected prospectively from 66 patients in January to February 2024. Patients entered the clinical pathway for Mild CTS, Moderate CTS, Severe CTS, and Ulnar Neuropathy
2. Activities included process mapping, patient journey mapping, Pathways referral, website and resource development, and evaluation
3. Outcome measures were evaluated
4. Pilot Phase: Patient Reported Outcome Measures (PROMs) were collected prospectively from 66 patients in January to February 2024. Patients entered the clinical pathway for Mild CTS, Moderate CTS, Severe CTS, and Ulnar Neuropathy
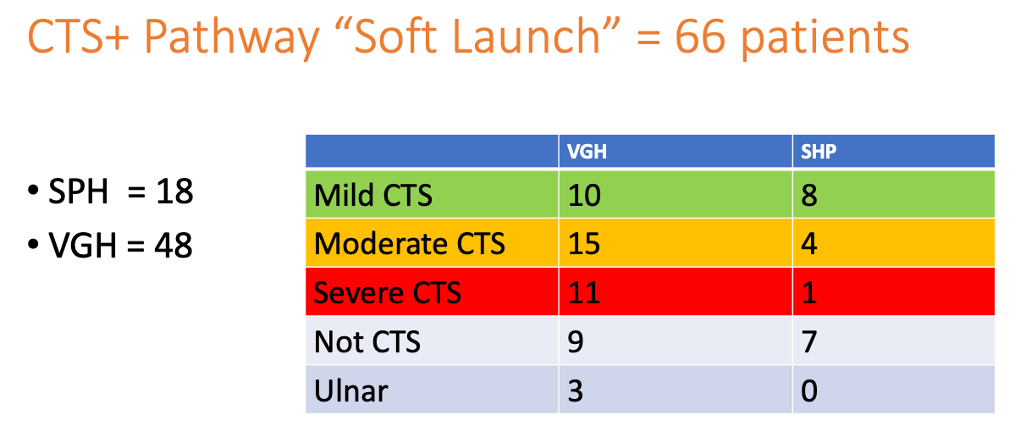
Table 1. Patient Category Distribution
Results
- 3- part Value Based Health Care workshop conducted with multi-disciplinary team, to build capacity for VBHC concepts and initiate IPU development
- Condition specific outcome measure developed including Boston CTS measure and a pain scale
- "One stop shopping" (ie. EMG and US guided injection on same visit), and expedited surgical assessment
- Education materials and website were developed to provide information to patients and referring physicians
- Streamlined referral process for the CTS+ Pathway established
Figure 2. Pathway Development
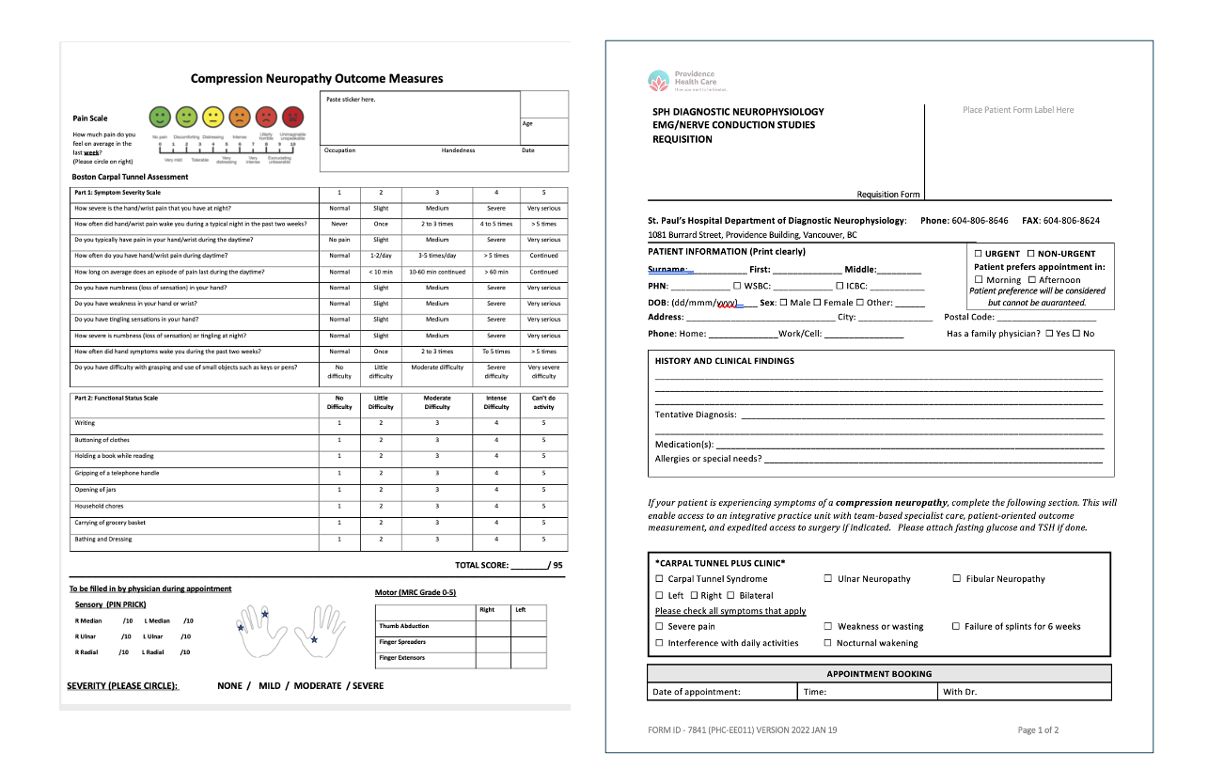
Figure 3. Outcome Measure Set and CTS+ Referral Form

Results
One stop shopping:
- Bloodwork
- Splints
- EMG, Ultrasound
- Resources/Website

Figure 4. Clinical Pathways Developed for Mild, Moderate, and Severe CTS
Conclusions
- A Value-Based Health Care framework supports the development of patient-centered, multidisciplinary care pathway
- By reducing the number of steps, following the patient through the full cycle of care for their compression neuropathy and expediting surgical assessment, we aim to improve patient experience and outcomes
- The pilot phase allows application of quality improvement techniques to streamline the patient journey and refine the outcome measure with a rapid PDSA cycle
- Evaluation of impact on wait times between steps in the pathway and patient experience is planned to validate the pathway
Using AI to revolutionize clinical training through OSCE-GPT: a focused exploration of user feedback on otolaryngology and neurology cases


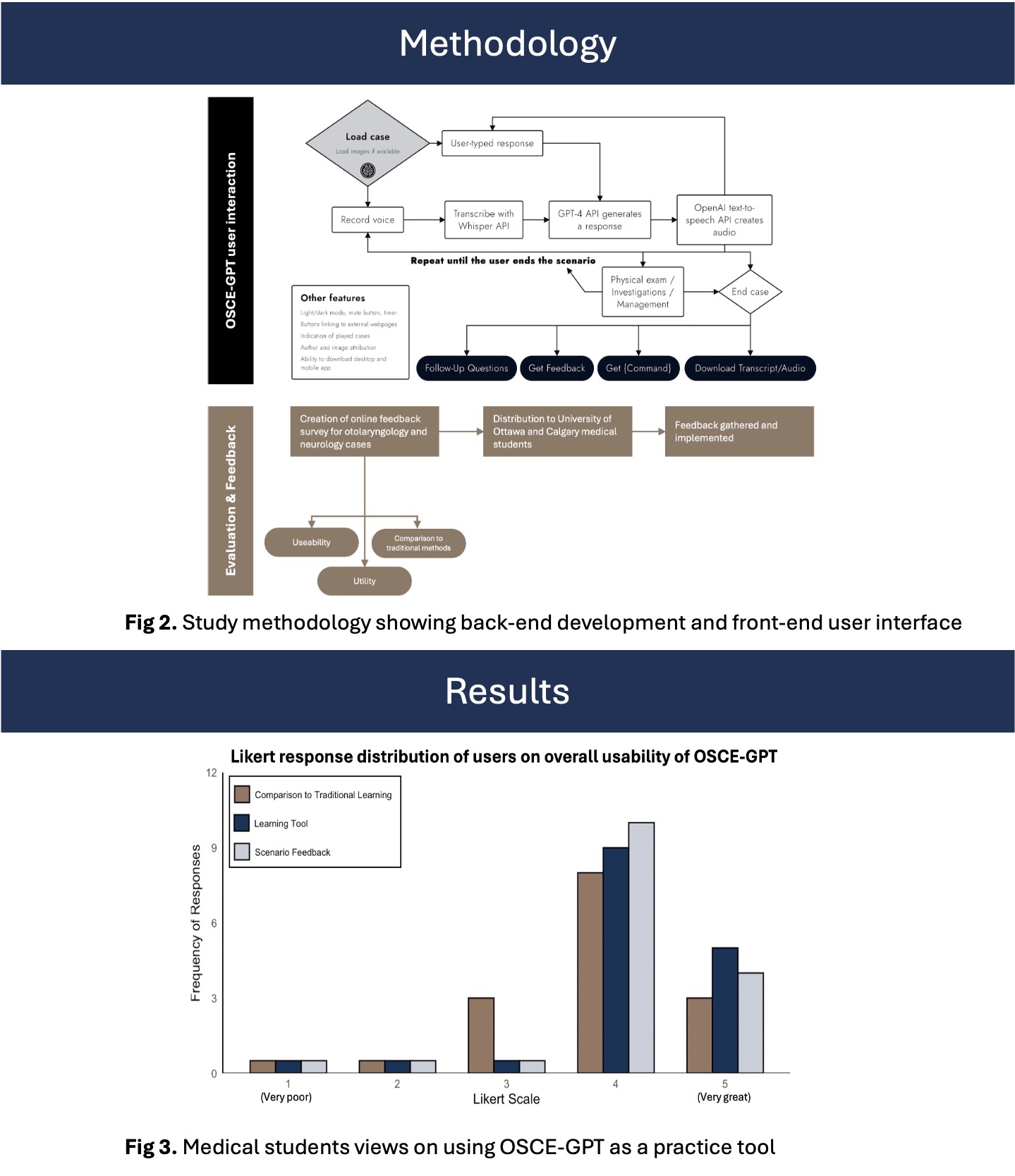
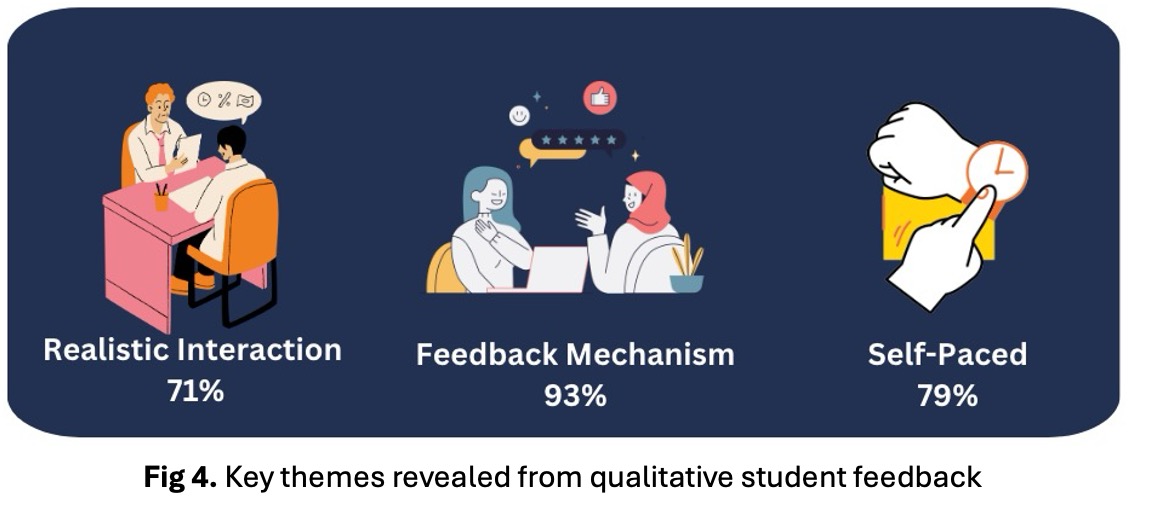
History of the endoscopic approach to the skull base with a highlight on Canada's contributions
The Early History of Transsphenoidal Approaches
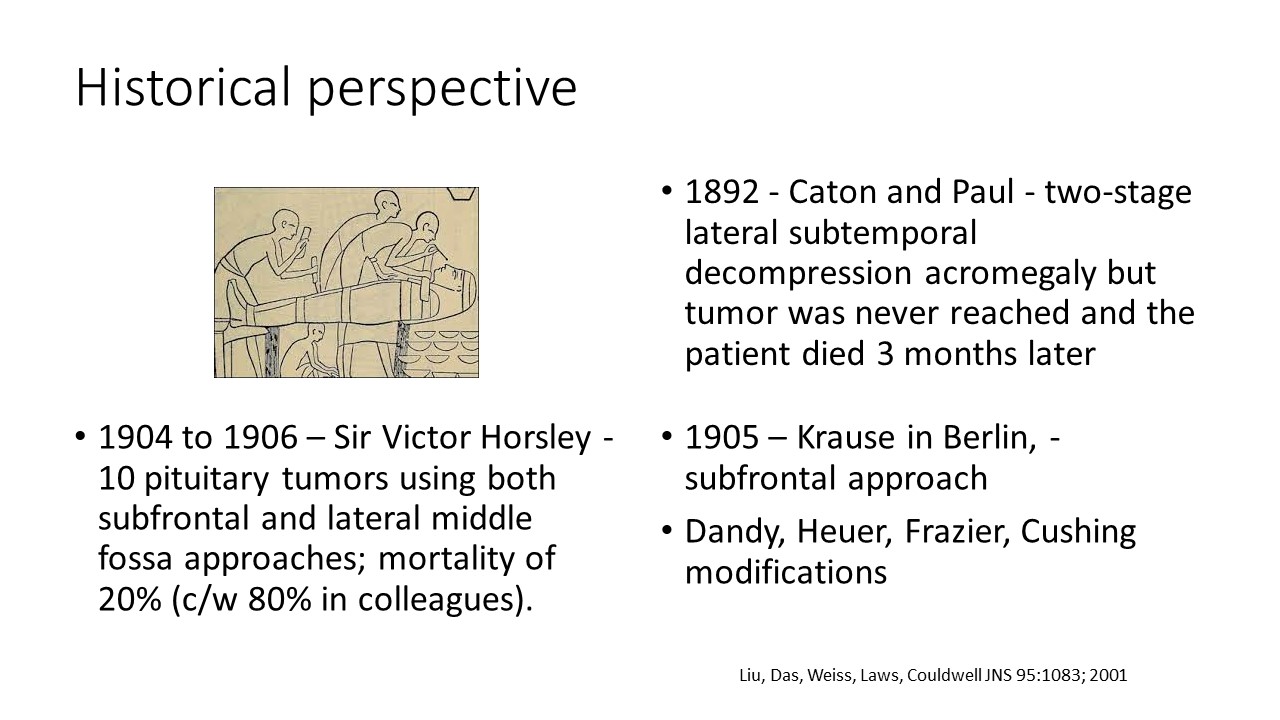
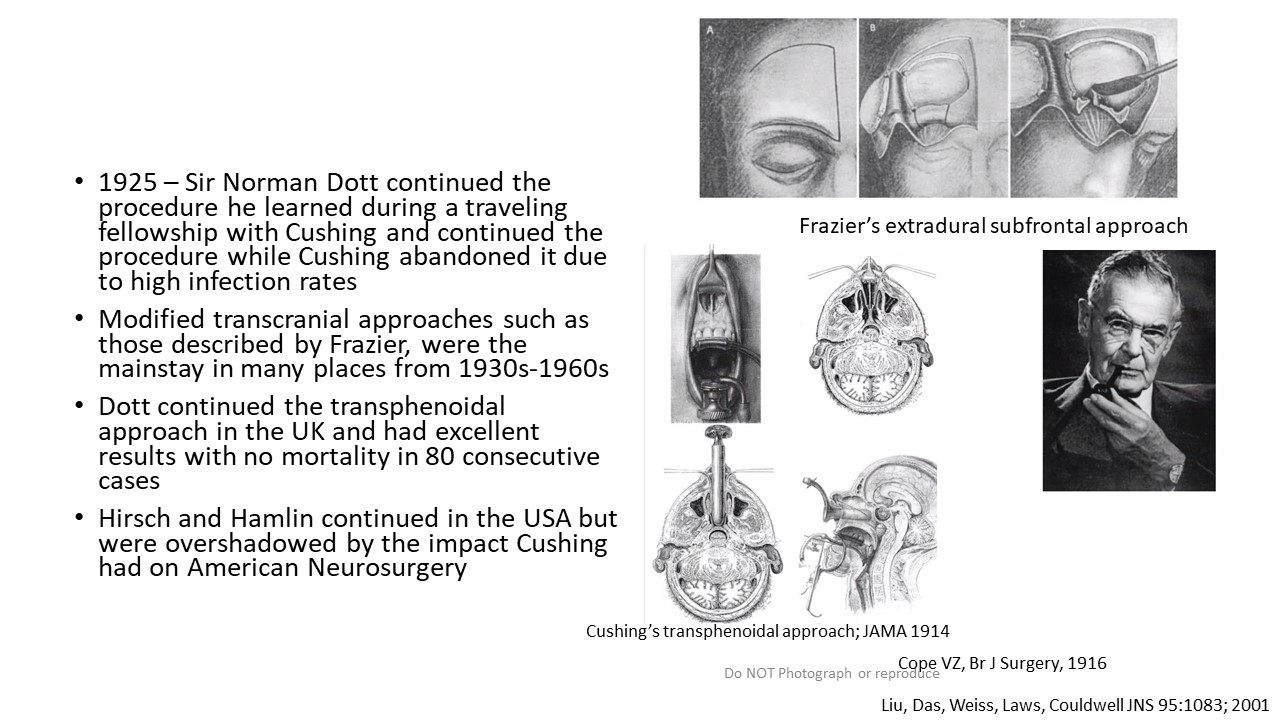
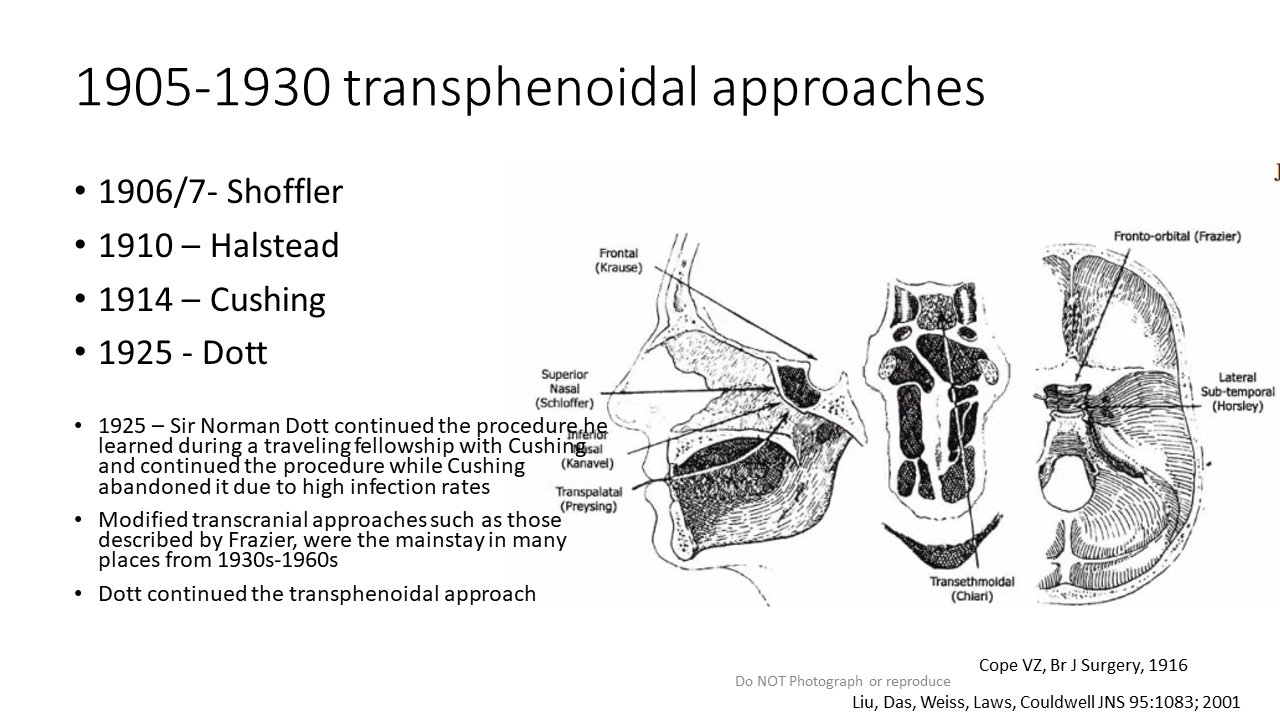
Transition from Microscope to Endoscopes

Expanded Fully Endoscopic Approach for a Giant PITNET using Our Technique
First Case of Fully Endoscopic Binostril 4-hand Transsphenoidal Approach to the Skull Base
First Publication done after several presentations to NASBS and others
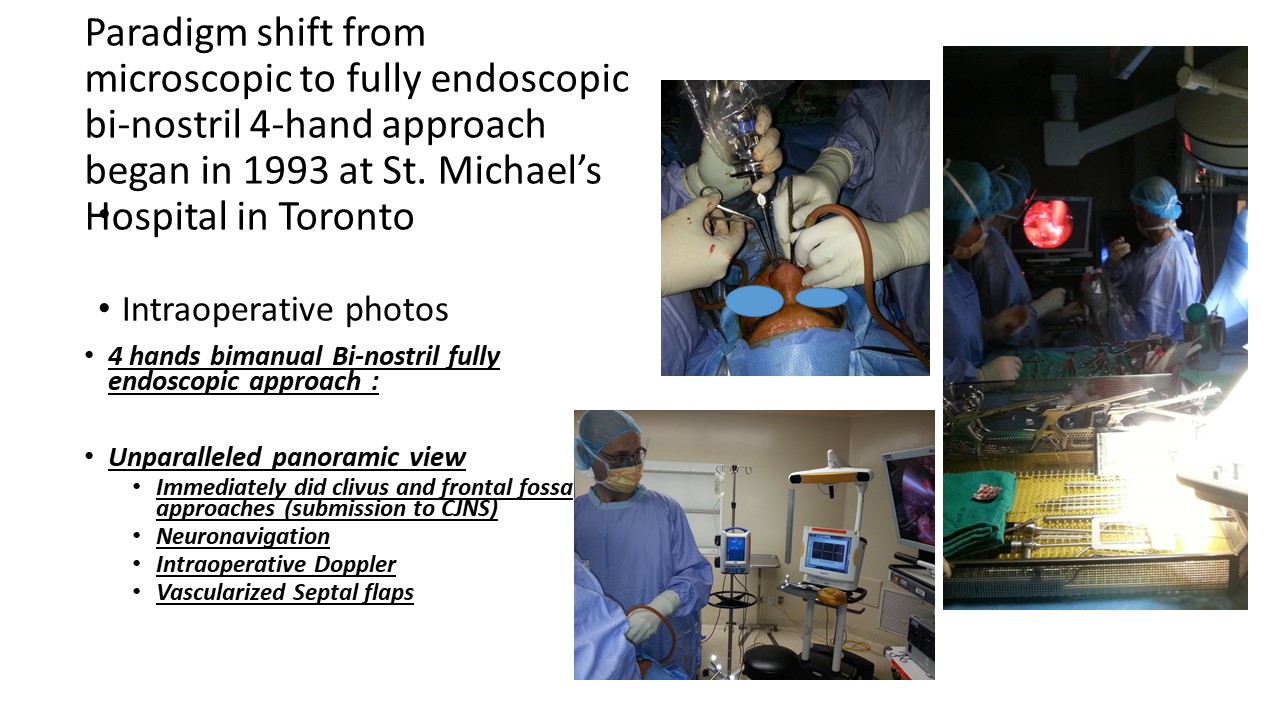
Dissemination of ETSS to other Surgeons and Sites Internationally

Expanded Endoscopic Approaches to all Regions of the Skull Base to C2
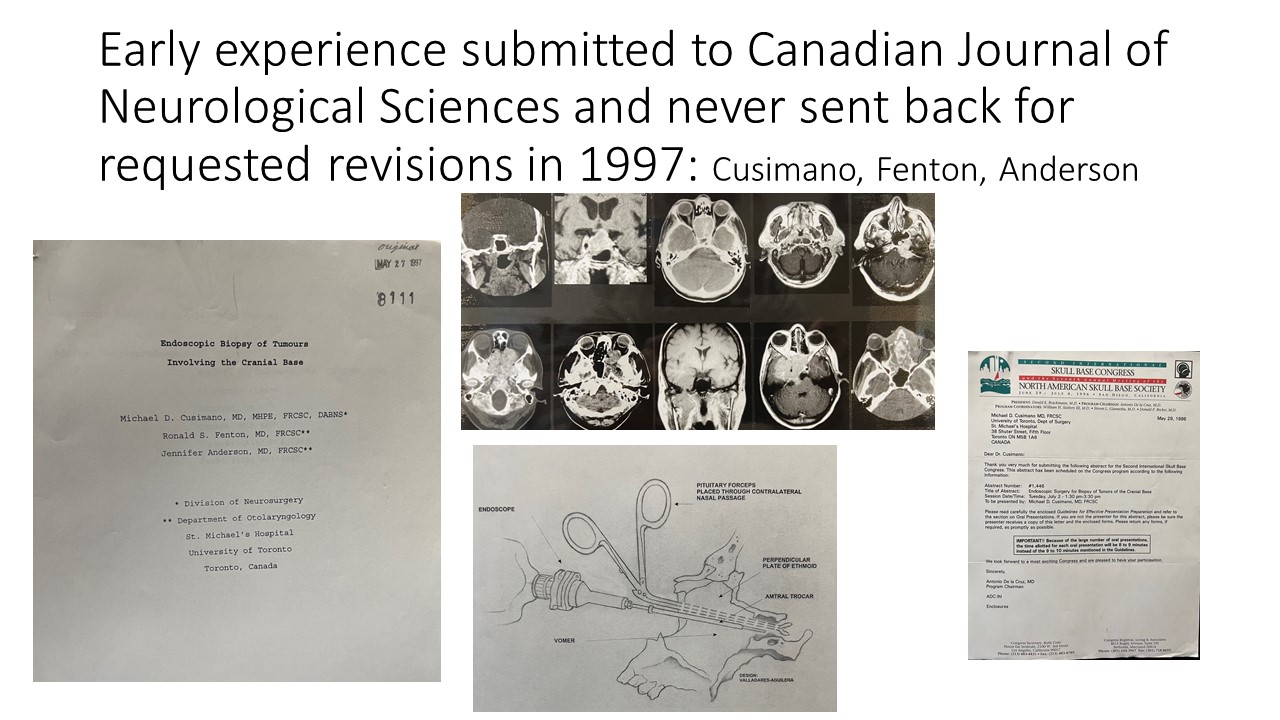
Spontaneous fluctuation of contrast enhancement in adult pilocytic astrocytoma and other low-grade brain tumors

Background
- Pilocytic astrocytoma is a slow-growing, WHO grade 1 tumor - up to 25% of pediatric brain tumors, less commonly occurs in adults.1
- Higher reported incidence of tumor recurrence (up to 30%), and malignant transformation amongst recurrent tumors (50-75%) in adults. 2-4
- Follow-up imaging is thus of import in assessing treatment response/stability - changes in tumor size, signal, and enhancement pattern most often used as markers of tumor activity.
- In diffuse low-grade gliomas (WHO grade 2), new or progressive enhancement is considered an indicator of progression and possible malignant transformation.5-7
- Pilocytic astrocytomas often demonstrate avid contrast enhancement in their solid portions and cyst walls, and can mimic high-grade gliomas with thick irregular peripheral enhancement.8-10
- Despite importance of imaging in follow-up of pilocytic astrocytomas and other low-grade brain tumors in adults, radiologic markers for malignant transformation are not well established in the literature. Further, increased enhancement is often interpreted as tumor progression.
- Objective: We aim to describe spontaneous fluctuations in contrast enhancement in adult pilocytic astrocytomas and other low-grade brain tumors, and help delineate its clinical significance.
Methods
- Retrospective review of institutional MRI database (2011-2021), search terms: "pilocytic", "pilomyxoid", "RGNT", "rosette", "glioneuronal", "DNET", and "dysembryoplastic"
- MRI reports, clinical records, and available surgical pathology reports reviewed for >900 results
- Exlulsion criteria: biopsy-proven WHO grade 3 or 4 tumors, age<19 years, equivocal findings for tumor diagnosis, less than 3 available MRI scans with tumor findings over at least 1 year
- MRIs of remaining 238 patients were reviewed - cases with changes in tumor enhancement in the absence of significant change in tumor size were indentified
- Conensus review of MRI scans by two neuroradiologists
Results

Table 1. Summary of demographic data, tumor characteristics, and imaging findings in patients with tumor contrast enhancement (CE) fluctuation.
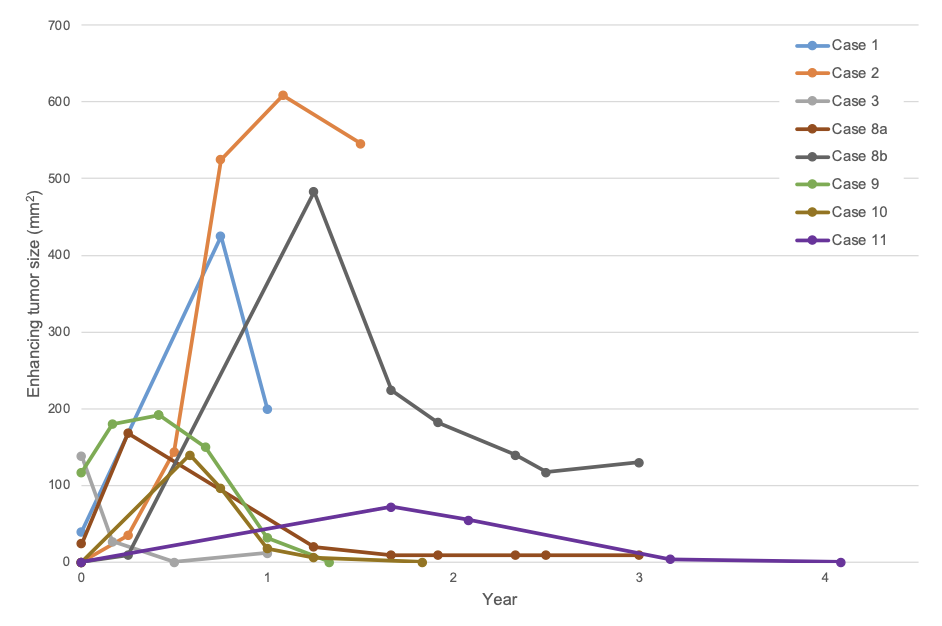
Figure 1. Patterns of contrast enhancement fluctuations. Enhancing tumor size (axial measurement product) plotted over time for each patient in our series. Two data sets were plotted for case 8, corresponding to enhancement in the thalamus (a) and cerebellum (b) in this patient with extensive tumor.
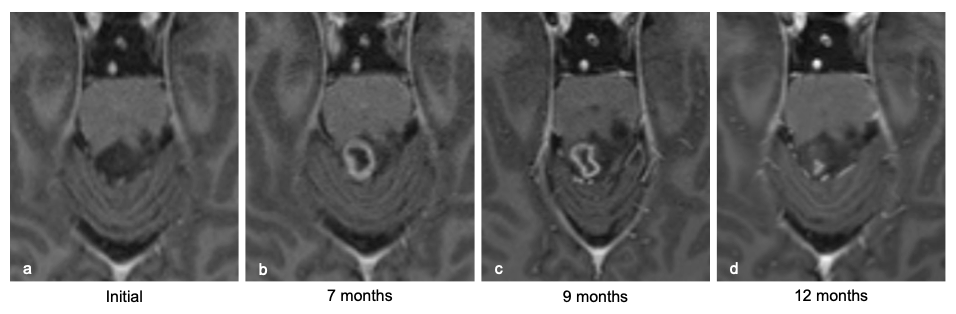
Figure 2. Case 10, low-grade glioma. Post-contrast T1-weighted axial images from 4 consecutive MRI scans done over 1 year show enlarging ring-like tumor enhancement in the midbrain tectum (a-b), with subsequent decrease (b-d).
Results
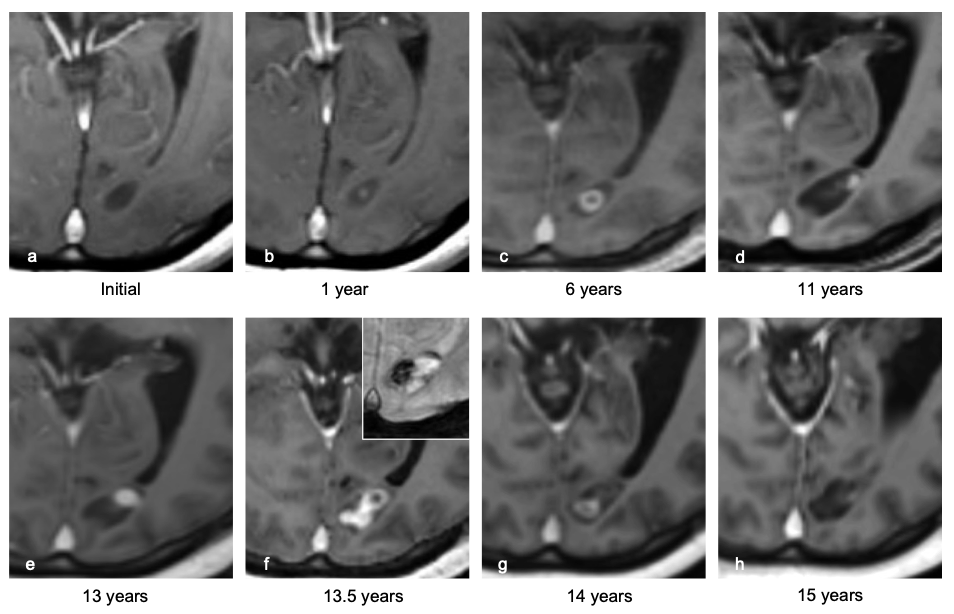
Figure 3. Case 7, pilomyxoid astrocytoma. Post-contrast T1-weighted axial images from representative non-consecutive MRI scans over 15 years demonstrate fluctuations in the size and morphology of tumor enhancement in the left occipital lobe (a-h). Gradient echo T2*-weighted image (f, inset) shows new intralesional hemorrhage during peak tumor enhancement at 13.5 years.
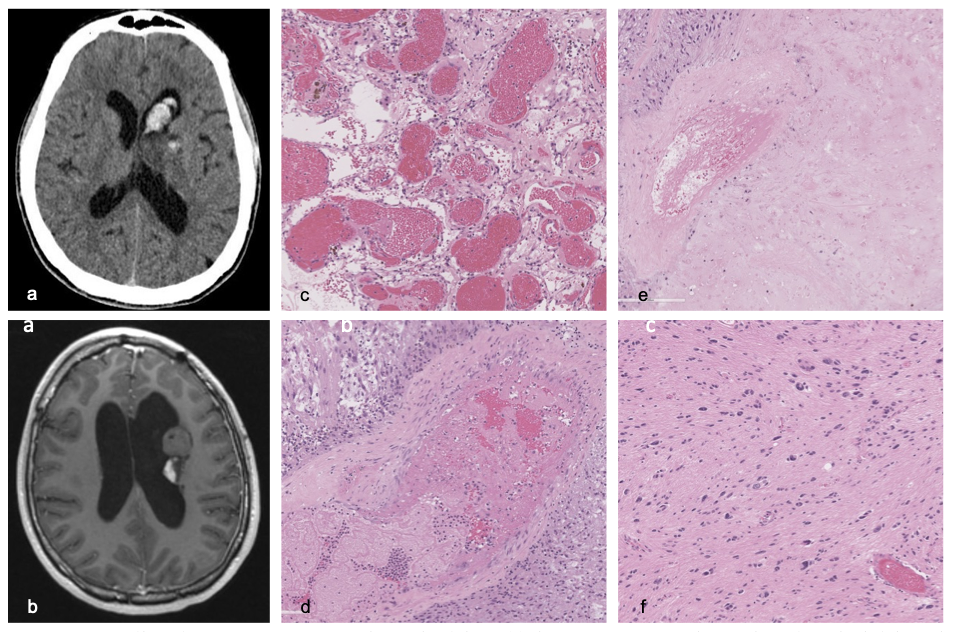
Figure 4. Case 1, pilocytic astrocytoma. Non-enhanced axial CT (a) demonstrates tumor hemorrhage into the left lateral ventricle, following patient’s presentation with new headache. Post-contrast T1-weighted axial images (b) show enhancing and non-enhancing components of the tumor in the left caudothalamic region. Photomicrographs of resected tumor demonstrate large dilated vessels (c), thrombosed vessel (d), and infarction (e) in its enhancing portion, and paucity of vascular changes in its non-enhancing component (f).
Conclusions
- First study in an adult population describing spontaneous changes in tumor enahncement despite stable size in pilocytic astrocytomas and pilomyxoid astrocytomas. Previously described in pediatric pilocytic astrocytomas, as well as adult RGNTs and DNETs.11-17
- Noted in supra- and infra-tentorial tumors, unresected and residual/recurrent tumors, and pilocytic astrocytoma, pilomyxoid astrocytoma, and RGNT low-grade glioma subtypes with no age predisposition.
- Patterns observed: appearance, increase, decrase, and/or disappearance of tumor enhancement. Four cases also demonstrated change in enhancement morphology.
- Despite fluctuations in enhancement size and morphology, clinical status was stable except in case 1.
- Proposed mechanism: cycles of vascular thrombosis, tumor infarction, and neovascularization (known to occur in pilocytic astrocytomas) - see histopathology correlation in case 1, and 2 cases with gross tumoral hemorrhage correlating during enhancement fluctuation.
- Prior studies show features resembling pilocytic astrocytoma on histology in resected DNETs and RGNTs with fluctuating enhancement, suggesting similar mechanism in other low-grade tumors.13,15-17
- Limitations: sample size, lack of corresponding histology at each stage of contrast enhancement, variable follow up intervals.
- Degree of enhancement of pilocytic astrocytoma on initial imaging has no correlation with clinical outcome, tumor progression, or recurrence.18
- We demonstrate that spontaneous contrast enhancement fluctuation in pilocytic astrocytomas and related low-grade tumors is not a reliable indicator of tumor behavior, and thus should not be used as a radiologic marker for progression or malignant transformation.
- This has the potential to circumvent unnecessary interventions or treatment changes in otherwise clinically stable patients.
Assessing the emergence and evolution of artificial intelligence and machine learning research in neuroradiology

Introduction
• Artificial intelligence (AI) is a field focusing on the development of tools that mimic human cognition, especially its learning, decision, and interpretation capabilities. In recent years, the field has rapidly grown in its knowledge base and complexity.
• In recent years interest in AI and machine learning (ML) has been growing in neuroradiology, but there is limited knowledge on how this interest has manifested into research and its respective qualities and characteristics.
• This study aims to characterize the emergence and evolution of AI/ML articles within neuroradiology and provide a comprehensive overview of the trends, challenges, and future directions of the field.
Methods
• We performed a bibliometric analysis of the American Journal of Neuroradiology (AJNR) where we included original research articles published between journal inception (January 1, 1980) to the date the query was conducted (Dec. 3, 2023) that contained any of the following key terms: “machine learning”, “artificial intelligence”, “radiomic”, “deep learning”, “neural network”, “generative adversarial network”, “object detection”, “natural language processing” and fit the definitions of AI and ML as described in Erickson et al. (2017) and Wagner et al. (2021).
• To better understand the limiting factors to Type 3 articles being published, our analysis focused more on the quantitative and qualitative characteristics of Type 2 articles as they should represent the precursor work leading to Type 3.
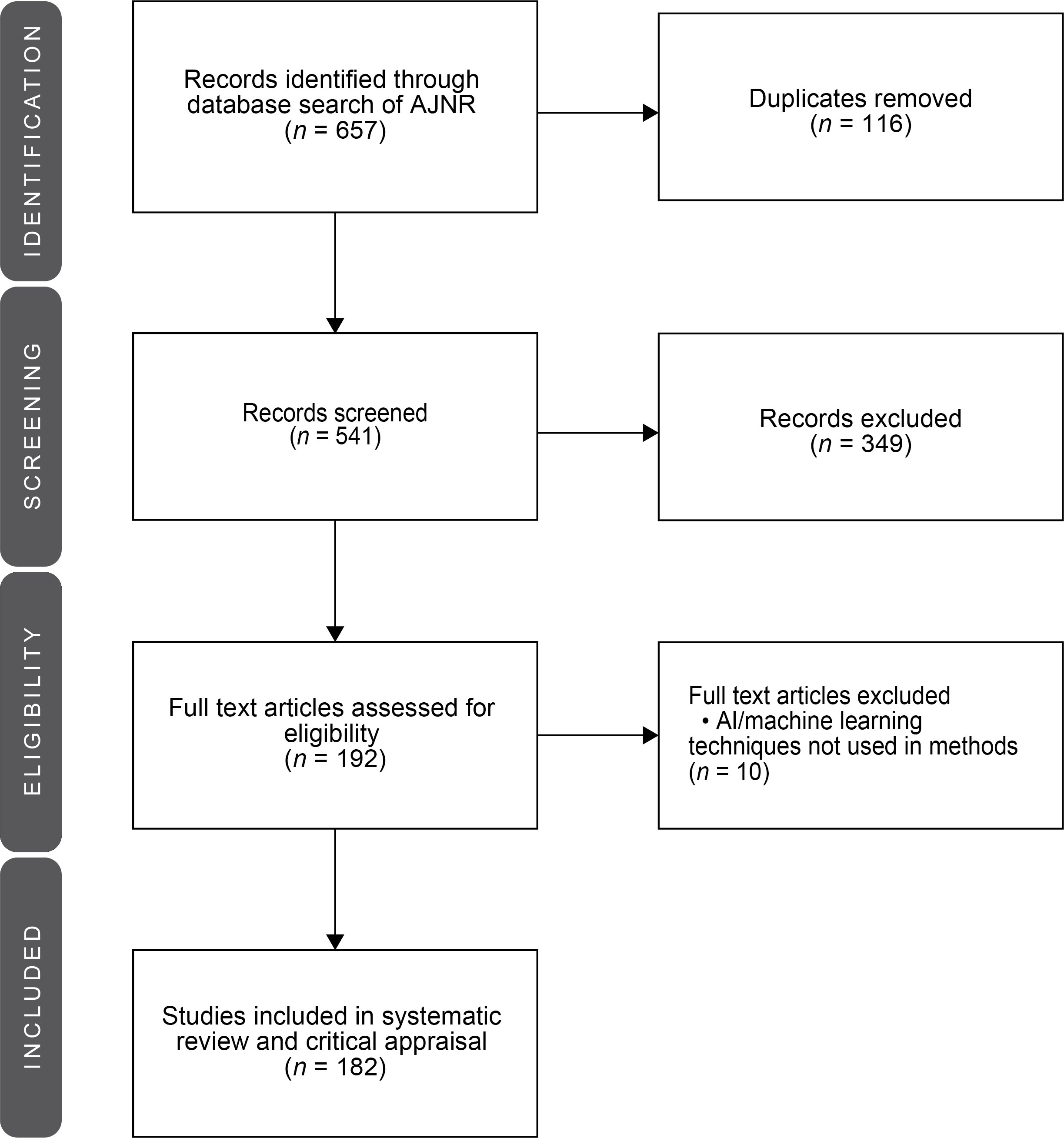
FIG 1. Flow chart of the article screening process.
Results
• The number of articles published has steadily grown since 2007 with a twenty-five- and five-fold increase in the last fifteen and five years respectively with non-integration mainly driving this growth.
• A total of 182 articles were identified with developmental research articles without direct clinical integration representing 79% of all AI/ML articles (Type 1 – Statistical Modelling, n = 53; Type 2 – AI/ML Development, n = 90) with the remaining 21% of articles being integration-focused (Type 3 – End-user application, n = 39).
• The vast majority of the ninety Type 2 articles focused solely on the adult population (n = 72, 80%) with the remainder focusing on pediatric (n = 14, 16%) or adult and pediatric populations (n = 4, 4%) (Fig 3c).
• Two-thirds (n = 57, 63%) of all Type 2 publications had a radiologist as a first or corresponding/senior author and among these radiologist-led Type 2 publications, sixty percent (n = 34, 60%) were led by a radiologist with graduate degrees, many of them being PhD and MBA degree holders.
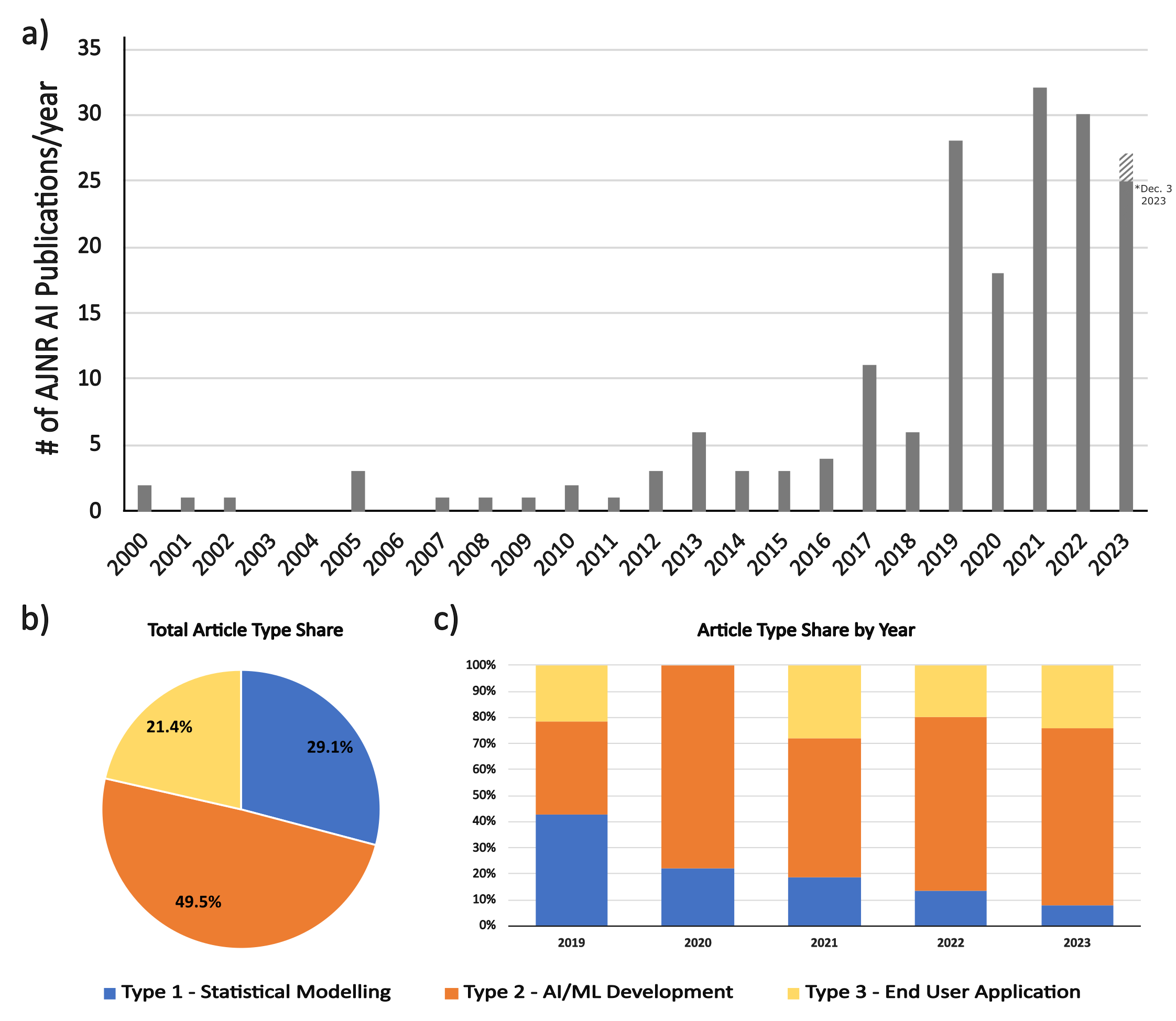
FIG 2. Global Results (Type 1, 2, and 3). Data characterizing the growth of all AI/ML articles (i.e., Type 1, 2, and 3). a) The number of all articles published from the first year an AI/ML article was published in the AJNR in 2000 to the article search date on Dec. 3rd, 2023. *Striped bar in 2023 indicates the extrapolated number of articles published in that year should the search have occurred at the end of the year. b) Pie chart breaking down the share each article type holds among all AI/ML publications. c) Percentile bar graph demonstrating article type share in the last five years.
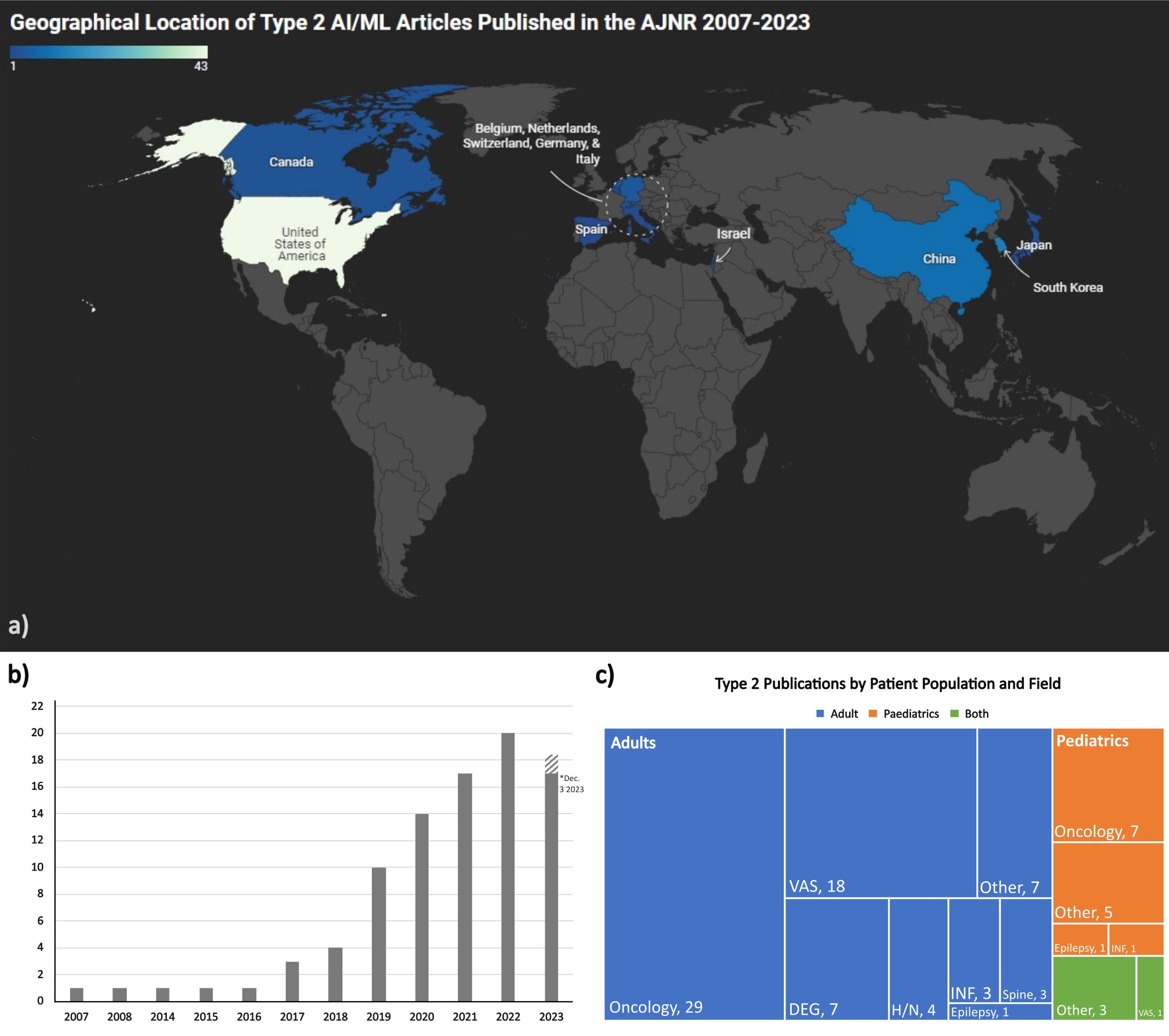
FIG 3. Qualitative Type 2 results. General overview of Type 2 publication characteristics (n = 90). a) A world map showing where studies were conducted. b) Bar graph demonstrating the number of Type 2 articles published in years with at least 1 article published. *Striped bar in 2023 indicates the extrapolated number of articles published in that year should the search have occurred at the end of the year. c) Graphic display of the patient populations and topics studied. VAS = Vascular, DEG = Degenerative, H/N = Head & Neck, INF = Inflammation.
Conclusion
• Our investigation confirmed the rapid growth of AI research in neuroradiology and that AI/ML developmental research work without direct clinical integration is the primary driver of publication growth.
• Improving the quality of this research work will be crucial to promote their integration into day-to-day practice.
• These results ultimately provide authors, editors, clinicians, and policymakers important insights to promote a shift towards integrating practical AI/ML solutions in neuroradiology.
Anatomy and pathology of the lacrimal apparatus: from the sac to the nasal fossa. what the neuroradiologist should know!

Purpose:
- To review anatomy and radiological features of common nasolacrimal duct pathologies.
- Describe different imaging features of common cases encountered and usually overlooked.
Educational Goal:
- The lacrimal apparatus includes the various structures related to the production and flow of tears. In this educational exhibit we will focus on the excretory apparatus from the lacrimal sac to the nasal fossa.
- We will provide an anatomical review of the various structures easily identifiable on CT and MRI. We will present various pathologies affecting the excretory lacrimal apparatus with attention to the specific features of each condition to facilitate an appropriate differential diagnosis.
- We will emphasize specific anatomical/imaging findings to help the diagnosis for the neuroradiologist and useful to the ENT surgeon.
Anatomy/Physiology:
- The lacrimal gland is situated at the superolateral aspect of the orbit. It is a serous gland that produces tears. These tears are mixed with mucous secretions produced by the eyelid and conjunctival glands, which produce an oily tear-resistant film across the eye globe.(1)
- The lacrimal sac occupies the bony lacrimal fossa. The anterior and posterior crests form the lacrimal bone. The nasolacrimal duct comprises intra-osseous and membranous parts that terminate below the inferior turbinate.
- The lacrimal drainage system facilitates the drainage of the tears.(1)
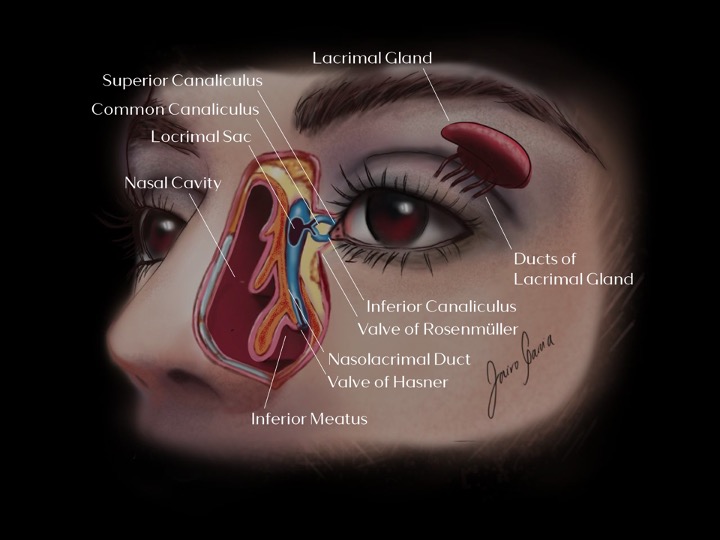
Illustration of normal nasolacrimal apparatus anatomy.
- There are two mechanisms of tear drainage:
- When the orbitalis oculi muscle contracts during eyelid closure, it creates positive pressure in the lacrimal sac, which closes the valve of Rosenmüller, forcing tears down the nasolacrimal duct. (2)(3)
- When the eyelids open, they create negative pressure in the lacrimal sac, causing the valve of Rosenmüller to open. This pushes the tears through the puncta into the canaliculi and the lacrimal sac.(2)(3)
- Finally, the tears go through the Hasner valve into the inferior meatus.
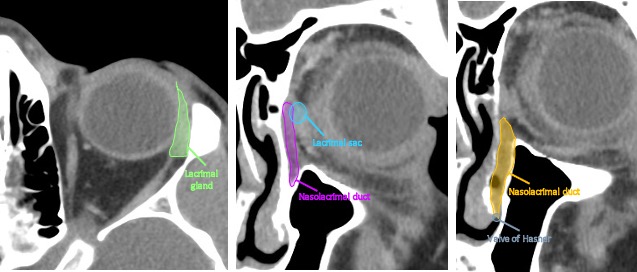
Radiological anatomy of the nasolacrimal apparatus.
Cases:
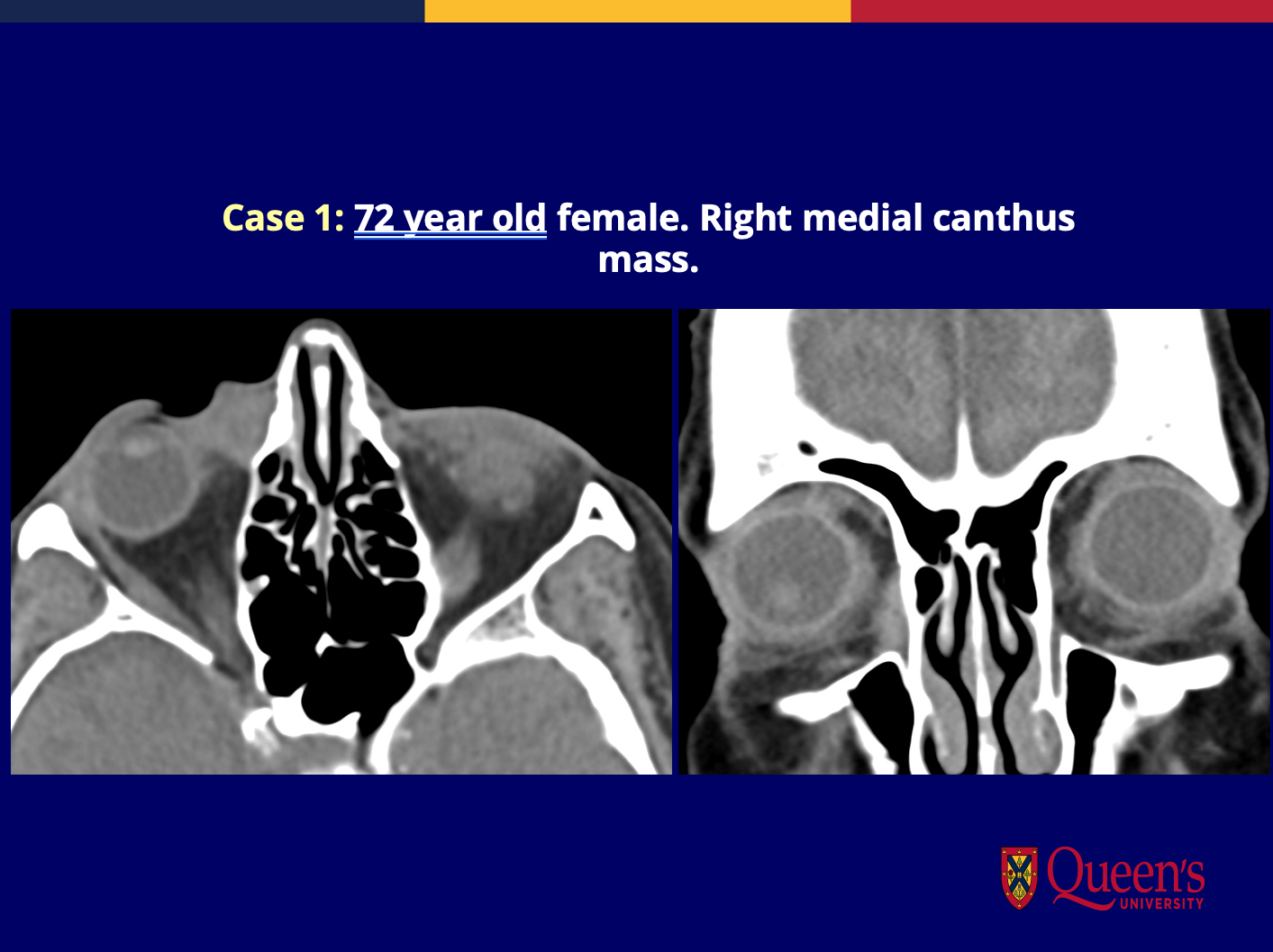
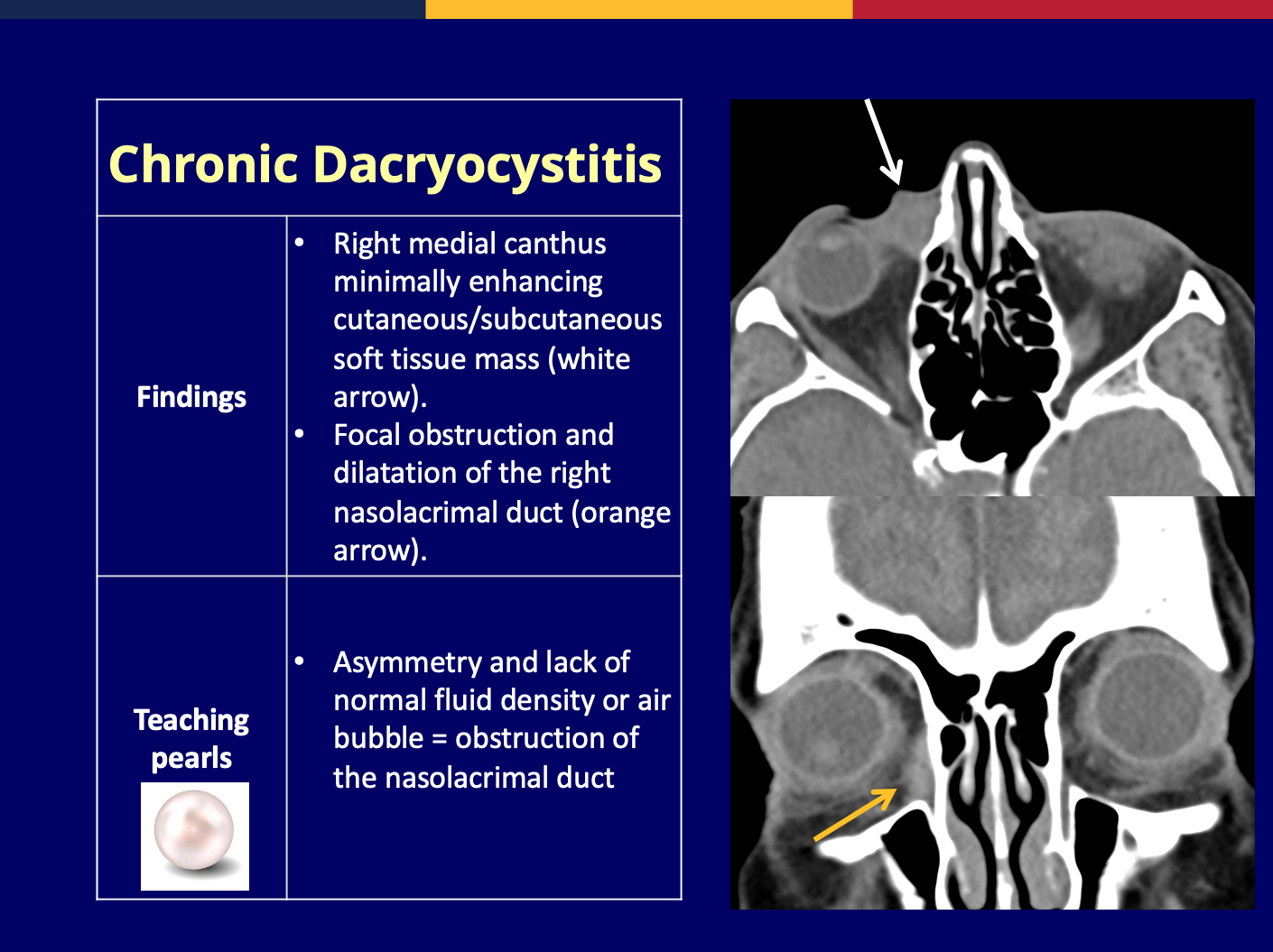
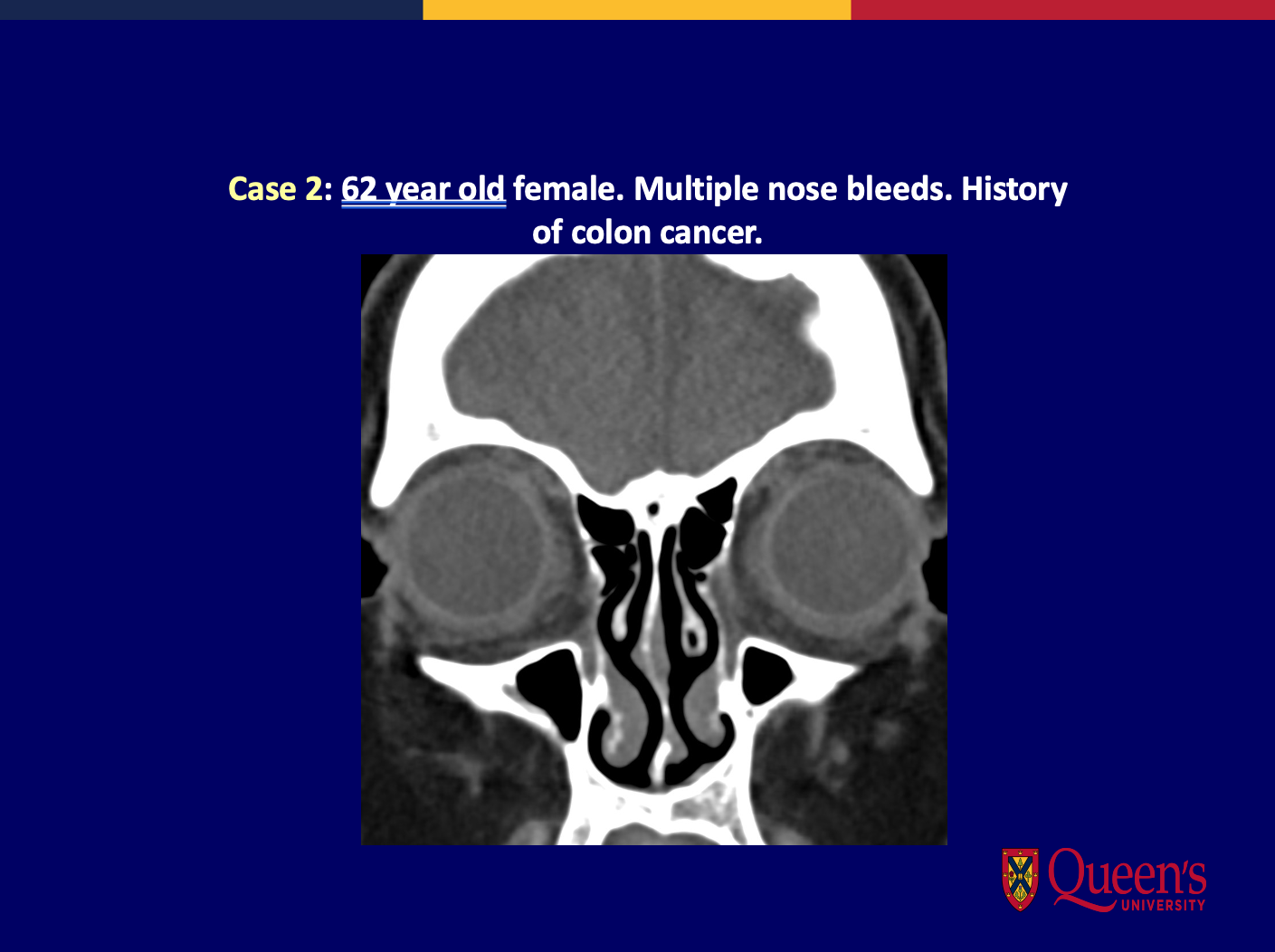
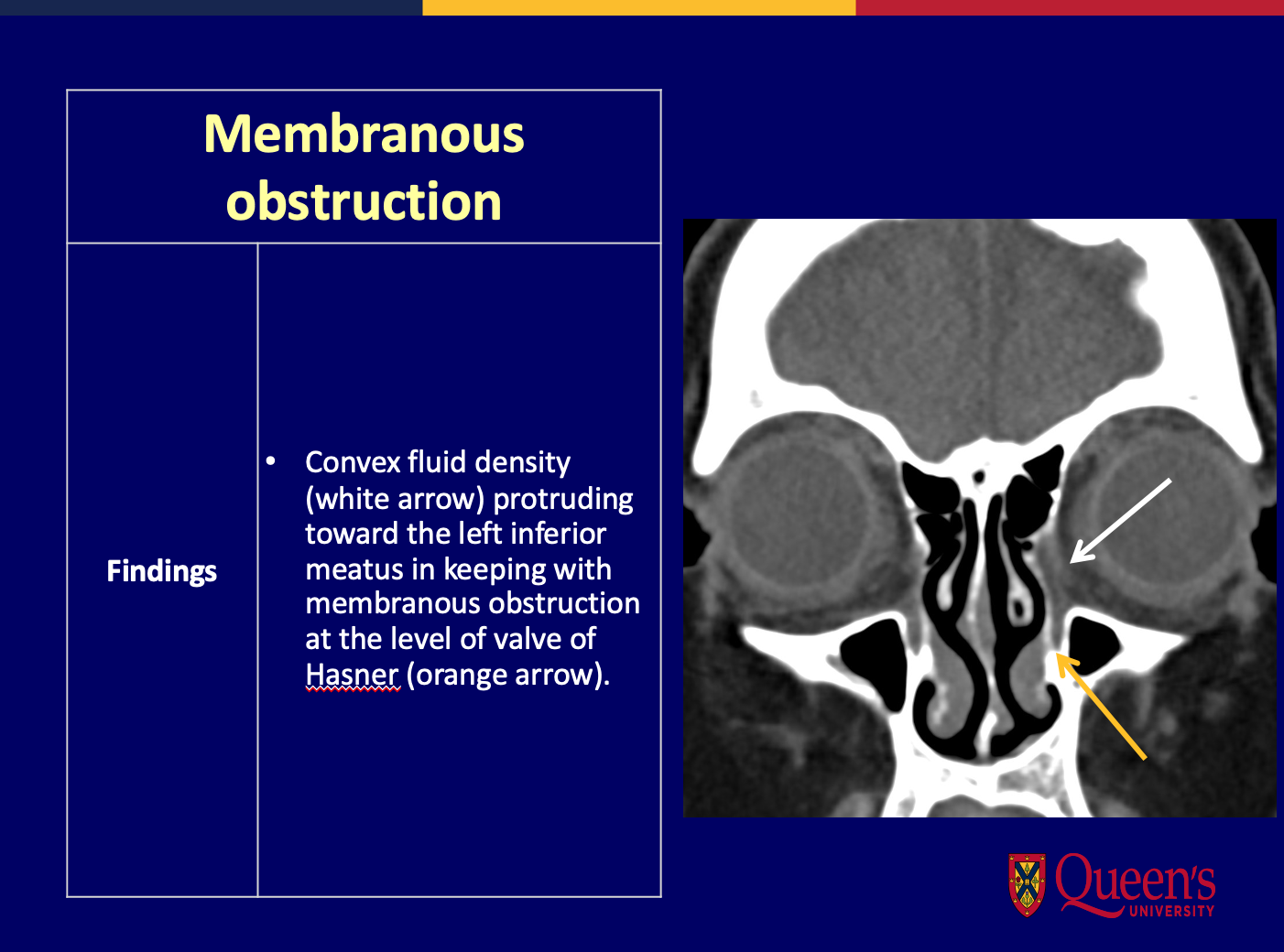

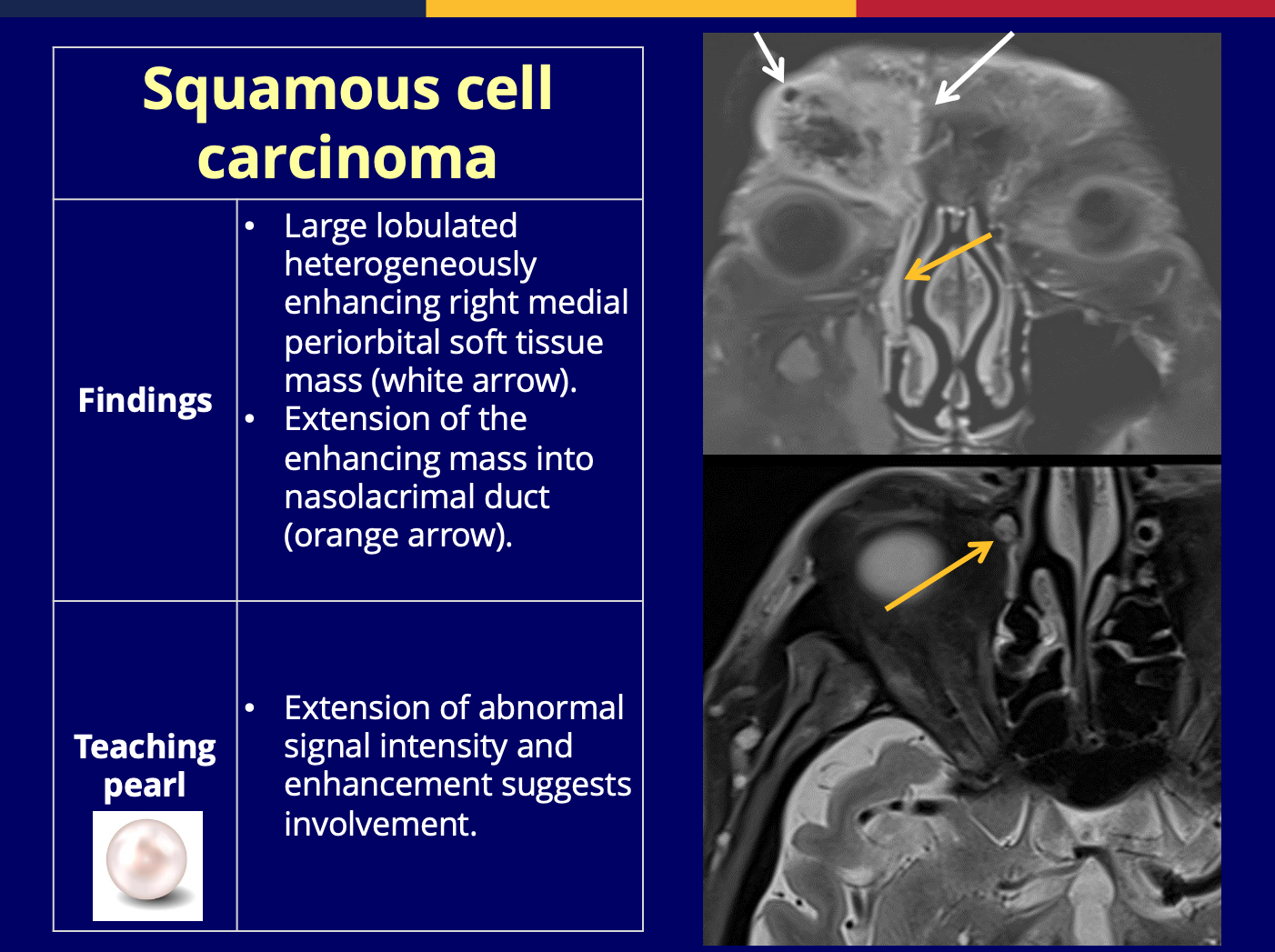
Cases:
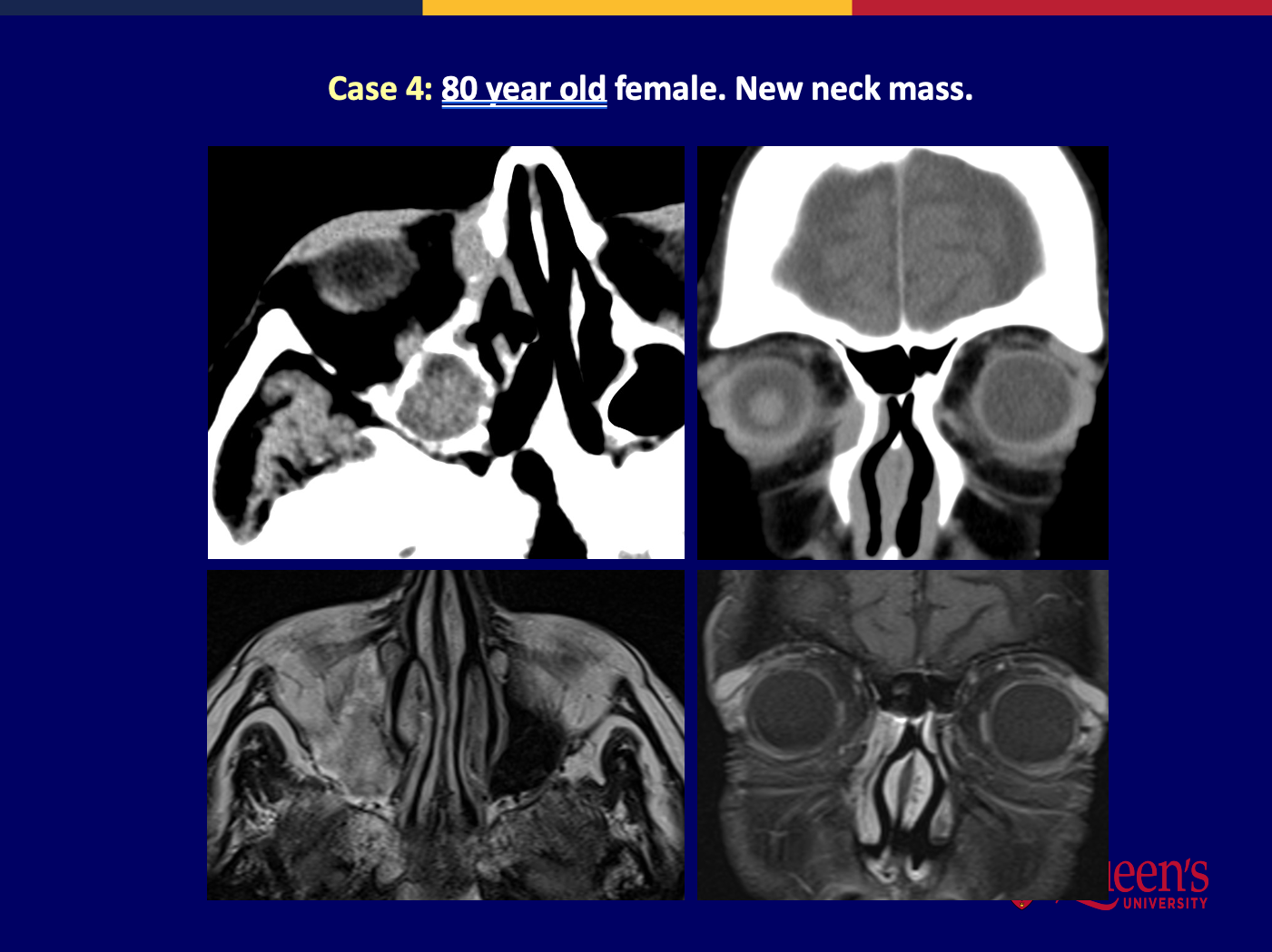
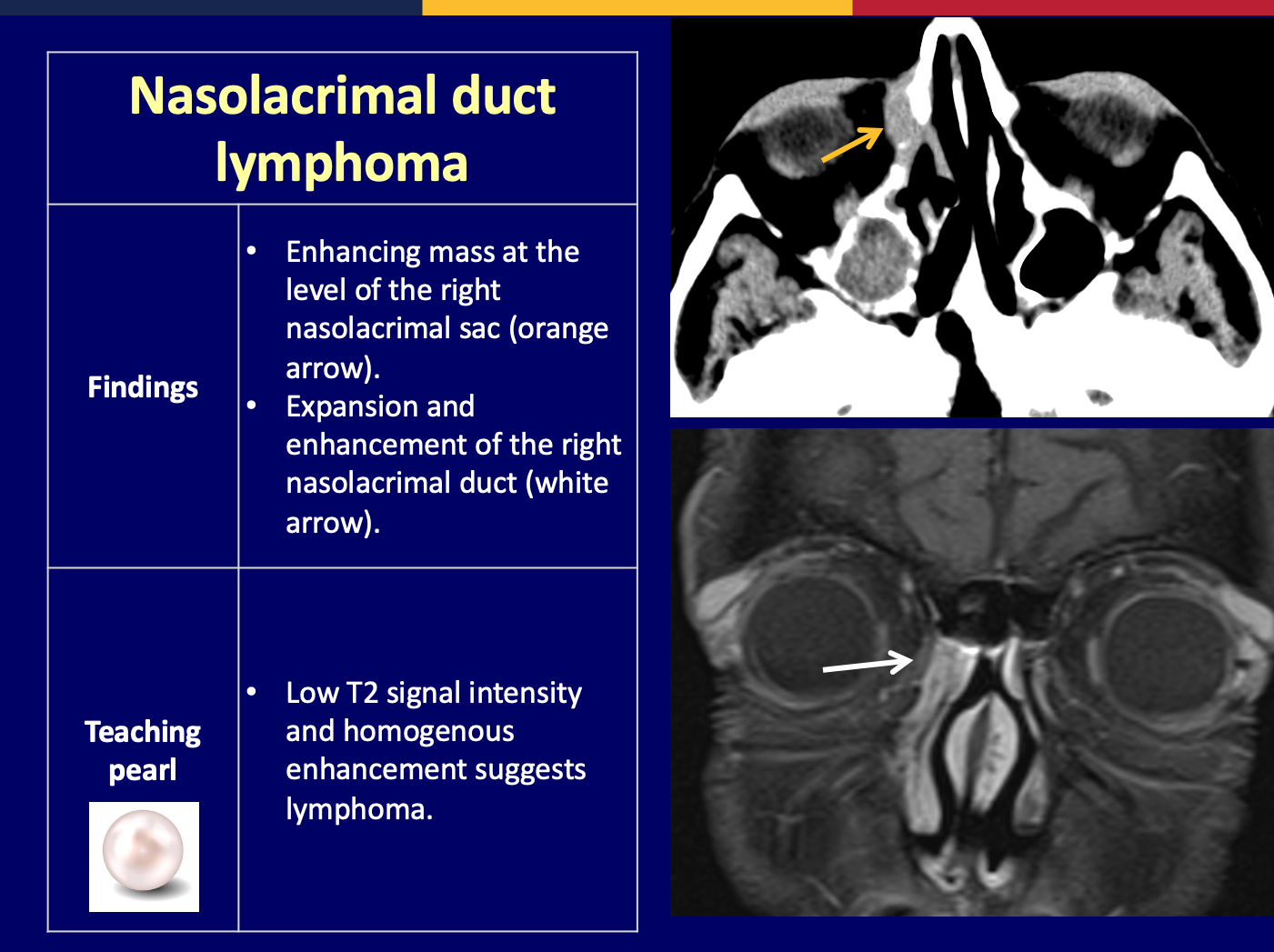
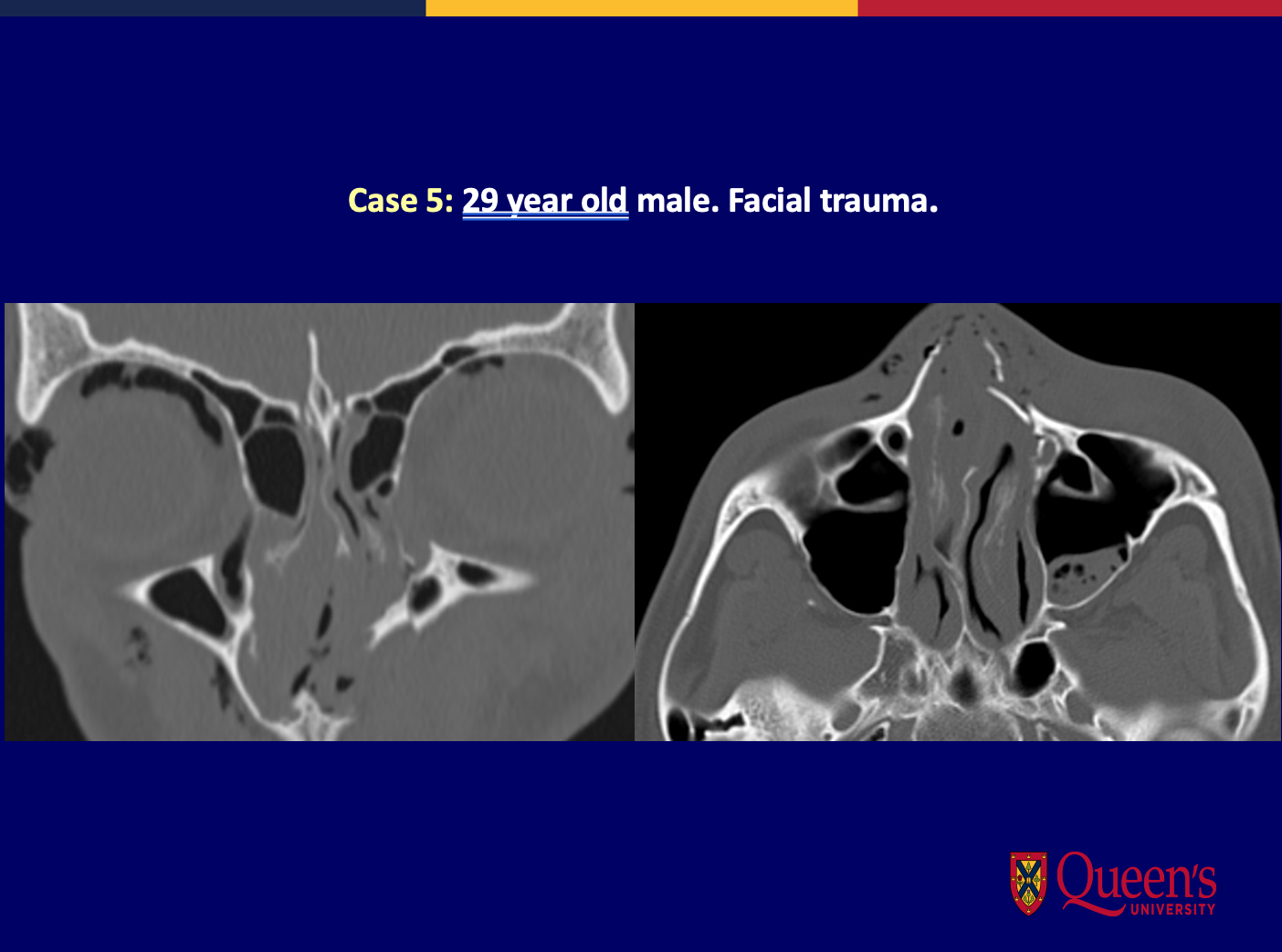
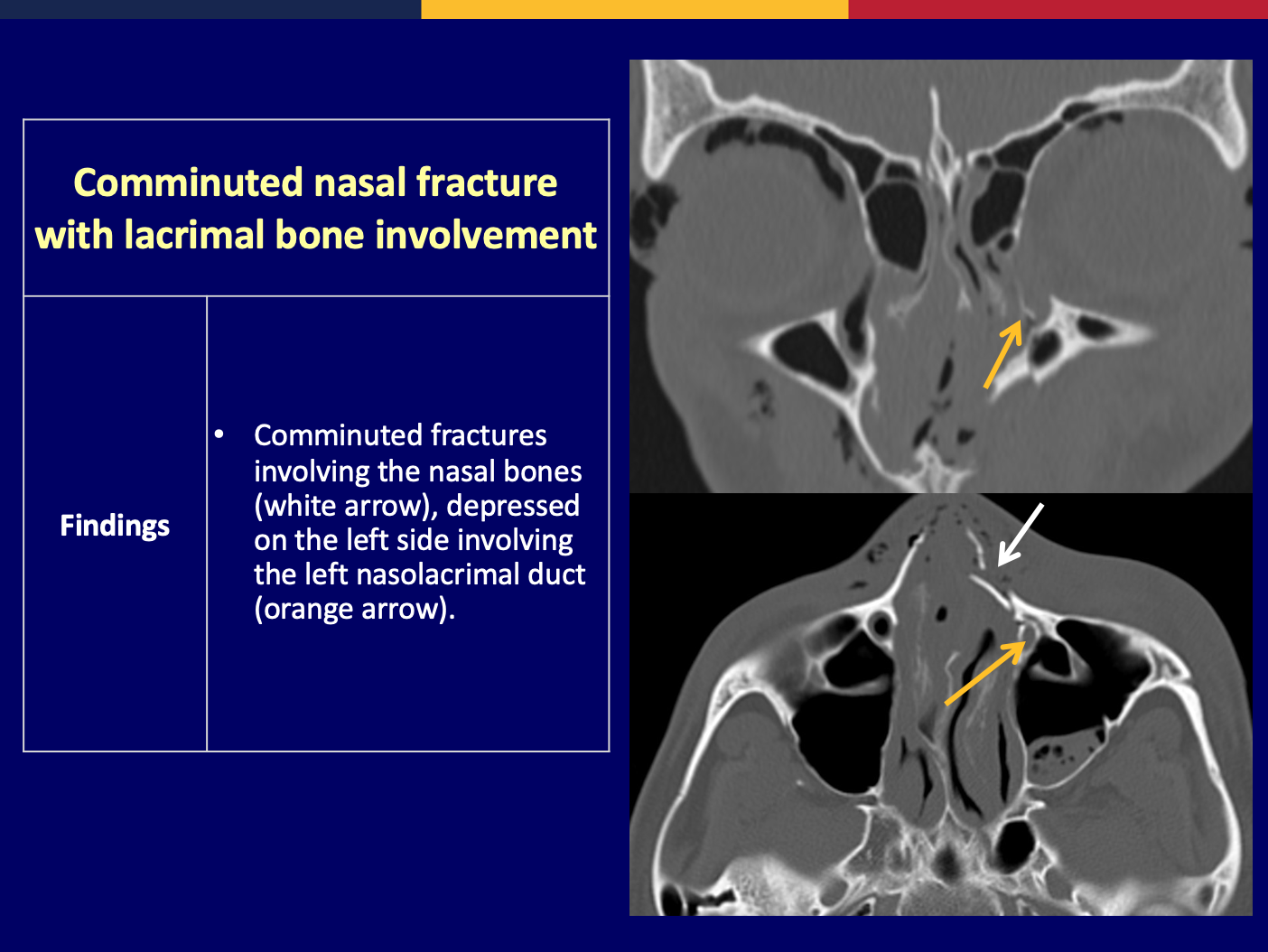
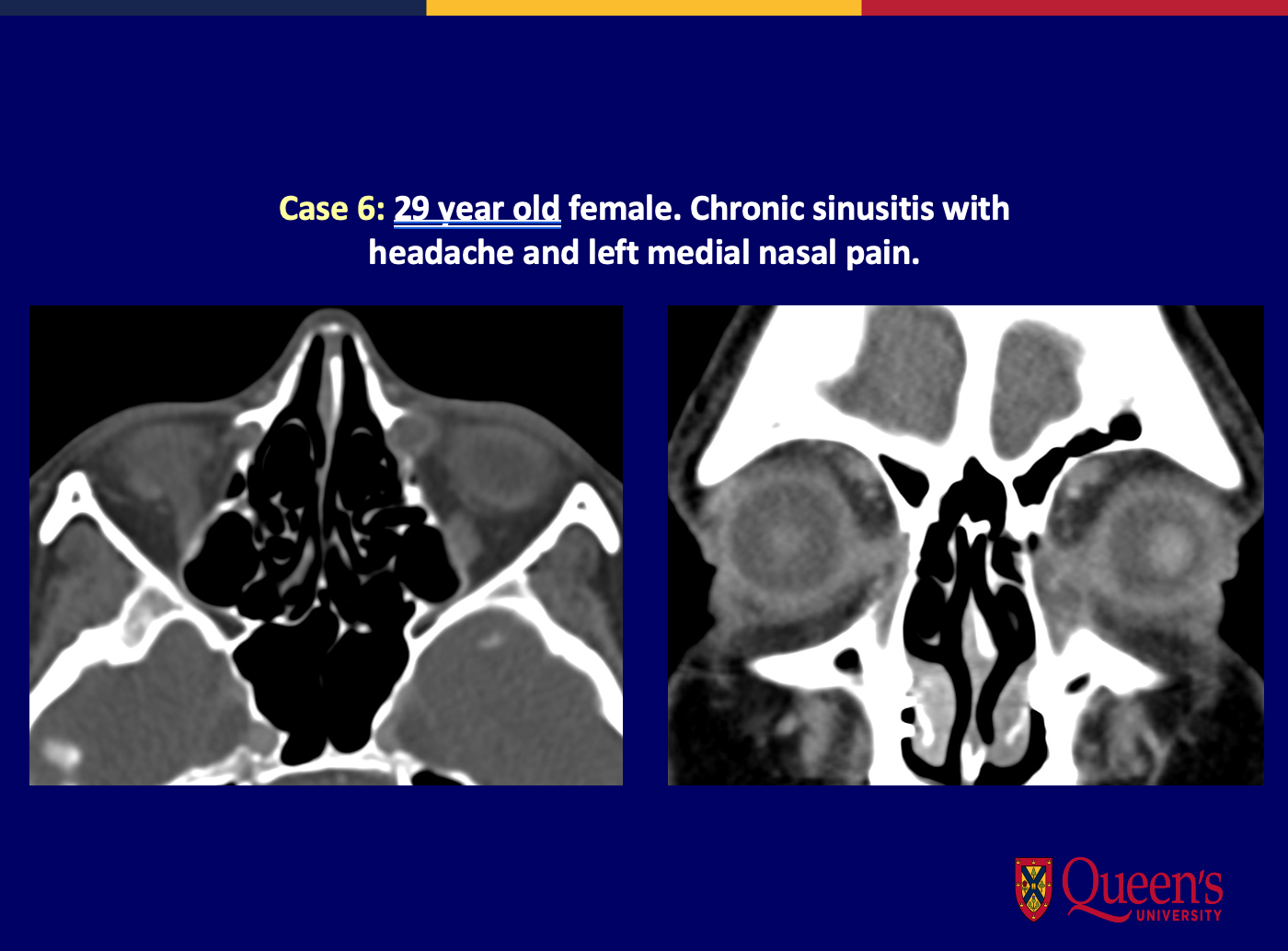
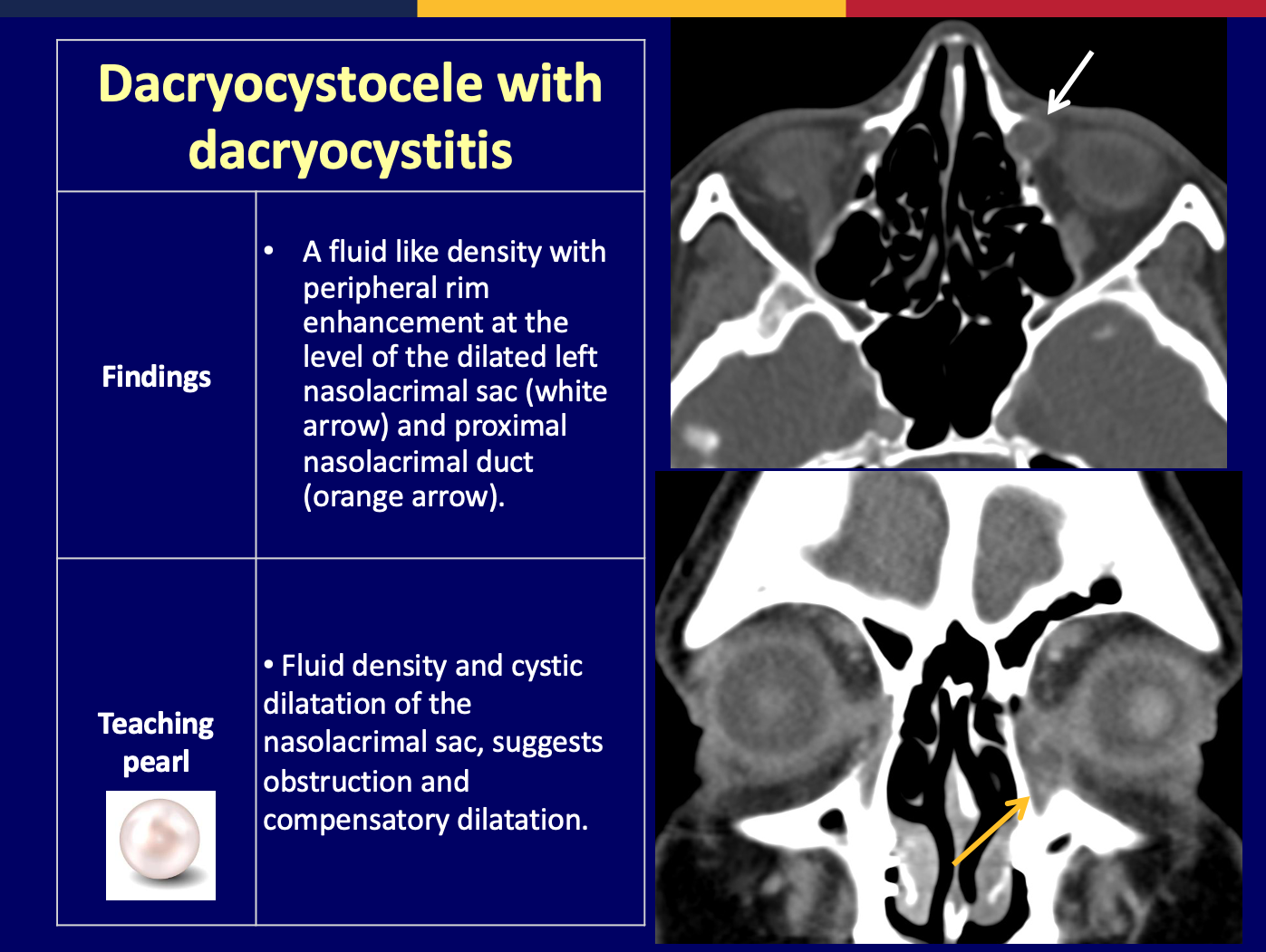
Cases:
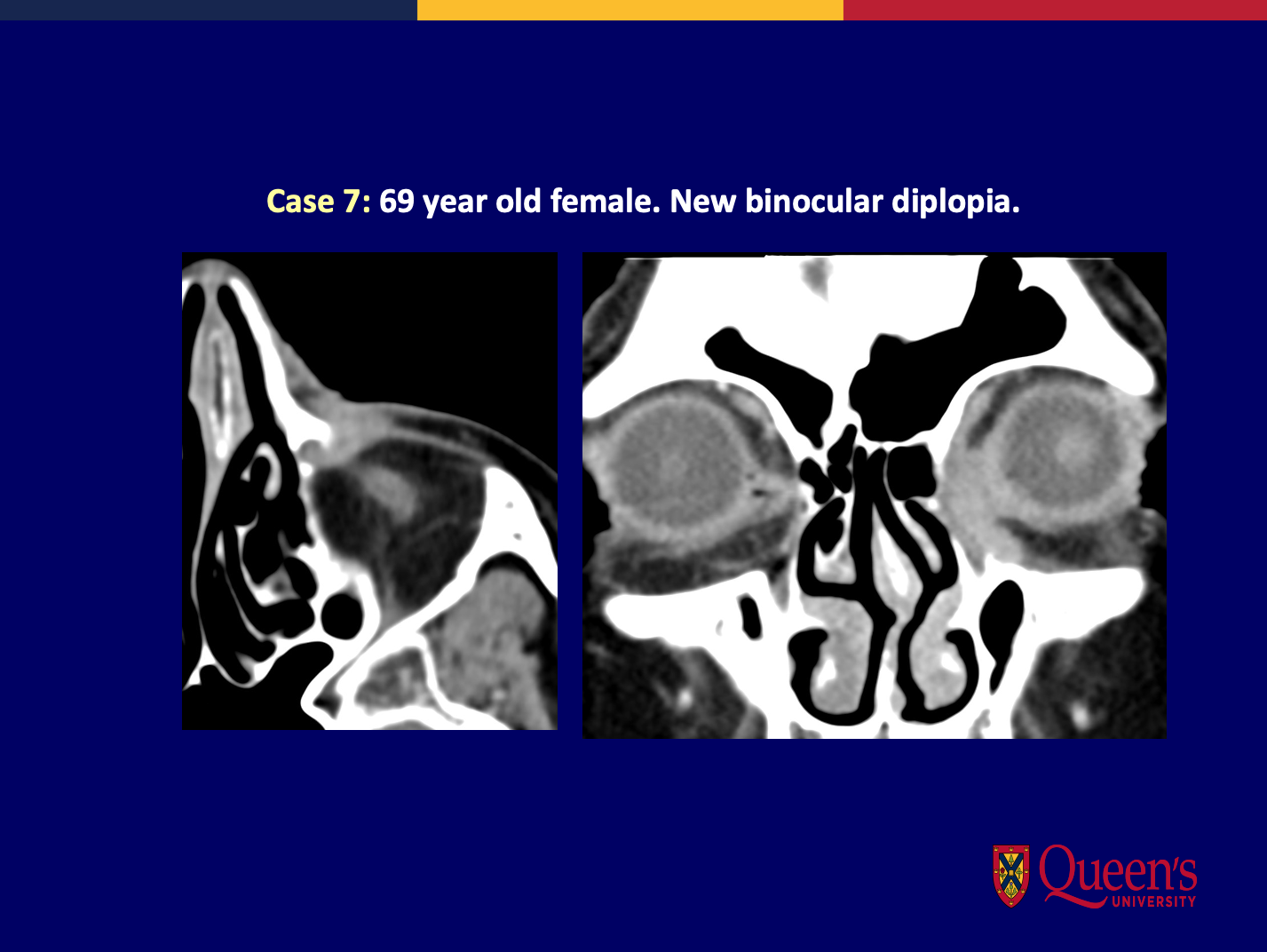

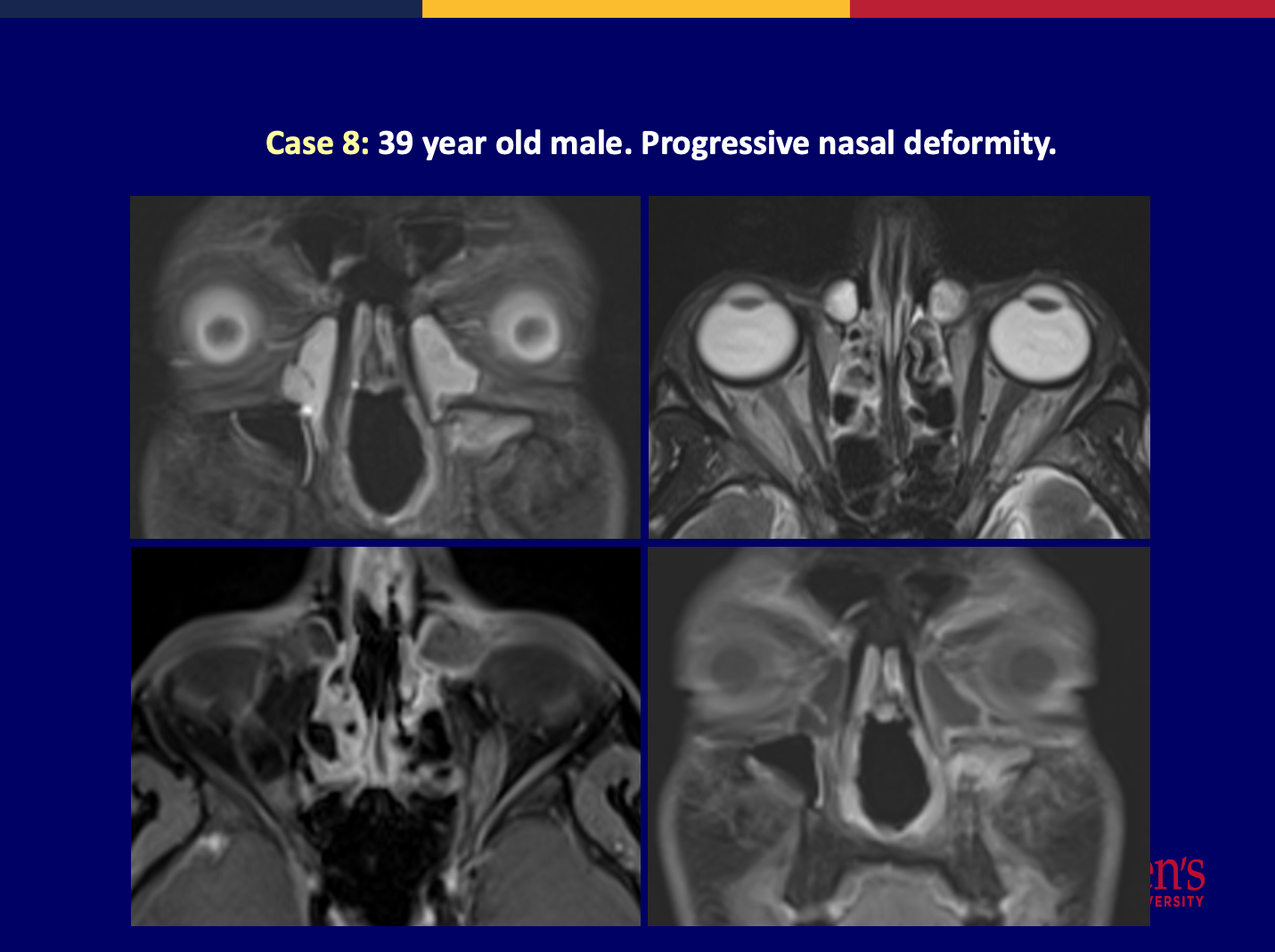
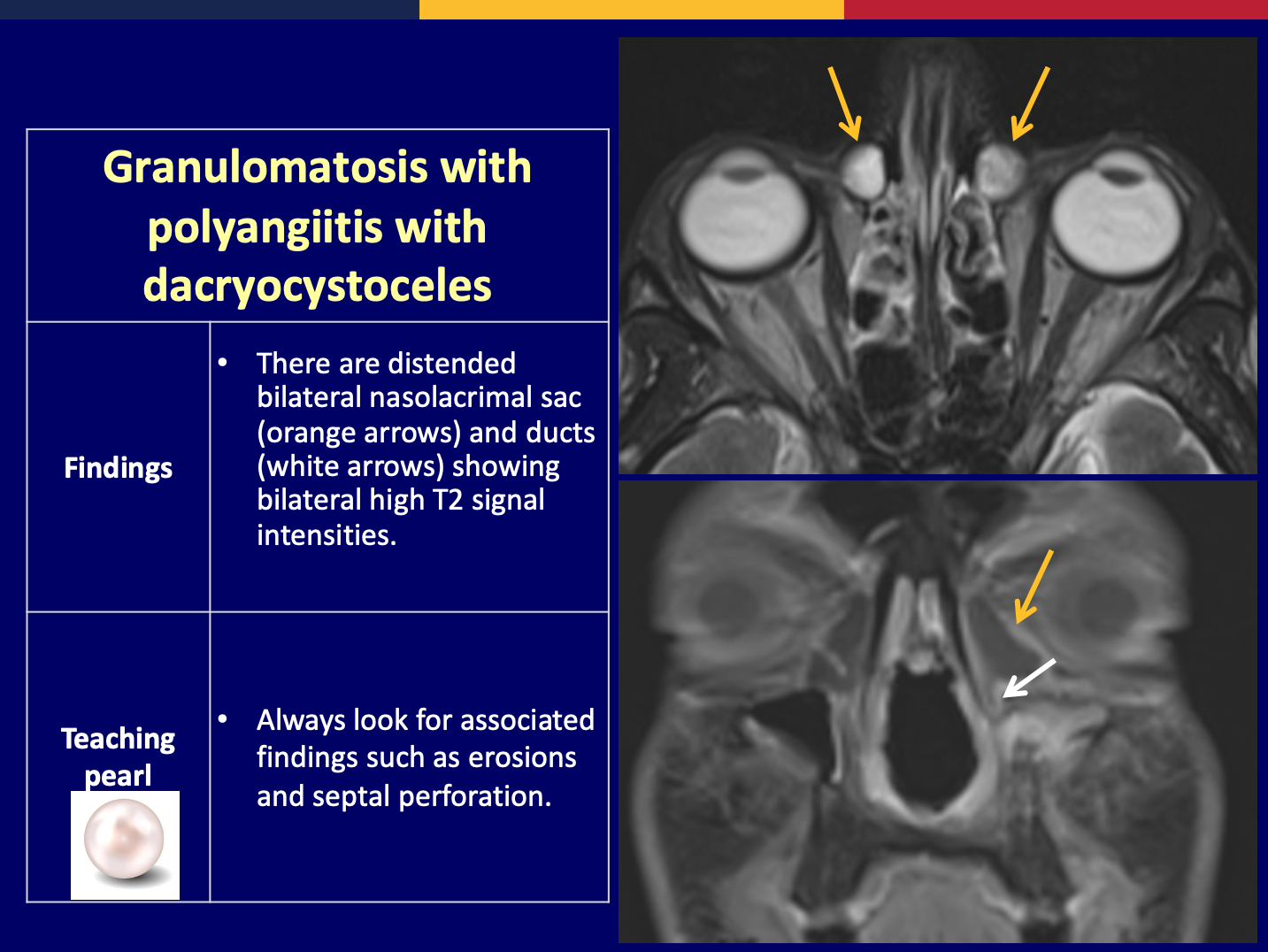
Conclusion:
•We reviewed the anatomy, physiology and common pathologies of nasolacrimal apparatus which are commonly overlooked.•The radiological features are non-specific, and correlation with clinical presentation and histopathology is recommended.
References:
- A comprehensive review of cross-sectional imaging of the nasolacrimal drainage apparatus: what radiologists need to know. 10.2214/AJR.19.21507.(1)
- Diagnostic imaging of the nasolacrimal drainage system. Part I. Radiological anatomy of lacrimal pathways. Physiology of tear secretion and tear outflow. 2014;20:628-638. (2)
- The forgotten lacrimal gland and lacrimal drainage apparatus: pictorial review of CT and MRI findings and differential diagnosis. 10.1259/BJR.20211333. (3)
Long-term outcomes of radiofrequency ablation for temporal lobe epilepsy

BACKGROUND
- Temporal lobe epilepsy (TLE) is the most common seizure disorder in adults, with mesial temporal sclerosis (MTS) being the most common etiology
- Anterior temporal lobectomy (ATL) is the gold standard treatment for TLE
- Radiofrequency ablation (RFA) is a minimally-invasive surgical procedure that has been used to treat TLE
- The long-term efficacy of RFA is not well-known and the techniques are not standardized
PROCEDURAL DETAILS
- All cases were done under neurolept sedation
- Lesions were planned with MRI to include the entire amygdala and the hippocampus
- Lesioning electrode was introduced via a lateral approach through a burr hole over the middle temporal gyrus
- Each lesion was made initially at 50-60oC for 60 s and then increased up to 85oC for 60 s
- Intraoperative scalp and intraventricular EEGs were monitored
OBJECTIVE
To determine long-term seizure outcomes and characteristics of patients who underwent RFA with a hope to guide future studies
METHODS
- Retrospective review of consecutive patients who underwent stereotactic RFA for TLE at our institution between 1994 and 2002
- Baseline demographics, procedural details, post-operative seizure outcomes, and information about additional treatments were collected
- Outcomes at last available follow-up were determined and seizure outcomes were classified based on Engel classifications
- Seizure-freedom after initial RFA treatment was estimated with Kaplan-Meier analysis
RESULTS
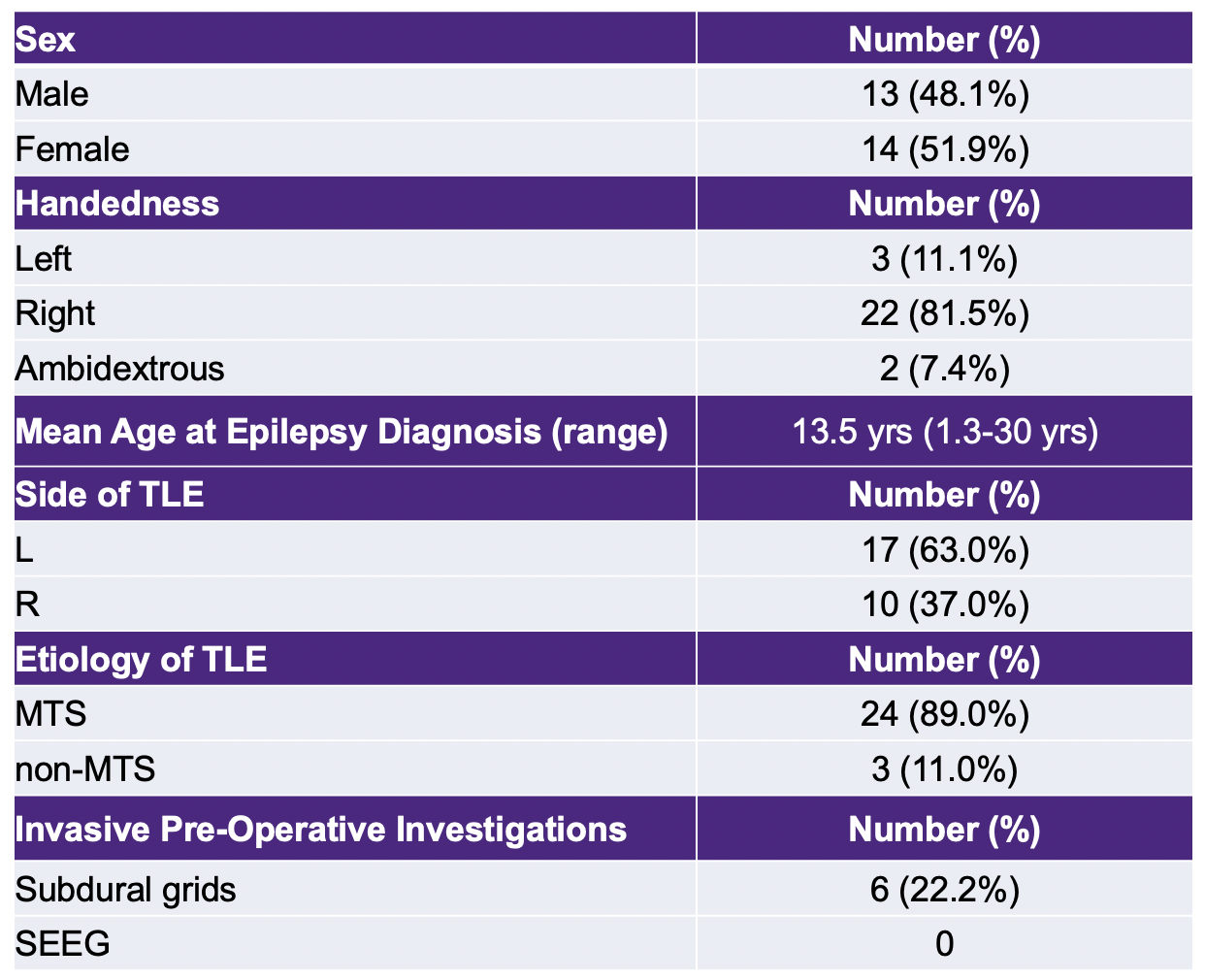
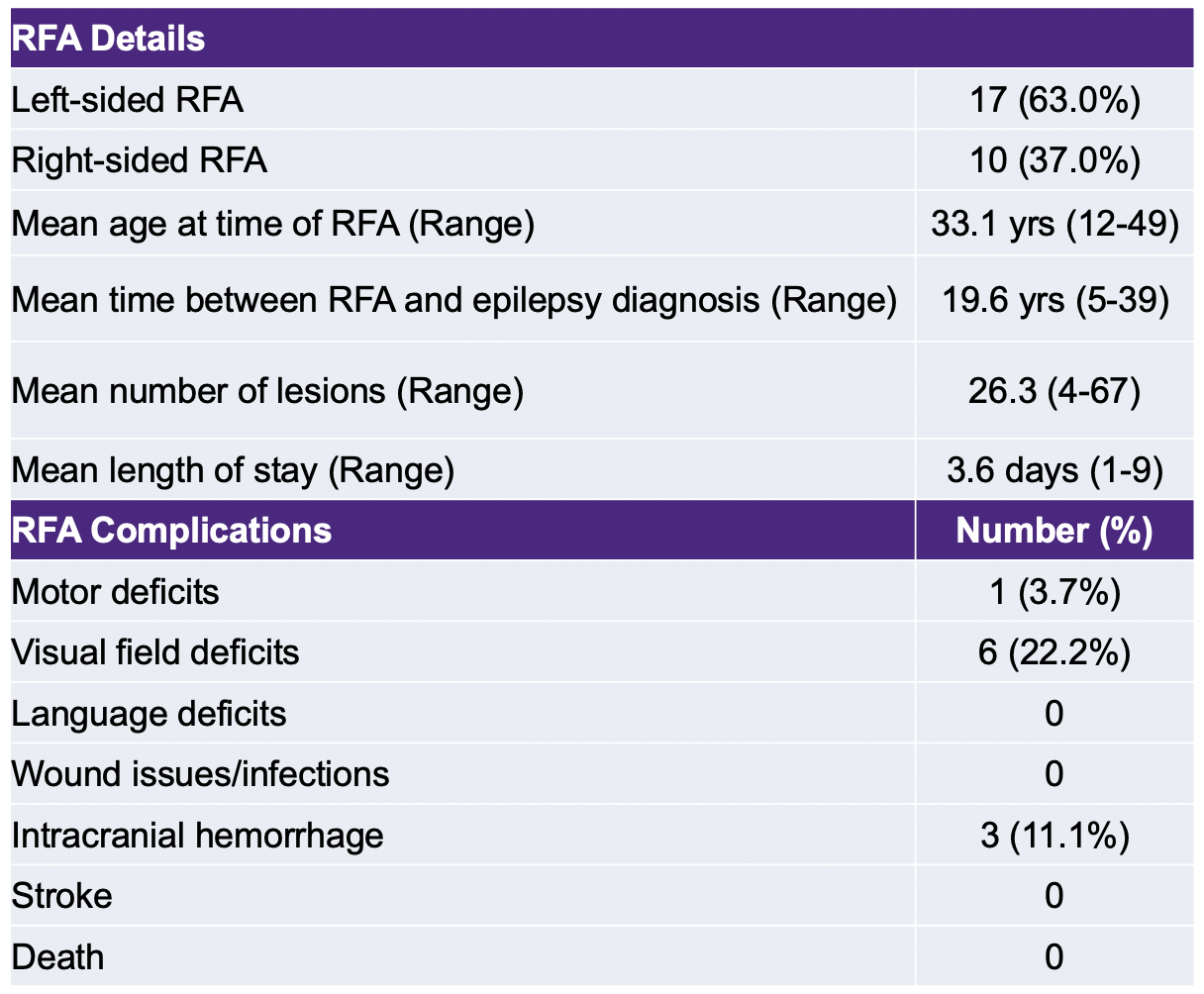
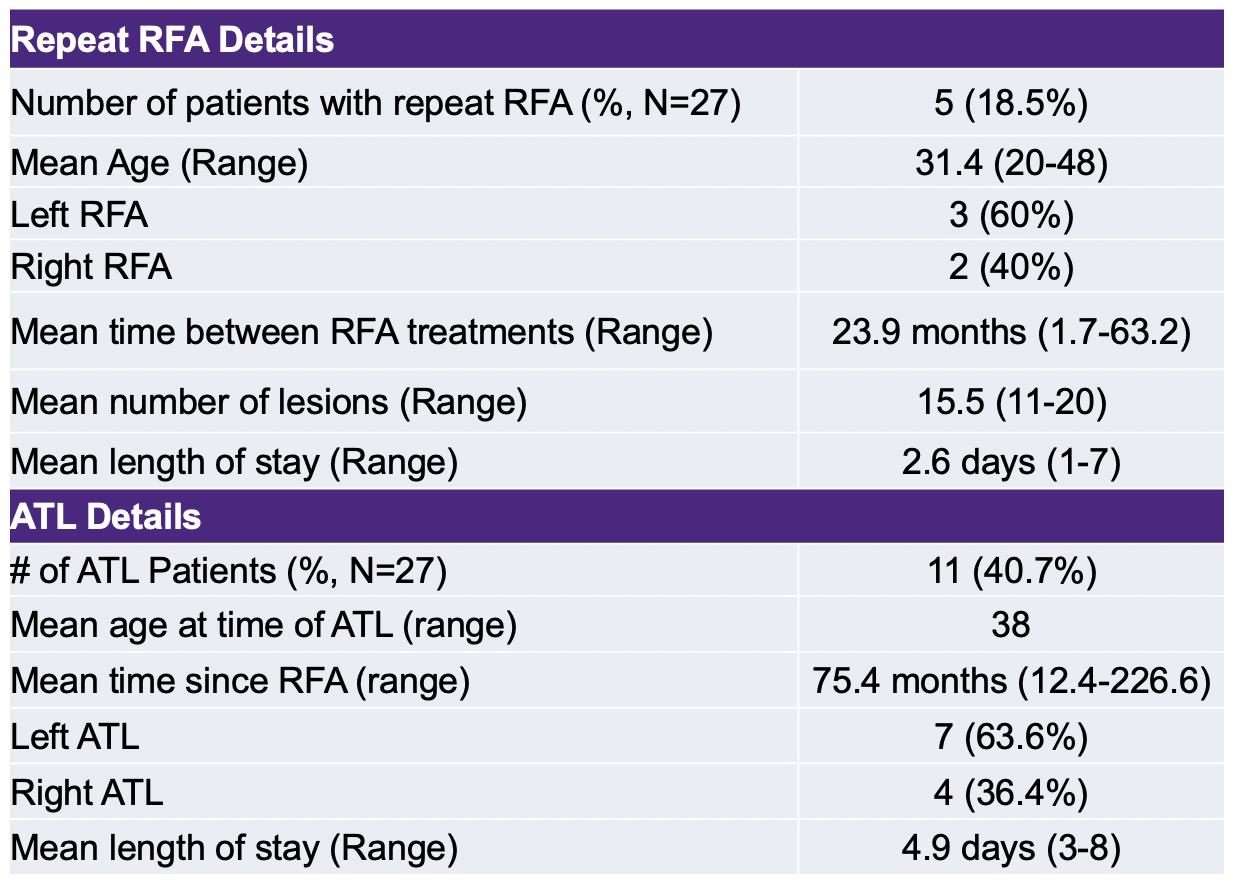
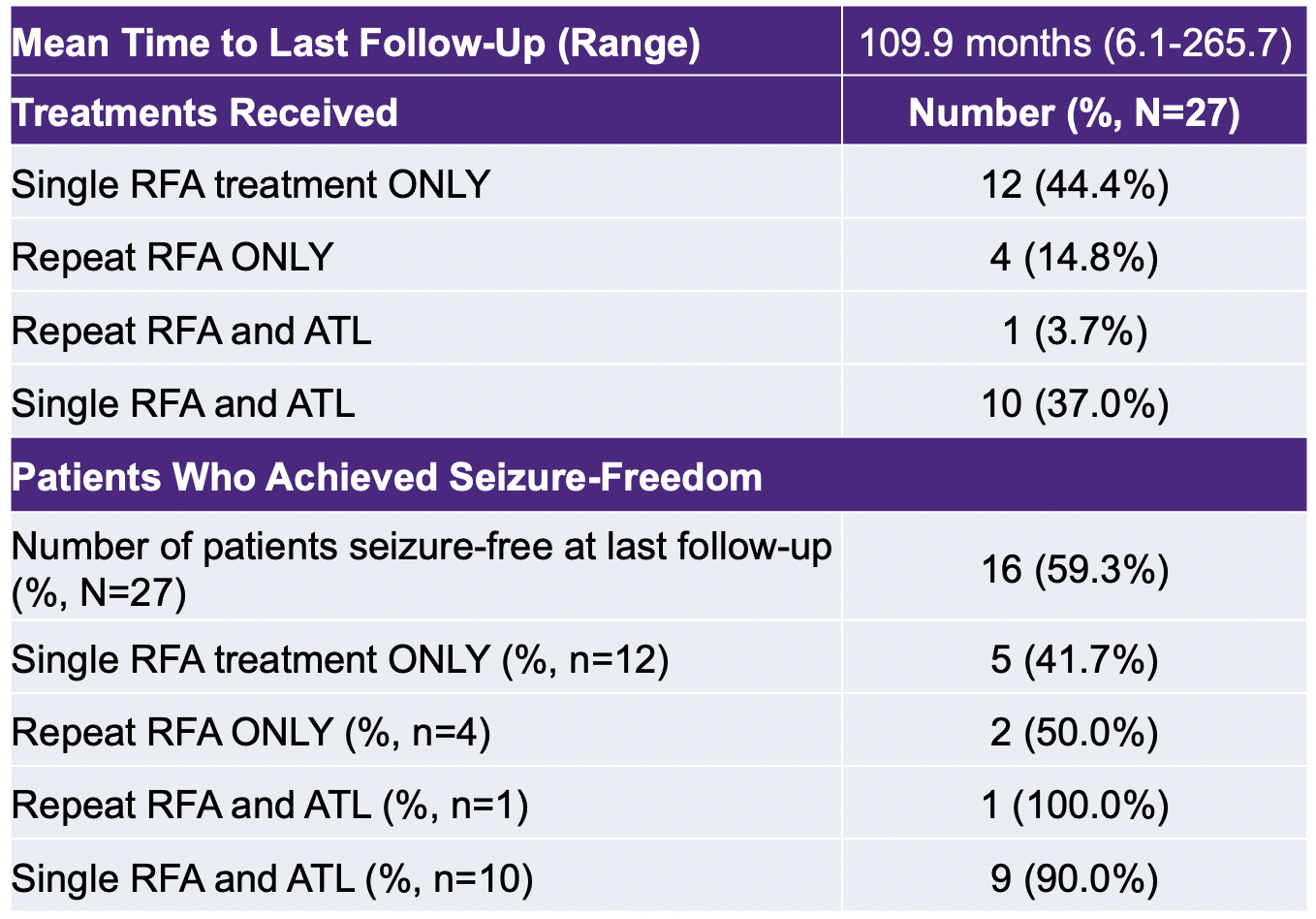
Table 1: Baseline patient characteristics. Table 2: RFA procedural details and complications.
Table 3: Details on repeat RFA procedures and ATL. Table 4: Outcomes at last follow-up.
Table 3: Details on repeat RFA procedures and ATL. Table 4: Outcomes at last follow-up.
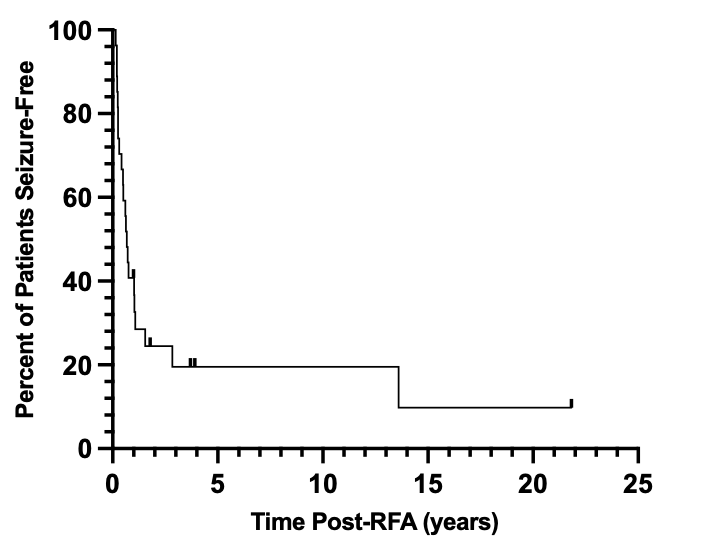
Figure 1: Kaplan-Meier analysis depicting the time to seizure recurrence after initial RFA.

Figure 2: Post-operative Engel Classification of seizure outcomes at last follow-up.
SUMMARY OF RESULTS
- 27 patients underwent RFA at our institution with 5 patients undergoing repeat RFA and 11 patients undergoing subsequent ATL
- At last follow-up (up to 22.1 years post-RFA), 5 (18.5%) patients who received a single RFA treatment, 2 (7.4%) patients who received a second RFA treatment, and 9 (33.3%) patients who underwent subsequent ATL were seizure-free
- The main complications associated with RFA were visual field deficits and small post-operative hematomas
CONCLUSIONS
- Based on this historical series, RFA is a minimally-invasive procedure that has a favourable safety profile and can provide a long-term improvement in seizures
- RFA could be used as an initial treatment before ATL
FUTURE DIRECTIONS
- Examine imaging characteristics of patients post-RFA
- Examine histopathological features of lobectomy samples
- Determine predictors of success for RFA
- Compare the efficacy of stereotactic RFA vs. SEEG-guided RFA
REFERENCES
- Parrent AG, Blume WT. Stereotactic amygdalohippocampotomy for the treatment of medial temporal lobe epilepsy. Epilepsia. 1999;40(10):1408-1416.
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A Randomized, Controlled Trial of Surgery for Temporal Lobe Epilepsy. The New England Journal of Medicine. 2001;345(5):311-318.
- Wang R, Beg U, Padmanaban V, et al. A Systematic Review of Minimally Invasive Procedures for Mesial Temporal Lobe Epilepsy: Too Minimal, Too Fast? Neurosurgery. 2021;89(2):164-176.
- Bourdillon P, Cucherat M, Isnard J, et al. Stereo-electroencephalography-guided radiofrequency thermocoagulation in patients with focal epilepsy: A systematic review and meta-analysis. Epilepsia. 2018;59(12):2296-2304.
- Vojtěch Z, Malíková H, Krámská L, Liščák R, Vladyka V. MRI-guided stereotactic amygdalohippocampectomy: A single center experience. Neuropsychiatric Disease and Treatment. 2015;11:359-374.
ACKNOWLEDGEMENTS
The authors would like to thank the Department of Clinical Neurological Sciences, London Health Sciences Centre, and Western University for their ongoing support. There are no conflicts of interest to disclose.
Relationships Between Anatomical Features and Outcome after Stereotactic Laser Amygdalohippocampotomy

Introduction
- Temporal lobe epilepsy (TLE) is the most common adult form of epilepsy, and Mesial Temporal Sclerosis (MTS) is its most common subtype.
- Stereotactic laser amygdalohippocampotomy (SLAH) is a novel procedure which has recently been shown to be comparable in effectiveness in the treatment of TLE to a traditional temporal lobectomy procedure1.
- Volume of SLAH ablation has previosuly been found to correlate with functional outcome2.
- The lateral mesencephalic sulcus (LMS) is a landmark that is frequently used during SLAH procedures.
- Optimal operative ablation location and extent is uncertain, as are the neuroanatomical features guiding successful ablations.
- Stereotactic laser amygdalohippocampotomy (SLAH) is a novel procedure which has recently been shown to be comparable in effectiveness in the treatment of TLE to a traditional temporal lobectomy procedure1.
- Volume of SLAH ablation has previosuly been found to correlate with functional outcome2.
- The lateral mesencephalic sulcus (LMS) is a landmark that is frequently used during SLAH procedures.
- Optimal operative ablation location and extent is uncertain, as are the neuroanatomical features guiding successful ablations.
Purpose
Identify anatomical features from pre-operative clinical T1w MRI scans of MTS patients which are associated with either post-opertative seizure freedom (Engel 1) or poor surgical outcome (Engel 2-4).
Methods
Data: T1 MRI scans pre and post surgery of patients treated with SLAH for MTS at Emory University between 2011 and 2019 (N=65)
- Manual segmentations of ablation regions using ITK-SNAP (3.8.0)
- Ablations were assessed in relation to:
1) Total volume
2) Whether crossed the coronal plane of the LMS3
3) Extent past the LMS
- Patients were analyzed with reference to their categorization on 12-month Engel classification score.
- Wilcoxon ranked-sign test was performed for each variable of interest between groups of patients with Engel score 1 versus Engel score 2-4.
- On a curated subset of 18 patients 32 anatomical fiducials were manually placed on MRI scans as per a previously validated protocol3.
- Anatomical fiducials were additionally placed on the same 18 patients subset and an additional 18 patient subset via an automated novel machine learning program.
- The anterior, posterior, medial, lateral, superior, and inferior extents of ablations were analyzed through pair-wise correlation with AFIDS placed on patient pre-operative scans.
Data: T1 MRI scans pre and post surgery of patients treated with SLAH for MTS at Emory University between 2011 and 2019 (N=65)
- Manual segmentations of ablation regions using ITK-SNAP (3.8.0)
- Ablations were assessed in relation to:
1) Total volume
2) Whether crossed the coronal plane of the LMS3
3) Extent past the LMS
- Patients were analyzed with reference to their categorization on 12-month Engel classification score.
- Wilcoxon ranked-sign test was performed for each variable of interest between groups of patients with Engel score 1 versus Engel score 2-4.
- On a curated subset of 18 patients 32 anatomical fiducials were manually placed on MRI scans as per a previously validated protocol3.
- Anatomical fiducials were additionally placed on the same 18 patients subset and an additional 18 patient subset via an automated novel machine learning program.
- The anterior, posterior, medial, lateral, superior, and inferior extents of ablations were analyzed through pair-wise correlation with AFIDS placed on patient pre-operative scans.
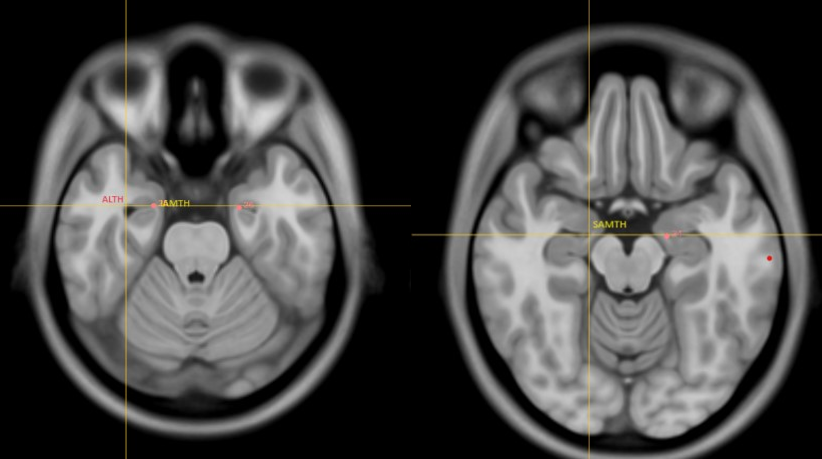
Fig 1. Anterior temporal horn fidicuals analyzed, ALTH (Anterior Lateral Temporal Horn), IAMTH (Inferior Anterior Medial Temporal Horn), SAMTH (Superior Anterior Medial Temporal Horn)
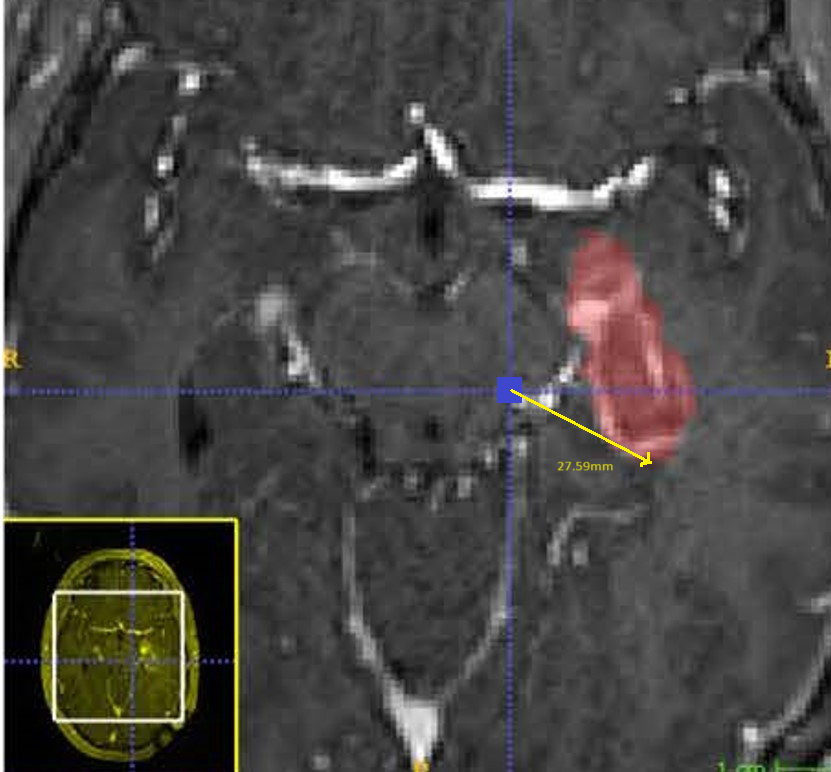
Fig 2. T1w MRI of post SLAH-patient and segmentation of SLAH lesion. Example of pairwise analysis of anatomical fiducials with parameters of ablation (e.g. shown here - Inferior Lateral Mesencephalic Sulcus with posterior extent of ablation)
Results
Volume of ablation
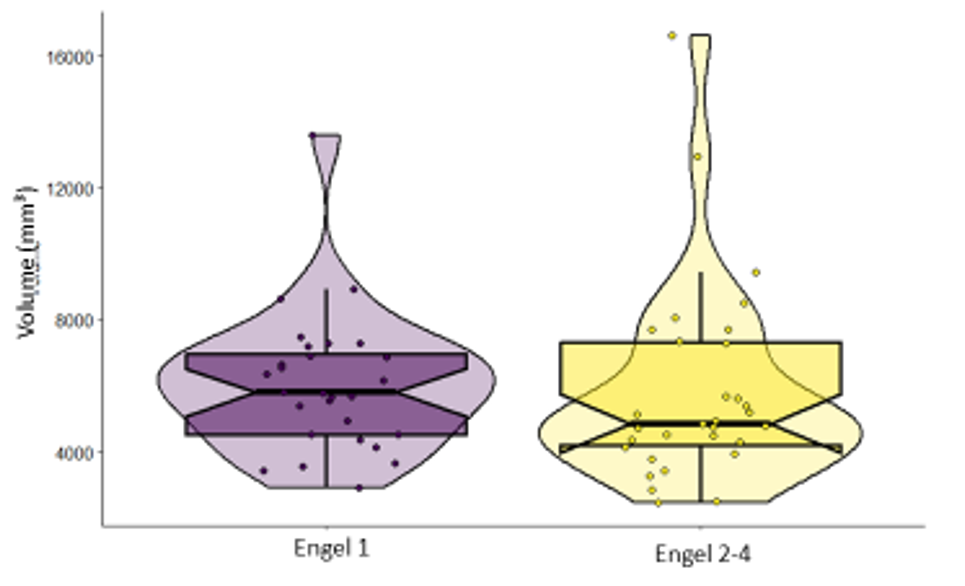
Distance posterior to the Lateral Mesencephalic Junction
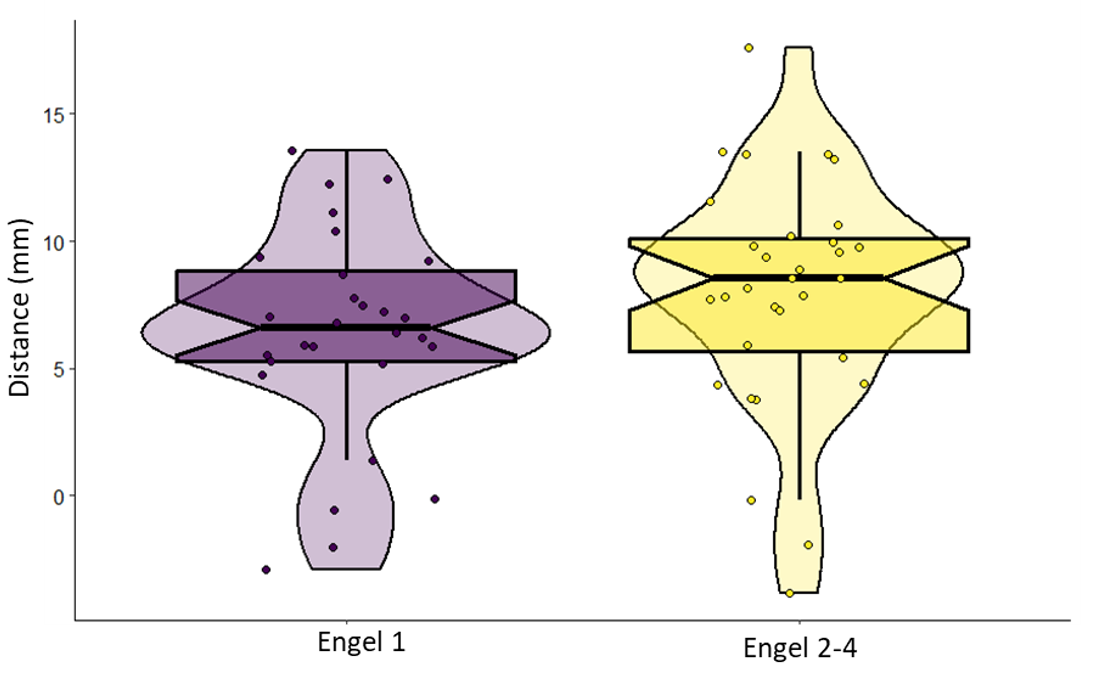
Fig 3. A) comparison of ablation volumes in mm3 between patient outcome groups. B) comparison of the absolute average distance of ablations from the LMS (mm). Distance was calculated manually, and was defined by the length of the most posterior extent of the ablation from the LMS
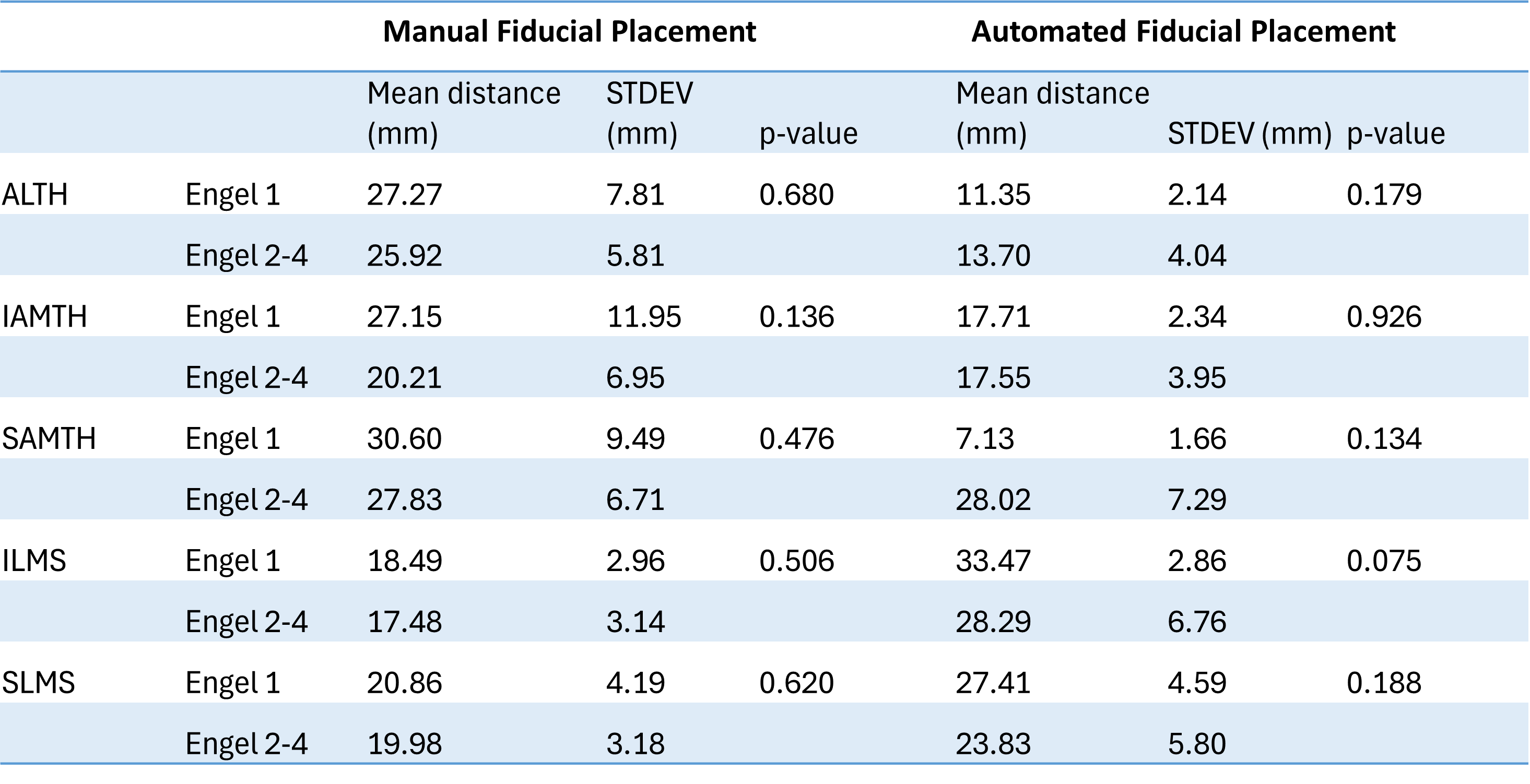
Table 1. Pairwise distances between anatomical fiducials and posterior extent of ablation. ALTH (Anterior Lateral Temporal Horn), IAMTH (Inferior Anterior Medial Temporal Horn), SAMTH (Superior Anterior Medial Temporal Horn), SLMS (Superior Lateral Mesencephalic Sulcus), ILMS (Inferior Lateral Mesencephalic Sulcus)
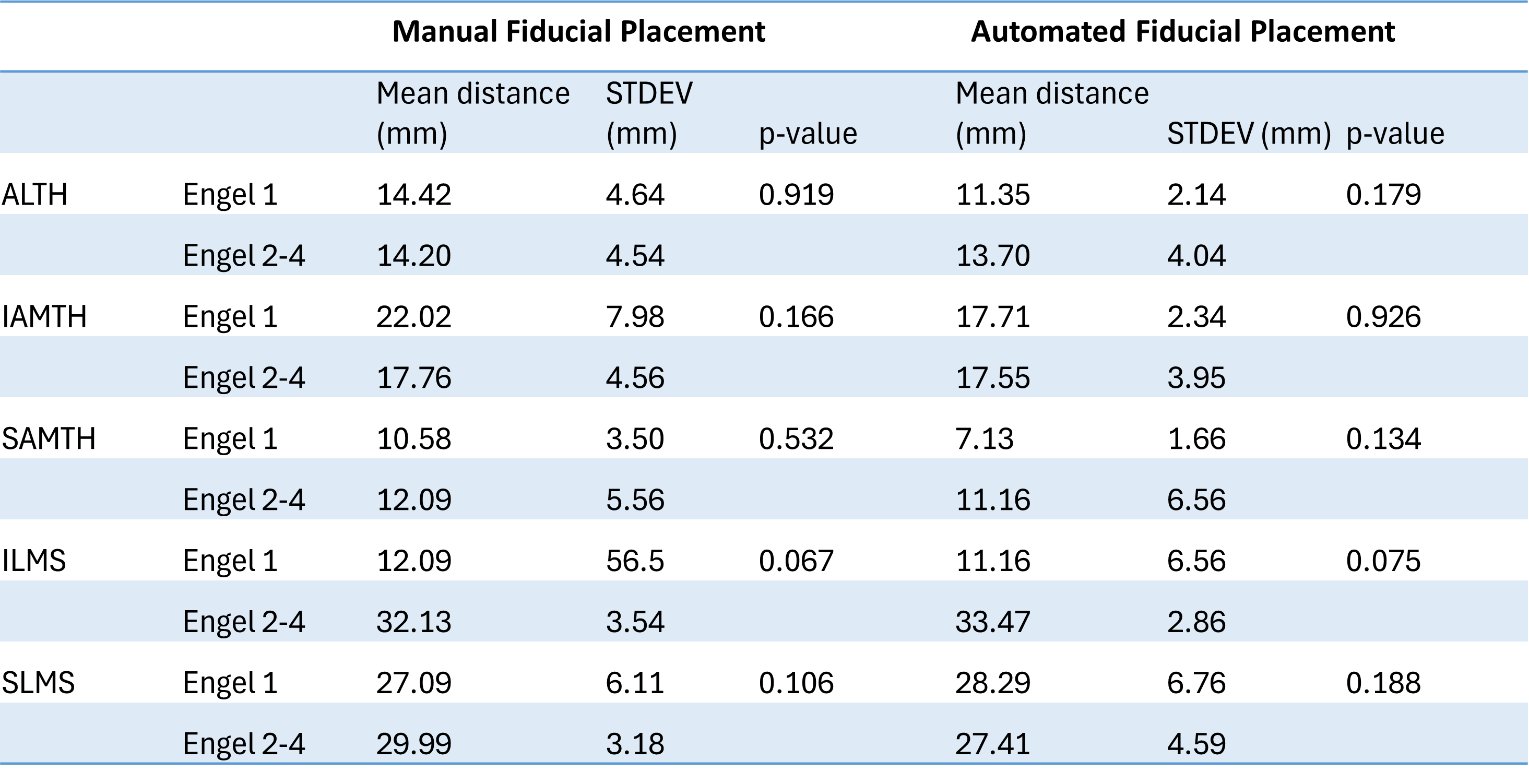
Table 2. Pairwise distances between anatomical fiducials and inferior extent of ablation
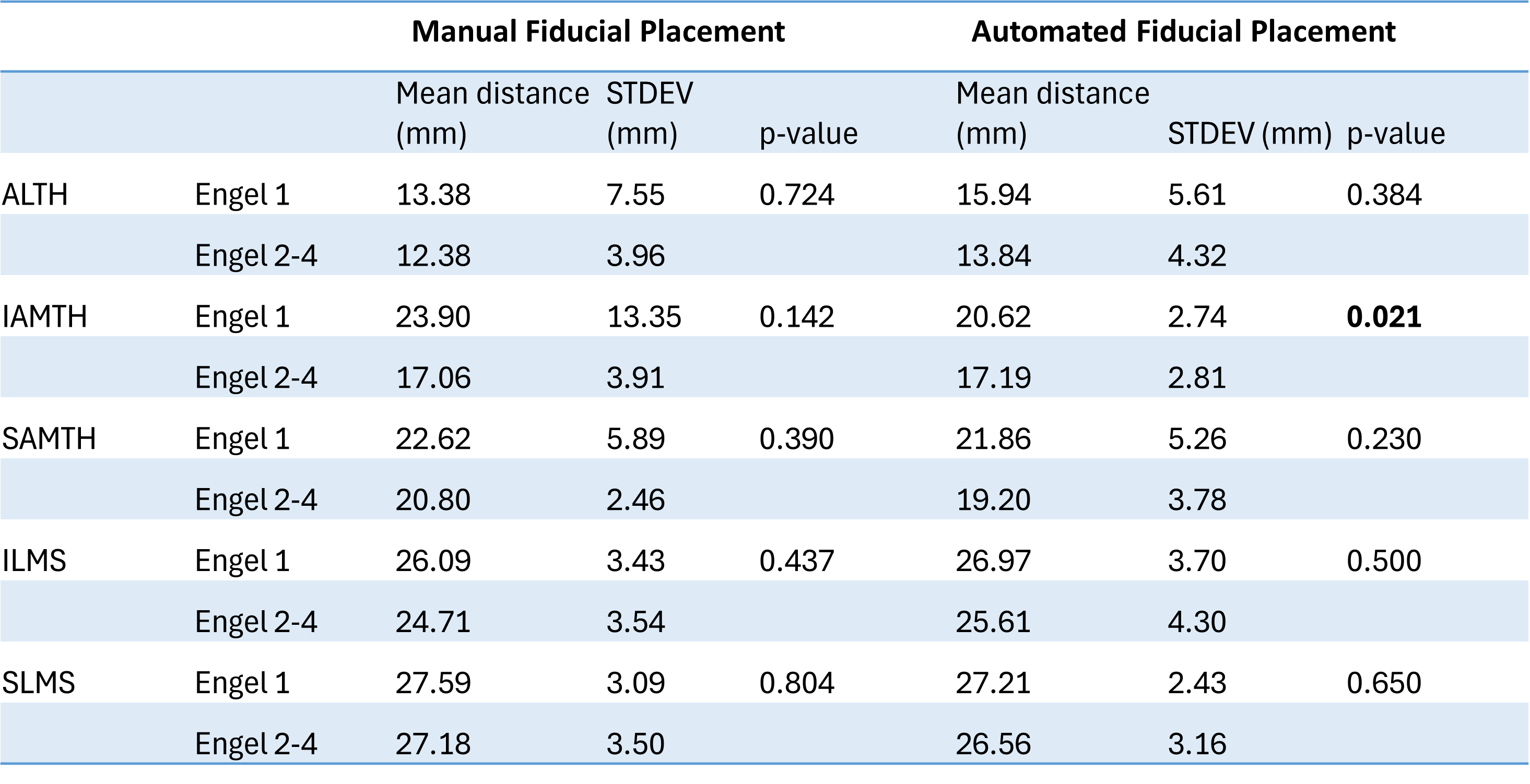
Table 3. Pairwise distances between anatomical fiducials and lateral extent of ablation
Conclusions
•Distance of ablation posterior to the coronal plane of the LMS was not significantly associated with 12-month seizure freedom rates.
•Distance of ablation posterior to the coronal plane of the LMS was not significantly associated with 12-month seizure freedom rates.
•Volume of ablation was not significantly associated with 12-month seizure freedom rates.
•Anatomical feature results are contrary to currently used practices in SLAH and highlight the use of anatomical landmarks in surgical planning.
•An automated (machine learning) fiducial placement program can accurately identify anatomical features of pre-surgical MRI scans predictive of post-operative seizure freedom. In the future, this could consit of paramaters of the anterior hippocampal region predictive of good surgical outcome and/or charactestics of the poserior hippocamal region predicitive of poor surgical outcome.
•In combination with neuroimaging modalities such as diffusion MRI, this approach could be used to better understand the optimal extent of SLAH ablations for functional outcome and potential surgical adverse consequences.
Conact
czajner@uwo.ca
Please contact for references
Conact
czajner@uwo.ca
Please contact for references
Subgaleal versus subdural drain after minicraniotomy for chronic subdural haematoma
BACKGROUND
Surgical evacuation with placement of a postoperative drain is the standard treatment for symptomatic chronic subdural haematoma (cSDH). Subdural and subgaleal drains are equally effective after burrhole craniostomy, but the optimal location of the drain after craniotomy is not clear.1, 2 We sought to compare the clinical and radiological outcomes of subdural and subgaleal drain placement in patients undergoing minicraniotomy for cSDH.
METHODS
A single-centre retrospective review of all patients who underwent minicraniotomy and drain insertion for cSDH in Melbourne, Australia, from 2019 to 2023. Patients were excluded if they: were <18 years of age, had a history or suspicion of intracranial hypotension, or had a cerebrospinal fluid (CSF) diversion device (e.g. ventriculoperitoneal shunt).
Patient characteristics assessed included the use of anticoagulants or antiplatelets, preoperative neurological status (Glasgow Coma Scale), premorbid functional status (Modified Rankin Score, mRS), focal neurological deficits and surgical technique including location of drain. Outcome measures included recurrence, functional status (mRS), mortality and discharge destination. Adverse events and complications that occurred were recorded.
Patient characteristics assessed included the use of anticoagulants or antiplatelets, preoperative neurological status (Glasgow Coma Scale), premorbid functional status (Modified Rankin Score, mRS), focal neurological deficits and surgical technique including location of drain. Outcome measures included recurrence, functional status (mRS), mortality and discharge destination. Adverse events and complications that occurred were recorded.
SURGICAL TECHNIQUE
At our institution surgical technique and drainage type are contingent on consultant surgeon preference. Drains were used in all patients undergoing minicraniotomy during this period. Sagittal incision along the superior temporal line (Figure 1).Elliptical craniotomy with the burrhole anteriorly. After linear durotomy and standard drainage of the cSDH, the dura was apposed and the dura at the burrhole coagulated back to keep it patent. The innermost layer (membrane) of the cSDH is not opened to obviate CSF egress or hygroma. Onlay Tachosil ®(Baxter) was placed over the durotomy, however the burrhole area was left patent, providing a pathway of efflux between the subdural and subgaleal space. A flat-white Jackson-Pratt (7 or 10 Fr) drain was placed over the burrhole cover in the subgaleal space and placed on thumb-print suction. Prior to the final galeal suture the cavity is filled with wash. Patients with subgaleal drains had no mobility restrictions.
At our institution surgical technique and drainage type are contingent on consultant surgeon preference. Drains were used in all patients undergoing minicraniotomy during this period. Sagittal incision along the superior temporal line (Figure 1).Elliptical craniotomy with the burrhole anteriorly. After linear durotomy and standard drainage of the cSDH, the dura was apposed and the dura at the burrhole coagulated back to keep it patent. The innermost layer (membrane) of the cSDH is not opened to obviate CSF egress or hygroma. Onlay Tachosil ®(Baxter) was placed over the durotomy, however the burrhole area was left patent, providing a pathway of efflux between the subdural and subgaleal space. A flat-white Jackson-Pratt (7 or 10 Fr) drain was placed over the burrhole cover in the subgaleal space and placed on thumb-print suction. Prior to the final galeal suture the cavity is filled with wash. Patients with subgaleal drains had no mobility restrictions.
Figure 1.
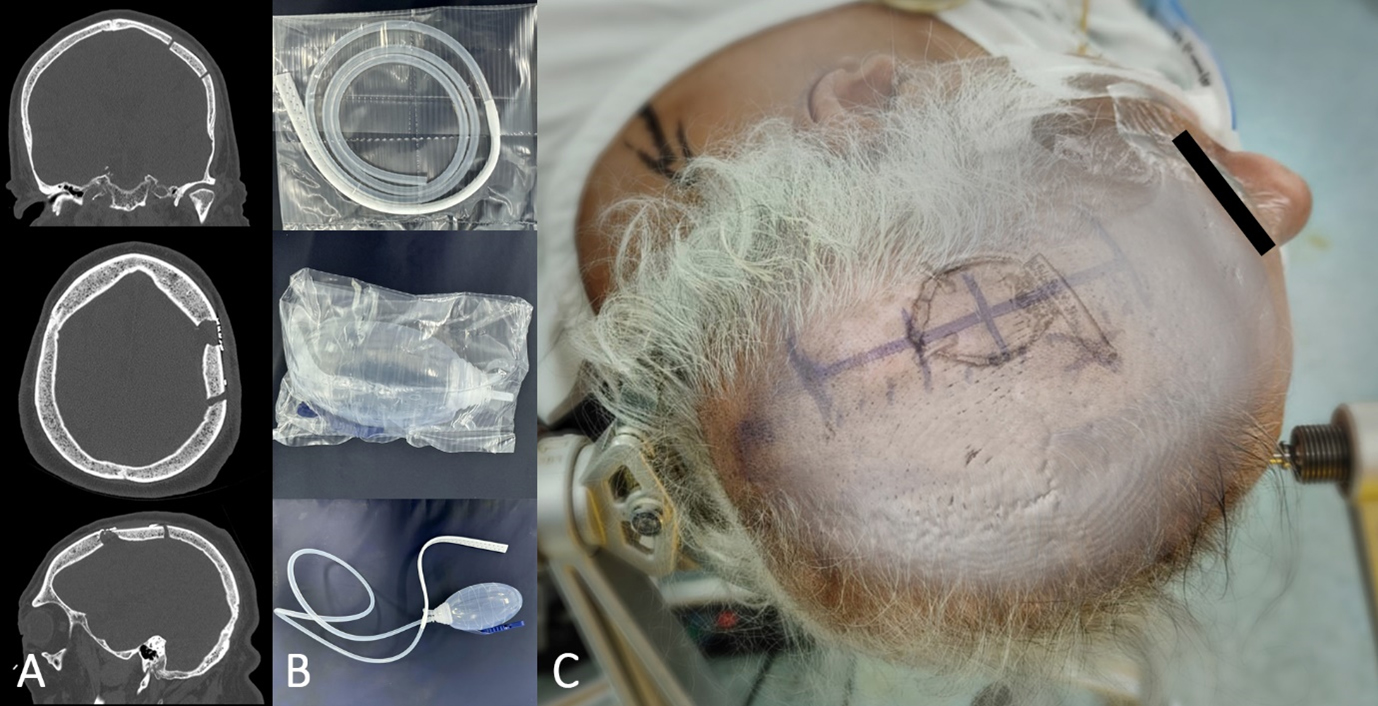
Example of craniotomy, antero-posterior incision, and placement of subgaleal drain
RESULTS
A total of 137 patients were included for analysis. Premorbid functional status was worse in patients undergoing subgaleal drainage (p<0.001), otherwise there were no significant differences between groups preoperatively 137 (Table 1). All patients were followed for at least 3 months (median 105 days).
Discharge
The majority of patients (62.8%) were discharged to their homes, 79.4% (27/34) in the subgaleal group and 57.3% (59/103) in the subdural group (p=0.02) (Table 2).
mRS
At discharge, the subgaleal group had a mean (±sd) improvement of 0.56±1.2 points, while the subdural group had a deterioration of 0.96±1.3 points (p<0.01) (Figure 2).
Recurrence and LOS
Although recurrence was more prevalent in the subdural group (13.6%; 14/103) than the subgaleal group (2.9%; 1/34), this difference did not achieve statistical significance (p=0.12). Mean length of admission was on average over 2 days shorter in the subgaleal group (7.14±5 vs 9.97±9 days, p=0.01).
Discharge
The majority of patients (62.8%) were discharged to their homes, 79.4% (27/34) in the subgaleal group and 57.3% (59/103) in the subdural group (p=0.02) (Table 2).
mRS
At discharge, the subgaleal group had a mean (±sd) improvement of 0.56±1.2 points, while the subdural group had a deterioration of 0.96±1.3 points (p<0.01) (Figure 2).
Recurrence and LOS
Although recurrence was more prevalent in the subdural group (13.6%; 14/103) than the subgaleal group (2.9%; 1/34), this difference did not achieve statistical significance (p=0.12). Mean length of admission was on average over 2 days shorter in the subgaleal group (7.14±5 vs 9.97±9 days, p=0.01).
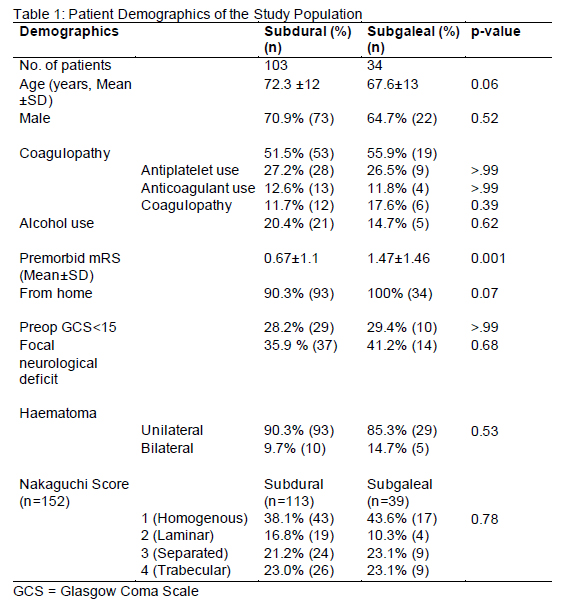
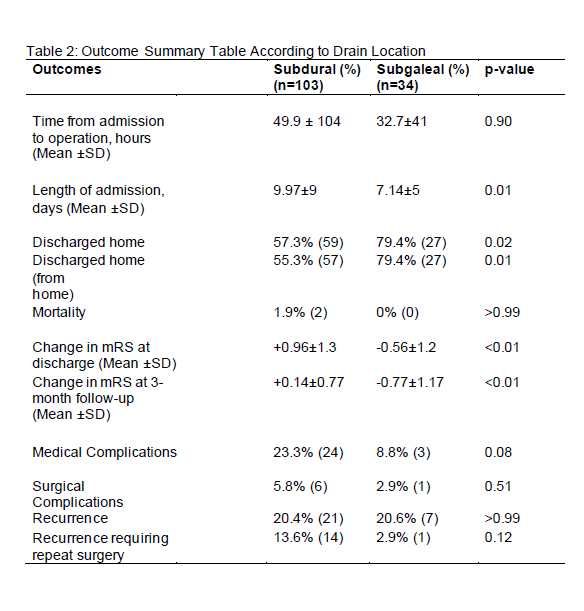
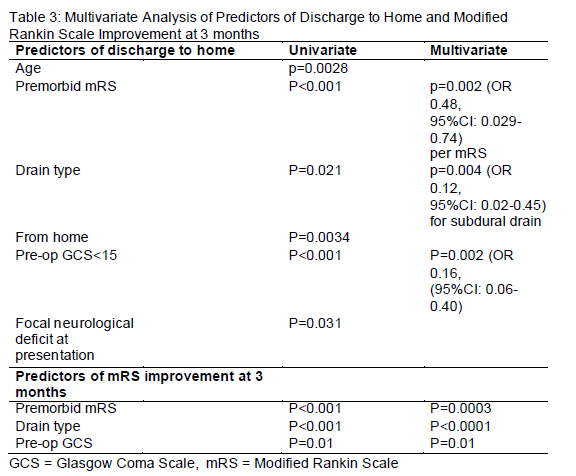
DISCUSSION AND CONCLUSION
In patients undergoing minicraniotomy for cSDH, subgaleal drains were associated with shorter hospitalisation, greater chance of discharge home, and greater improvement in functional status at 3-month postoperative period. Our study is the first to present these findings and describe the operative technique for effective use of subgaleal drains after minicraniotomy for cSDH.
Although retrospective, no clear selection bias was evident in any of the common cSDH surgical characteristics, including age, coagulopathy, unilateral vs bilateral, and Nakaguchi grade, although patients were more disabled preoperatively in the subgaleal drainage group.
Given subgaleal drains were associated with shorter hospitalisation, greater chance of discharge home, and better functional outcomes than subdural drains we propose this to be the future standard of care.
Although retrospective, no clear selection bias was evident in any of the common cSDH surgical characteristics, including age, coagulopathy, unilateral vs bilateral, and Nakaguchi grade, although patients were more disabled preoperatively in the subgaleal drainage group.
Given subgaleal drains were associated with shorter hospitalisation, greater chance of discharge home, and better functional outcomes than subdural drains we propose this to be the future standard of care.
REFERENCES
1. Santarius T, Kirkpatrick PJ, Ganesan D, et al. Use of drains versus no drains after burrhole evacuation of chronic subdural haematoma: a randomised controlled trial. Lancet 2009;374(9695):1067-73.
2. Soleman J, Lutz K, Schaedelin S, et al. Subperiosteal vs Subdural Drain After Burr-Hole Drainage of Chronic Subdural Hematoma: A Randomized Clinical Trial (cSDH-Drain-Trial). Neurosurgery. 2019;85(5):E825-E834.
2. Soleman J, Lutz K, Schaedelin S, et al. Subperiosteal vs Subdural Drain After Burr-Hole Drainage of Chronic Subdural Hematoma: A Randomized Clinical Trial (cSDH-Drain-Trial). Neurosurgery. 2019;85(5):E825-E834.
Hearing preservation and quality of life outcomes in partial labyrinthectomy petrous apicectomy for microsurgical resection of large posterior fossa skullbase tumors
BACKGROUND
The Partial Labyrinthectomy Petrous Apicectomy (PLPA) is a skullbase approach often used for large posterior fossa skullbase tumors such as petroclival meningiomas originating or extending anterior to the internal auditory meatus and above the tentorium.1, 2, 3, 4 Historically such lesions have been known for their challenging planes and high neurological and perioperative morbidity. The approach aims to give transpetrosal access whilst preserving hearing.2 Despite its acceptance and uptake, there are few studies that assess rates of microsurgical resection and morbidity, and no large studies that document its ability to preserve hearing in the setting of large skullbase tumors. Additionally, the effect of surgical resection on long-term quality of life in the context of hearing loss, either before or after surgery is unknown. Because of this we present the first large series with long-term follow up assessing the utility of the PLPA approach with intraoperative neuromonitoring on preserving hearing and quality of life whilst achieving tumor controlMETHODS
RESULTS
Of 73 PLPA surgeries identified, comprehensive data was available for 56 patients undergoing 57 PLPAs, the majority of which were for petroclival meningioma (57.8%), epidermoid tumors (21.0%) or cerebellopontine schwannoma (10.5%). The mean age and tumor diameter sizes were 51.6 years and 44mm respectively.
Gross total resection was achieved in 23 (40.3%), near total resection in 9 (15.8%) and subtotal resection in 25 (43.8%) cases. There was no perioperative mortality.
Preoperative hearing was present in 39 patients of which 27 (69.2%) were preserved, 10 (25.6%) were lost and outcome for 2 were unknown.
Attempted hearing preservation was not associated with decreased rates of resection (p-value 0.183). Preservation of brainstem auditory evoked responses (BAER) was associated with preserved hearing.
Gross total resection was achieved in 23 (40.3%), near total resection in 9 (15.8%) and subtotal resection in 25 (43.8%) cases. There was no perioperative mortality.
Preoperative hearing was present in 39 patients of which 27 (69.2%) were preserved, 10 (25.6%) were lost and outcome for 2 were unknown.
Attempted hearing preservation was not associated with decreased rates of resection (p-value 0.183). Preservation of brainstem auditory evoked responses (BAER) was associated with preserved hearing.
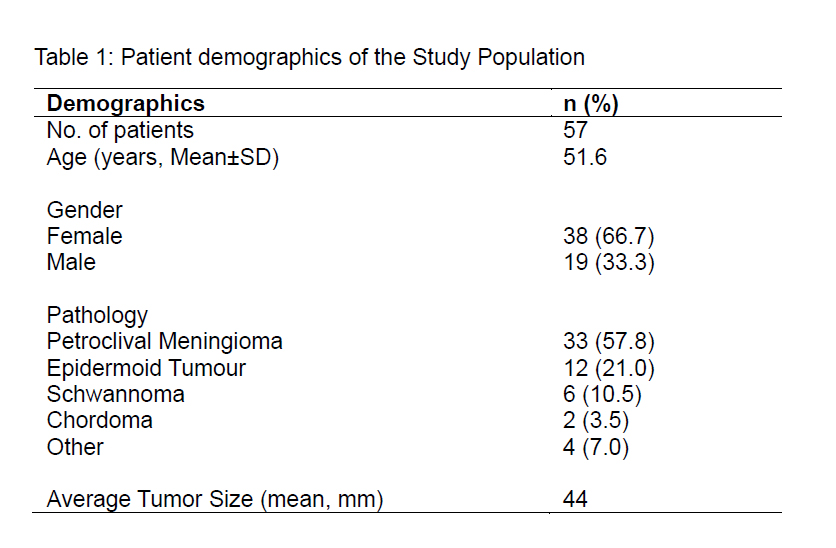
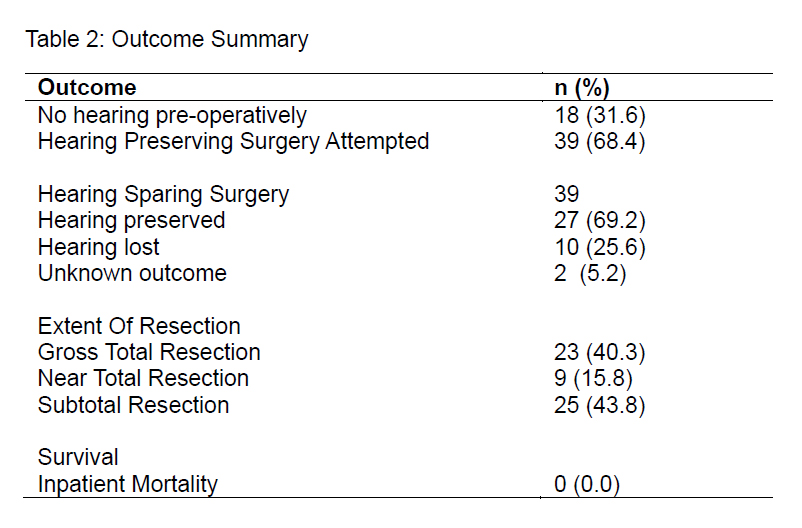
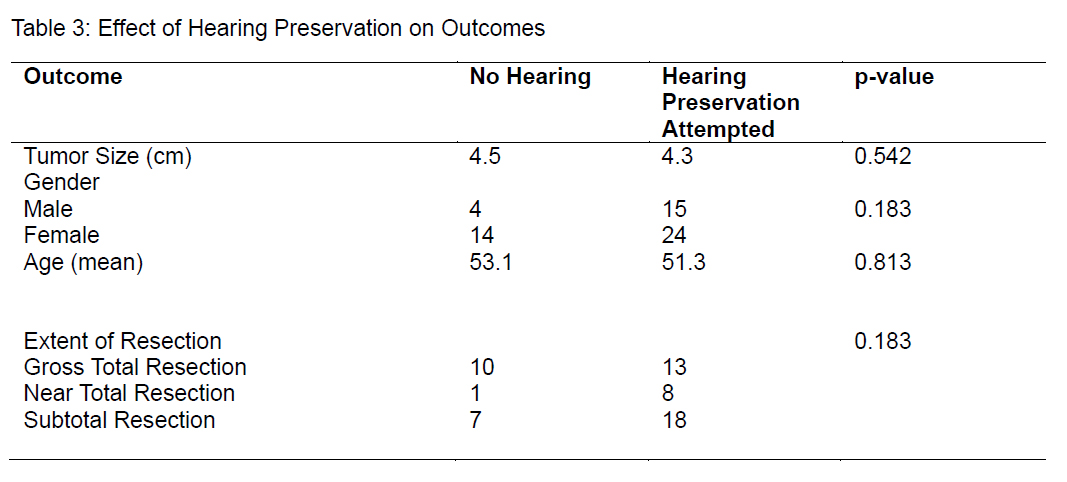
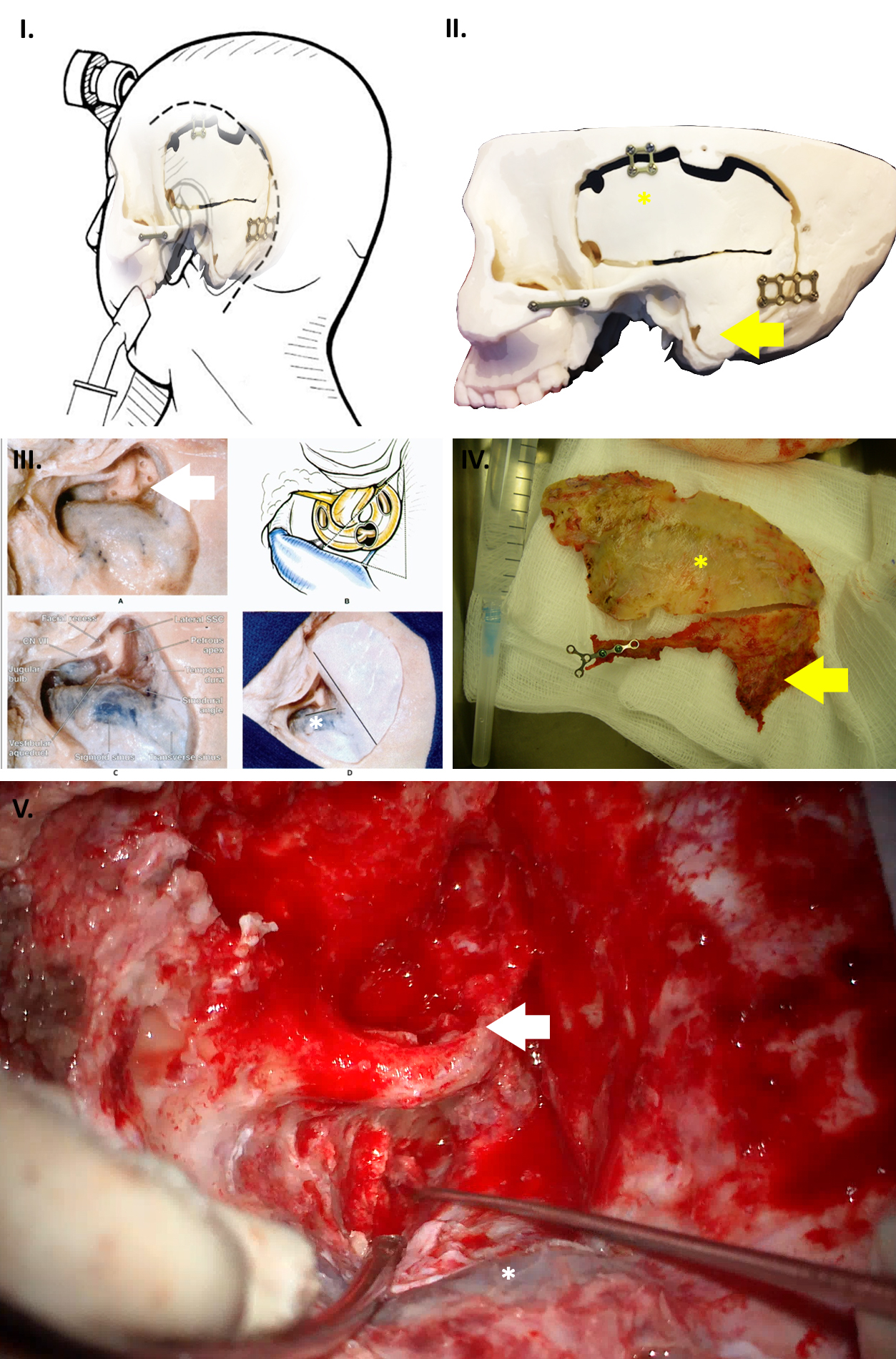
Multiple panels demonstrating the Partial Labyrinthine Petrous Apicectomy Approach: Overlay, skull model and intraoperative photo demonstrating positioning, incision, and temporal craniotomy(yellow *) along with cosmetic zygomatico-mastoid osteotomy(yellow arrow) that can be replaced for reconstruction. Cadaver, schematic and intraoperative microscope photograph demonstrating presigmoid (*) approach to reach lesions infront of the internal auditory meatus, with mastoid drilling and preservation of the hearing apparatus (white arrow)
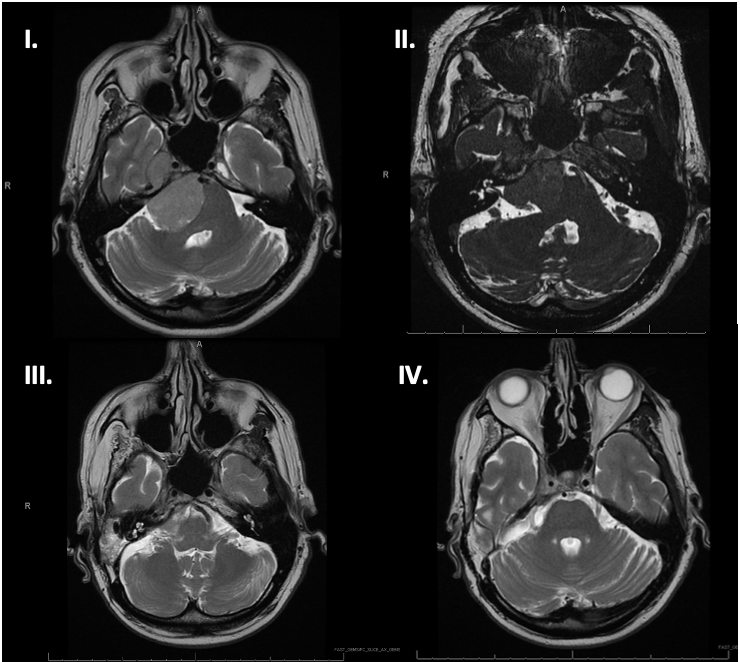
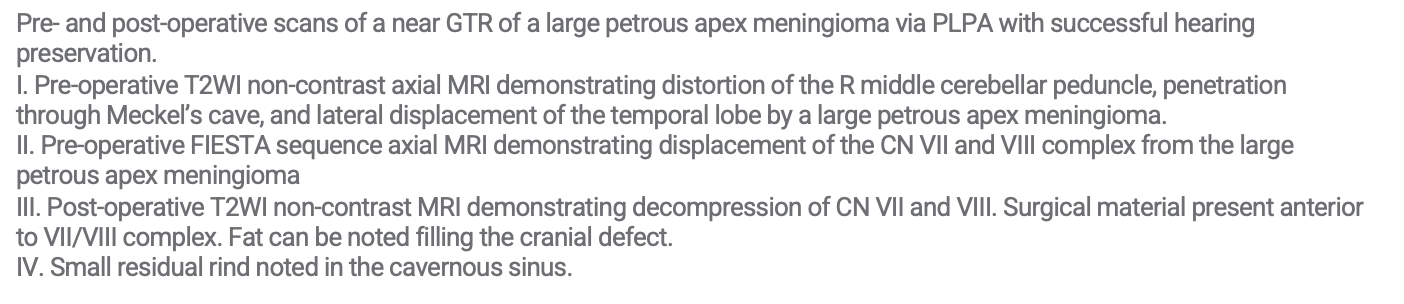
DISCUSSION AND CONCLUSION
Large improvements in modern microsurgical technique and intraoperative neuromonitoring when utilising the PLPA approach have resulted in far lower perioperative mortality and morbidity compared to historical cohorts whilst achieving a high rate of combined tumor resection, hearing preservation and maintaining quality of life.
REFERENCES
1. Hirsch BE, Cass SP, Sekhar LN, Wright DC. Translabyrinthine approach to skull base tumors with hearing preservation. American Journal of Otolaryngology. 1993;14(6):533-43.
2. Sekha LN, Schessel DA, Bucur SD, Raso JL, Wright DC. Partial labyrinthectomy petrous apicectomy approach to neoplastic and vascular lesions of the Petroclival Area. Neurosurgery. 1999;44(3):537-550. doi:10.1097/00006123-199903000-00060
3. Seifert V, Raabe A, Zimmermann M. Conservative (labyrinth-preserving) transpetrosal approach to the Clivus and petroclival region ? indications, complications, results and lessons learned. Acta Neurochirurgica. 2003;145(8):631-642. doi:10.1007/s00701-003-0086-2
4. Xu F, Karampelas I, Megerian CA, Selman WR, Bambakidis NC. Petroclival meningiomas: An update on surgical approaches, decision making, and treatment results. Neurosurgical Focus. 2013;35(6). doi:10.3171/2013.9.focus13319
Chordoma Management with Artificial Intelligence: A Scoping Review of Current Applications and Future Prospects

Background
Chordomas are rare malignant bone tumours with complex location & propensity for recurrence, making diagnosis & prognosis difficult.1∙ Artificial intelligence (AI) & machine learning (ML) are potential tools for the clinical management of chordomas due to their ability to extract insights from complex, high-dimensional data.
- Convolutional neural networks (CNNs): tumour volume estimation & segmentation tasks.2
- Clustering algorithms: identify distinct clusters based on shape, texture, & DNA methylation.3
- Bayesian algorithms: the potential of probabilistic models for diagnosis & prognosis.4
- Logistic regression & tree-based models: identify tumour types & anticipate recurrence.5,6
- Support vector machines (SVMs): provide a framework for differentiating complex tumour types.7
Objectives
To review the current landscape of AI applications in chordoma management, delineate the existing knowledge gaps, & elucidate potential future directions.
Methods
- Databases: MEDLINE, Cochrane, Embase, Scopus, & Web of Science.
- Screening was executed by two independent reviewers using Covidence. Cohen’s kappa statistic was used to evaluate inter-rater variability.
- A comparison was made between the consensus results from the title & abstract screening, & an automated screening program based on GPT-4.8
- Publication Type: Peer-reviewed research articles, conference papers/abstracts, & systematic reviews
- Topic: AI techniques or methods in the context of chordoma
- Methodology: Studies involving any form of AI
- Non-English Language
- Irrelevant Topics
- Non-Peer Reviewed Sources
- Duplicate Publications
- Review Articles
- Animal Studies
Results
Figure 1. PRISMA flowchart of the study selection process.
Figure 2. (a) Types of included studies (n=18). (b) Number of articles published.
Table 1. Studies organized by algorithm type and clinical task.
_______
Figure 3. (a) Input data modalities to the algorithms. (b) Location of the chordoma. (c) Type of algorithm used. (d) Primary outcome of the included studies.
Table 2. Evaluation metrics organized by clinical task (number of studies in parentheses).

*E.g., logrank test for comparing survival distributions. ASSD, average symmetric surface distance; AUROC, area under the receiver operating characteristic curve
Discussion
- Inter-rater variability assessment had a kappa of 0.441 (absolute agreement of 0.932). Kappa was 0.933 between the GPT-4 model and the human final consensus results.
- The search yielded 1,006 records, with a total of 18 studies included for analysis (Fig. 1).
- All studies were conducted after 2017 (Fig. 2).
- ML models were derived from volumetric imaging in 12 studies, with 8 studies using MRI-based imaging, 4 using CT-based imaging, and 2 using ML derived from patient clinical data (Fig. 3a).
- The reported chordoma location was predominantly at the skull base (Fig. 3b) and the reported primary outcome was classification (Fig. 3d).
- CNNs were notably employed for tumour volume estimation, showcasing enhanced efficiency and precision (Table 1).
- Clustering algorithms demonstrated potential in diagnostic and prognostic evaluations (Table 1).
- Bayesian algorithms, logistic regression, tree-based models, and SVMs also showed application in diagnostic and prognostic tasks (Table 1).
Limitations
The studies encountered several limitations, including small datasets, absence of hyperparameter optimization, and a lack of validation on external datasets. Moreover, there was a failure to incorporate radiological descriptors or images, which are crucial for comprehensive analysis. Additionally, the significant heterogeneity observed in some studies among skull-based chordoma tissues impeded the robustness of classification. Furthermore, susceptibility to intra-observer variability and the scarcity of data from rare tumours were reported across studies.
References
- Walcott BP, et al. Lancet Oncol (2012). doi: 10.1016/S1470-2045(11)70337-0.
- Huang C, et al. Multimed Tools Appl (2022). doi: 10.1007/s11042-022-12335-y
- Ezugwu AE, et al. Eng Appl Artif Intell (2022). doi: 10.1016/j.engappai.2022.104743
- Ma SX, et al. Radiol Artif Intell (2023). doi: 10.1148/ryai.210187
- Li J, et al. Comput Biol Med (2022). doi: 10.1016/j.compbiomed.2021.105154.
- Yesilkaya B, et al. J Comput Sci (2022). doi: 10.1016/j.jocs.2022.101775
- Shirzadfar H, et al. Signif Bioeng Biosci (2019). doi: 10.31031/sbb.2019.03.000563
- Guo E, et al. J Med Internet Res (2024). doi: 10.2196/48996
Evaluating AI Performance in Written Neurosurgery Exams: A Comparative Analysis of Large Language Models

Background
The integration of Artificial Intelligence (AI) in medical education is an area of growing importance. While AI models have been evaluated extensively in multiple-choice (MC) question formats, their proficiency in written exams remains to be explored. The integration of AI in healthcare holds potential; however, understanding each model's applications and limitations remains a subject of ongoing discussion.1,2 A recent study evaluated the responses of four AI models in medical scenarios relating to anaesthesia, emergency care, critical care, and cardiology3:
- GPT-4 (OpenAI) scored well on clarity of answers
- Claude-2.1 (Anthropic) provided more complete and thorough responses
- Gemini Pro/Bard (Google) demonstrated better clarity in test responses but variable consistency
- Perplexity 70B (Perplexity) showed good completeness and clarity in responses
Objectives
To explore the proficiency of various AI models in written medical examinations, particularly with regards to factual-based questions versus higher reasoning questions in neurosurgery-related scenarios.
Methods
Four AI models—GPT-4 (OpenAI), Claude-2.1 (Anthropic), Gemini Pro (Google), and Perplexity 70B (Perplexity)—were tested using the Canadian Royal College Sample Neurosurgery Exam. The written and applied exams covered diagnostic reasoning, knowledge of neurosurgical conditions, and understanding of radiographic imaging techniques.
Limitations
There may be bias in choosing scenarios and training data for different AI models. Datasets with privacy restrictions are not used to train AI models, therefore the response scope may be limited. As well, the static nature of AI responses fail to capture the dynamics of decision-making in actual clinical situations.
Sample Written Exam
_____
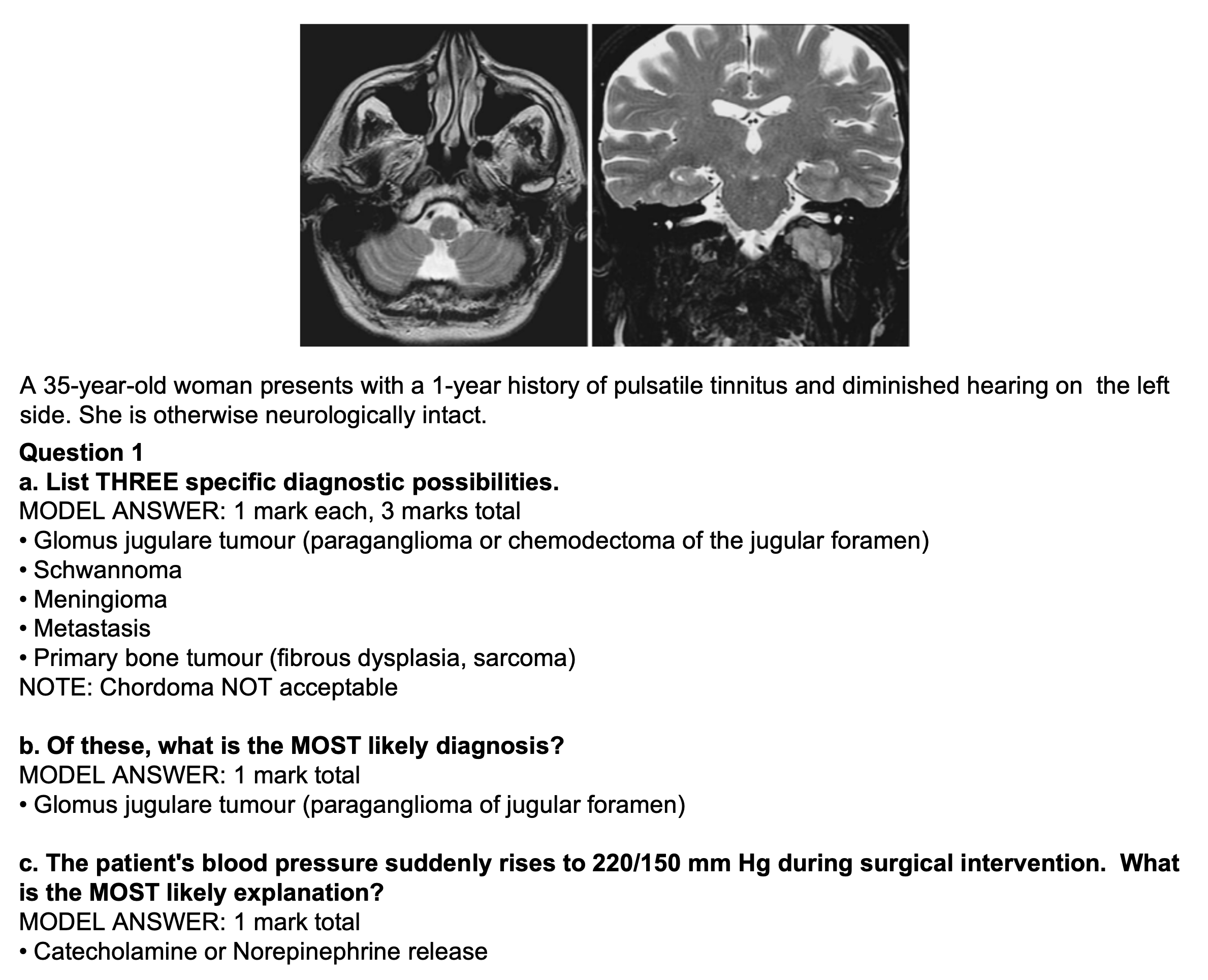
Sample Applied Exam
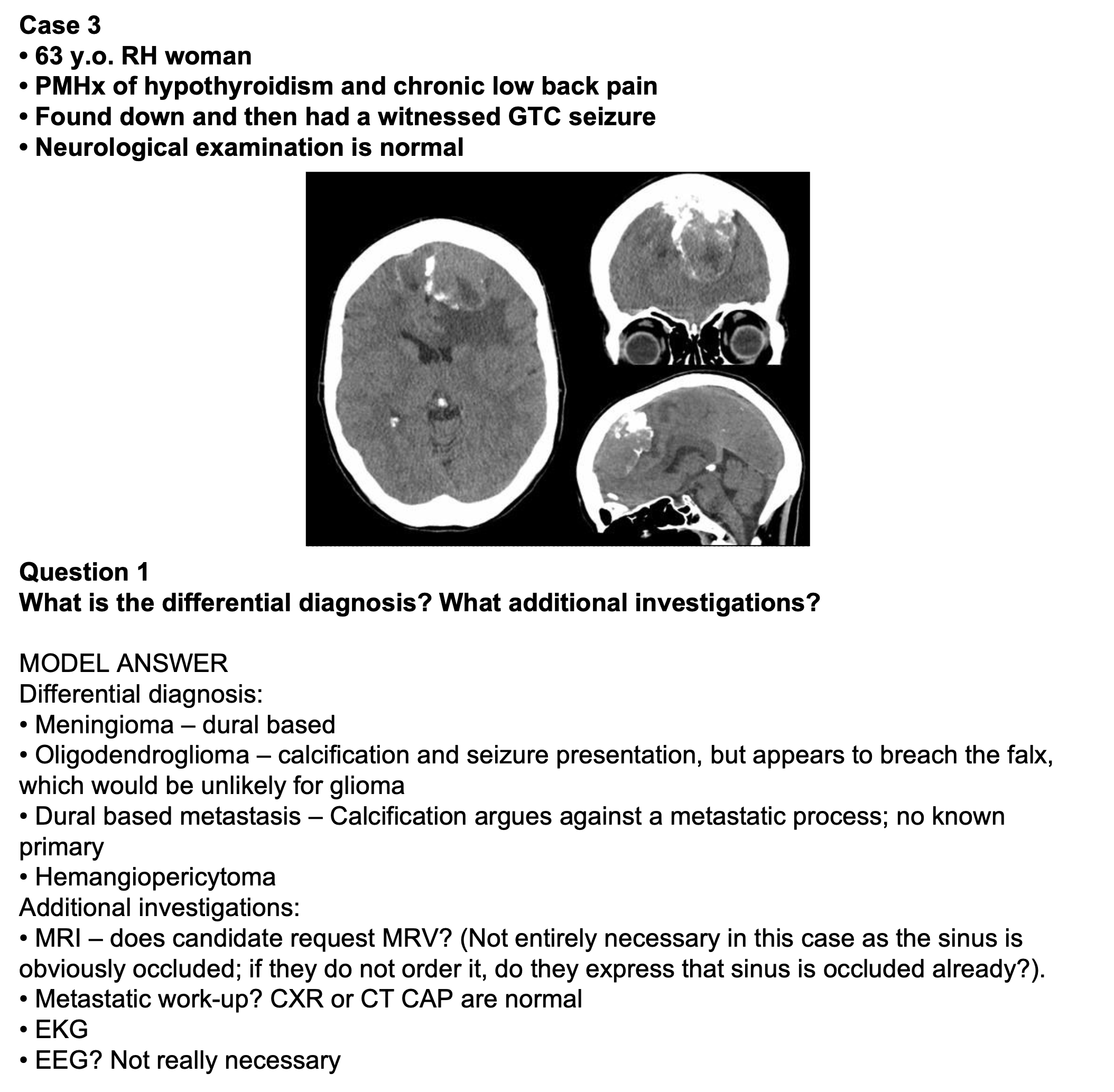
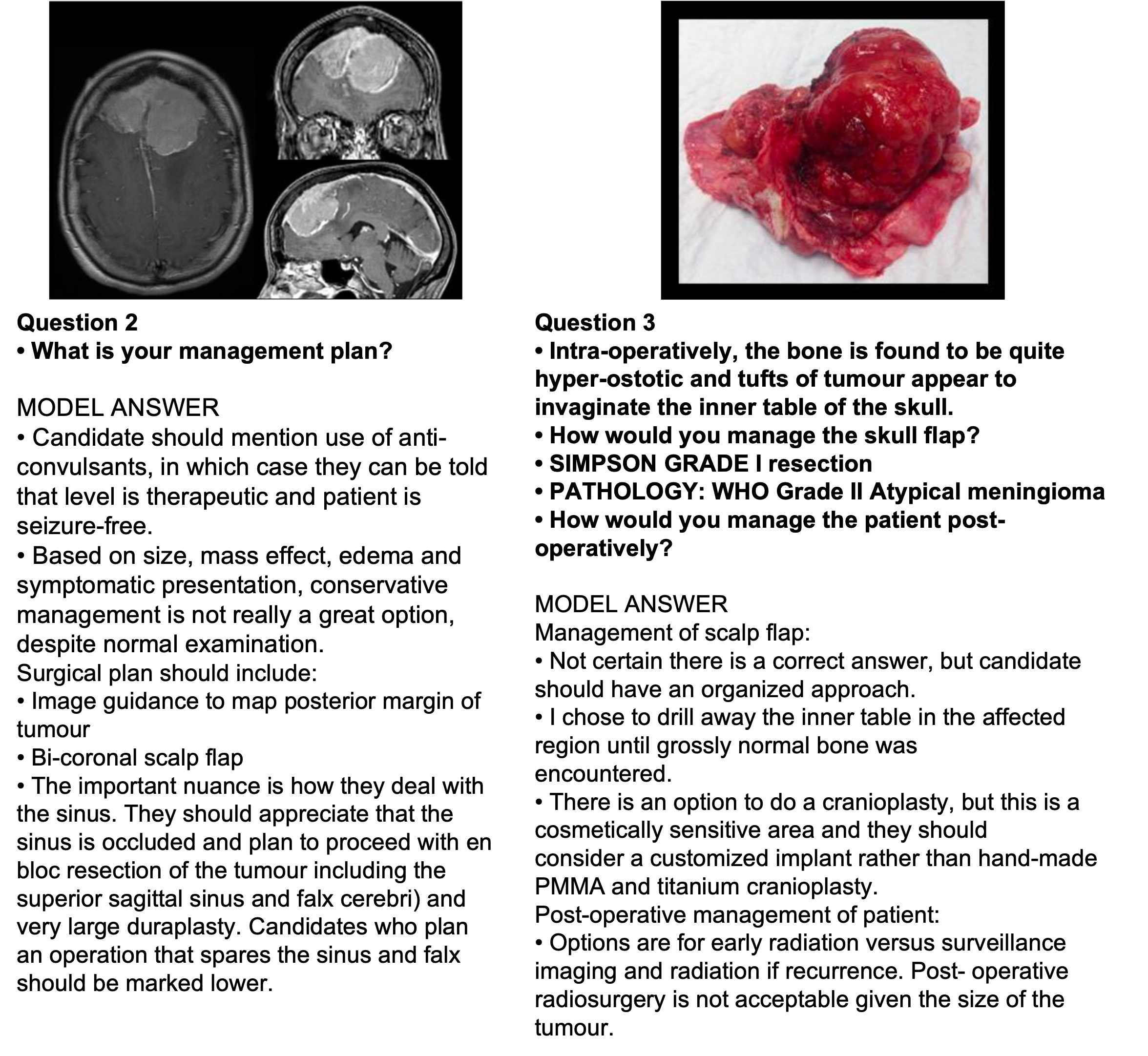
Results
Figure 1. AI model scores on the Canadian Royal College Sample Neurosurgery Exam.
- GPT-4 and Perplexity 70B both achieved a score of 68.42%, followed by Claude-2.1 with 60.53%, and Gemini Pro with 57.89%.
- The models showed proficiency in answering questions that required factual knowledge, such as identifying pathogens in spinal epidural abscess.
- The models struggled with more complex diagnostic reasoning tasks, particularly in explaining the pathophysiology behind a sudden rise in blood pressure during surgery and interpreting radiographic characteristics of intracranial abscesses on MRI.
The findings indicate that while AI models like GPT-4 and Perplexity 70B are adept at handling factual neurosurgical questions, their performance in complex diagnostic reasoning in a written format is less consistent. This underscores the need for more advanced and specialized AI training, particularly in the nuances of medical decision-making.
References
1. Compagnucci MC, et al., editors. AI in eHealth: Human autonomy, data governance and privacy in healthcare. Cambridge University Press (2022). doi: 10.1017/9781108921923.
2. Lee P, et al. N Engl J Med (2023). doi: 10.1056/NEJMsr2214184.
3. Uppalapati VK, et al. Cureus (2024). doi: 10.7759/cureus.52485.
2. Lee P, et al. N Engl J Med (2023). doi: 10.1056/NEJMsr2214184.
3. Uppalapati VK, et al. Cureus (2024). doi: 10.7759/cureus.52485.
Canadian Neurosurgical Healthcare Spending Trends

Background
- Neurosurgical procedures, given their complexity and necessity for advanced technology, are inherently costly.1
- In the United States and Canada, approximately 1.1 million neurosurgical cases are reported yearly, with around 665,000 requiring operative procedures.2
- Median wait time for a neurosurgical specialist consultation is 45.7 weeks and patients wait on average 13.3 weeks before receiving treatment.3
- Prolonged wait times reflect the high demand for neurosurgical services, strain on healthcare resources, and potential impacts on patient outcomes.
- A notable gap exists in a comprehensive economic analysis of neurosurgical healthcare spending in Canada.4
Objectives
This study aims to provide a detailed analysis of healthcare spending trends related to neurosurgery in Canada. It seeks to offer insights into the financial implications of managing neurosurgical cases, considering factors like healthcare costs, volume of cases, and length of stay (LOS).
Methods
Data Source and Collection
- Data was obtained from the Canadian Institute for Health Information National Health Expenditure Trends dataset available publicly online.5,6
- The healthcare database represents various metrics across Canada from the fiscal year 2015 to 2019.
- The dataset classified neurosurgical interventions using Case Mix Groups+ (CMG+) methodology.7
- Decision tree performances were measured using the F1-score, precision, and recall.
- The average acute LOS was stratified into quintiles.
- All error estimates are reported using one standard error of the mean unless otherwise indicated.
- Python version 3.9.16 and the packages Pandas, Matplotlib, and Numpy were used for to create all figures and analyses.
Results
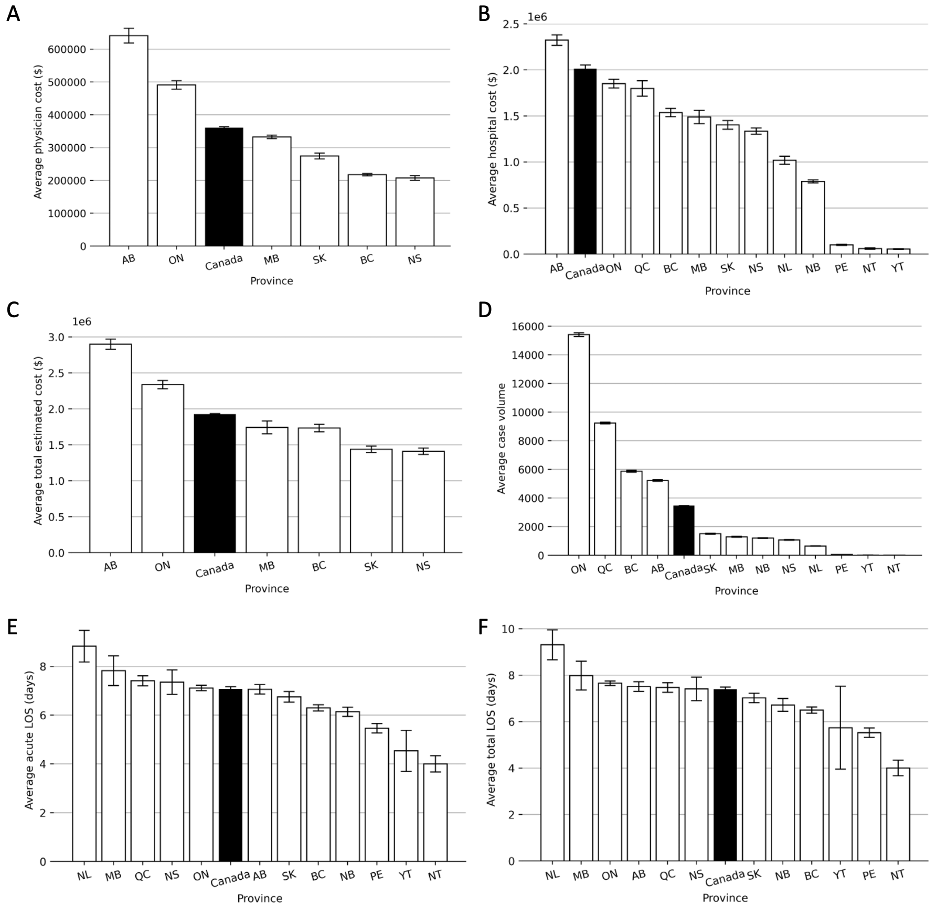
Figure 1. Per province analysis of (A) average physician cost, (B) average hospital cost. (C) average total estimated cost, (D) average case volume, (E) average acute LOS, and (F) average total LOS. LOS = length of stay.
Table 1. Annual case volumes and associated physician and hospital costs.
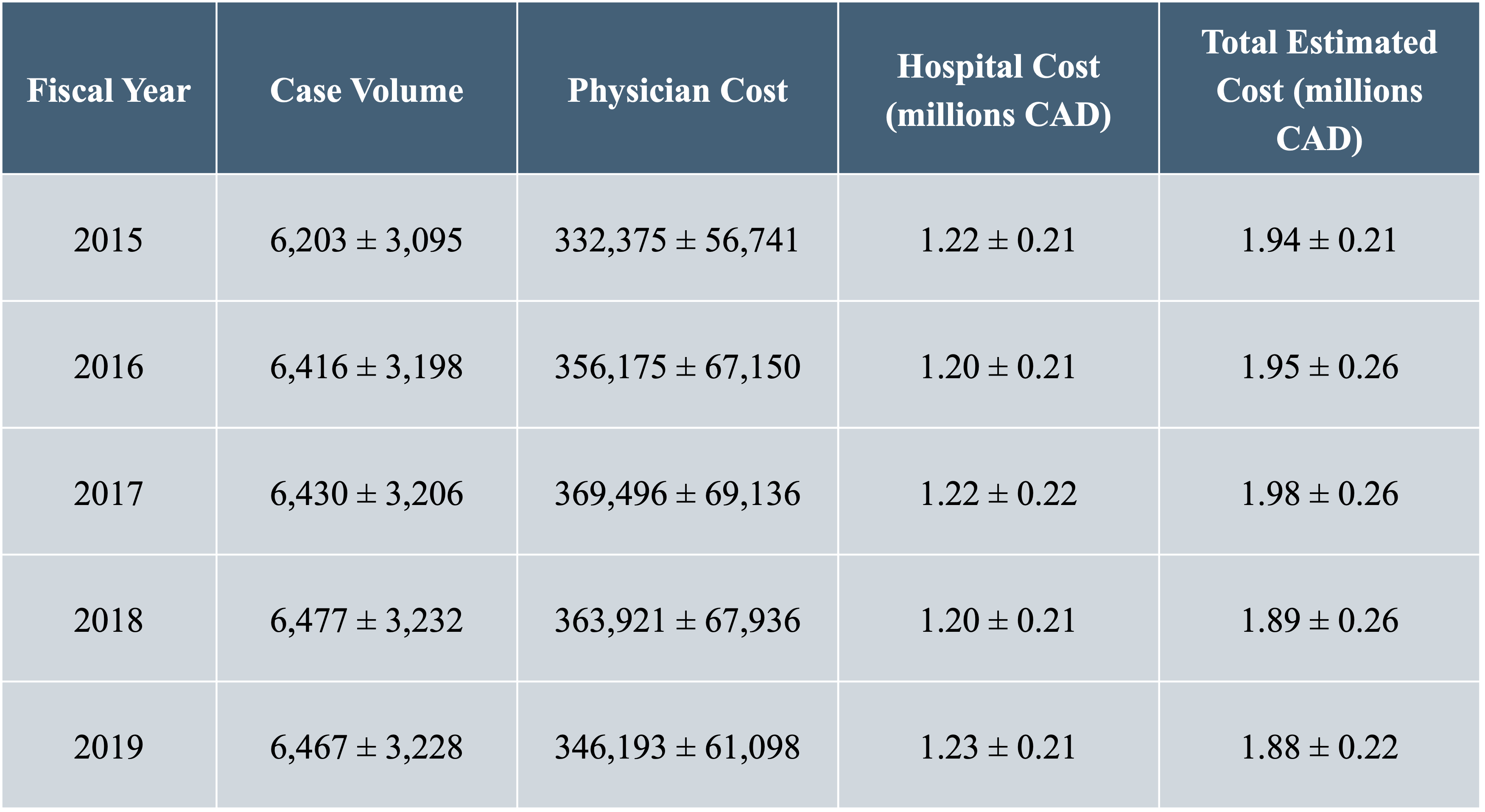
___

Figure 2. Case volume and total estimated cost by intervention group.
Table 2. Healthcare costs and average stay lengths by age group in Canada, with hospital and physician expenses in CAD. LOS = length of stay. ALC = alternative level of care.
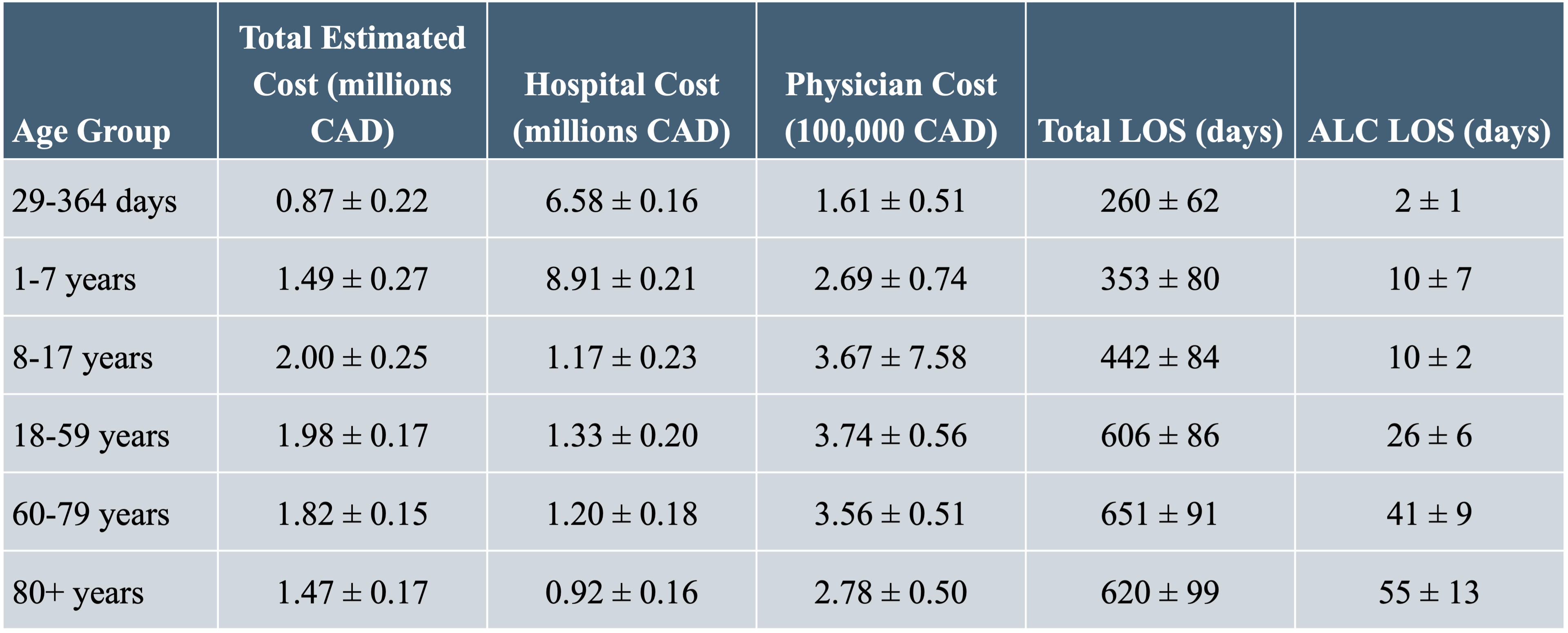
Table 3. Decision tree to predict the average total length of stay (5 bins) from the average acute length of stay and age group for various neurosurgical interventions.
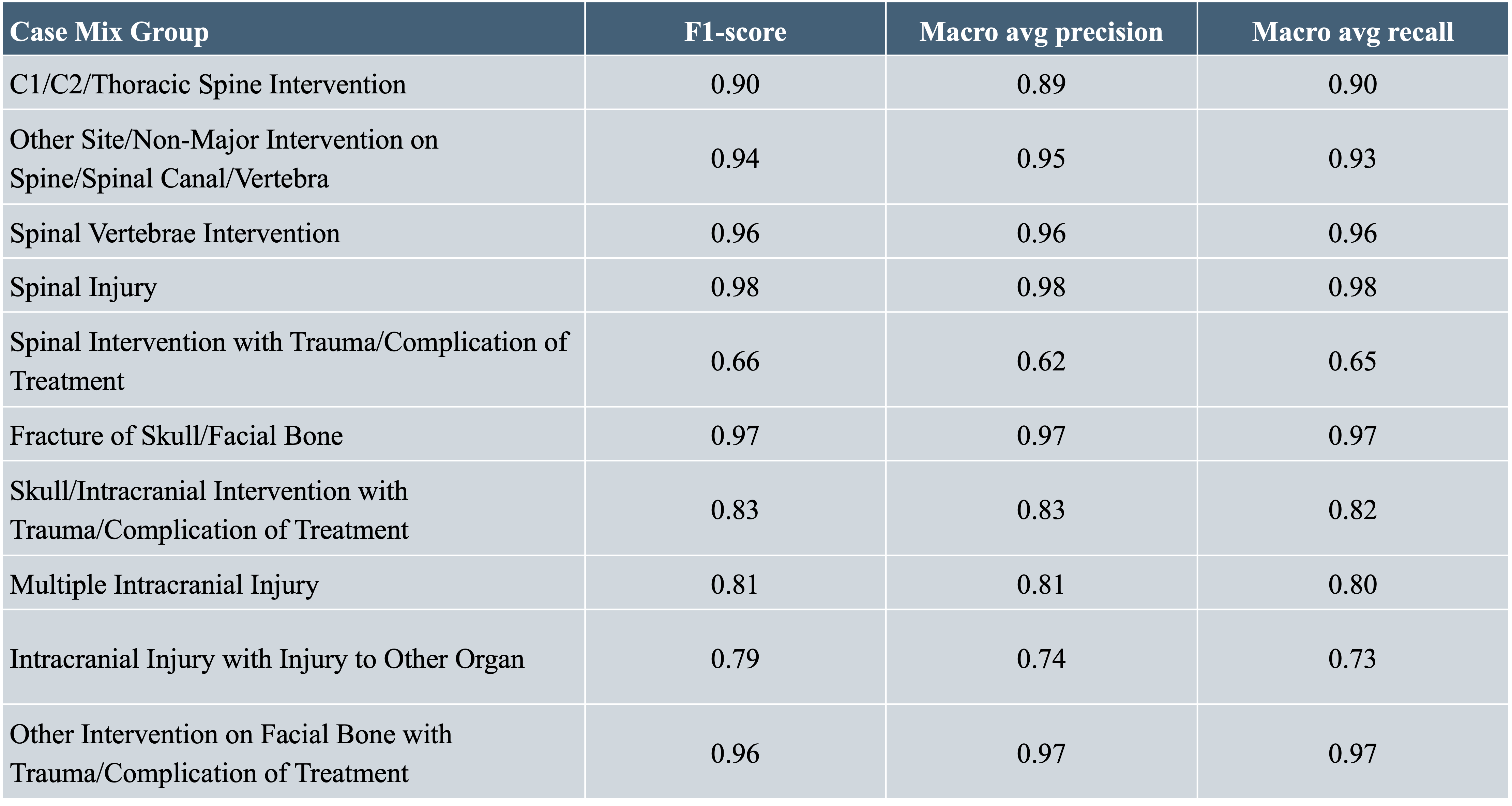
Discussion
- Alberta reported the highest average physician costs (641,449 ± 22,657 CAD, Fig. 1A) and hospital costs, (2,324,680 ± 127,683 CAD, Fig. 1B), despite lesser access to advanced neurosurgical and imaging technologies, versus Ontario and Quebec.
- Manitoba recorded the longest average acute LOS, while Newfoundland & Labrador showed the highest average total LOS, both at nine days (Fig. 1E).
- There was a modest increase in case volumes from 6,220 ± 3,103 in 2015 to 6,492 ± 3,240 in 2018, with a slight decrease in 2019 (Table 1).
- The total estimated hospital costs remained stable over five years, ranging from 2.27 ± 0.38 million CAD in 2015 to 2.23 ± 0.44 million CAD in 2019 (Table 1).
- The highest costs were seen in the 18-59 age group, at 2.53 ± 0.43 million CAD (Table 2).
- Decision tree models showed high accuracy for predicting LOS in cases like spinal injury (F1- score: 0.98) but were less accurate for interventions with trauma or complications (F1-scores ranging from 0.66 to 0.97) (Table 3).
Limitations
The temporal scope of the data spanning from 2015 to 2019 represents a relatively short duration for observing and extrapolating long-term healthcare trends and impacts. Disparities between compensation models can complicate direct comparisons of physician costs across provinces, potentially skewing the understanding of regional cost variations. Predicting the total LOS based on age group and average acute LOS may not fully capture the intricacies and individualized nature of illness recovery.
References
- Ravindra VM, et al. World Neurosurg (2015). doi:10.1016/j.wneu.2015.06.046
- Mukhopadhyay S, et al. J Neurosurg (2019). doi:10.3171/2018.10.JNS171723
- Moir M, et al. Fraser Institute (2022). https://policycommons.net/artifacts/3336916/waiting-your-turn/4135742/
- Benzil DL, et al. J Neurosurg (2008). doi:10.3171/JNS/2008/109/9/0378
- Canadian Institute for Health Information. National health expenditure trends (2023). https://www.cihi.ca/en/national-health-expenditure-trends
- Canadian Institute for Health Information. Patient Cost Estimator (2024). https://www.cihi.ca/en/patient-cost-estimator
- Canadian Institute for Health Information. Introduction to CMG+ Aggregation Variables (2022). https://www.cihi.ca/sites/default/files/document/introduction-to-CMG-plus-aggregation-variables-en.pdf
Use of jugular venous pressure to optimize outcomes of vestibular schwannoma resection: a review of the literature and proof of concept
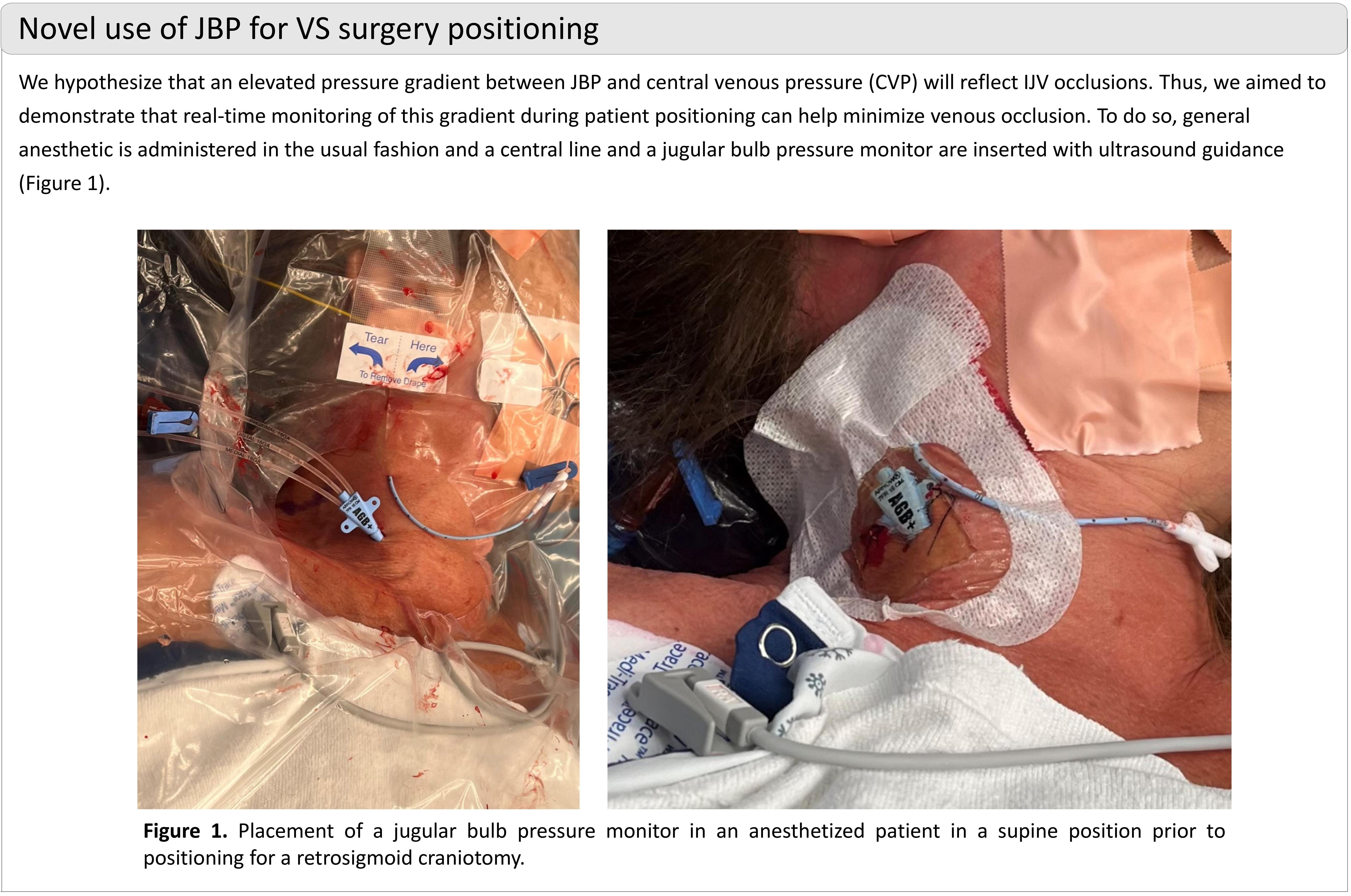
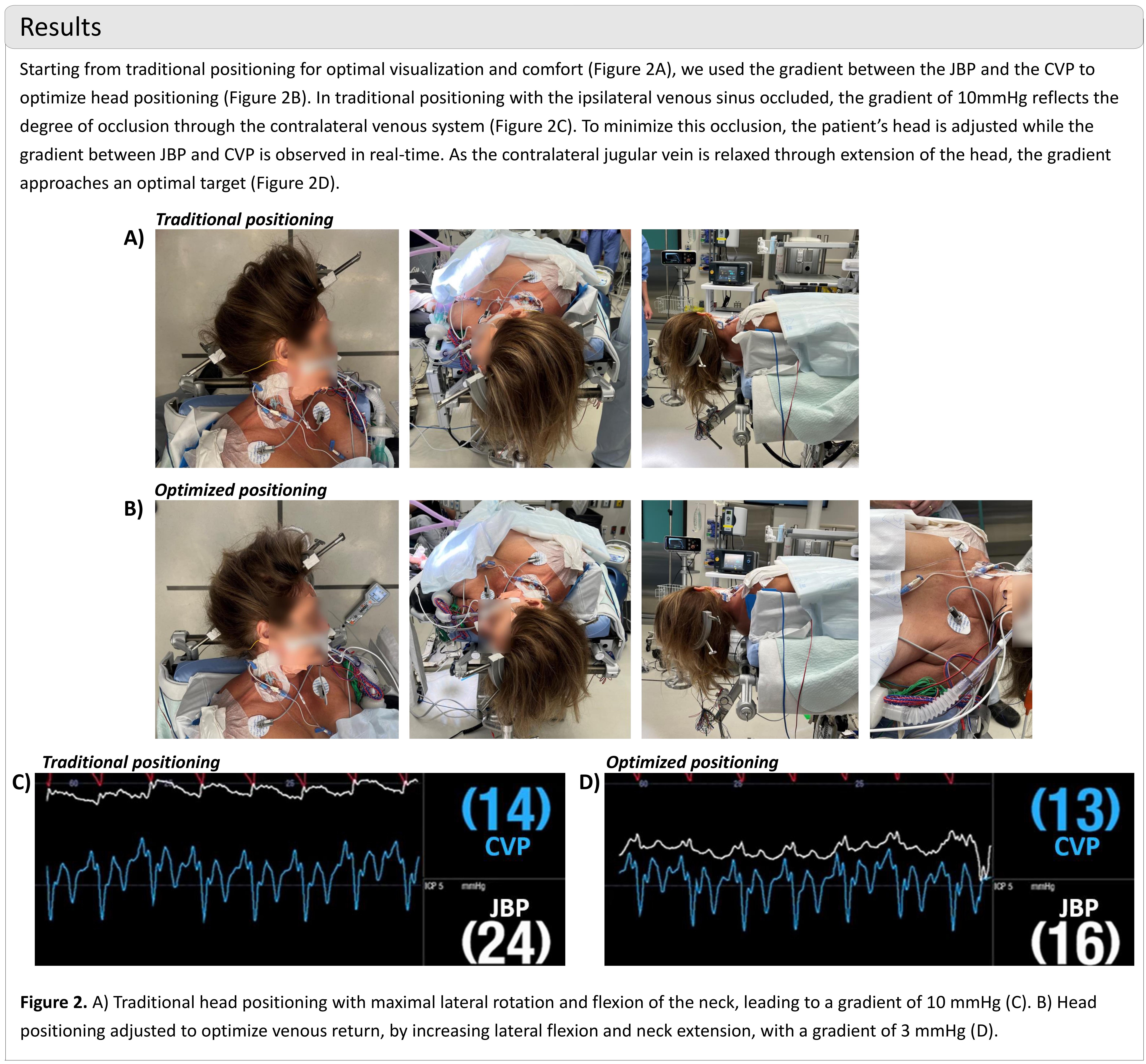

INTRODUCTION
High grade gliomas (HGG) are incurable, aggressive brain malignances that occur in patients of all ages. These cancers carry universally poor prognoses. To elucidate mutations and transcriptional changes driving glioma growth and progression, we used a Nestin-Cre mouse model in combination with an extrinsic chemical mutagen (N-ethyl-N-nitrosurea, ENU), to sample discrete lesions during premalignant, early stage tumor, and end stage tumor phases.
METHODS
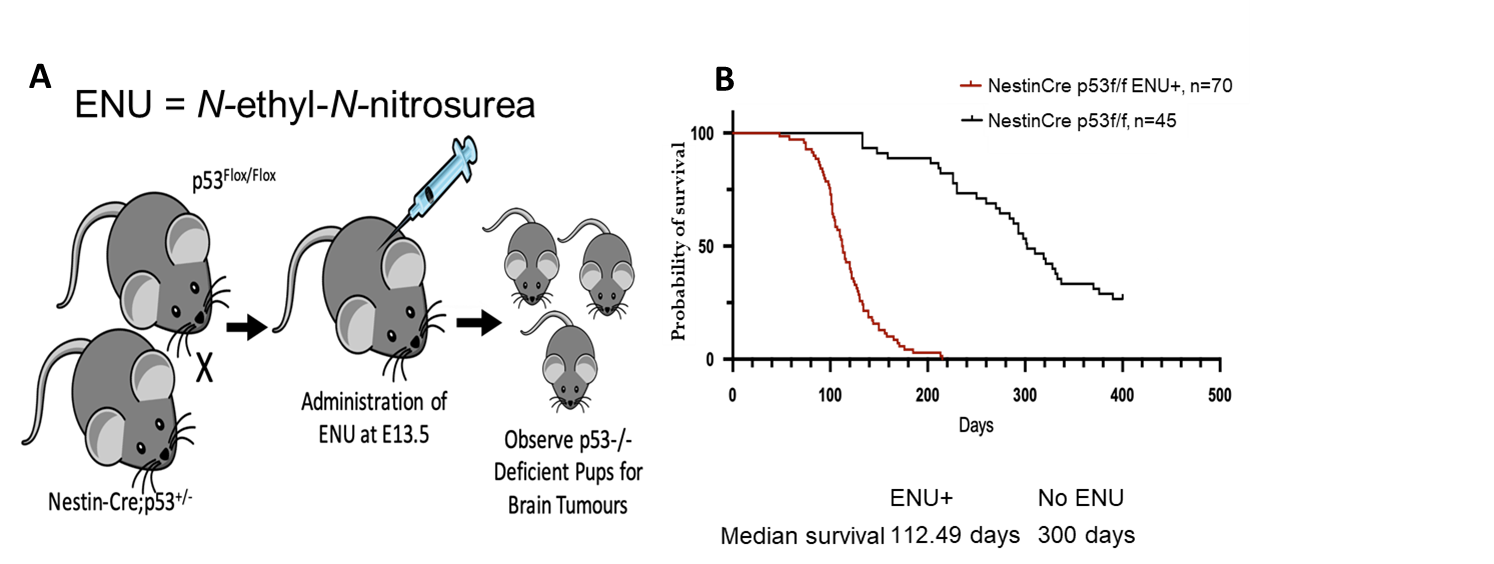
Figure 1. A) Experimental workflow for Nestin-Cre;p53 flox/flox mice receiving ENU administration. B) Survival curves of mice with and without ENU administration.
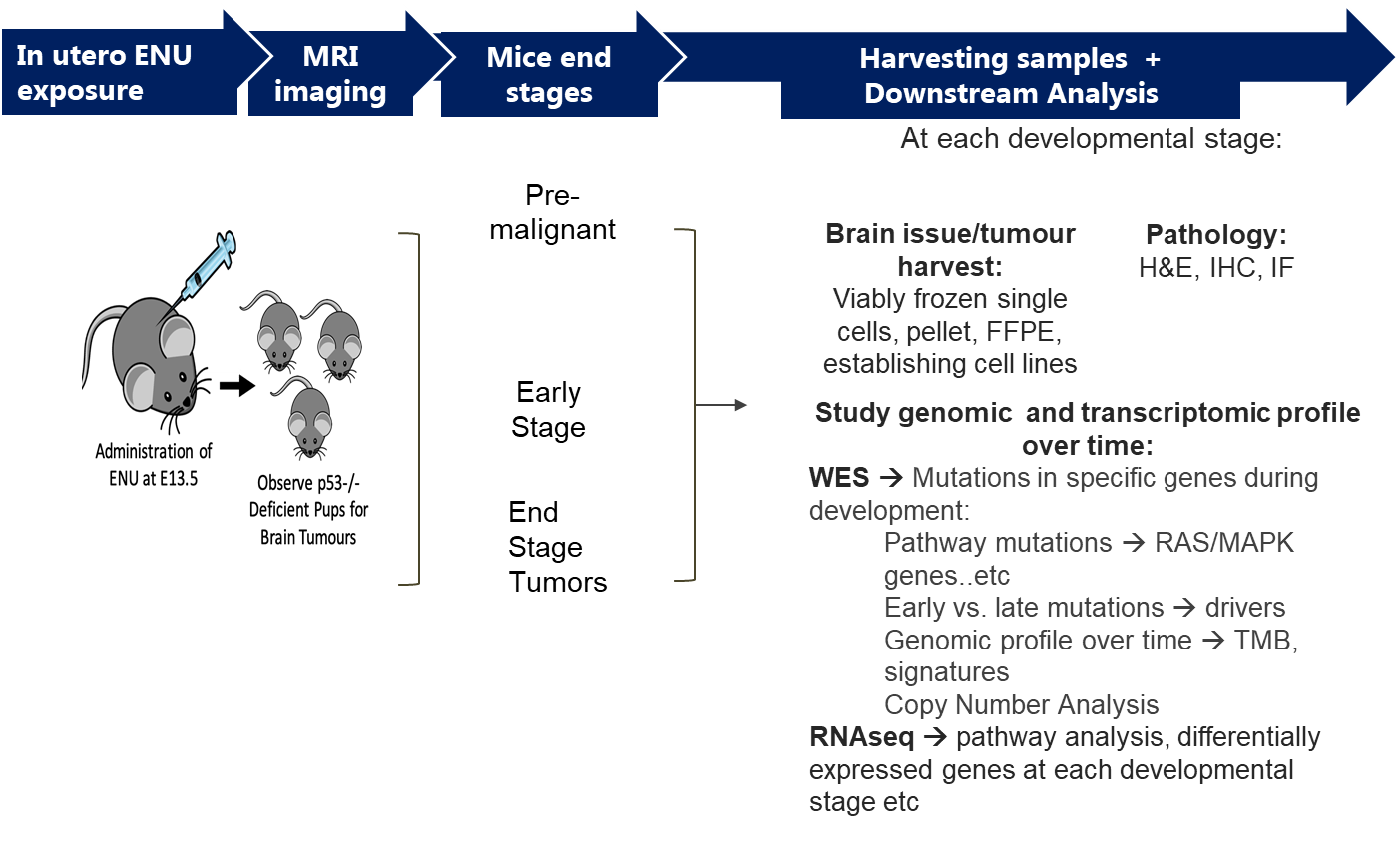
Figure 2. Experimental workflow with tissue sampling at discrete stages of tumor growth
SOMATIC MUTATION AND CNV ANALYSIS
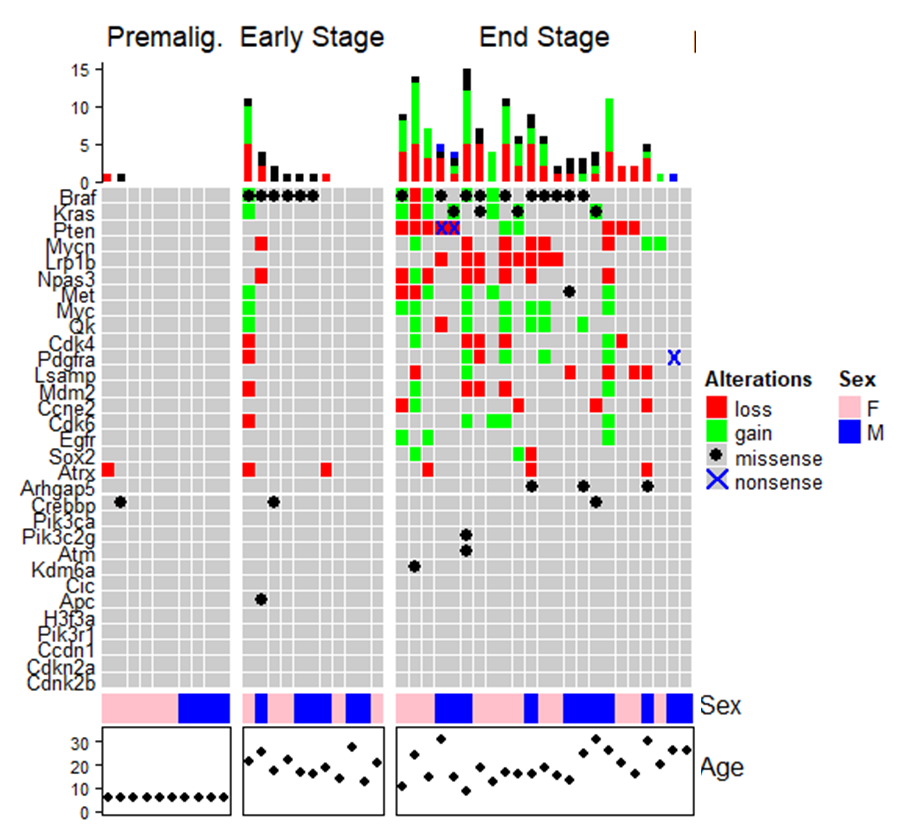
Figure 4. Somatic mutation and CNV analysis of experimental groups

Figure 5. Transcriptional heatmap shows clustering of early and end stage tumors
GSEA OF MAPK PATHWAYS
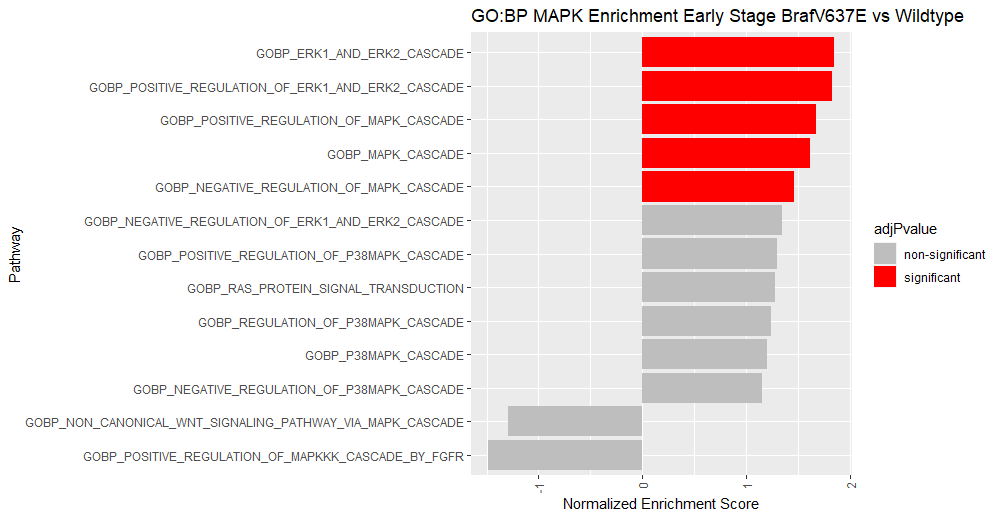
Figure 6. Differentially enriched GO:BP MAPK Pathways between early stage lesions with and without BrafV637E mutation.
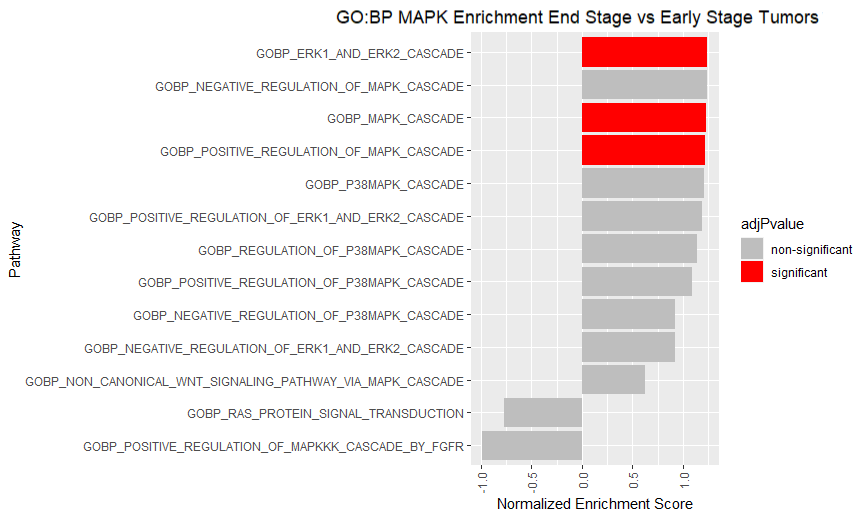
Figure 7. Differentially enriched GO:BP MAPK Pathways between end stage tumors and early stage lesions.
CONCLUSIONS
We show that the somatic mutations, copy number changes, and transcriptional profiles of tumors vary depending on the stage of growth. Importantly, we show that the Raf/Ras pathway is key for tumor growth with a recurring Braf mutation occurring in early stage lesions. Additionally, gene set enrichment analysis (GSEA) shows that end stage tumors have increased immunogenic/inflammatory activity, and increased signaling through Raf/Ras. Overall, this work sheds light on important differences between early and late stage tumors.
The effect of after-hours surgical resection on the outcomes in patients with high grade gliomas
Introduction
- High grade gliomas (HGG) are malignant central nervous system tumors that present with rapid progression and portend a poor prognosis.
- The standard of care for HGGs is maximal safe resection and multiple studies have demonstrated a clear benefit of near total and gross total resection. (1)
- Surgical intervention for HGGs may occasionally occur in the evening or weekend due to clinical presentation or operating room constraints.
- There are many studies demonstrating increased rates of morbidity and mortality in patients presenting in the evening or weekend, a term coined the "weekend effect". (2, 3)
- There is limited research on the impact of this effect on neurosurgical patients undergoing tumor resection.
Aim
- To evaluate the effect of surgical timing on the outcomes for patients with high grade gliomas undergoing resection, with a focus on safety and efficacy.
Methods
Study design:
- Retrospective review.
- All patients presenting emergently to Vancouver General hospital who underwent high grade glioma resection.
- January 1, 2021 to March 31, 2023.
- Patients undergoing surgical intervention after-hours were compared to patients undergoing surgical intervention during regular hours.
- Greater than 50% of the surgical time between 1630h and 0659h or surgery conducted on the weekend.
- Extent of resection, operative time, estimated blood loss, length of stay, intraoperative complications, postoperative complications, reoperation within 30 days, postoperative ECOG performance status and 6-month mortality rates.
Results
| After-hours (n=19) | Regular hours (n=19) |
p-value | |
| Male (%) | 16 (84.2) | 14 (73.7) | 0.426 |
| Mean age, years (SD) | 57.7 (13.6) | 60.2 (10.0) | 0.535 |
| Presenting GCS, mean (SD) | 14.4 (1.6) | 13.9 (2.7) | 0.875 |
| GCS ≤ 8 on presentation (%) | 1 (5.3) | 2 (10.5) | 0.547 |
| Neurological deficits on presentation (%) | 11 (57.9) | 12 (63.2) | 0.740 |
| Surgical adjunct use (%) | 16 (84.2) | 13 (68.4) | 0.252 |
| WHO Grade Grade IV (%) Grade III (%) |
18 (94.7) 1 (5.3) |
18 (94.7) 1 (5.3) |
1.0 |
| 1D Tumor size, cm (SD) | 4.55 (1.57) | 4.85 (1.35) | 0.524 |
| 3D Tumor size, cm^3 (SD) | 36.5 (28.2) | 48.6 (39.4) | 0.352 |
| Eloquent tumor location (%) | 10 (52.6) | 9 (47.4) | 0.746 |
| Recurrent (%) | 2 (10.5) | 2 (10.5) | 1.0 |
| After-hours (n=19) | Regular hours (n=19) | p-value | |
| Gross total resection (%) | 5 (26.3) | 2 (10.5) | 0.2093 |
| Gross/near total resection (%) | 9 (47.4) | 8 (42.1) | 0.7442 |
| Intraoperative complications (%) | 0 (0) | 0 (0) | 1.0 |
| Postoperative complications (%) | 4 (21.1) | 4 (21.1) | 1.0 |
| Reoperation in 30 days (%) | 0 (0) | 1 (5.3) | 0.3109 |
| Death within 6 months (%) | 2 (10.5) | 3 (15.8) | 0.6315 |
| After-hours (n=19) | Regular hours (n=19) | p-value | |
| Estimated blood loss, mean mL (SD) | 123.7 (69.5) | 205.3 (112.9) | 0.0278 |
| Operative time, mean min (SD) | 136.9 (29.9) | 174.3 (72.7) | 0.0643 |
| Length of stay, median days (SD) | 5 (11.0) | 3 (2.0) | 0.0601 |
| ECOG score, median (SD) | 1 (1.0) | 1 (0.7) | 0.3953 |
Discussion
- Maximally safe resection and avoidance of complications is key for high grade glioma patients.
- There was no difference in extent of resection, complication rates, reoperation rates, mortality or functional outcomes between after-hours group and regular hours group.
- This is likely attributable to neurosurgeon surgical expertise and protocol driven standard of care which may override the potential negative factors associated with after-hours care.
- This study was a retrospective review with a limited sample size at a single institution.
Conclusions
- Our study demonstrates that high grade glioma patients undergoing emergent after-hours tumor resection do not have increased morbidity or mortality, nor is there a meaningful impact on extent of resection or complication rates.
References
- Hottinger AF, Abdullah KG, Stupp R. Current standards of care in glioblastoma therapy. Glioblastoma. Elsevier; 2016. p. 73-80.
- Desai V, Gonda D, Ryan SL, et al. The effect of weekend and after-hours surgery on morbidity and mortality rates in pediatric neurosurgery patients. J Neurosurg Pediatr. 2015;16:726-731.
- Charest-Morin R, Flexman AM, Bond M, et al. ‘After-hours’ non-elective spine surgery is associated with increased perioperative adverse events in a quaternary center. Eur Spine J. 2019;28:817-828.
Optic nerve sheath diameter correlates with both success and failure of hydrocephalus treatment in pediatric patients with pineal region lesions
Introduction
- Pineal region lesions in the pediatric population are often symptomatic due to occlusive hydrocephalus and thus elevated intracranial pressure (ICP).
- Optic nerve sheath diameter (ONSD), measured on MRI, has been shown to be a useful non-invasive technique in assessment of ICP. (1)
- Post-operative radiographic evaluation of patients post-ETV or with treatment failure can be challenging as ventricular volume may not change immediately. (2)
- To compare pre-operative and post-operative ONSD with both clinical examination as well as frontal occipital horn ratio (FOHR).
Methods
Study design:
- Retrospective review.
- Pediatric patients with pineal region lesions who underwent surgical intervention at BC Children's Hospital.
- 2010 to 2023.
- Optic nerve sheath diameter (ONSD) and frontal occipital horn ratio (FOHR) measured preoperatively and postoperatively (within 2 weeks, 3 months, and 12 months) using MRI.
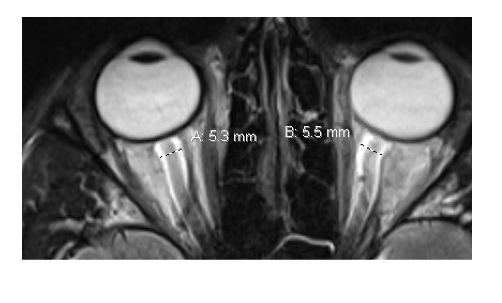
Image 1. ONSD measurements taken 3 mm from the papilla perpendicular to the trajectory of the optic nerve using T2 weighted MRI sequence.
Results
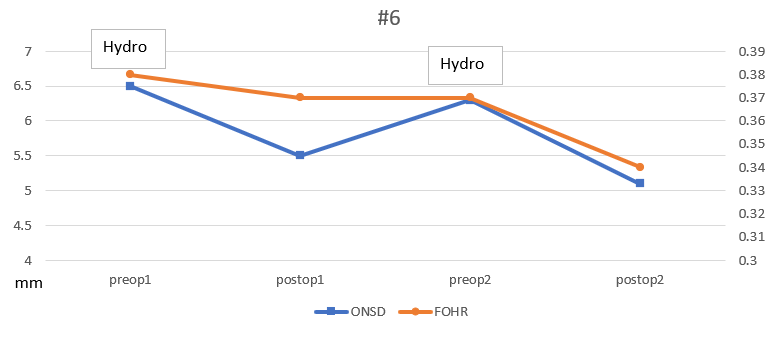

Figure 1. Relationship between ONSD and FOHR in three patients with treatment failure. FOHR did not increase despite increased ONSD and clinical signs of hydrocephalus.
| Preoperative | Postoperative | 3 months | 12 months | Without hydro | |
| ONSD (mm) | 6.5 ± 0.7 | 5.7 ± 0.7 (p<0.001) | 5.8 ± 0.6 (p<0.001) | 5.7 ± 0.7 (p<0.001) | 5.5 ± 0.4 (p=0.006) |
| FOHR | 0.42 ± 0.08 | 0.38 ± 0.06 (p=0.006) | 0.36 ± 0.09 (p=0.003) | 0.35 ± 0.06 (p<0.001) | 0.35 ± 0.08 (p=0.031) |
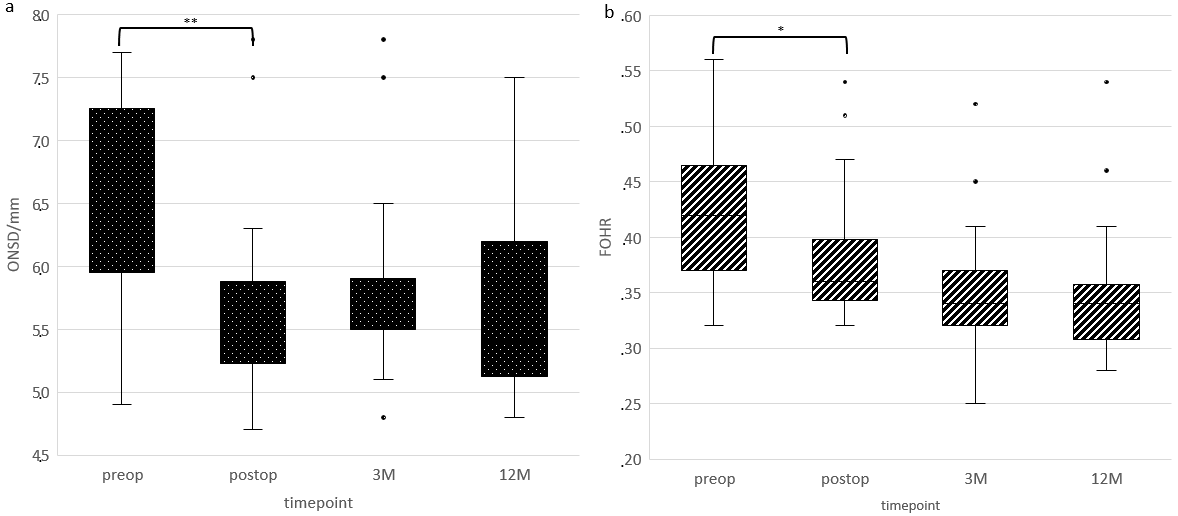
Figure 2. Preoperative and postoperative ONSD and FOHR changes in patients with hydrocephalus. ONSD demonstrates a larger immediate postoperative decrease compared to FOHR.
Discussion
- Our results showed a significant postoperative decrease of both ONSD and FOHR.
- ONSD showed a larger decrease postoperatively than FOHR and more reliably demonstrated treatment failure.
- This is a retrospective study with a relatively small sample size.
Conclusion
- ONSD measurements may have utility in evaluating intracranial hypertension due to hydrocephalus in pediatric patients with pineal region tumors.
- ONSD changes post-operatively appear to have value in assessing treatment failure.
References
- Kerscher, Susanne R et al. “The relation of optic nerve sheath diameter (ONSD) and intracranial pressure (ICP) in pediatric neurosurgery practice - Part II: Influence of wakefulness, method of ICP measurement, intra-individual ONSD-ICP correlation and changes after therapy.” Child's nervous system vol. 36,1 (2020): 107-115.
- Coulter, Ian C et al. “Cranial and ventricular size following shunting or endoscopic third ventriculostomy (ETV) in infants with aqueductal stenosis: further insights from the International Infant Hydrocephalus Study (IIHS).” Child's nervous system vol. 36,7 (2020): 1407-1414.
Factors affecting health-related quality of life among adult meningioma patients: a systematic review
BACKGROUND
Meningiomas are common brain neoplasms that can significantly influence health-related quality of life (HRQOL), yet the factors influencing HRQOL in adult patients remain unclear. We aimed to bridge this knowledge gap by determining these key factors.
OBJECTIVE
To determine what factors affect HRQOL in adult meningioma patients at various stages of treatment.
METHODS
We conducted a systematic review, searching EMBASE, MEDLINE, CINAHL, Scopus, and PsycINFO up to March 2023. We included original, peer-reviewed studies focusing on adult patients (>18 years) with current or past meningioma at any stage of treatment that measured HRQOL or its proxies in relation to tumour-, treatment-, and patient-related factors. Two independent reviewers screened abstracts and full texts, selecting studies with acceptable risk of bias1 for data extraction and narrative synthesis.
RESULTS
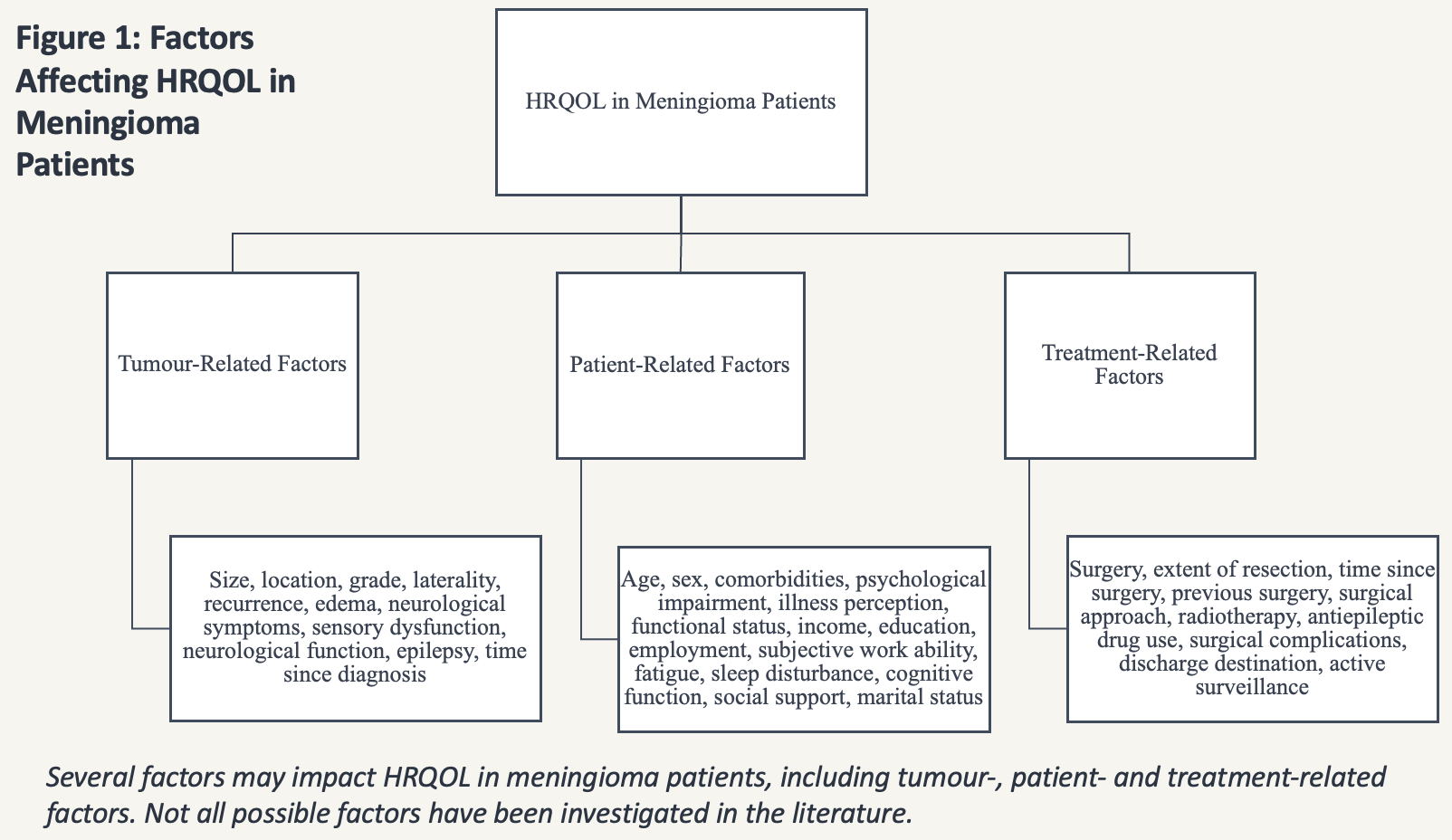
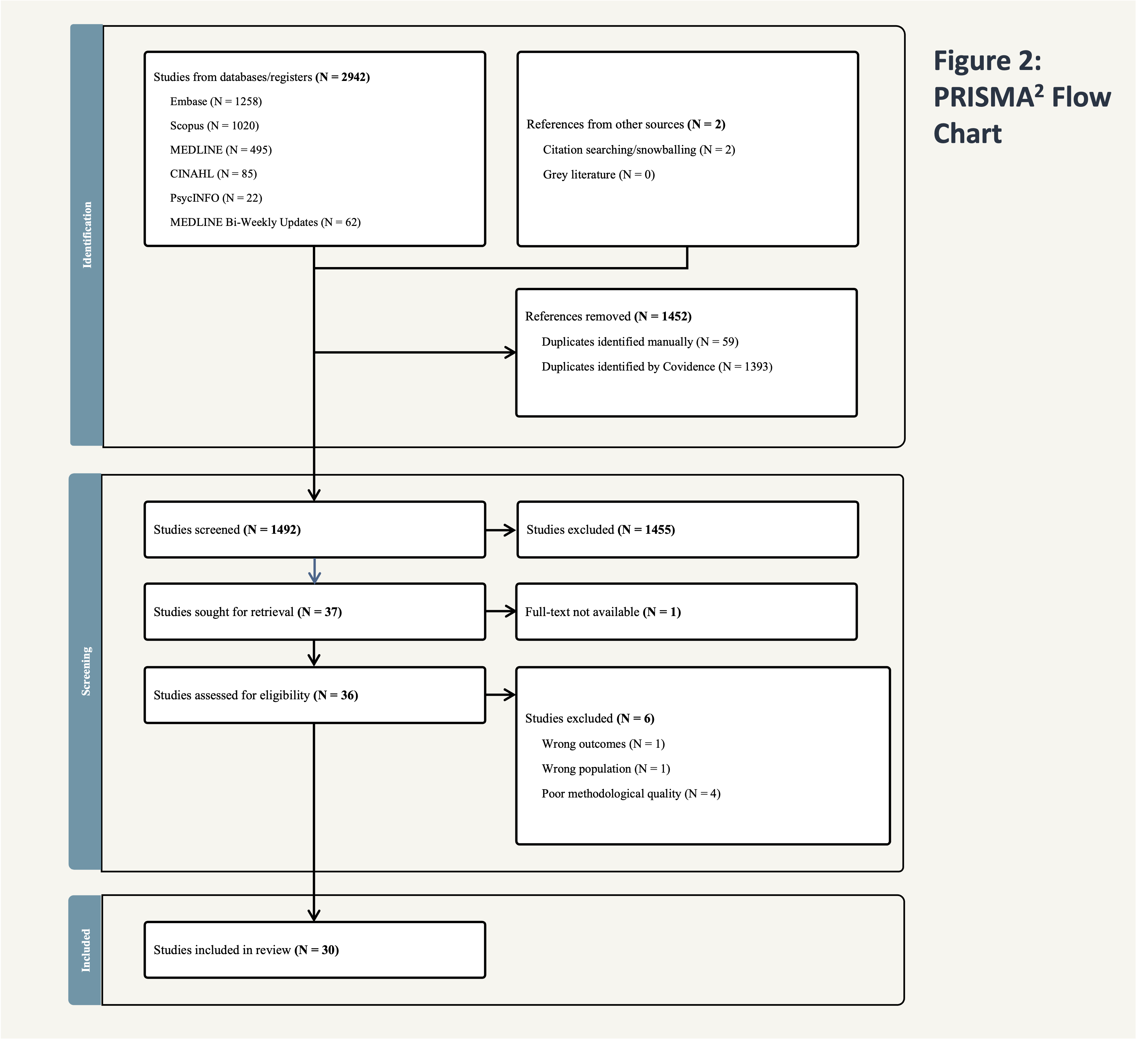
Of N=2942 identified studies, N=30 were included.3-32 Key factors found to influence HRQOL in adult meningioma patients include surgery, radiotherapy, neurological function, functional status, comorbidities, sleep quality, psychological impairment, age, and employment. Factors related to tumour characteristics yielded inconsistent findings. Heterogeneity and inconsistencies in HRQOL measurement across studies hindered definitive conclusions about the impact of factors on HRQOL.
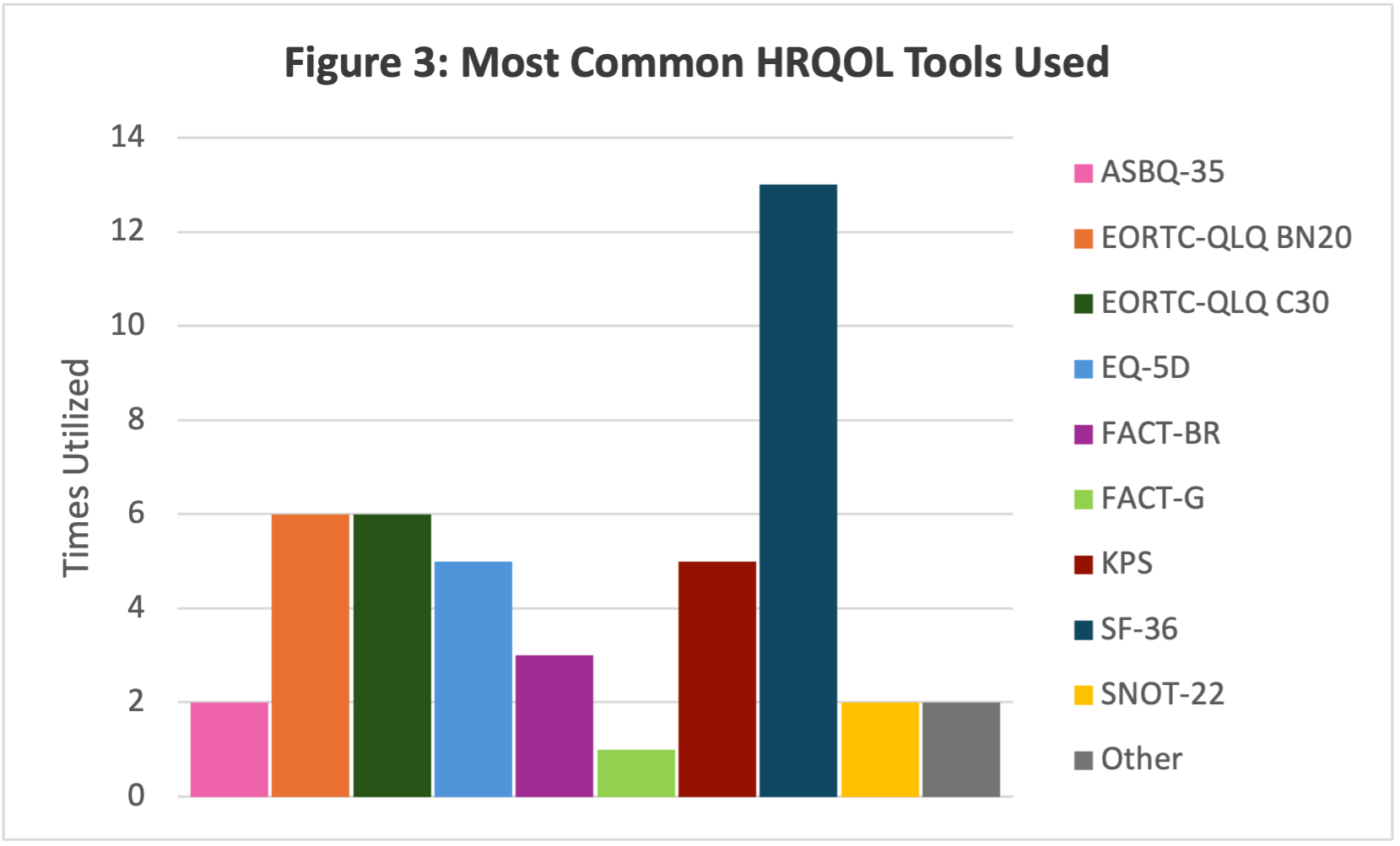
CONCLUSION
Our review emphasizes the need for standardized, disease-specific HRQOL assessments in meningioma patients. More consistent, large-scale, prospective research is essential to comprehensively understand and improve HRQOL, and thereby ensure tailored care for this population.
Future Directions

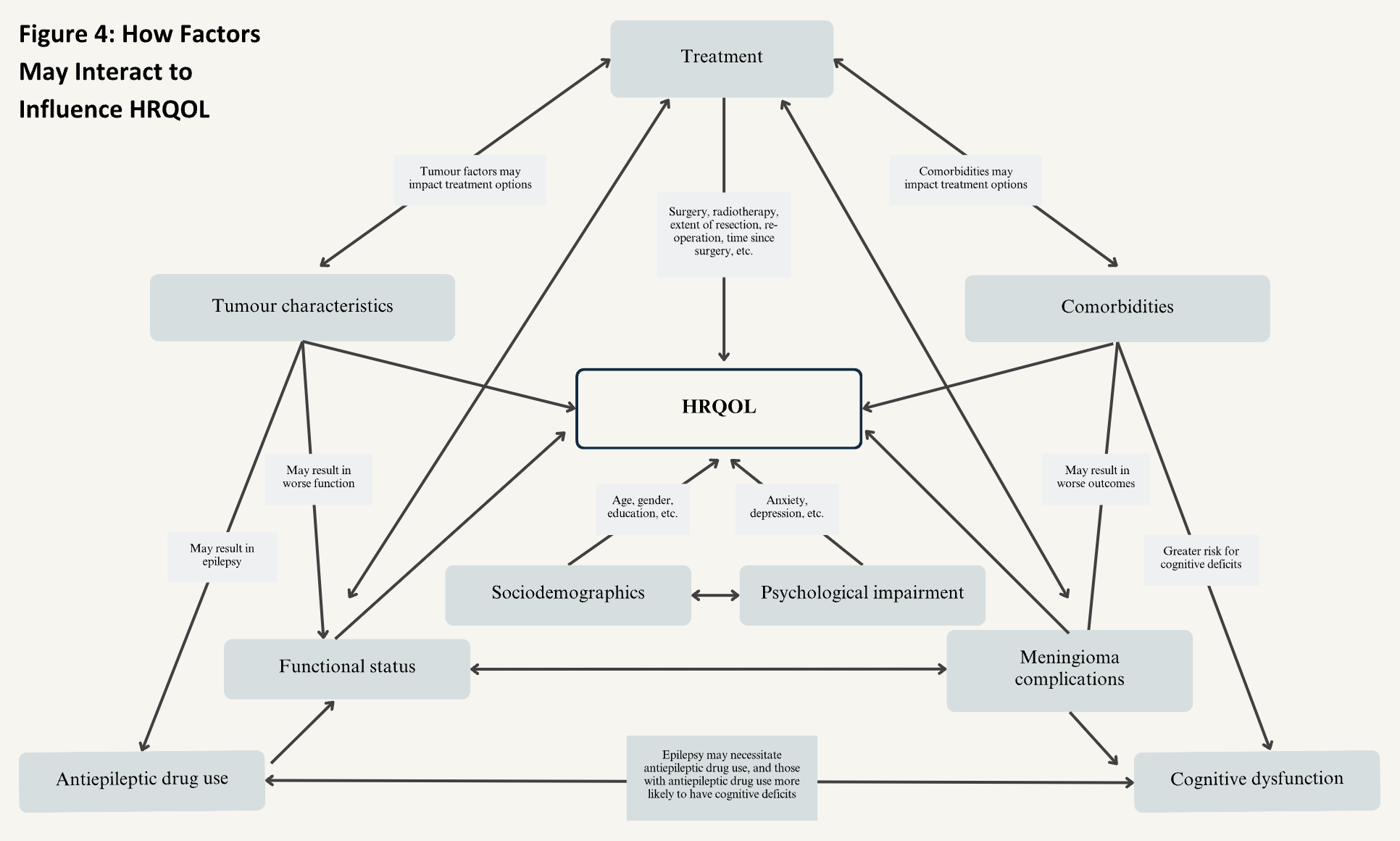
For questions or comments regarding this poster, please contact kara.jonas@mail.utoronto.ca
Wounded glioma syndrome: neurologic worsening in patients with subtotal resection in high-grade gliomas

ABSTRACT
- Subtotal resection (STR) of Grade III & IV gliomas
- Avg % volume resected: 26.5%
- Post-op infarct, hematoma, edema, and hydrocephalus may account for neurologic deficits 1 month post-STR
INTRODUCTION
-
High-grade gliomas (HGGs): maximal surgical resection, radiation and chemotherapy
- Wounded glioma syndrome: hemorrhage at surgical site post STR [2]
-
Objectives:
- Primary: Determine average % volume resected during STR in patients with post-op neurologic worsening
-
Secondary:
- Characterize new/worsening post-STR neurologic deficit
- Characterize radiographic factors associated with above
METHODS
- Single-institution retrospective chart review of WHO Grade III & IV gliomas (VGH 2000-2021) showing neurologic worsening 1 month post STR (<100% resection): n=78
- Pre vs. post-op neurologic deficits and peritumoral factors
RESULTS
| Age (SD) | 57.5 (15.5) |
|
Sex
Male
Female
|
n (%)
45 (57.7)
33 (42.3)
|
|
Final Pathology
WHO Grade III
WHO Grade IV
|
n (%)
19 (24.3)
59 (75.6%)
|
|
Number of Glioma Resections
Index
2nd
3rd or Greater
|
n (%)
62 (79.5)
14 (17.9)
2 (2.5)
|
Post-op Neurologic Worsening in Major Domains
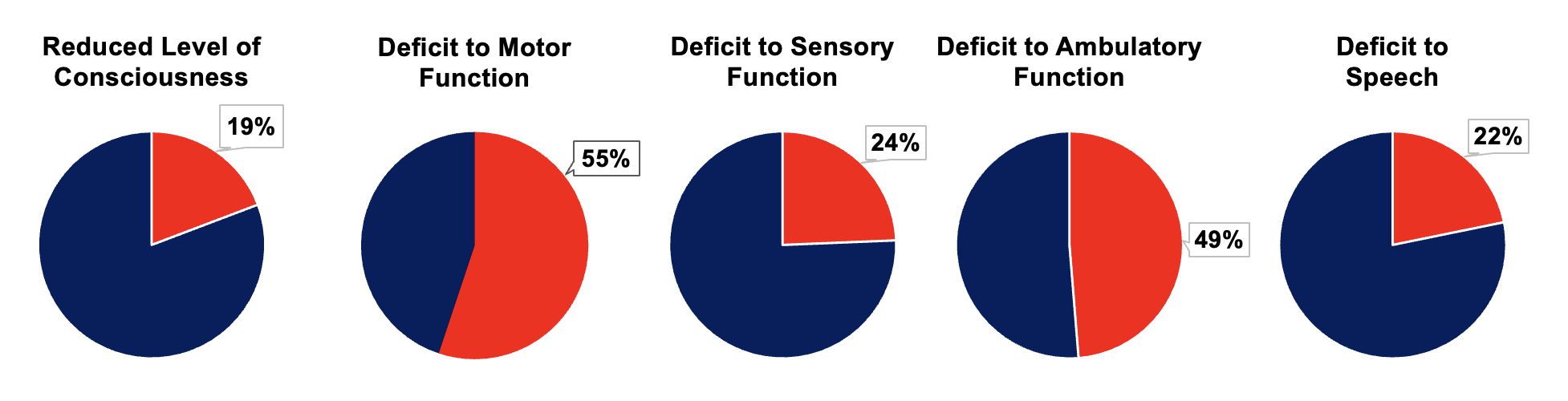
Pre vs. Post-op Peri-Tumoural Factors
| Peri-tumoural Factor (Imaging) | Pre-op n- (%) |
Post-op n - (%) |
P value (T-test, paired, one tail) |
| Enhancement | 77 (98.7) | 76 (97.8%) | 0.16 |
| Infarct* | 0 (0) | 6 (7.7) | 0.0067 |
| Hematoma* | 4 (5.1) | 22 (28.2) | 0.000032 |
| Edema* | 47 (60.3) | 69 (88.5) | 0.000013 |
| Hydrocephalus* | 1 (1.3) | 4 (5.1) | 0.042 |
| Midline Shift/Mass Effect* | 42 (53.8) | 29 (37.2) | 0.0030 |
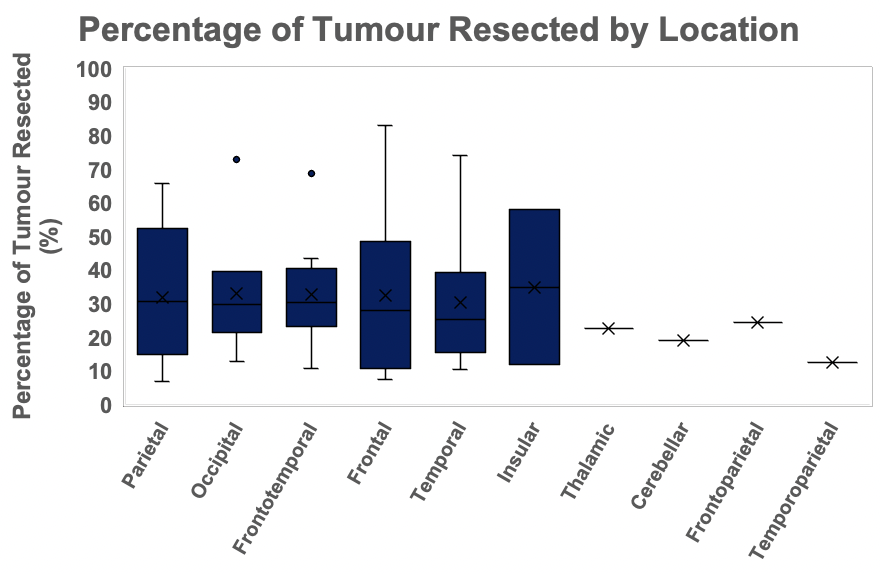
% Volume Resected in Patients with Post-op Neurologic Worsening
| Parameter | Average (SD) | Min | Max |
| Volume Resected (cm3) | 15.8 (19.2) | 0.2 | 119.5 |
| Residual Volume (cm3) | 35.7 (32.9) | 1.1 | 171.8 |
| % volume residual | 73.5 (19.7) | 17.1 | 93.0 |
| % volume resected | 26.5 (19.7)* | 7.0 | 74.2 |
DISCUSSION
- Neurologic worsening post STR, average % tumor volume resected = 26.5%
-
Our results support wounded glioma syndrome in STR:
- GBM: rapid early progression 4-6 weeks postop (OR 6.96%) [3,8]
-
Surgical disruption:
- Surgery upregulates local cerebral blood flow/edema [2], and increase blood/CSF redistribution [7,8]
- Malignant tumors are vascular; hypoxia and angiogenesis [3,4,5,6]
- Debulking tumor may increase hypercoagulability/ischemia [3]
- Microtrauma stimulates inflammation/edema [3,6]
- Limitations/Next Steps: single-centre retrospective centre,?postop imaging accounts for worsening, heterogeneous and need for matching, generalizability
CONCLUSION
- Primary Objective: % tumor volume resected via STR in patients with neurologic worsening = 26.5%
-
Secondary Objectives:
- Pre and post-op STR patients experience wide variety of neurologic deficits
- Significant worsening of post-op infarct, hematoma, edema, and hydrocephalus which may explain above
References:
[1] Nayak et al. (2017). Continuum (Minneapolis, Minn.), 23(6, Neuro-oncology) 1548–1563. [2] Calubayan & Opinaldo (2023). Neurooncol Adv 5(Suppl 3), iii26 [3] Koebbe et al. (2001). Neurosurg 48 (4): 940-944. [4] Misra et al. (1988). Surg. Neurol 29(1), 73–76. [5] Ahir et al. (2020). Mol. neurobiol 57(5), 2461–2478. [6] Fukamachi et al. (1985). Surg. neurol 23(6), 575–580. [7] Petersen et al. (2003). Anesthesiology 98(2), 329–336. [8] Girotto et al. (2023). World neurosurg 175, e738–e744.
Volumetric extent of resection and visual outcomes in pituitary adenoma patients presenting with visual compromise undergoing the endoscopic endonasal approach

BACKGROUND
- Extent of resection (EOR) reporting is not standardized in pituitary macroadenoma (PM) surgery via endoscopic endonasal approaches (EEA)
- Use of 3D volumetric analysis is proposed for accurate measurement of tumor volumes; and their association with visual outcomes was explored
METHOD
- Retrospective analysis of a single-surgeon series from 2006-2021
- Inclusion: PM patients presenting with visual compromise who underwent EEA
- HOROS software used to calculate pre- and post-operative tumor volumes
- Primary outcome: visual field (VF) and acuity (VA) at one year, assessed by licensed neuro-ophthalmologist
- Mean VF deviation of > 3 dB = improved/worse
- Change in VA = improved/worse
- Secondary outcomes: CSF leak, endocrine status, mortality, need for re-resection due to visual deterioration
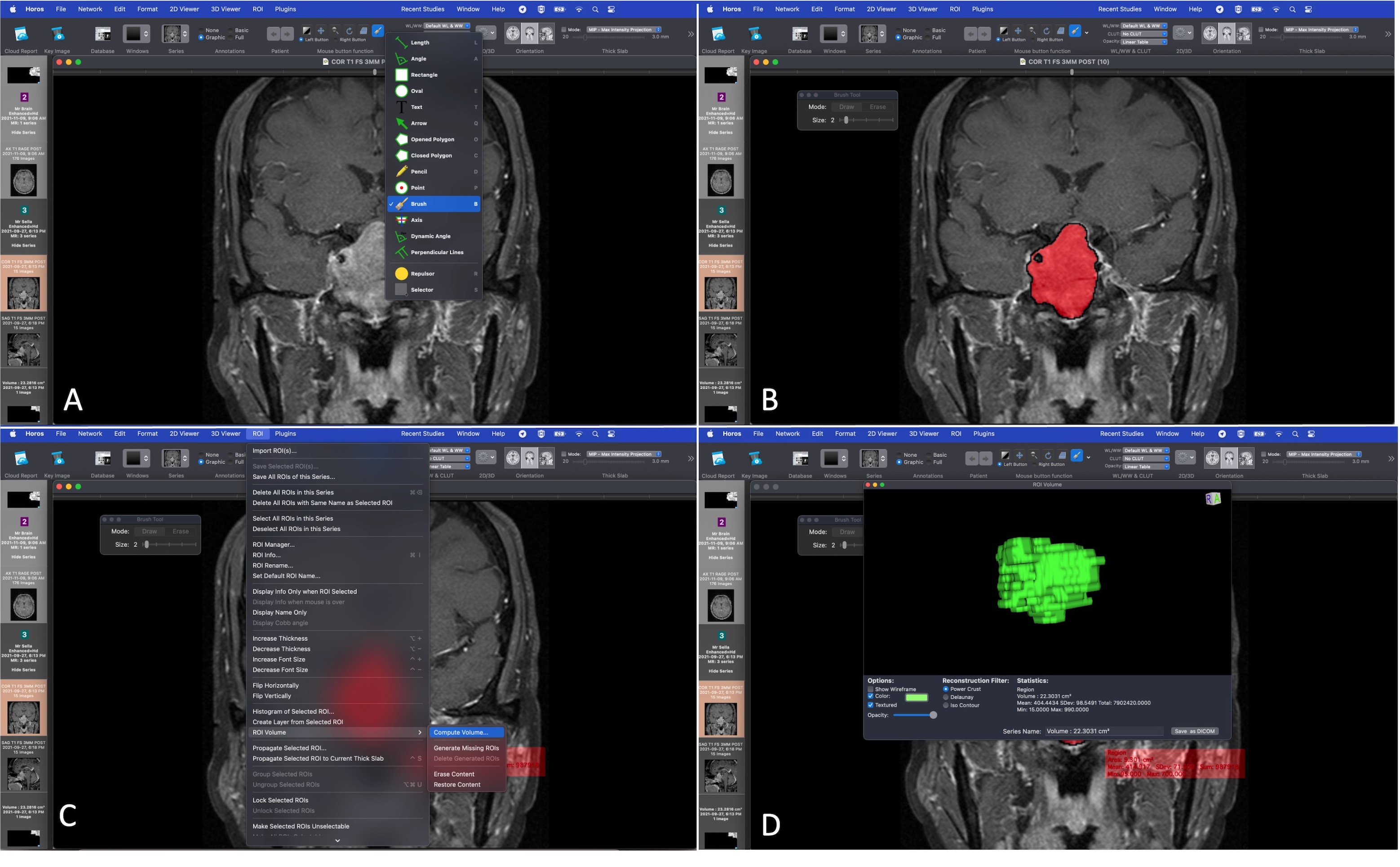
Use of HOROS software to determine tumor volumes with the "Brush" tool using different brush sizes to delineate regions of interest (tumor)
RESULTS
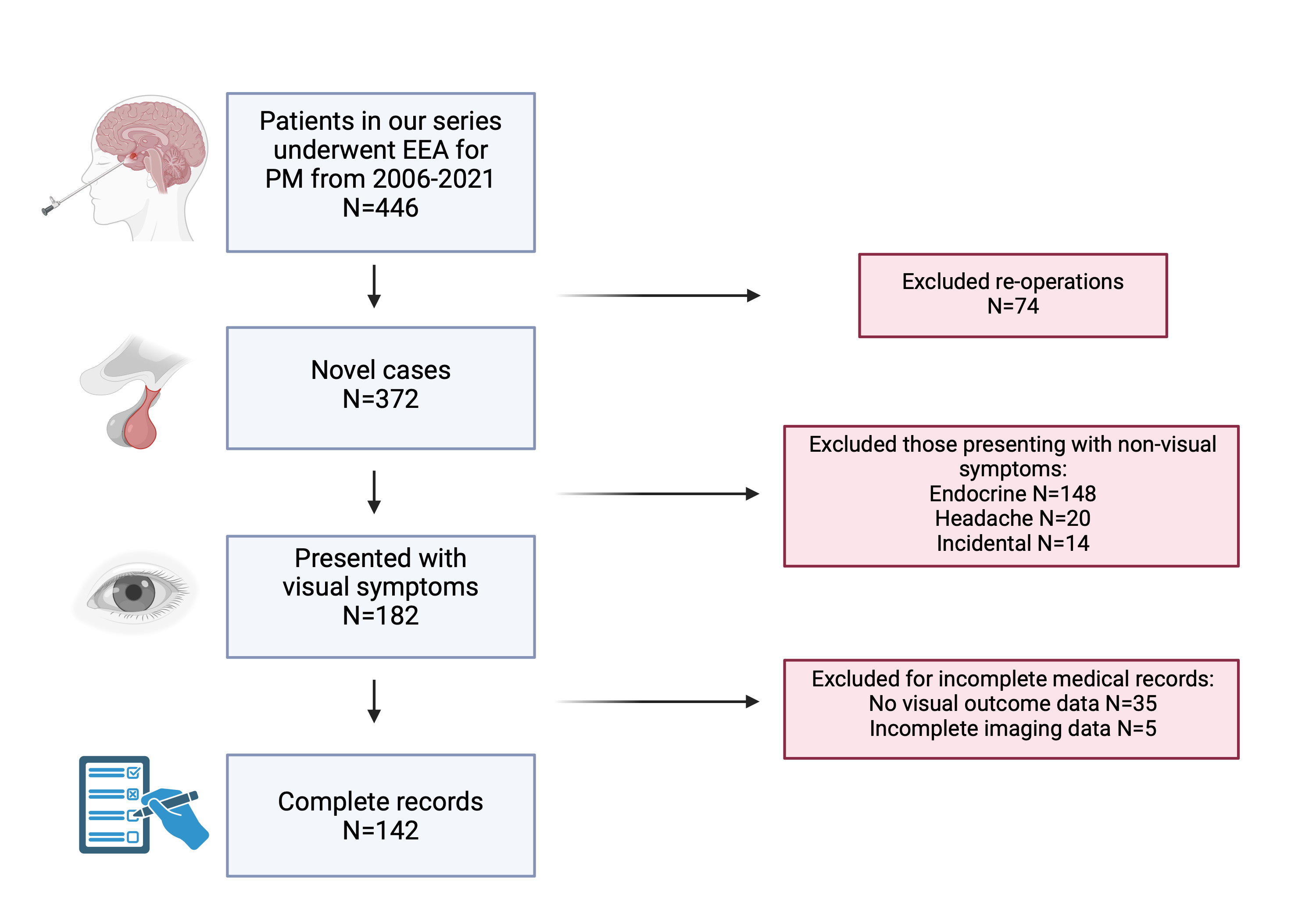
Demographics
- N = 142; Mean age: 57.1 years; Female: 33.3%; NFPA: 58.9%
- Mean suprasellar extent: 13 mm; Knosp 1 (24.1%), 2 (37.6%)
- Mean pre- vs post-op tumor size: 11.3 cm3 vs 1.9 cm3
- Mean EOR: 84.5% (range 21.5 to 99.8%)
Primary Outcomes
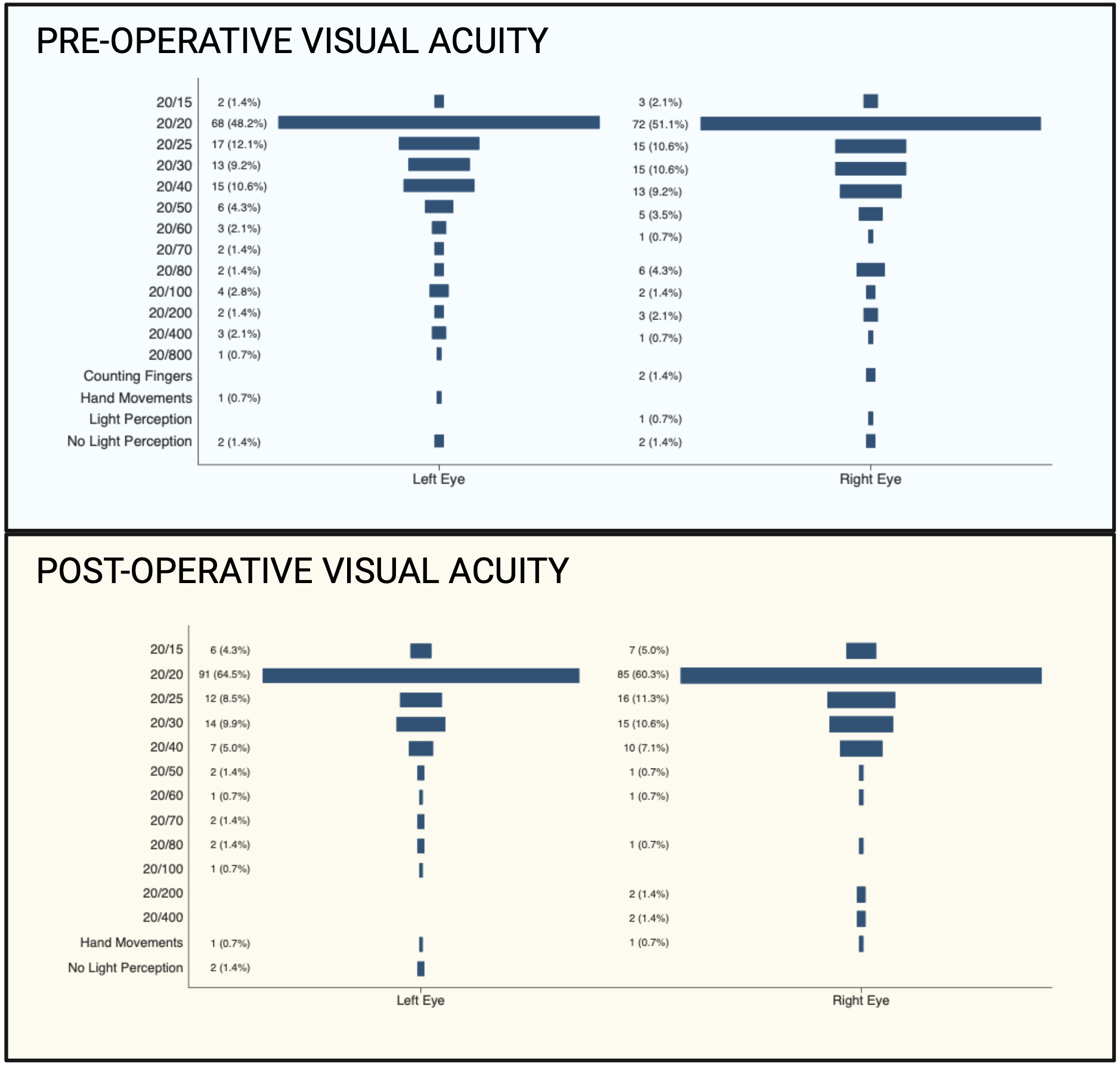
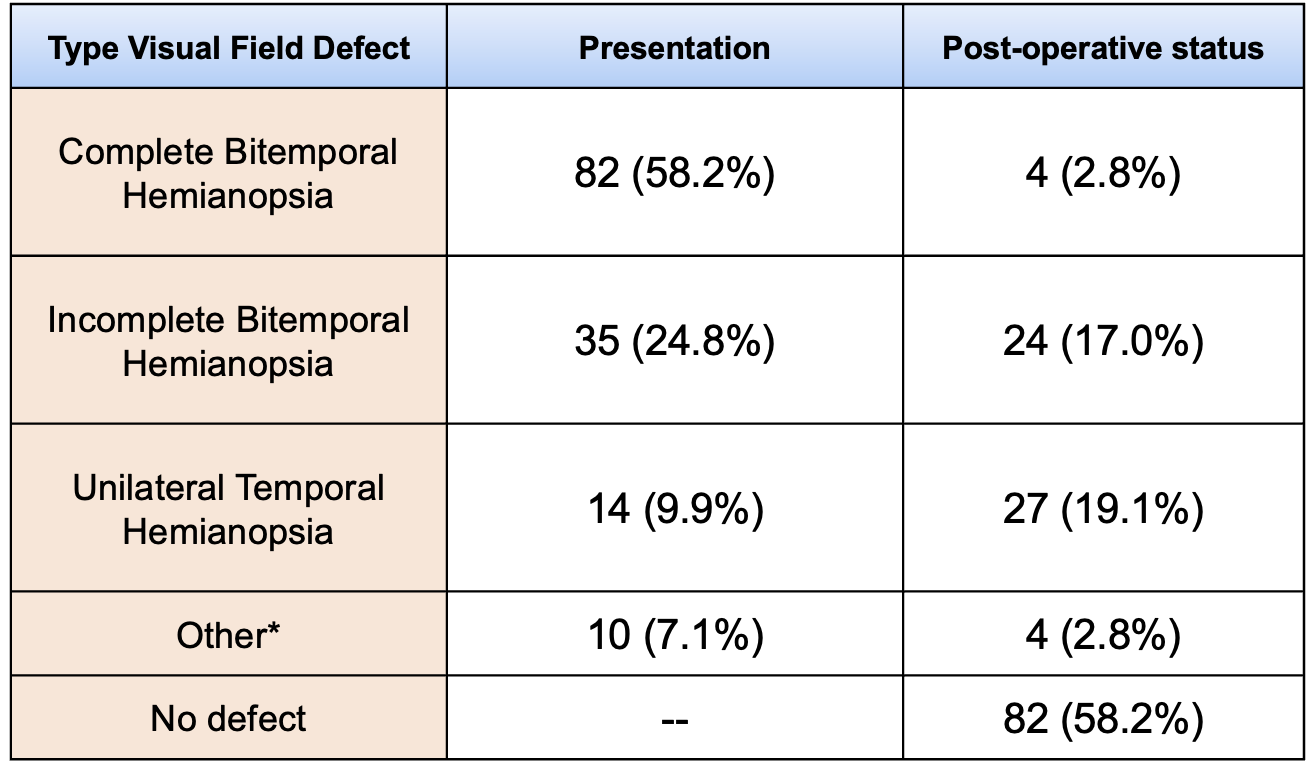
*Other visual field cuts observed: Complete unilateral nasal hemianopsia, complete homonymous hemianopsia, monocular anopsia, unilateral anopsia with incomplete contralateral anopsia
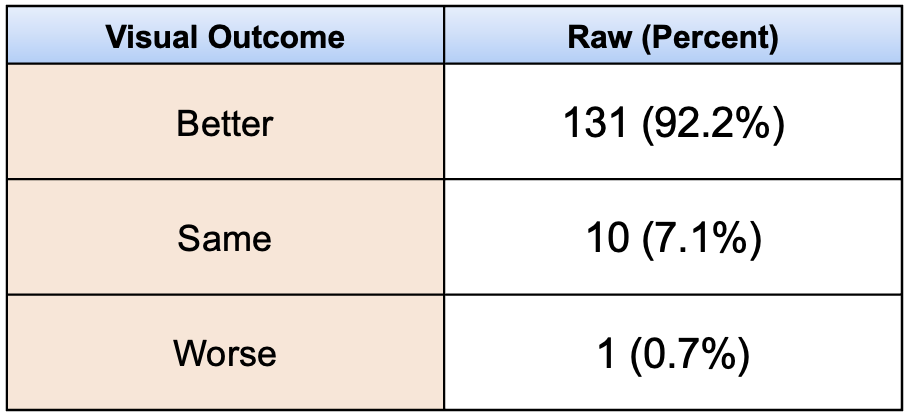
- Visual function improved in 92.2%, remained the same in 7.1%, and worsened in 0.7%
- Mean length of stay 3.7 days; Mean follow-up: 44.5 months
- CSF leak: Intraoperative = 11.3%, Post-operative=2.1%
- Endocrine: DI = 8.5%, AI = 24.1%, panhypopituitarism = 12.8%; 30-day mortality = 0
- No clinical/tumor/excision variables found to be associated with primary and secondary outcomes
- EOR was not associated with visual outcomes
- Re-resection for visual deterioration: 5.7% (8/142); mean time to re-resection: 2.4 years
- Significant association found between EOR and need for re-resection (mean EOR 66.7% vs 85.6%, p=0.002)
KEY FINDINGS
- Our findings help support the notion that maximal resective surgery need not necessarily be the goal for EEA for PM with visual compromise
- EOR was significantly associated with need for resection due to visual compromise
- Use of volumetric analysis allows more robust measurements of EOR, and in the future may allow comparison, and possibly standardization, of EOR across studies
Third ventricular pituicytoma: Case report and review of the literature
Background
Pituicytoma is a rare tumour of the sellar or suprasellar region. It is typically a well circumscribed, solid neoplasm that originates at the neurohypophysis or infundibulum. It histologically corresponds to World Health Organization (WHO) grade I1. At baseline, sellar pituicytomas are exceedingly rare, with less than 100 case reports documented since their discovery in the 1950s. Here we present a case of primarily suprasellar pituicytoma located in the third ventricle.
Clinical Presentation
A 56 year-old right hand dominant female was referred to the neurosurgery outpatient clinic with a history of menstrual cycle abnormalities, hyperprolactinemia, and progressive visual field impairment. The patient’s past medical history was pertinent for a benign cervical cyst and a breast fibroadenoma, both of which had been resected. She was otherwise healthy.
Five years prior, the patient had developed menorrhagia. Investigations revealed a mildly elevated prolactin (30ng/mL). MRI revealed a suprasellar mass, which prompted neurosurgery referral. Upon first consultation, she did not have any gross visual field deficit. The decision at this time was to repeat imaging in 6 months with clinic follow up. The repeat MRI revealed tumour growth and in the interim she had developed a new bitemporal visual field deficit. Besides bitemporal hemianopsia, which was slightly worse on the left side, neurologic examination did not reveal any other abnormalities.
Management and Outcome
The patient underwent right supra-orbital craniotomy with trans-lamina terminalis approach to resection. This approach was preferred due to less brain retraction, better access to tumour, lateral walls and floor of the third ventricle, avoiding injury to the corpus callosum, and less manipulation of the pituitary and infundibulum. Intra-operative VEP monitoring was used. A small residual was left behind due to its proximity and adherence to the hypothalamus and vasculature. Post-operatively she developed transient diabetes insipidus. Once this resolved, she had no further complications and was discharged home.
Pathology showed positive nuclear TTF-1, positive S100, and negative GFAP and EMA. Final pathology reported WHO grade 1 pituicytoma. Due to the small amount of residual, she recieved stereotactic radiosurgery. Follow up imaging has shown disease stability and she continues to be managed by endocrinology for central hypothyroidism and adrenal insufficiency.
Imaging
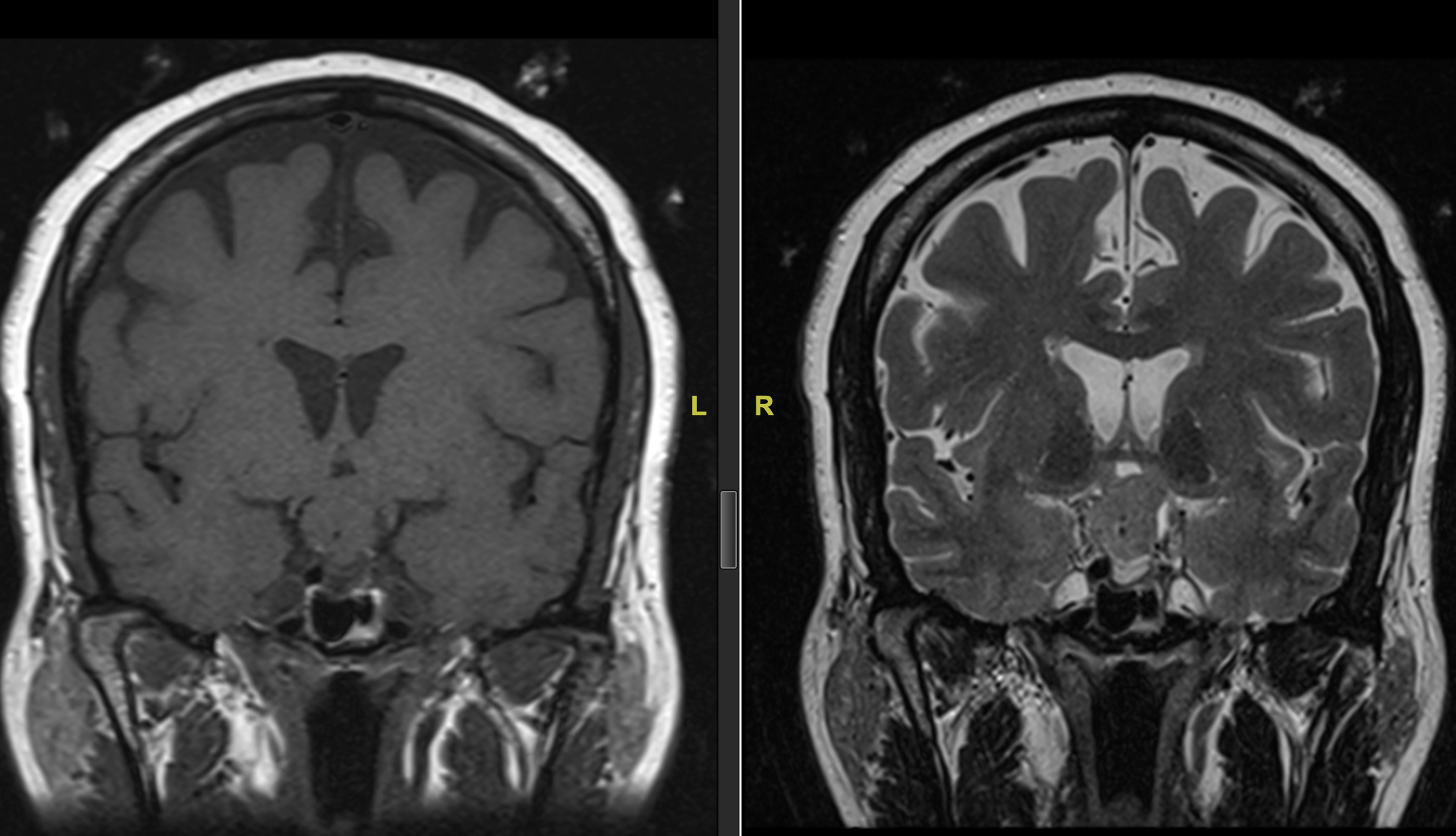
Figure 1. Coronal T1 and T2 MRI without contrast of suprasellar lesion.
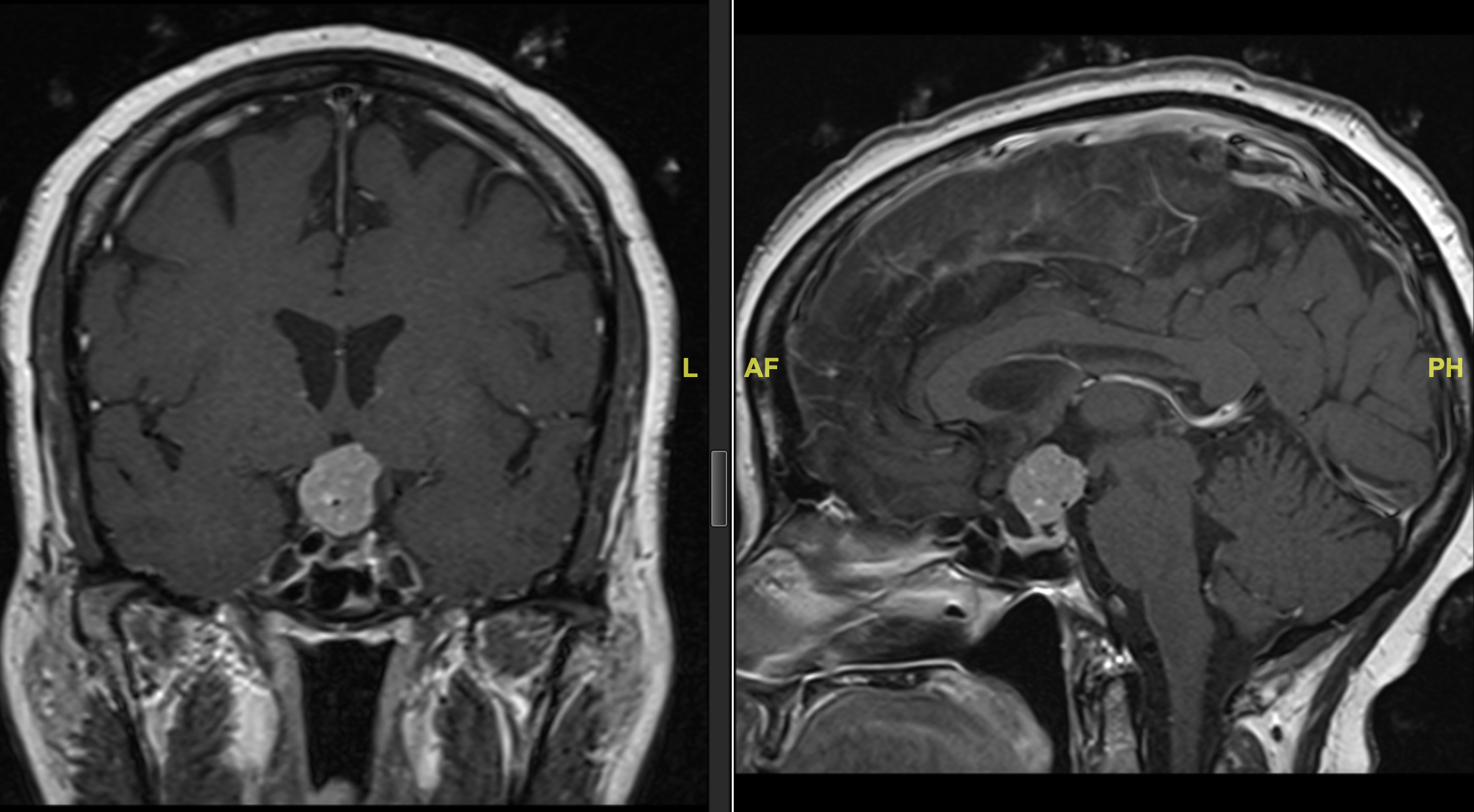
Figure 2. Coronal and sagittal views of contrast enhanced MRI images of suprasellar/third ventricular lesion.
MRI brain showed a 2.1 cm avidly enhancing mass at the base of the infundibulum, protruding into the anterior and inferior third ventricle, separate from the pituitary gland. The lesion is in close proximity to bilateral A1 and supraclinoid ICA. It appears vascular with prominent flow voids. Initial differential included glioma, craniopharyngioma, meningioma and lymphoma. It doesn't arise from the posterior pituitary which would typically suggest pituicytoma.
Discussion
Pituicytoma is a rare entity, our knowledge of which is based primarily on case reports or series. The term pituicytoma has been used in the past to describe a variety of different pathologies2. The definition has metamorphosized over the years, until the 2007 WHO classification formally recognized pituicytoma as its own unique entity. It is classically described as a well-circumscribed, WHO grade I tumour arising from pituicytes of the neurohypophysis or infundibulum. Due to its rarity, epidemiologic data is not available, however it generally occurs in the 5th or 6th decade and is slightly more common in males3.
Pituicytomas are predominantly sellar or suprasellar and can be difficult to discern from other sellar pathologies. In the current case, the lesion was predominantly third ventricular and appeared to extend from the base of the infundibulum rather than the entire infundibulum or neurohypophysis. For this reason, pituicytoma was not particularly high on the differential and was a surprising pathology result.
Classically, pituicytoma arises from glial cells in the neurohypophysis called pituicytes. Microscopically it is composed almost entirely of bipolar spindle cells arranged in interlacing fascicles or storiform pattern. Immunohistochemical staining reveals high reactivity of S-100 and vimentin and diffusely positive nuclear staining for TTF-1. Surgical resection is the mainstay of treatment, though radiation can be considered in the event of residual tumour, as we described.
Due to the rarity of pituicytoma overall, our education on this pathology relies heavily on case reporting, particularly of unique presentations. Our case describes the presentation, imaging and surgical approach to a unique presentation of third ventricular pituicytoma.
References
1. Louis DN, et al. (2021). The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 23(8):1231-1251
2. Salge-Arrieta FJ, et al. (2019). Clinical features, diagnosis and therapy of pituicytoma: an update. J Endocrin Inv., 42(4), 371–384
3. Chen B, Fan X, & Zhang Z (2021). Pituicytoma: Report of three cases and a systematic literature review. Clin Neurol Neurosurg, 205
3. Chen B, Fan X, & Zhang Z (2021). Pituicytoma: Report of three cases and a systematic literature review. Clin Neurol Neurosurg, 205
Synthetic data reliably reproduces brain tumor primary research data
Background
Synthetic data have garnered heightened attention in contemporary research due to confidentiality barriers and its capacity to simulate variables challenging to obtain. This study aimed to evaluate the reliability and validity of synthetic data in the context of neuro-oncology research, comparing findings from two published studies with results from synthetic datasets.
Methods
Two seminal neuro-oncology studies focusing on prognostic factors such as serum albumin and systemic inflammation scores were selected, and their methodologies were replicated using MDClone platform to generate five synthetic datasets for each. MDClone is a healthcare data exploration tool that enables the creation of synthetic data that replicate the statistical characteristics and correlations of real-world data. We used Chi-Square test to assess inter-variability between synthetic datasets. Survival outcomes were evaluated using Kaplan-Meier, and T-test was used to determine statistical significance.
Results
Methods
Two seminal neuro-oncology studies focusing on prognostic factors such as serum albumin and systemic inflammation scores were selected, and their methodologies were replicated using MDClone platform to generate five synthetic datasets for each. MDClone is a healthcare data exploration tool that enables the creation of synthetic data that replicate the statistical characteristics and correlations of real-world data. We used Chi-Square test to assess inter-variability between synthetic datasets. Survival outcomes were evaluated using Kaplan-Meier, and T-test was used to determine statistical significance.
Findings from synthetic data consistently reflected outcomes from both original articles, with serum albumin and systemic inflammation scores correlating with survival prognosis in glioblastoma and metastasis patients. Reported findings, demographic trends and survival outcomes showed similarity with synthetic datasets.
Conclusion
Synthetic data consistently reproduced the statistical attributes of real patient data. Integrating synthetic data into clinical research offers excellent potential for providing accurate predictive insights without compromising patient privacy. In neuro-oncology, where patient follow-up pose challenges, the adoption of synthetic datasets can be transformative.
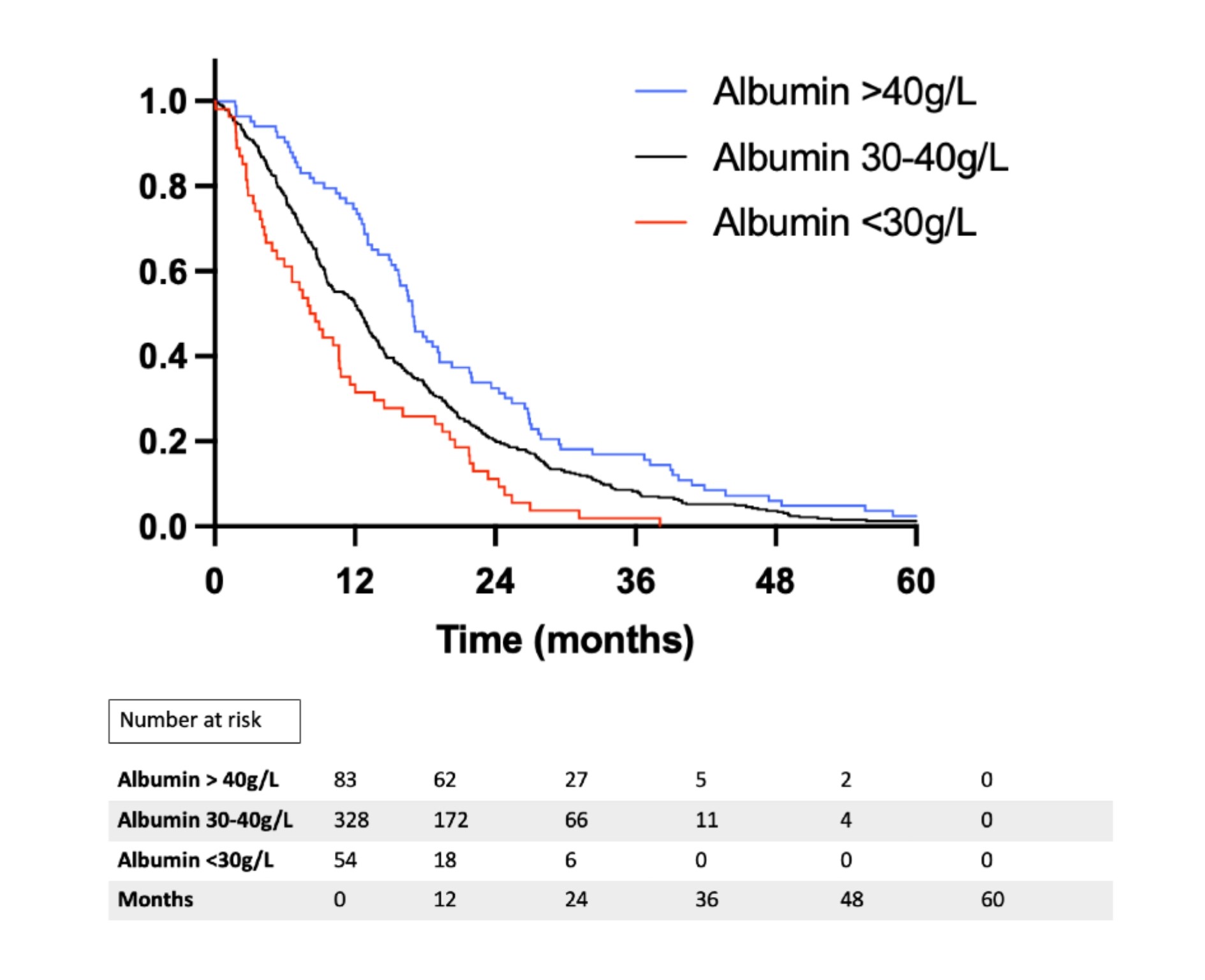
Figure 1. Kaplan-Meier survival curve of the synthetic dataset cohort subdivided into three categories:
Hypoalbuminemic (red-lined, Albumin <30g/L, median=7.0 months), lower-normal serum albumin (black-lined, Albumin 30-40g/L, median=12.9 months) and upper-normal serum albumin (blue-lined, Albumin >40g/L, median=16.2 months) (Log-rank P<0.001).
Hypoalbuminemic (red-lined, Albumin <30g/L, median=7.0 months), lower-normal serum albumin (black-lined, Albumin 30-40g/L, median=12.9 months) and upper-normal serum albumin (blue-lined, Albumin >40g/L, median=16.2 months) (Log-rank P<0.001).

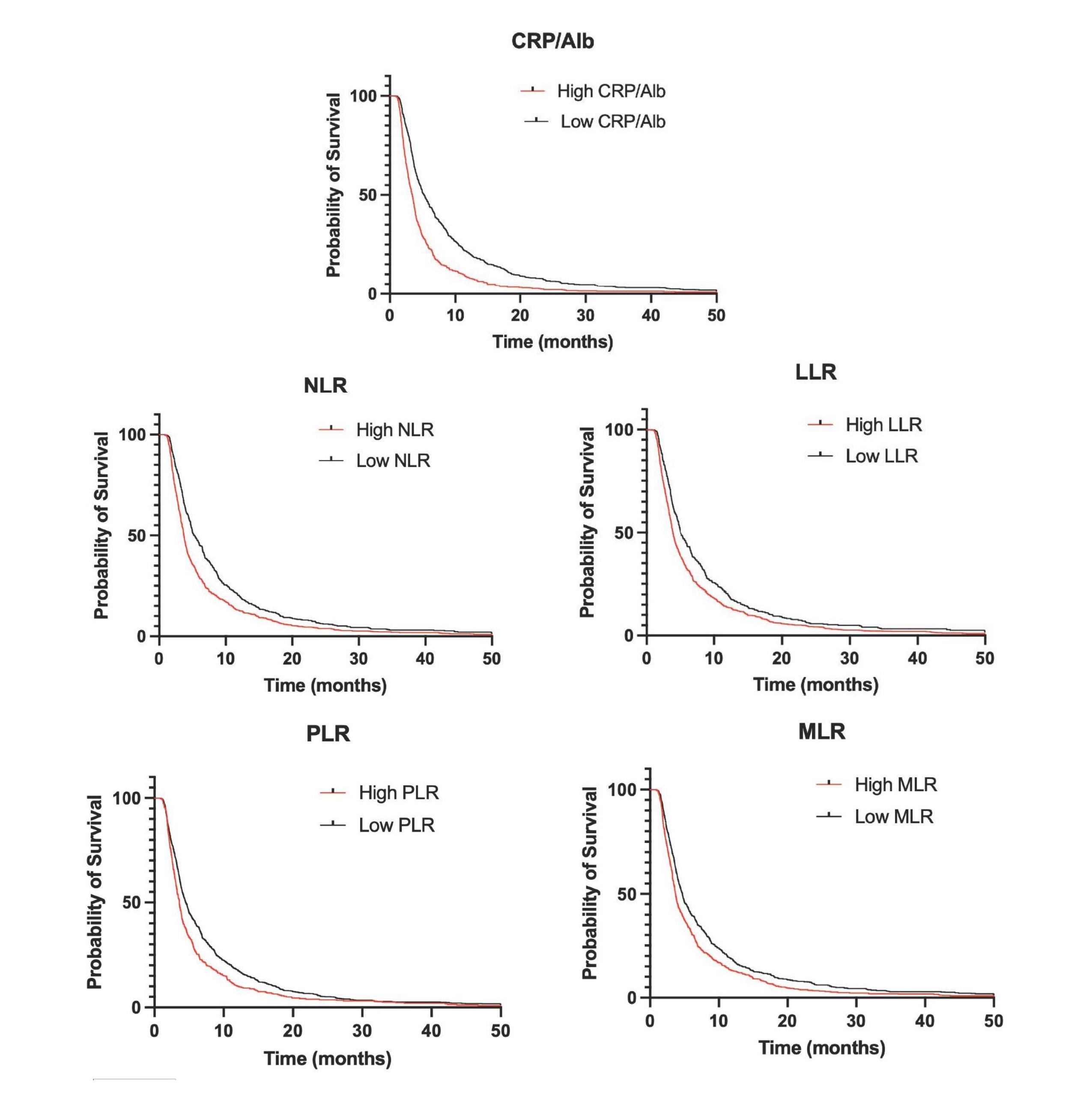
Figure 2. Kaplan-Meier survival curves of the primary synthetic dataset of patients with brain metastasis depending on level of serum inflammatory markers.
A) Compares high CRP/Alb with low serum CRP/Alb (median survival 3.4 vs 5.2 months, mean of differences 3.5 [95% CI 2.5-4.5], P<0.0001).
B) Compares high NLR with low NLR (median survival 3.7 vs 5.1 months, mean of differences 2.2 [95% CI 1.0-3.4], P=0.0004).
C) Compares high LLR with low LLR (median survival 3.8 vs. 5.1 months, mean of differences 2.5 [95% CI 1.1-3.8], P=0.0003).
D) Compares high PLR with low PLR (median survival 3.6 vs 4.7 months, mean of differences 1.3 [95% CI 0.07-2.7], P=0.04).
E) Compares high MLR with low MLR (median survival 3.7 vs 4.7 months, mean of differences 1.6 [95% CI 0.6-2.7], P=0.002).
A) Compares high CRP/Alb with low serum CRP/Alb (median survival 3.4 vs 5.2 months, mean of differences 3.5 [95% CI 2.5-4.5], P<0.0001).
B) Compares high NLR with low NLR (median survival 3.7 vs 5.1 months, mean of differences 2.2 [95% CI 1.0-3.4], P=0.0004).
C) Compares high LLR with low LLR (median survival 3.8 vs. 5.1 months, mean of differences 2.5 [95% CI 1.1-3.8], P=0.0003).
D) Compares high PLR with low PLR (median survival 3.6 vs 4.7 months, mean of differences 1.3 [95% CI 0.07-2.7], P=0.04).
E) Compares high MLR with low MLR (median survival 3.7 vs 4.7 months, mean of differences 1.6 [95% CI 0.6-2.7], P=0.002).
Acknowledgments
We would like to acknowledge Santiago Marquez Fosser for facilitating access to the MDClone platform and Lena Zack for their assistance during its utilization.
Incidence of tissue-sampled brain metastases pre- and post-COVID-19 in Newfoundland and Labrador: an eight-year review
Background
The COVID-19 pandemic had several impacts on cancer care, including increased wait times, decreased screening, decreased oncologic surgeries, and higher stage of tumours at presentation and diagnosis.1-3
Objectives
- Assess whether COVID-19 had an impact on the incidence of histologically diagnosed brain metastases in Newfoundland & Labrador.
- Compare incidence rates from different primary tumour locations (e.g., lung, breast) before and after COVID-19.
- Compare incidence rates across regions within the province.
Methods
We queried Meditech for all pathology reports relating to brain tumours between 2015-2022. Three authors (LB, AK, TN) reviewed all the resultant pathology reports. Cases included:
aUsed as a proxy to exclude presumed recurrent cases
- Histologically confirmed metastatic brain tumours. Cases with unknown or uncertain primary locations were included (labelled as “other” compared to known locations).
- First instances of a particular tumour type for each patienta
- Adult cases (pediatric cases were excluded)
aUsed as a proxy to exclude presumed recurrent cases
References
- Boire A, Brastianos PK, Garzia L, Valiente M. Brain metastasis. Nat Rev Cancer. 2020;20(1):4-11. doi:10.1038/s41568-019-0220-y
- Englum BR, Prasad NK, Lake RE, et al. Impact of the COVID-19 pandemic on diagnosis of new cancers: A national multicenter study of the Veterans Affairs Healthcare System. Cancer. 2022;128(5):1048-1056. doi:10.1002/cncr.34011
- Heer E, Ruan Y, Boyne DJ, et al. Impact of the COVID-19 pandemic on cancer diagnoses, stage and survival in Alberta. CMAJ. 2023;195(23):E804-E812. doi:10.1503/cmaj.221512
Case characteristics
We included 173 cases in which a histological diagnosis was made between 2015-2022:
| Cases, total | 173 |
| Cases, male | 75 |
| Cases, female | 98 |
| Median age at the time of diagnosis (range) | 66 (26-85) |
_
_
_
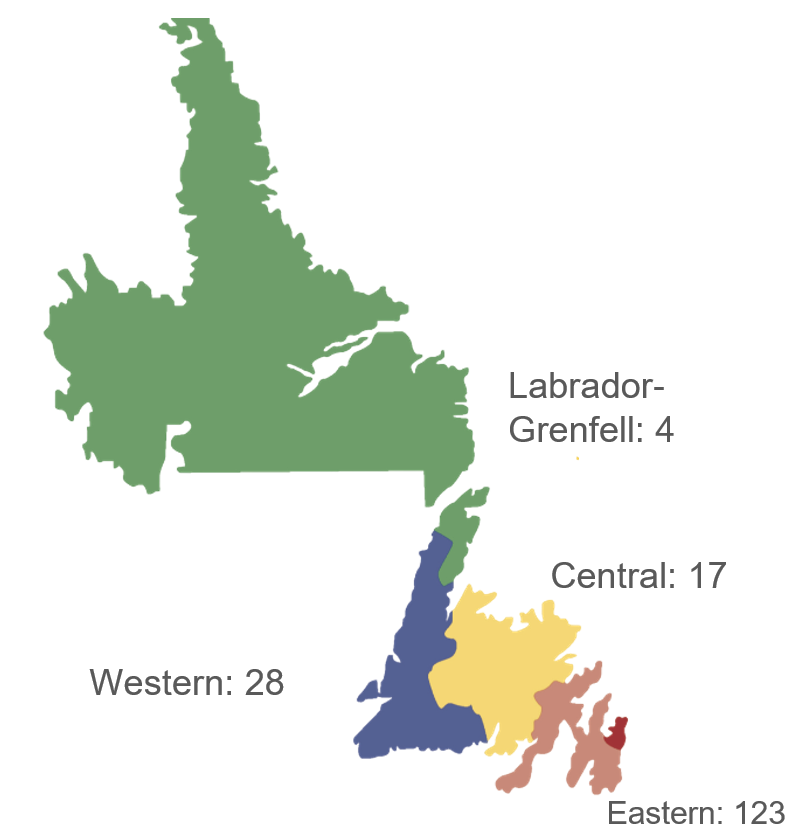
Brain metastasis cases by region
Regions defined by jurisdiction of regional health authorities
Regions defined by jurisdiction of regional health authorities

Case incidence by brain tumour location
Error bars represent the 95% confidence interval
Error bars represent the 95% confidence interval
Overall case incidence pre- and post-COVID-19
The average annual age-standardized incidence rate of brain metastases requiring tissue sampling per 100,000 increased from 2.5 (95% CI: 2.0-3.1) pre-COVID-19 to 4.1 (95% CI: 3.3-5.0) post-COVID-19. Brain metastases from lung primaries accounted for 69% of this increase.
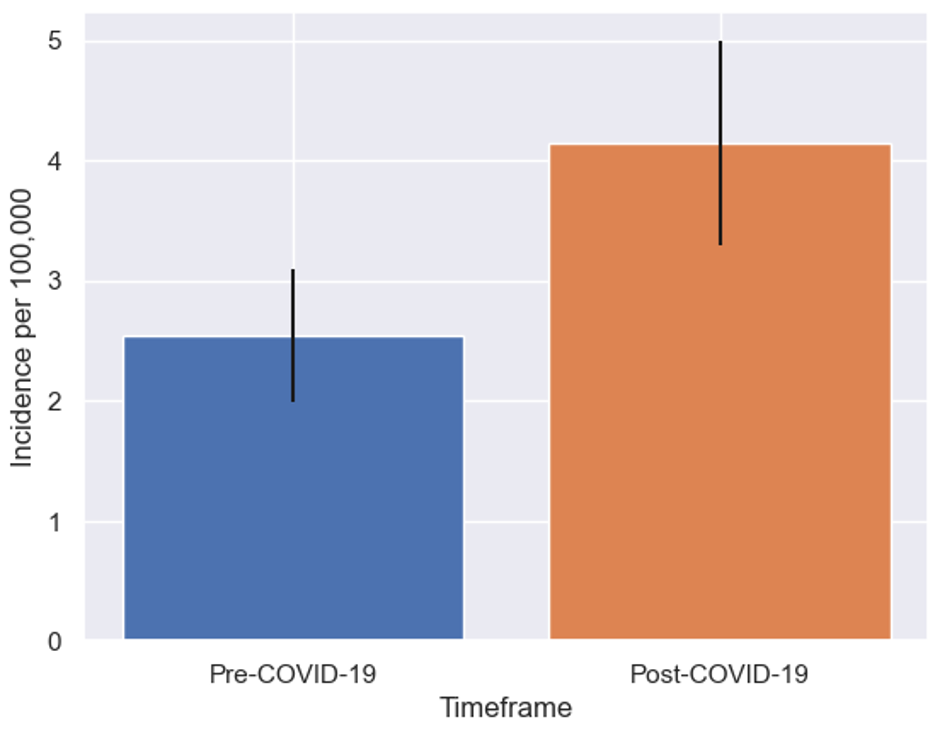
Overall case incidence pre- and post-COVID-19
Error bars represent the 95% confidence interval
Error bars represent the 95% confidence interval
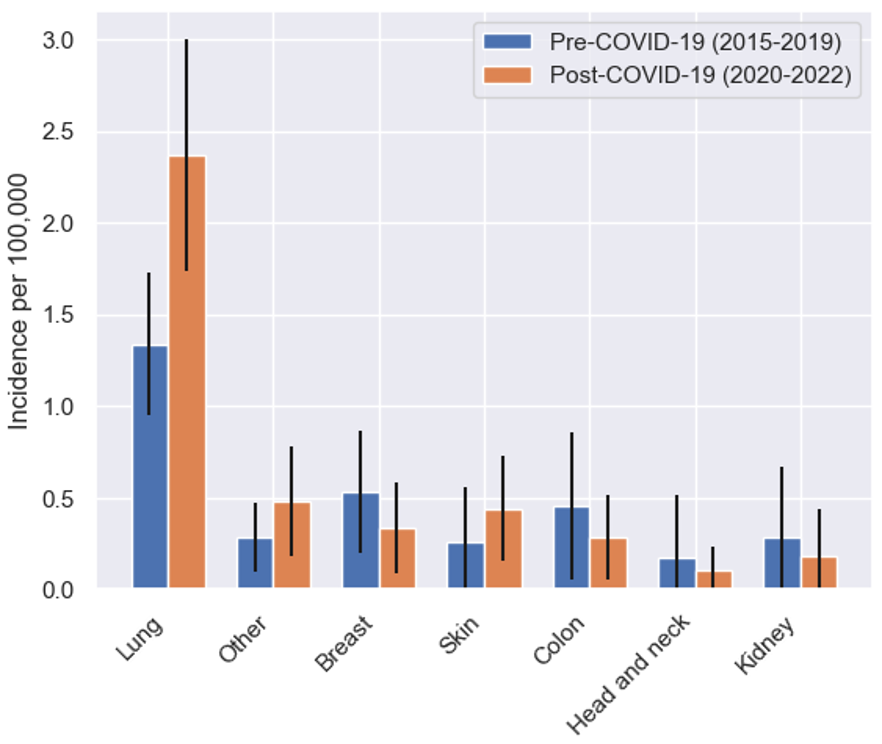
Case incidence by primary tumour location, pre- and post-COVID-19
Error bars represent the 95% confidence interval.
Error bars represent the 95% confidence interval.
Regional trends
Eastern and Western health authorities saw spikes in brain metastases during and after the COVID-19 pandemic. Incidence declined to near-baseline in the Eastern provincial population by 2022 (3.3; 95% CI: 1.5-5.1). Meanwhile, incidence rose into 2022 in the Western population (8.6 per 100,000; 95% CI: 3.9-13.2).
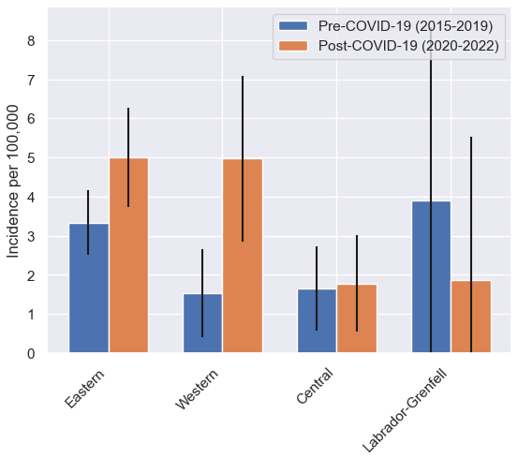
Case incidence by region, pre- and post-COVID-19
Error bars represent the 95% confidence interval
Error bars represent the 95% confidence interval
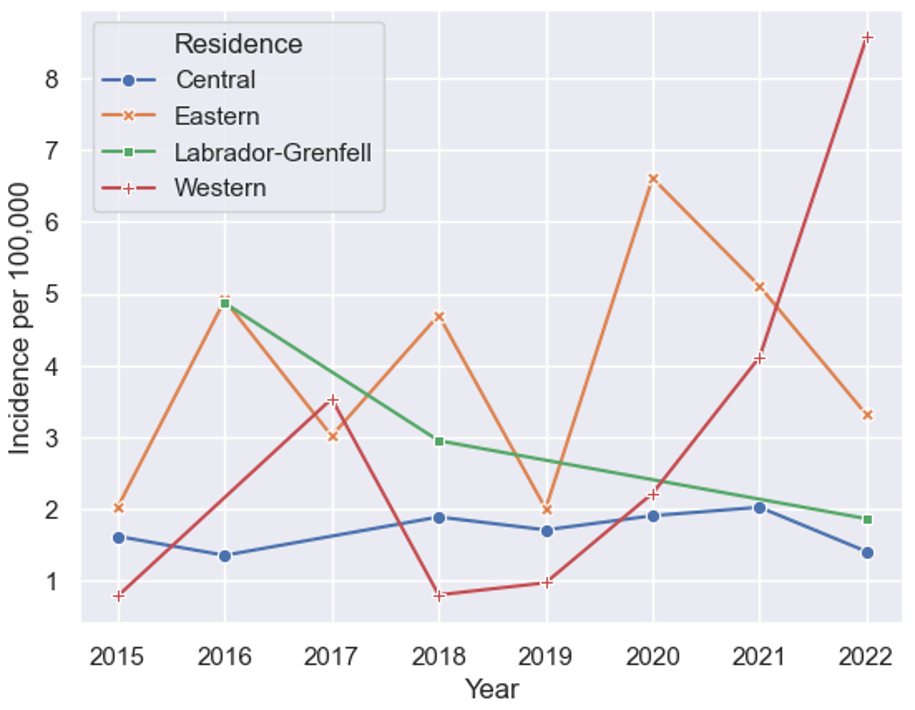
Temporal case incidence trend by region, 2015-2022
Conclusions
These data suggest a delayed presentation of malignancies during the COVID-19 pandemic and underscore the importance of screening, surveillance, and treatment during times of strain on healthcare systems. Regional, temporal trends suggest regions distant from tertiary care centres could face challenges in resolving cases with delayed presentation post-COVID-19.
Incidence of pathologically confirmed primary malignant brain tumours in Newfoundland and Labrador: an eight-year review spanning 2015-2022
Background
Newfoundland & Labrador (NL) has some of the highest cancer incidence rates in Canada, with unique genetics playing a predisposing role. The incidence of primary, malignant brain tumours in NL hasn’t been quantified since 2017.1
Objectives
- Quantify the incidence of histologically confirmed primary, malignant brain tumour subtypes in NL from 2015-2022, comparing to the most recent national figures.
- Compare incidence rates across regions within the province.
- Investigate incidence trends over time, paying particular attention to the advent of the COVID-19 pandemic from 2020-2022.
Methods
We queried Meditech for all pathology reports relating to brain tumours between 2015-2022. Three authors (LB, AK, TN) reviewed all the resultant pathology reports. Cases included:
aClassification system used by the Brain Tumour Registry of Canada1
bUsed as a proxy to exclude presumed recurrent cases
- Primary (i.e., non-metastatic), malignant brain tumours, as defined by the Central Brain Tumour Registry of the U.S.a
- First instances of a particular tumour type for each patientb
- Adult cases (pediatric cases were excluded)
aClassification system used by the Brain Tumour Registry of Canada1
bUsed as a proxy to exclude presumed recurrent cases
Case characteristics
We included 362 cases in which a histological diagnosis was made between 2015-2022:
| Cases, total | 362 |
|---|---|
| Cases, male | 199 |
| Cases, female | 163 |
| Median age at the time of diagnosis (range) | 62 (19-87) |
Sex difference consistent with known higher incidences of primary, malignant brain tumours in males1
Regional trend: low incidence rates in Labrador-Grenfell
The overall incidence of histologically confirmed primary, malignant brain tumours in the Labrador-Grenfell region was 5.1 per 100,000 (95% CI: 2.5-7.6), compared to 6.9 (95% CI: 6.2-7.6) averaged elsewhere. While this difference could indicate a true discrepancy in underlying incidence between Labrador-Grenfell and the rest of the province, it may also indicate undersampling due to decreased access to neurosurgical care.
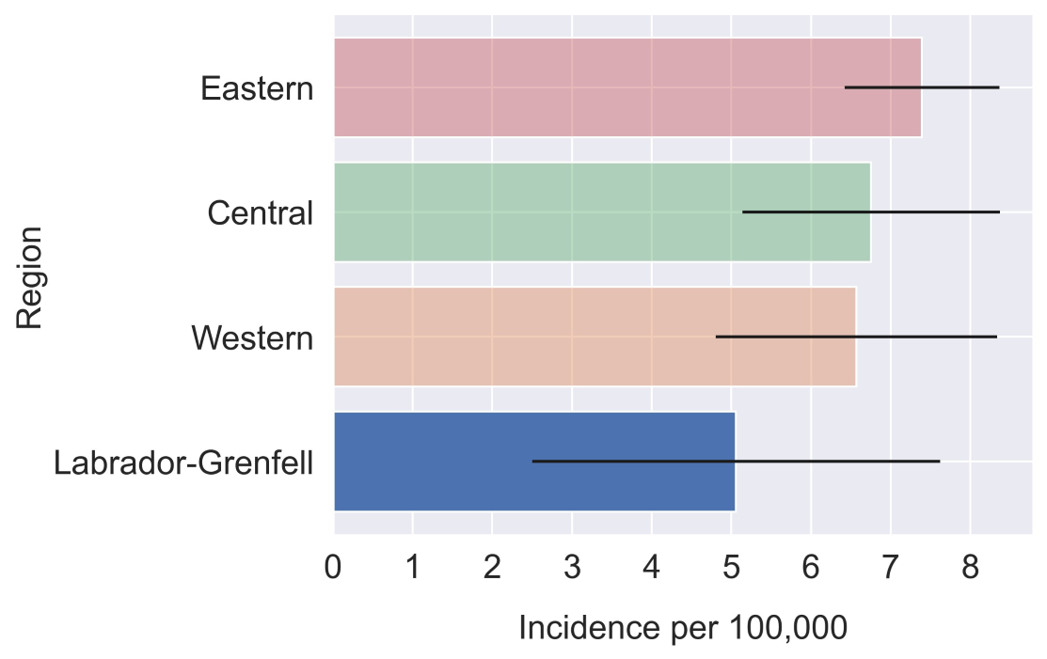
Regional incidence of primary, malignant brain tumours in Newfoundland & Labrador
Error bars represent the 95% confidence interval.
Error bars represent the 95% confidence interval.
NL has the highest rates of glioblastoma, nationally
Glioblastoma is the most common & aggressive primary, malignant brain tumour. The current incidence in NL is 5.1 (95% CI: 4.5-5.7), compared to the most recent national average of 4.05 (95% CI: 3.95-4.16).
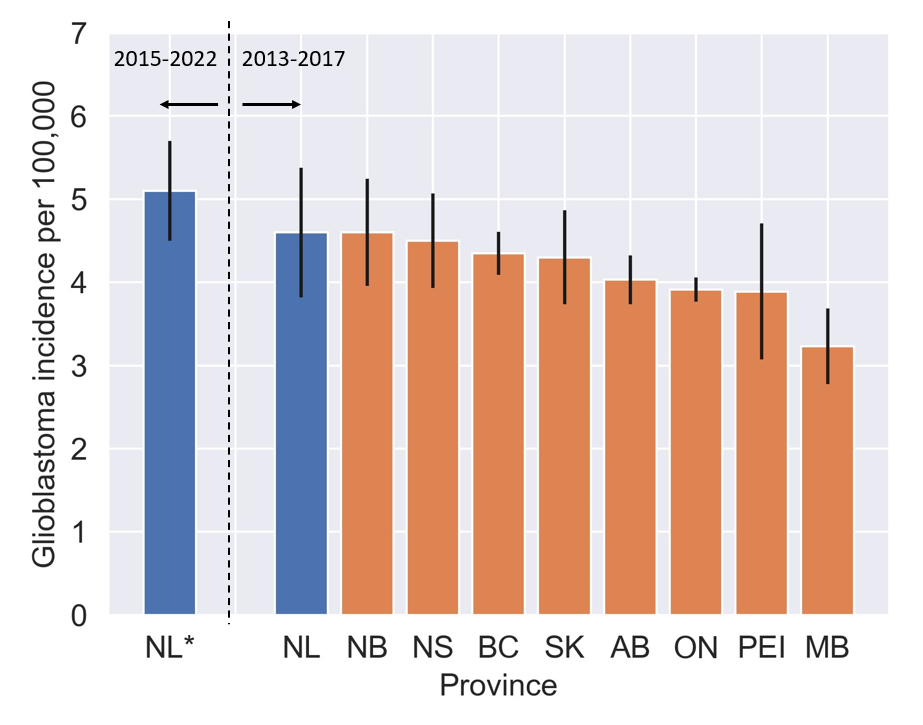
Glioblastoma incidence by province
NL* represents our data; data to the right of the dashed line is from the Brain Tumour Registry of Canada Incidence Report.1
NL* represents our data; data to the right of the dashed line is from the Brain Tumour Registry of Canada Incidence Report.1
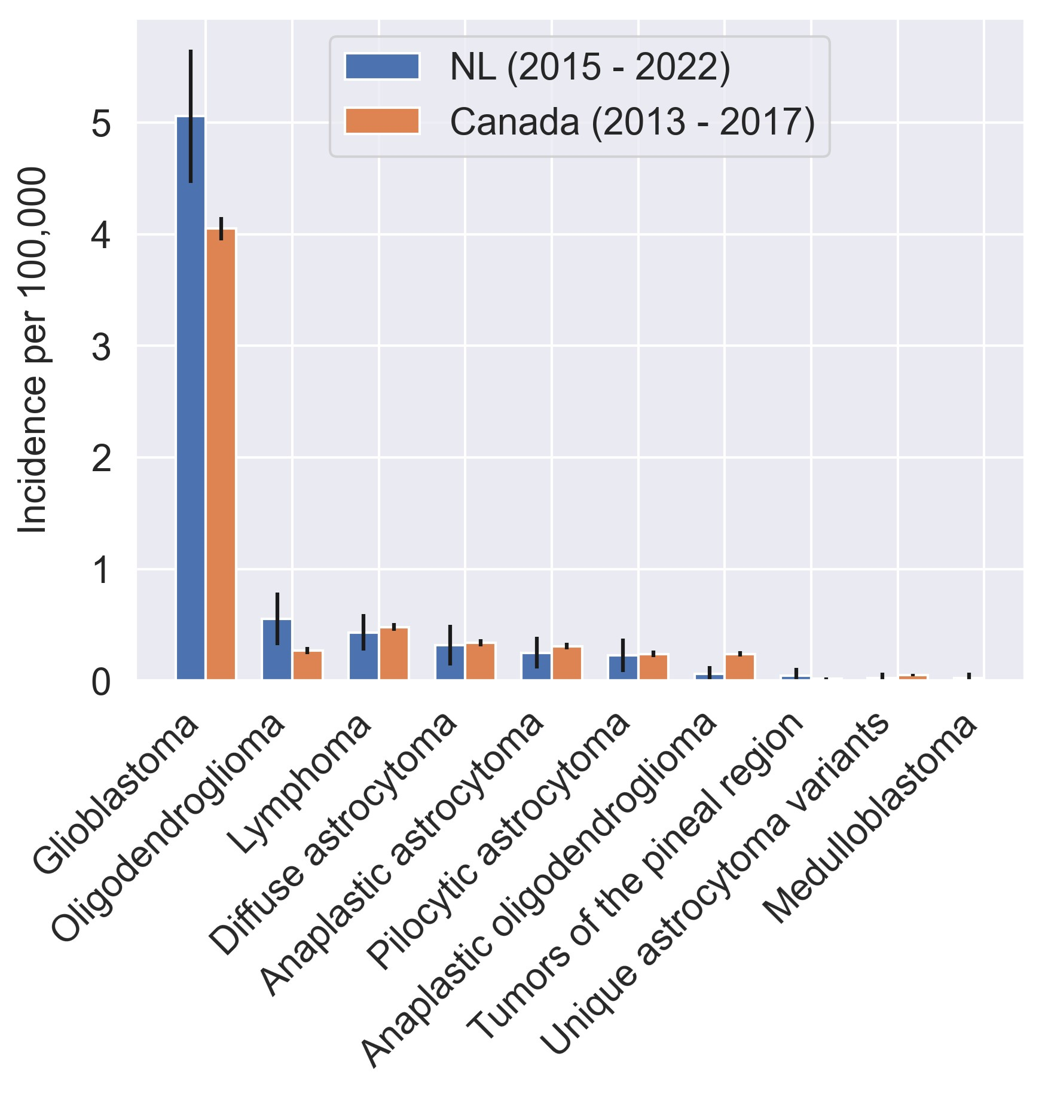
Incidence of all primary, malignant tumour subtypes in NL vs. Canadian average
Error bars represent the 95% confidence interval
Error bars represent the 95% confidence interval
A surge in oligodendroglioma cases accompanied COVID-19
The incidence of oligodendroglioma (ODG), a rare tumour derived from oligodendrocytes, jumped from 0.5 (95% CI: 0.2-0.7) in 2015-2019 to 1.5 (95% CI: 0.4-2.6) in 2020 during the COVID-19 pandemic. Weak evidence exists for a viral cause of ODG2, making this an interesting finding; however, low case numbers, high variability, and the effects of COVID-19 on illness presentation urge cautious interpretation.
Incidence over time for the three most common primary, malignant tumour subtypes
Error bands represent the standard error
Error bands represent the standard error
Conclusions
Regional trends could suggest less access to care in remote populations and underestimated incidence. High rates of glioblastoma in NL could have a genetic or multi-factorial cause. The increased occurrence of ODG during the COVID-19 pandemic necessities broader investigation.
BMI as a predictor of recurrence in high-grade meningioma: A single center retrospective cohort study

Abstract
Methods: This is a retrospective cohort study of patients with Grade 2 or Grade 3 meningioma at a single tertiary case center between 2008 and 2017. We collected clinical data including age, sex, BMI, anatomic location, Simpson grade, brain invasion, and radiation treatments. Disease control was monitored on follow up MRI scans. We stratified patients by greater than or less than 25.
Results: A total of 45 patients were included. Recurrence was observed in 15 patients (33.3%). There were 32 (71.1%) patients with BMI > 25 and 13 (28.9%) patients with normal BMI. Patients with elevated BMI had higher risk of recurrence (p=0.04). Multivariate analysis identified BMI as an independent predictor of recurrence.
Conclusions: Our results suggest that overweight patients with a Grade 2 or Grade 3 meningioma are at higher risk of recurrence than patients with normal BMI. The explanation for this association is unknown. Further research is suggested to confirm and better characterize this association.
Introduction
Meningiomas are the most common primary brain tumor, accounting for approximately one-third of all primary central nervous system tumors1. Most meningiomas are benign (WHO grade 1). However, up to 25% of all meningiomas are considered atypical (WHO grade 2) or malignant (WHO grade 3). Notably, the WHO classification of meningiomas was revised in 2021.
Complete surgical resection is desirable in the treatment of meningioma when indicated, as it can be curative. Despite this, recurrence is common, especially in Grade 2 and Grade 3 lesions2.
In addition to surgical resection, adjuvant treatment with radiotherapy is effective in the management of meningioma2. Various scoring systems have been developed to help predict the likelihood of recurrence, assessing Simpson grade, WHO grade, and methylation profiles3,4. To date, BMI has not yet been investigated as risk factor for meningioma recurrence in Grade 2- or 3- lesions.
Complete surgical resection is desirable in the treatment of meningioma when indicated, as it can be curative. Despite this, recurrence is common, especially in Grade 2 and Grade 3 lesions2.
In addition to surgical resection, adjuvant treatment with radiotherapy is effective in the management of meningioma2. Various scoring systems have been developed to help predict the likelihood of recurrence, assessing Simpson grade, WHO grade, and methylation profiles3,4. To date, BMI has not yet been investigated as risk factor for meningioma recurrence in Grade 2- or 3- lesions.
Methods and Materials
- Retrospective cohort study of patients with Grade 2 or Grade 3 meningioma at a single tertiary care center between 2008 and 2017.
- Combination of paper charts, electronic medical records and our local picture archiving and communication software to collect clinical data
- Stratified patients by BMI greater than or less than 25.
- Statistical analysis
- Combination of paper charts, electronic medical records and our local picture archiving and communication software to collect clinical data
- Stratified patients by BMI greater than or less than 25.
- Statistical analysis
Results
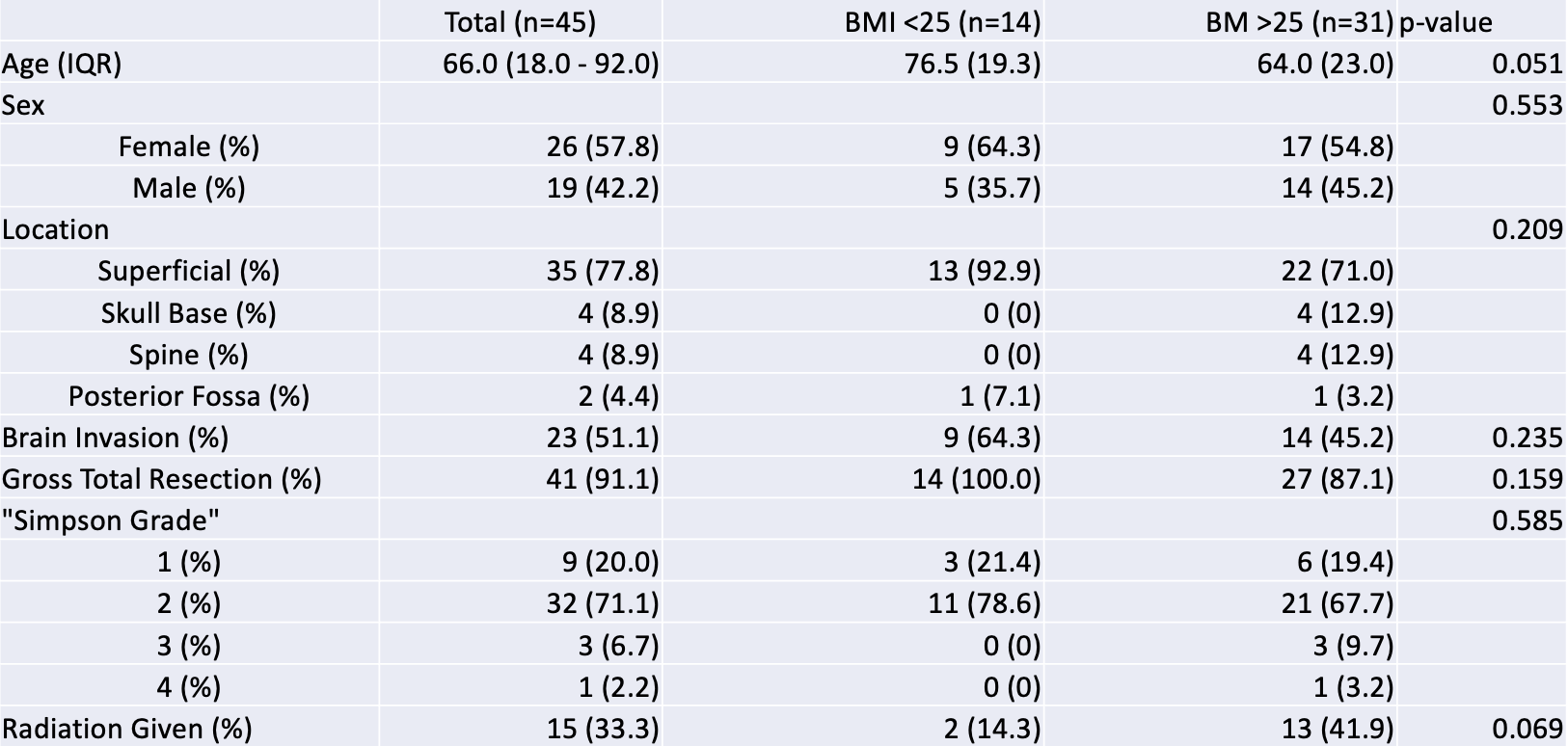
Table 1. Demographics

Table 2. Outcomes

Table 3. Multivariate analysis
Results
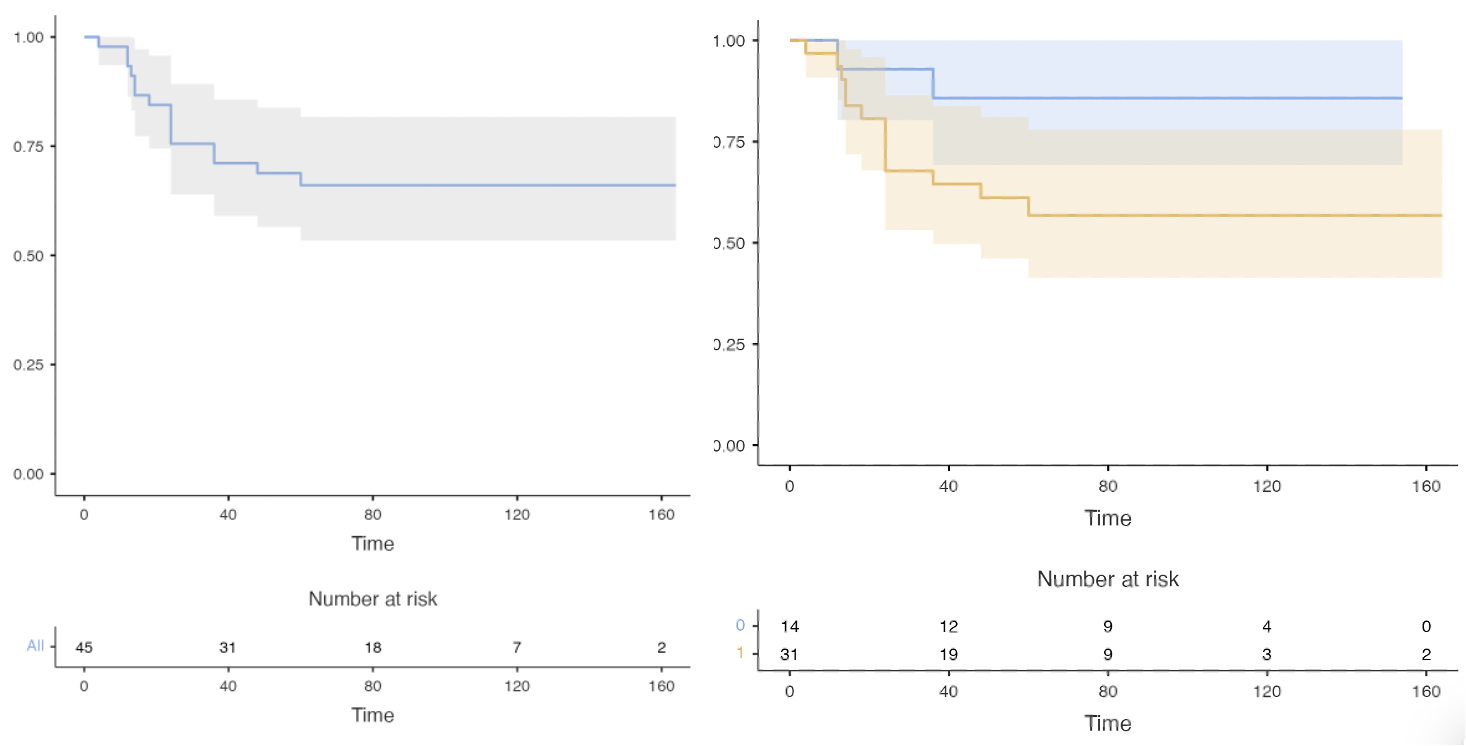
Figure 1. Recurrence of meningioma. Kaplan-Meier plot demonstrating risk of recurrence in patients with BMI<25 (blue) and BMI>25 (orange).
Discussion
The association between obesity and meningioma has been examined previously, with some studies finding a statistically significant link5-6. General, conceptual explanations for this link include a shared genetic susceptibility, as well as the downstream effects of chronic inflammation.
Insulin-like growth factor (IGF) has been proposed as a key player in the link between obesity and tumor growth7. Obesity-related insulin resistance and the subsequent hyperinsulinemia results in a downstream increase in insulin-like growth factor 1 (IGF-1). Meningioma has been shown to demonstrate an overexpression of IGF-1, IGF-2, and IGF-1R genes, which stimulates tumor growth and prevents apoptosis8. Further molecular profiling of Grade 2 and Grade 3 meningiomas in both our series and others’ may reveal informative, novel associations useful in determining both prognosis and treatment.
In this retrospective cohort study, we found that BMI > 25 is an independent predictor of recurrence and patients with BMI > 25 recur sooner than patients with a normal BMI. Further research is required to confirm this association. An explanation of the underlying mechanism likely requires subsequent molecular profiling, which may then be useful for predicting the risk of meningioma recurrence.
Insulin-like growth factor (IGF) has been proposed as a key player in the link between obesity and tumor growth7. Obesity-related insulin resistance and the subsequent hyperinsulinemia results in a downstream increase in insulin-like growth factor 1 (IGF-1). Meningioma has been shown to demonstrate an overexpression of IGF-1, IGF-2, and IGF-1R genes, which stimulates tumor growth and prevents apoptosis8. Further molecular profiling of Grade 2 and Grade 3 meningiomas in both our series and others’ may reveal informative, novel associations useful in determining both prognosis and treatment.
In this retrospective cohort study, we found that BMI > 25 is an independent predictor of recurrence and patients with BMI > 25 recur sooner than patients with a normal BMI. Further research is required to confirm this association. An explanation of the underlying mechanism likely requires subsequent molecular profiling, which may then be useful for predicting the risk of meningioma recurrence.
Role of selective neck dissections in the management of carotid body tumours

INTRODUCTION
- Carotid body tumors (CBT) are rare neoplasms originating from the paraganglia at the carotid bifurcation.
- Although typically benign, these tumors occasionally exhibit malignant behavior and metastasize to nearby lymph nodes.
- Histopathologic analysis alone is insufficient to determine malignancy in CBT, and metastasis to non-neuroendocrine tissue is required for definitive diagnosis.
- Universal clinical guidelines on management of CBT are lacking, and the role of selective neck dissections (SND) in detecting CBT malignancy and guiding management is uncertain.
OBJECTIVES
- Analyze the characteristics of CBT managed at our institution over a 20 year period
- Evaluate the outcomes of surgical management that routinely included SND
- Evaluate the utility of performing SND in CBT resections, and its implications for treatment decisions
METHODS
- Retrospective chart review of 21 patients undergoing CBT resection between 2002 and 2022 was performed.
- Patient demographics, genetic and laboratory testing, pre-operative imaging, intra-operative and post-operative complications, and follow up results were collected.
- SND were performed on all 21 patients.
- Histopathological analysis of neck dissection contents and primary tumor specimens were assessed.
RESULTS
- Of the 21 resections, there were three cases (14.3%) of carotid artery injuries and six cases (28.6%) of nerve injuries, including six to the vagus nerve and one to the hypoglossal nerve.
- One patient (4.8%) experienced an intra-operative stroke, likely related to tumour embolization under the same anaesthetic.
- Three patients (14.3%) were found to have lymph node involvement, indicating the presence of malignancy, and later received adjuvant radiotherapy.
- Fisher's exact test showed a statistically significant relationship between carotid injury and malignancy.
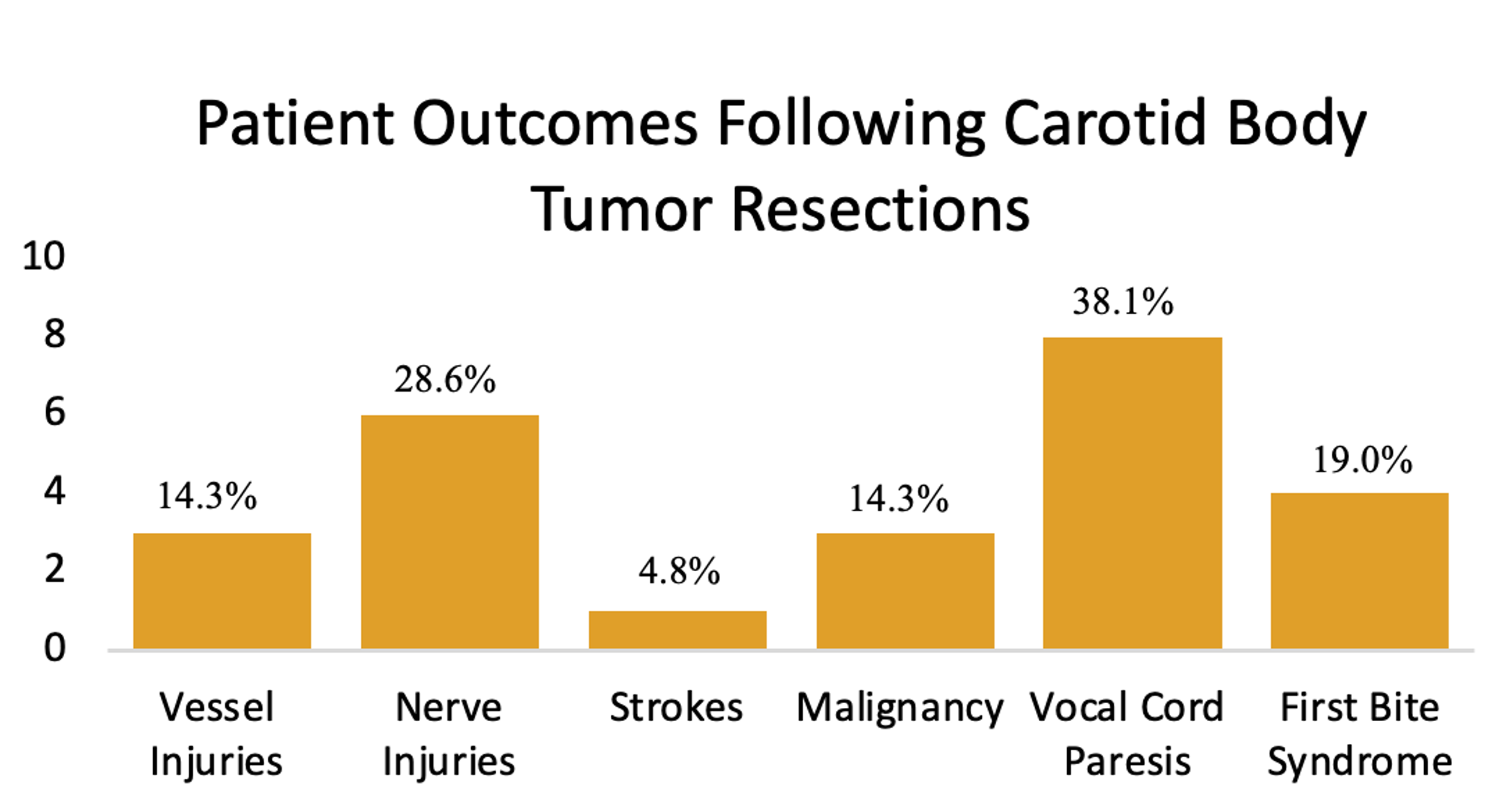
Figure 1: Summary of patient outcomes
DISCUSSION
- Performance of SND does not considerably prolong the operation or add substantial complexity.
- Eliminates need for second surgery when metastatic disease is suspected following the primary operation.
- Allows for tailored approach to post-surgical management, including prompt planning of additional treatment modalities.
- Provides reassurance to patients with non-metastatic disease.
- Study limitations: retrospective nature; small sample size due to rarity of condition; benefit on long-term outcomes not assessed.
CONCLUSION
- SND are a useful adjunct in detecting malignancy during CBT resections.
- The incidence of malignancy in CBT is low but not negligible.
- This study's 14.3% incidence of malignancy supports the utility of systematic SND during primary CBT resection to enhance diagnostic accuracy and subsequent management.
- Malignancy of CBT is a risk factor for carotid injury during resection.
- Due to the limited sample size, further studies with larger patient populations are required.
REFERENCES
- Kruger AJ, Walker PJ, Foster WJ et al. Important observations made managing carotid body tumors during a 25-year experience. J Vasc Surg. 2010 Dec 1;52(6):1518–23.
- Illuminati G, Pasqua R, Nardi P et al. Results of resection of carotid body tumors with and without lymphnodes’ dissection. Surg Oncol. 2021 Jun;37:101555.
- Mohebali J, Edwards HA, Schwartz SI et al. Multispecialty surgical management of carotid body tumors in the modern era. J Vasc Surg. 2021 Jun 1;73(6):2036–40.
- Obholzer R, Hornigold R, Connor S et al. Classification and management of cervical paragangliomas. Ann R Coll Surg Engl. 2011 Nov 1;93(8):596–602.
- Ma H, Wei M, Wang X et al. Necessity of Intraoperative Level IIA Lymph Node Dissection in Patients with Carotid Body Tumors: A Retrospective Study of 126 Cases. ORL J Oto-Rhino-Laryngol Its Relat Spec. 2022;84(4):271–7.
Trends in End-of-Life Care for People with Glioblastoma: A Population-Based Study

Background & Aim
- End-of-life care is defined as the period prior to death when symptoms increase and antitumoural therapy is no longer effective
- Glioblastoma (GBM) is a common and malignant brain tumour with a median survival of less than 2 years
- The end-of-life phase of care is an important aspect of care for patients with GBM as aggressive care at the end-of-life is associated with poor patient and caregiver satisfaction as well as increased healthcare costs.
- This study aims to describe end-of-life care patterns in GBM patients, assesing their temporal evoluation, regional disparities, and socioeconomic influences.
Methods
- This was a retrospective study of all patients with GBM treated in Ontario between 1994 and 2018 using administrative health data housed at ICES data.
- Patient demographic characteristics and comorbidities are described.
- Outcomes were the proportion of patients using palliative care (inpatient & outpatient services), emergency department visits, hospital admissions including ICU within 30 days of death, chemotherapy administration within 14 days of death, and location of death
- Logistic regression was used estimate the odds ratio of each outcome adjusting for: patient age at diagnosis, sex, rurality, neighbourhood income quintile, diagnosis year era, and other covariates.
- Crude proportions were estimated and trends in patient proportions were assessed with the Cochrane-Armitage trend test.
Figure 1: Geographic distribution of rurality (left) and household income (right).
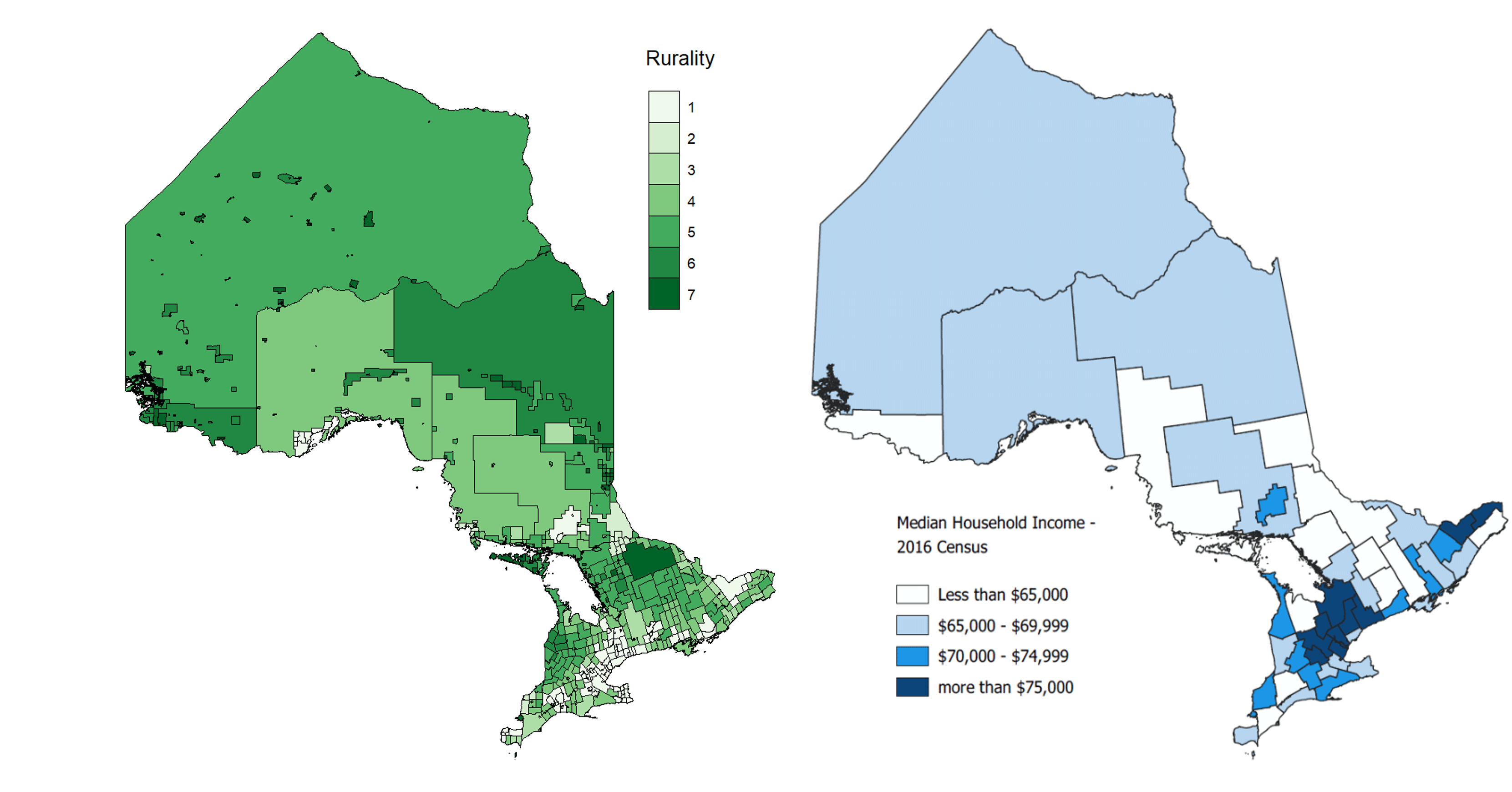
Source: Statistics Canada Boundary Files, Census, & FAO
Results
Table 1: Patient demographics and baseline characteristics.
| Variable | Total (N= 9013) |
| Age at diagnosis | |
| Mean year (SD) | 63.25 (12.69) |
| Sex (N, %) | |
| Female | 3,730 (41.4%) |
| Male | 5,283 (58.6%) |
| Diagnosis year (N, %) | |
| 1994 - 1998 | 1,381 (15.3%) |
| 1999 - 2003 | 1,700 (18.9%) |
| 2004 - 2008 | 1,489 (16.5%) |
| 2009 - 2013 | 2,178 (24.2%) |
| 2014 - 2018 | 2,265 (25.1%) |
| Nearest Census Based Neighbourhood Income Quintile (N, %) | |
| 1 | 1,418 (15.8%) |
| 2 | 1,788 (19.8%) |
| 3 | 1,783 (19.8%) |
| 4 | 1,923 (21.3%) |
| 5 | 2,101 (23.3%) |
| Rurality | |
| Large urban | 5,953 (66.0%) |
| Small urban | 2,083 (23.1%) |
| Rural | 875 (9.7%) |
| Unknown | 102 (1.1%) |
Figure 2: Temporal trends of care in GBM patients.
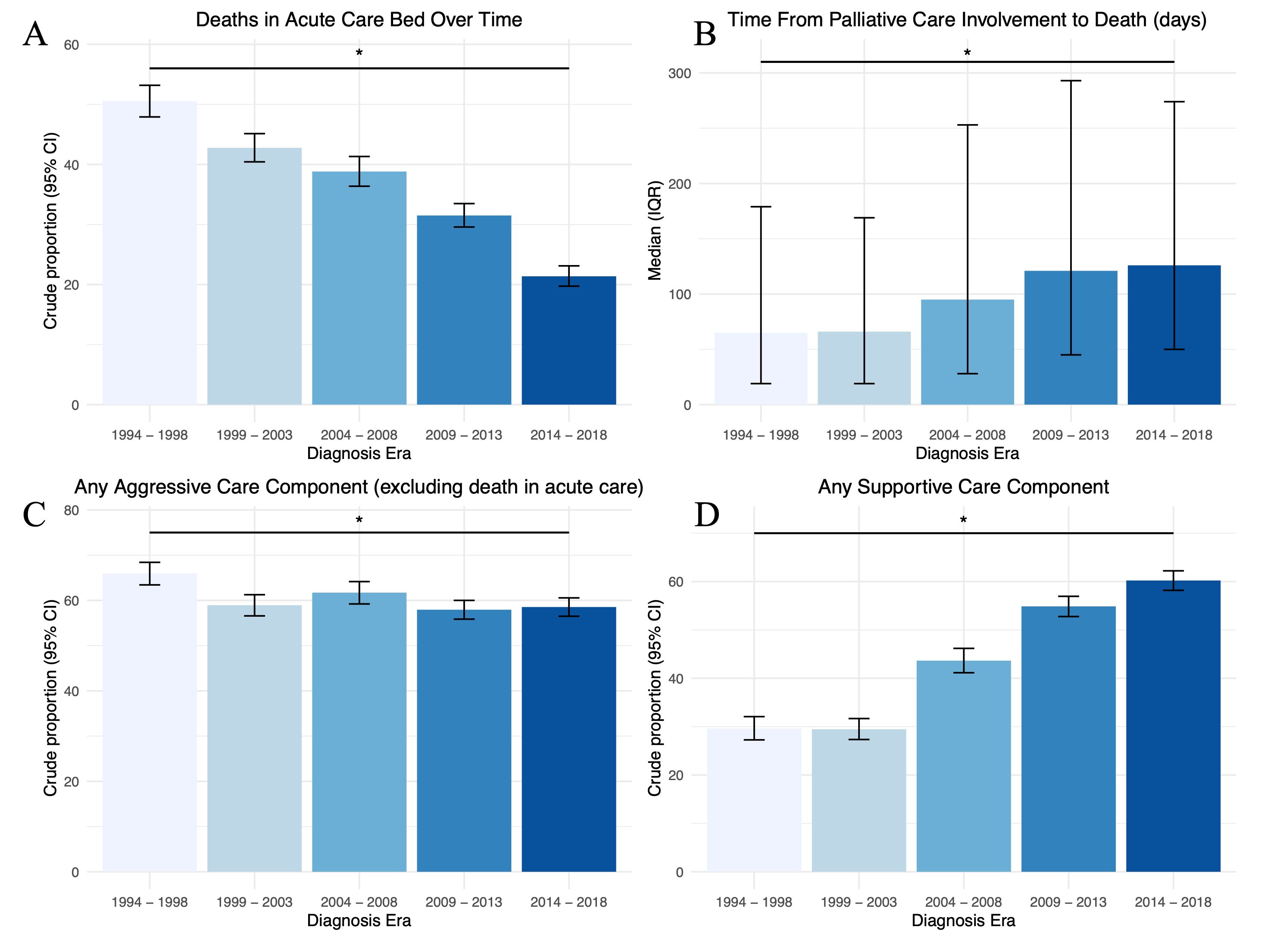
Figure 3: Regional and socioeconomic trends of care in GBM patients

Summary
- There was a gradual increase in the utilization of palliative at end-of-life as well as earlier integration of palliative care and a reduction of deaths in acute care beds over the study period.
- There was a concurrent decrease in aggressive components of care at the end of life.
- Patient’s geographical region as well as socioeconomic status influenced the nature of end-of-life care.
Funding
- This work was funded by a research grant from the department of surgery, Queen’s university.
Plasma extracellular vesicle sampling from high grade gliomas demonstrates a small RNA signature indicative of disease and identifies lncRNA RPPH1 as a novel biomarker

INTRODUCTION
High grade gliomas (HGGs) and cells of the tumour microenvironment (TME) secrete extracellular vesicles (EVs) into the plasma that contain genetic and protein cargo which function in paracrine signaling. Isolation of these EVs and their cargo from plasma could lead to a simplistic tool that can inform on diagnosis and disease course of HGG. Small RNA consisting of (miRNA, snoRNA, tRNA, LINC RNA fragments <300bp and mRNA fragment) contained with EVs may be able to rapidly alter target cells and therefore may make good biomarkers when studying HGG disease progression.
Methods: In the present study, plasma EVs were captured utilizing a peptide affinity method (Vn96 peptide) from HGG patients and normal controls followed by next generation sequencing (NovaSeq6000) to define a small RNA (sRNA) signature unique to HGG.
Methods: In the present study, plasma EVs were captured utilizing a peptide affinity method (Vn96 peptide) from HGG patients and normal controls followed by next generation sequencing (NovaSeq6000) to define a small RNA (sRNA) signature unique to HGG.
METHODS
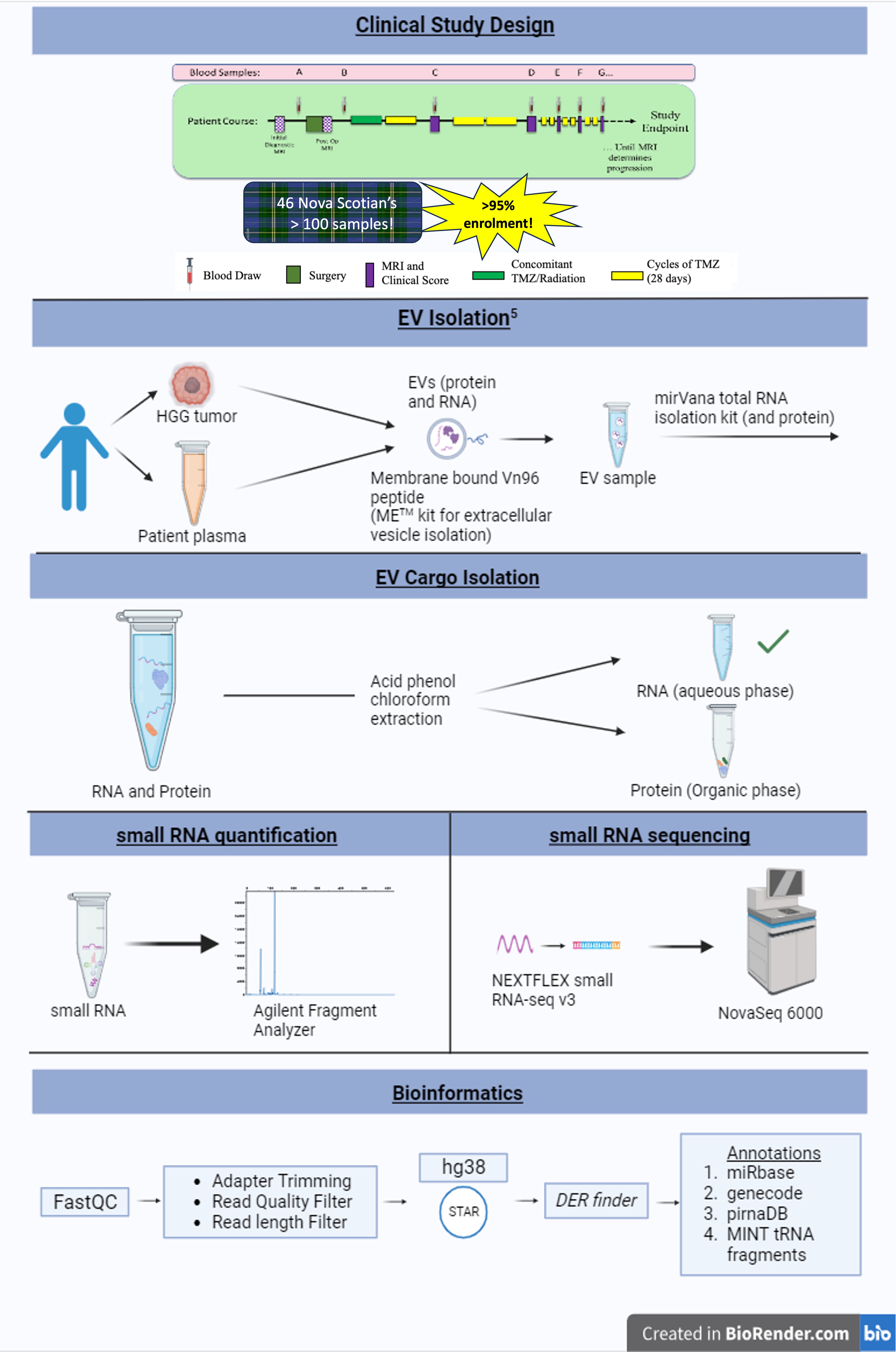
RESULTS
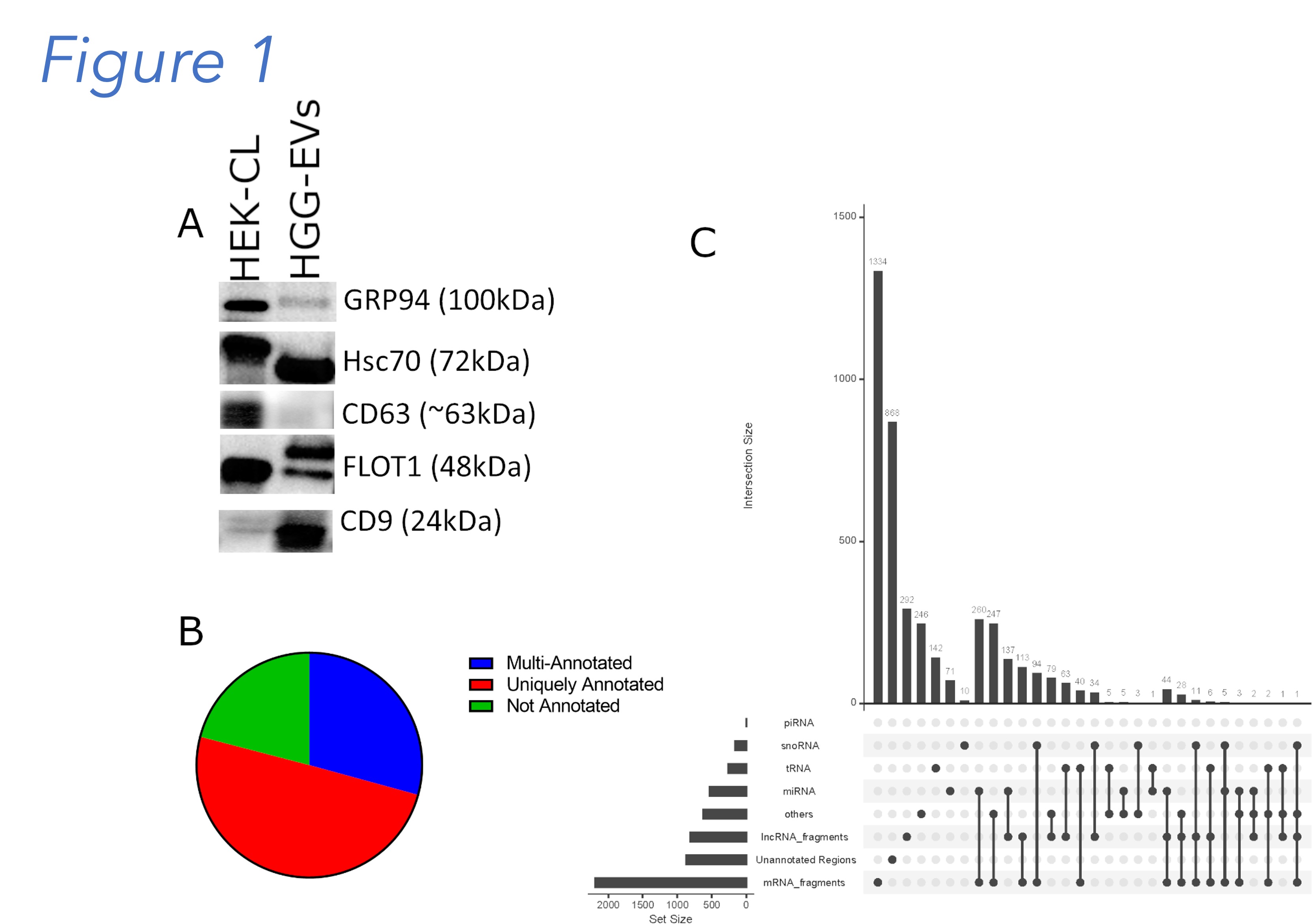
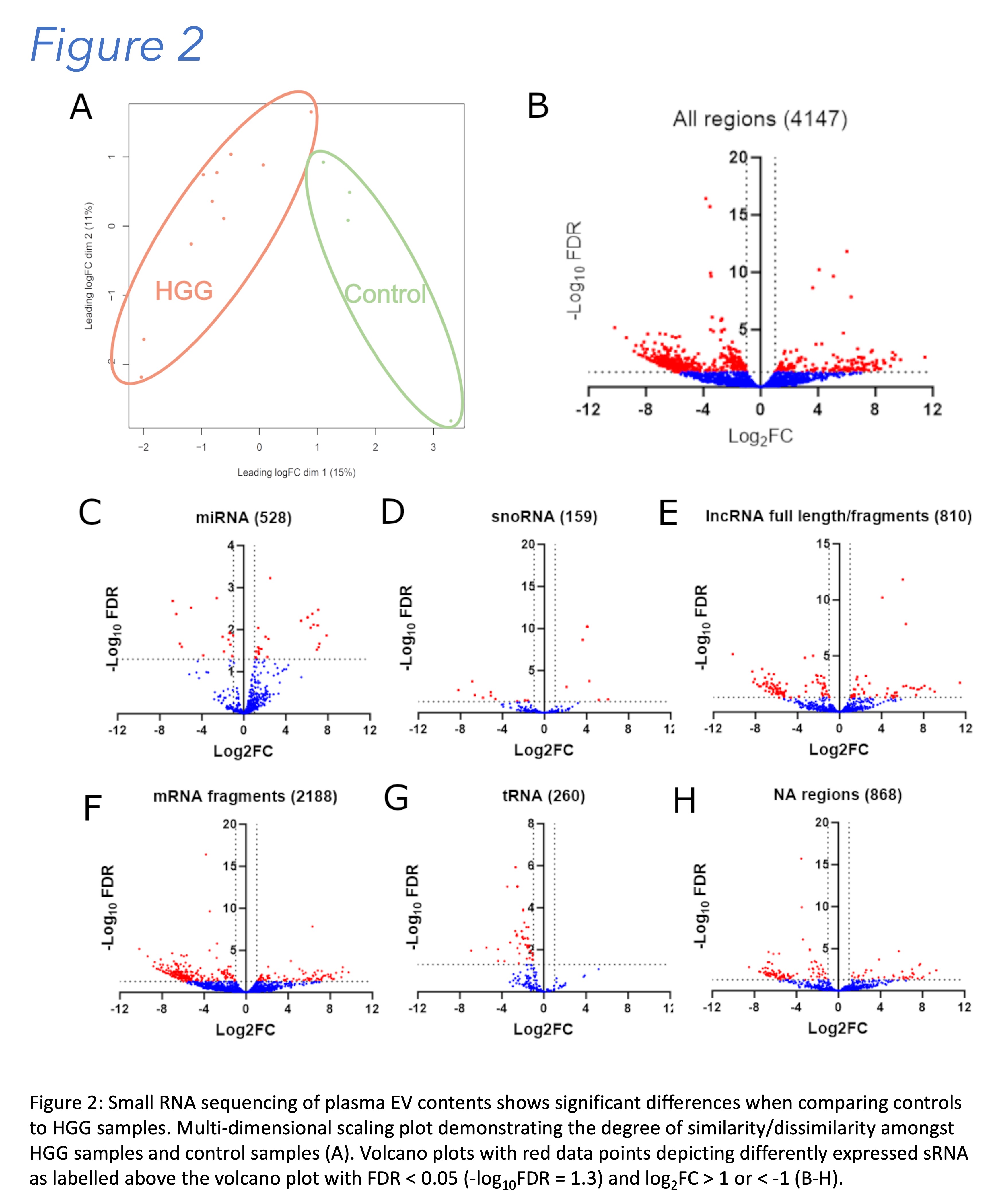
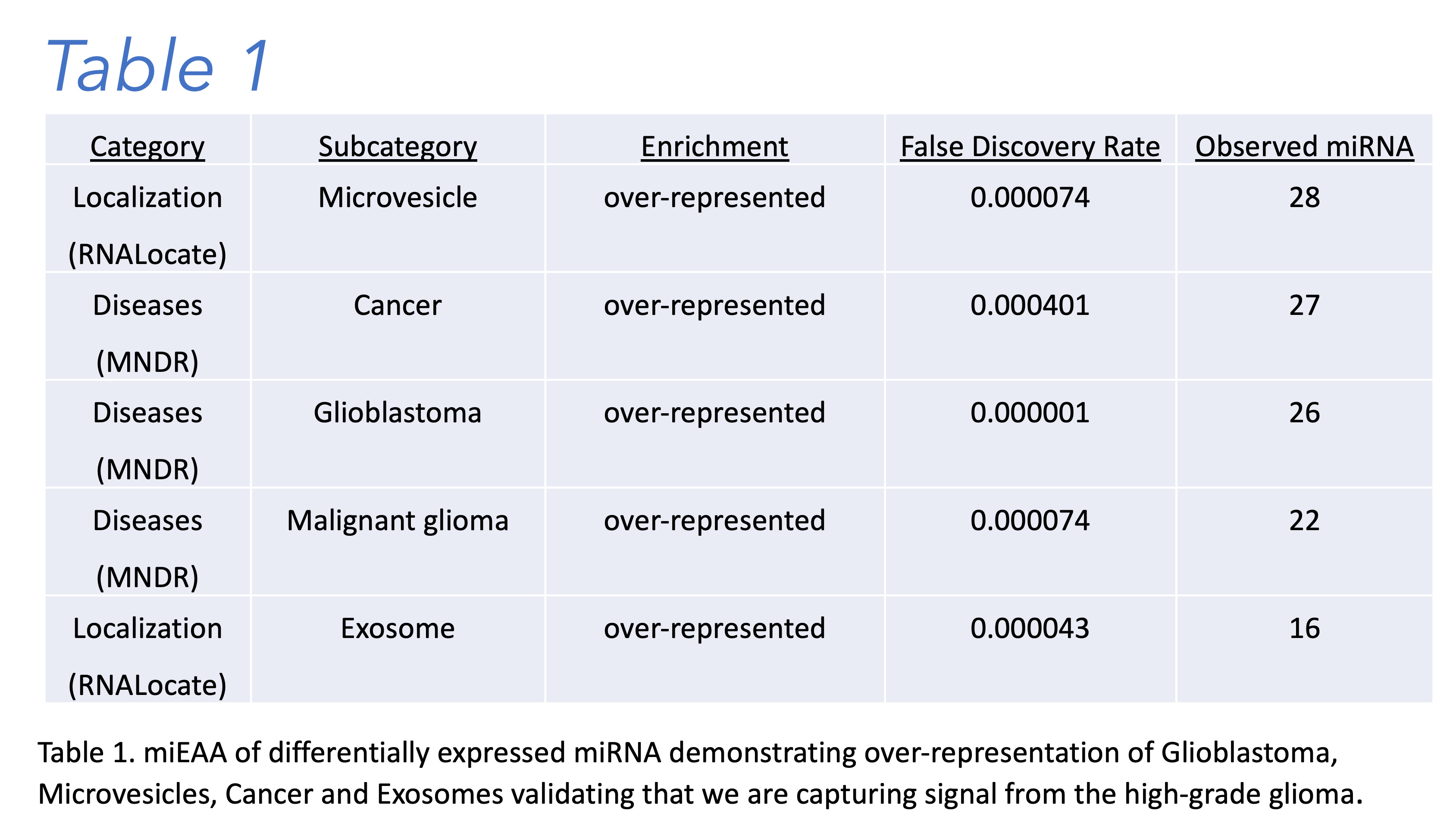
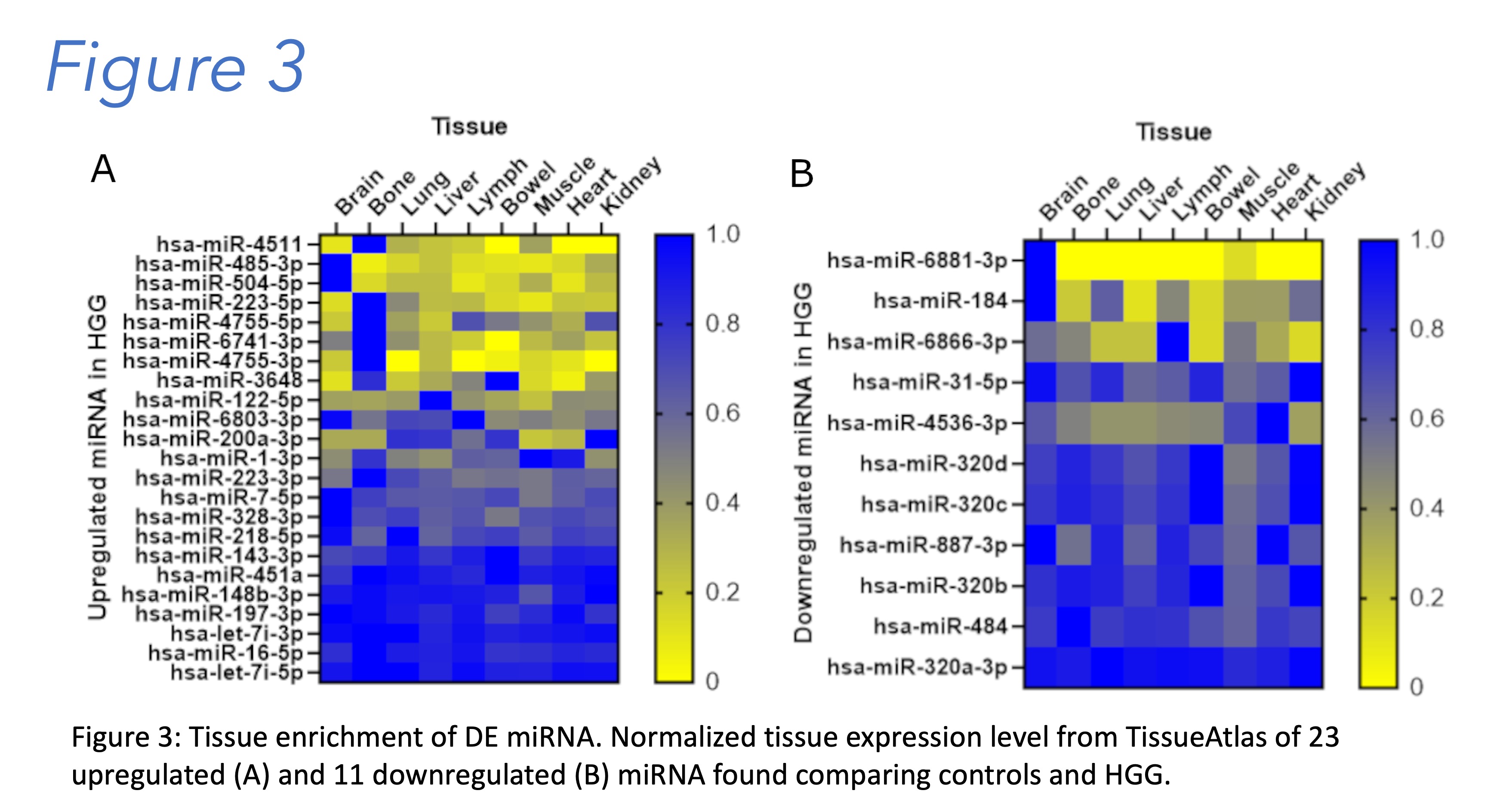
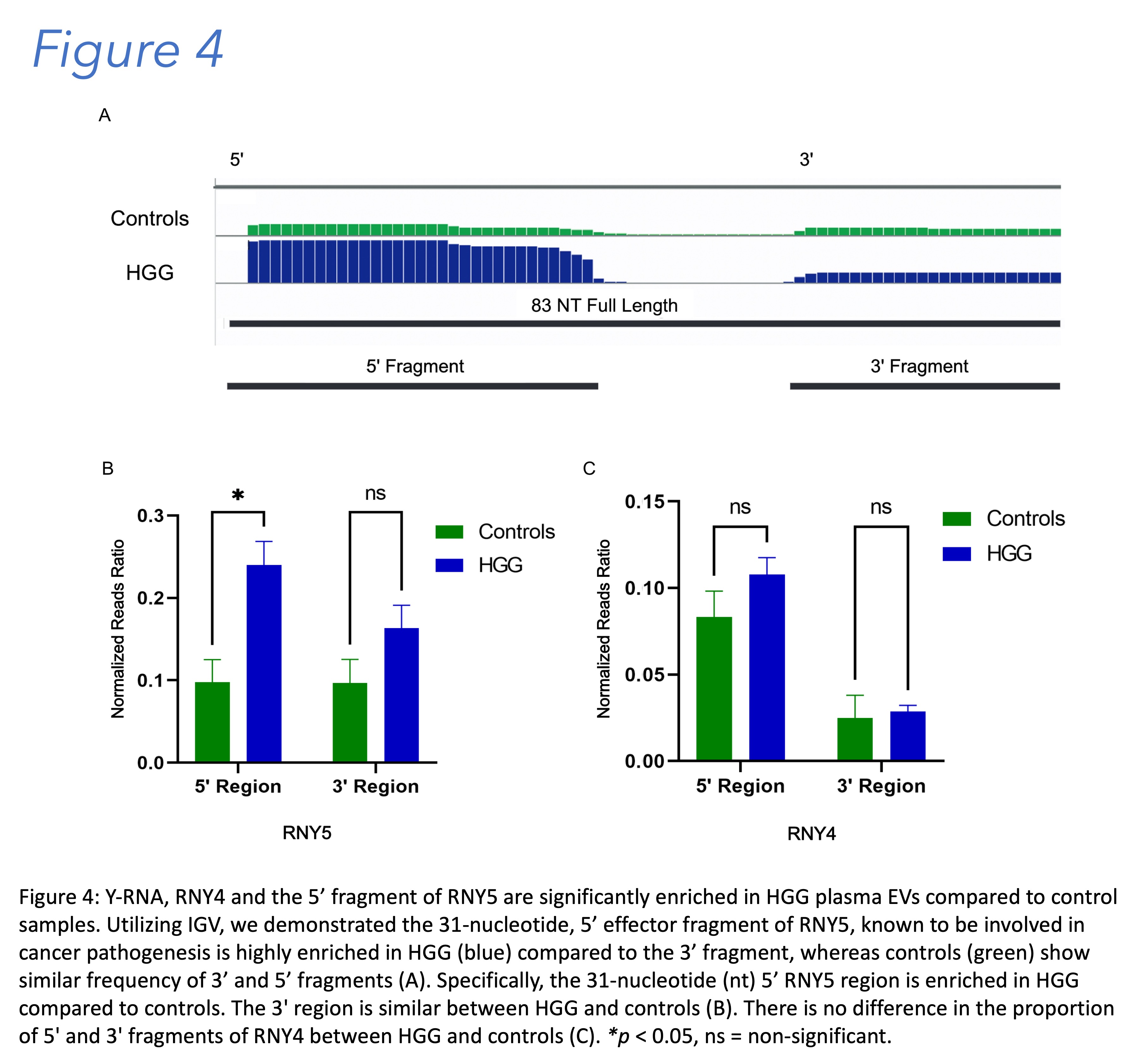
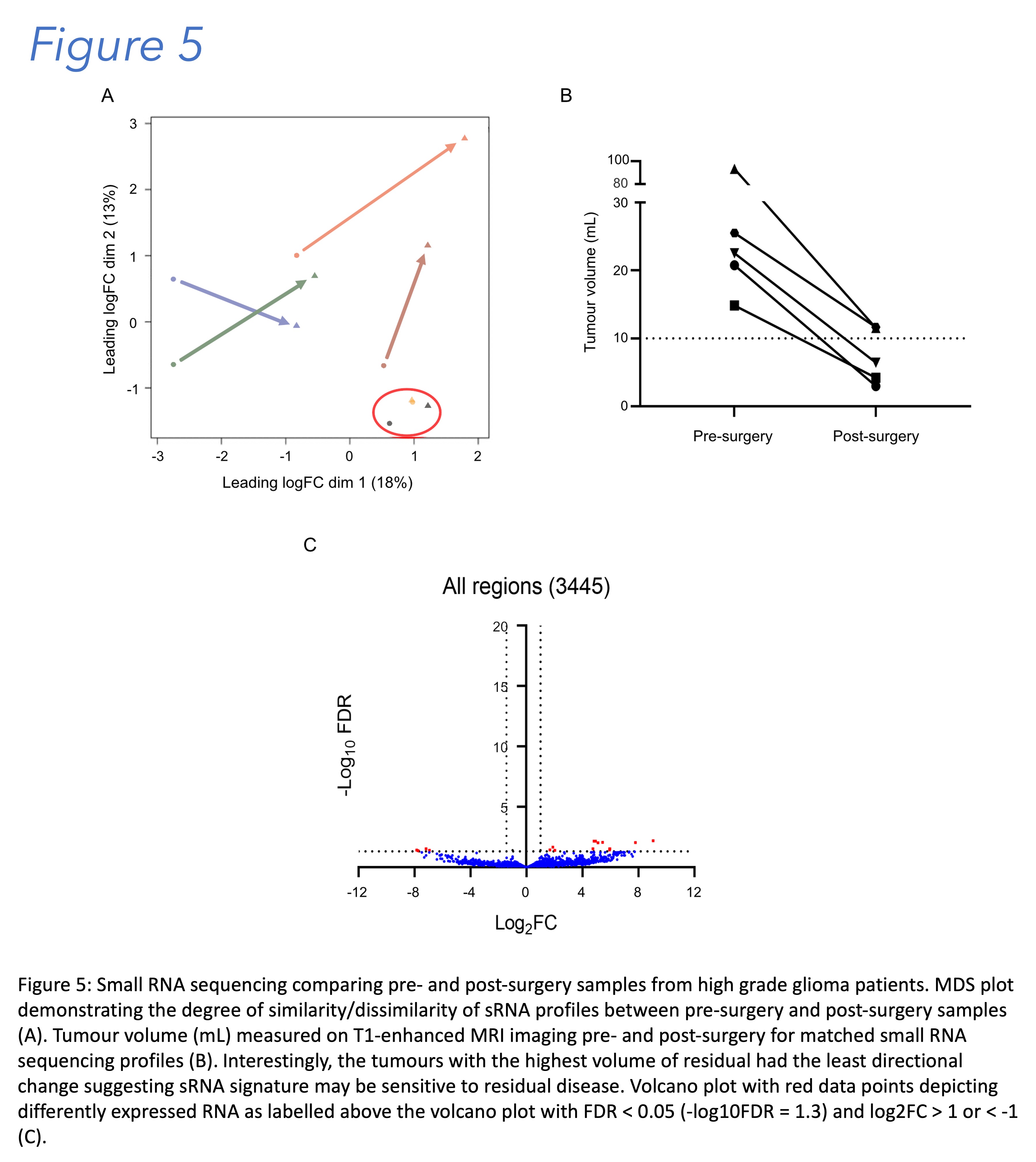
Figure 1: Western blot analysis demonstrating EVs isolated from pooled HGG-EVs utilizing Vn96 peptide affinity have canonical markers of EVs including Hsc70, CD63, FLOT1 and CD9. The non-EV marker GRP94 is detected at low levels. HEK 293T total cell lysate (HEK-CL) was used as a positive control (A). Distribution of multi-annotated, uniquely annotated, and not annotated RNA reads upon sequencing control and HGG samples (B); Upset plot illustrating the distribution and frequency of uniquely annotated RNA sequences and multi-annotated sequences in plasma stratified by type of annotated small RNA. The columns are sorted according to a decreasing number of uniquely annotated RNA, double-annotated RNA, and multi-annotated RNA with three or more different annotations (C).
FUNDING

Figure 6: RPPH1 expression from HGG plasma EVs serves as a candidate biomarker. RPPH1 is DE in HGG (n = 10) relative to control plasma EVs (n = 4), shows significant reduction in expression following surgery (n = 6), and shows significant elevation in expression with clinically defined progression of HGG (n = 5) (A). RPPH1 expression is significantly greater in HGG tissue when compared to normal tissue and higher expression is associated with worsened prognosis in HGG patients. Violin plot comparing relative RPPH1 expression levels between normal brain tissue (n = 1141, GTEx database) and HGG (n = 144, TCGA database) as generated using Xena (B). Kaplan-Meier curve demonstrating worse disease specific survival for the upper quartile vs. lower quartile of RPPH1 expression as generated using Xena and querying TCGA low grade glioma and glioblastoma databases (C). *p < 0.05; **p < 0.01; ****p < 0.0001.
DISCUSSION
Over 750 differentially expressed sRNA (miRNA, snoRNA, lncRNA, tRNA, mRNA fragments and non-annotated regions) were identified between HGG and controls. MiEAA 2.0 pathway analysis of the miRNA in the sRNA signature revealed miRNA highly enriched in both EV and HGG pathways demonstrating the validity of results in capturing a signal from the tissue microenvironment. Also revealed were several novel HGG plasma EV sRNA biomarkers including lncRNA RPPH1 (Ribonuclease P Component H1), RNY4 (Ro60-Associated Y4) and RNY5 (Ro60-Associated Y5). Furthermore, in paired longitudinal patient plasma sampling, RPPH1 informed on surgical resection (decreased on resection) and importantly RPPH1 increased again on clinically defined progression. Our next goal is to sequence small RNA in the corresponding tissue samples to correlate EV expression with tissue expression.
ACKNOWLEDGMENTS
Patients involved, Lauren Westhaver, Megan Lambert, Sam Warren, Stacey Siler
Integration of Ultrasensitive electroluminescent immunoassay and cell-free DNA methylation analysis for the non-invasive discrimination of adult diffuse gliomas

Background
Gliomas are highly aggressive brain tumors with nearly universal recurrence rates. Monitoring for tumor recurrence relies solely on serial MRI imaging, which is complicated by treatment effects such as pseuoprogression. Moreover, MRI is unable to anticipate when recurrence will occur, and cannot capture potential molecular changes that these tumors undergo to allow for recurrence. These issues highlight the need for both prognostic and monitoring biomarkers. Despite the plethora of candidates for non-invasive biomarkers, all suffer from one of several problems: low clinical sensitivity, specificity, lack of evidence of survival difference, or high cost. Due to the low accuracies of individual serum markers, we have proposed the use of an integrated, multi-platform approach to biomarker discovery. Here we leverage two distinct platforms: cell free methylation DNA sequencing (cfMeDip) which captures epigenetic markers on circulating free DNA, and an ultrasensitive electroluminescent immunoassay for proteomic analysis, Proximity Extension Assay (PEA).
Gliomas are highly aggressive brain tumors with nearly universal recurrence rates. Monitoring for tumor recurrence relies solely on serial MRI imaging, which is complicated by treatment effects such as pseuoprogression. Moreover, MRI is unable to anticipate when recurrence will occur, and cannot capture potential molecular changes that these tumors undergo to allow for recurrence. These issues highlight the need for both prognostic and monitoring biomarkers. Despite the plethora of candidates for non-invasive biomarkers, all suffer from one of several problems: low clinical sensitivity, specificity, lack of evidence of survival difference, or high cost. Due to the low accuracies of individual serum markers, we have proposed the use of an integrated, multi-platform approach to biomarker discovery. Here we leverage two distinct platforms: cell free methylation DNA sequencing (cfMeDip) which captures epigenetic markers on circulating free DNA, and an ultrasensitive electroluminescent immunoassay for proteomic analysis, Proximity Extension Assay (PEA).
Methods
A cohort of adult glioma plasma samples underwent plasma proteomic consisting of a panel of serum proteins (FABP4, GFAP, NFL, Tau and MMP3, MMP4 &MMP7) quantified through ultrasensitive electrochemiluminescence multiplexed immunoassays, and plasma DNA methylation analysis, captured through cell-free methylated DNA immunoprecipitation and high-throughput sequencing. Mean serum protein concentrations were compared using the Wilcoxon statictical test, and survival analysis was completed through Cox regression. Unsupervised heirarchal clustering was completed on serum protein markers and a GLMnet model was utilized for the training of a predictive model for both tumor type and recurrence prediction.

Results
Serum Proteiomics and cfMeDIP-seq allows for the prediction of IDH Status and Recurrence through a cominded modelling approach
Conclusion
Our serum proteomic panels is effective in disciminating IDH-status and recurrence, and correlates with overall survival. The combination of DNA methylation signatures captured through cfMeDIP-seq and plasma proteomics showcases that an integrative approach improves the ability of these techniques to disciminate recurrent samples from primary, suggesting that they may be adapted for the serial monitoring of adult diffuse gliomas patients.
Our serum proteomic panels is effective in disciminating IDH-status and recurrence, and correlates with overall survival. The combination of DNA methylation signatures captured through cfMeDIP-seq and plasma proteomics showcases that an integrative approach improves the ability of these techniques to disciminate recurrent samples from primary, suggesting that they may be adapted for the serial monitoring of adult diffuse gliomas patients.
Prognostic value of NIRS regional oxygen saturation based cerebrovascular reactivity in TBI: a Canadian high resolution traumatic brain injury (CAHR-TBI) cohort study
Background
- Contemporary critical care management of moderate to severe traumatic brain injury (TBI) remains focused on guideline-based universal intracranial pressure (ICP) and cerebral perfusion pressure (CPP) targets.1
- Near-infrared spectroscopy regional cerebral oxygen saturation (rSO2) has gained interest as a raw parameter and as a basis for measuring cerebrovascular reactivity (CVR) due to its non-invasive nature and high spatial resolution.2
- However, the prognostic utility of these parameters has not yet been determined.
- This study aimed to identify threshold values of rSO2 and rSO2 based CVR at which outcomes worsened following traumatic brain injury (TBI).
Methods
- A retrospective multicenter cohort study was performed leveraging prospectively collected high-resolution physiologic data and clinical outcome data from the CAHR-TBI Research Collaborative.3
- Data was collected at four university-affiliated hospitals: Foothills Medical Centre (University of Calgary), Health Sciences Centre Winnipeg (University of Manitoba), Maastricht University Medical Center (University of Maastricht), and Vancouver General Hospital (University of British Columbia).
- The cerebral oxygen indices, COx (using rSO2 and cerebral perfusion pressure) as well as COx_a (using rSO2 and arterial blood pressure) were calculated for each patient.
- Grand mean thresholds along with exposure-based thresholds were determined utilizing sequential Chi-squared analysis and univariate logistic regression, respectively.
Results
- In total, 129 subjects from the CAHR-TBI database were included in the study with admission to hospital between November 2016 and December 2022.
- In total 751,060 minutes of unique physiologic recording was collected with a median recording duration of 4,578 minutes (IQR: 2,346 to 8,275 minutes) per subject.
- No identifiable threshold for raw rSO2 at which outcomes were found to worsen.
- For both COx and COx_a, an optimal grand mean threshold value of 0.2 was identified for both survival and favorable outcomes while percent time above -0.05 was uniformly found to have the best discriminative value. (Figure 1)
Figure 1 Plots of chi-square results for incremental thresholds of the cerebral perfusion pressure variant of the cerebral oxygen index (COx) and the arterial blood pressure variant of the cerebral oxygen index (COx_a). Panels A and C display the discriminative value of thresholds for favorable outcomes for average COx and COx_a, respectively. Panels B and D display the discriminative value of thresholds for survival for average COx and Cox_a, respectively. Red points indicate chi-square values that reached statistical significance (p < 0.05). Of note, while COx and COx_a theoretically extend from -1 to +1, in this dataset average values extended over a more limited range.
Conclusions
In this multi-institutional cohort study, raw rSO2was found to contain no significant prognostic information. However, rSO2 based indices of CVR, COx and COx_a, were found to have a uniform grand mean threshold of 0.2 and exposure-based threshold of -0.05, above which clinical outcomes markedly worsened. This study lays the groundwork to transition to less invasive means of continuously measuring CVR.
References
- Carney N, Totten AM, O’Reilly C, et al (2017) Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 80:6–15. https://doi.org/10.1227/NEU.0000000000001432
- Mathieu F, Khellaf A, Ku JC, et al (2020) Continuous Near-infrared Spectroscopy Monitoring in Adult Traumatic Brain Injury: A Systematic Review. J Neurosurg Anesthesiol 32:288–299. https://doi.org/10.1097/ANA.0000000000000620
- Bernard F, Gallagher C, Griesdale D, et al (2020) The CAnadian High-Resolution Traumatic Brain Injury (CAHR-TBI) Research Collaborative. Can J Neurol Sci 47:551–556. https://doi.org/10.1017/cjn.2020.54
Acknowledgements and Funding
Alwyn Gomez is supported through a CIHR Fellowship (Grant #: 472286).

Gomez, A., Froese, L., Griesdale, D. et al. Prognostic value of near-infrared spectroscopy regional oxygen saturation and cerebrovascular reactivity index in acute traumatic neural injury: a CAnadian High-Resolution Traumatic Brain Injury (CAHR-TBI) Cohort Study. Crit Care 28, 78 (2024).
Corpus callosum changes in children affected by infantile hydrocephalus
INTRODUCTION
Infantile hydrocephalus: atypical accumulation of cerebrospinal fluid treated before age 2.
Posterior cortex affected in hydrocephalus1,2.
Research links hydrocephalus to corpus callosum (CC) thinning due to ventricular dilatation creating upward elevation and compression of periventricular and subcortical white matter 3,4,5,6,7,8.
Posterior cortex affected in hydrocephalus1,2.
Research links hydrocephalus to corpus callosum (CC) thinning due to ventricular dilatation creating upward elevation and compression of periventricular and subcortical white matter 3,4,5,6,7,8.
METHODS
18 patients with infantile hydrocephalus treated with a ventriculoperitoneal shunt (mean age = 9 years) and 18 age and sex matched typically-developing healthy children, participated in the study.
The CC of both groups was measured and segmented including the splenium, isthmus, body, genu, and rostrum.
Structural magnetic resonance imaging and diffusion tensor imaging were utilized to assess CC volume and microstructure.
The CC of both groups was measured and segmented including the splenium, isthmus, body, genu, and rostrum.
Structural magnetic resonance imaging and diffusion tensor imaging were utilized to assess CC volume and microstructure.
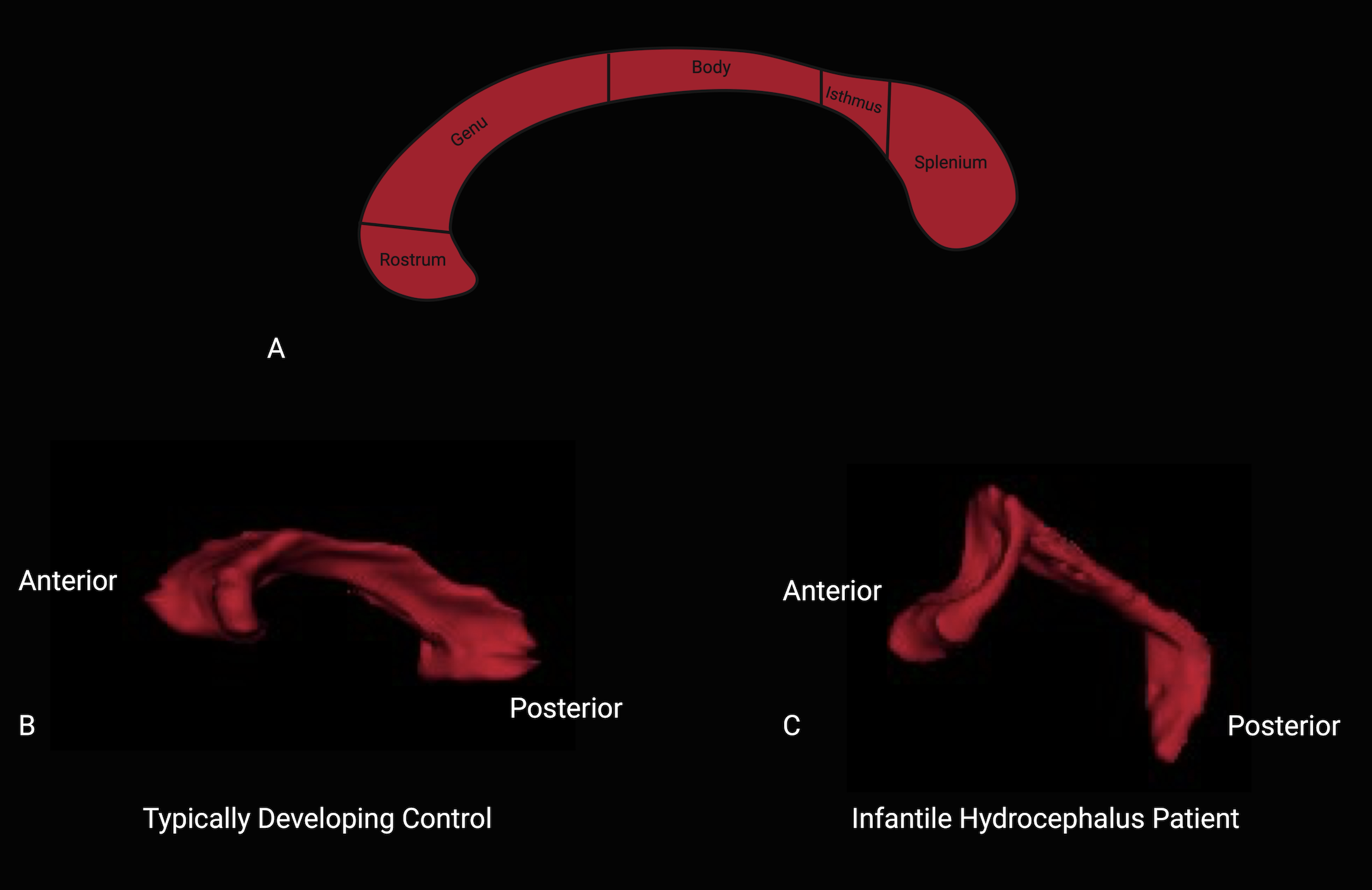
RESULTS
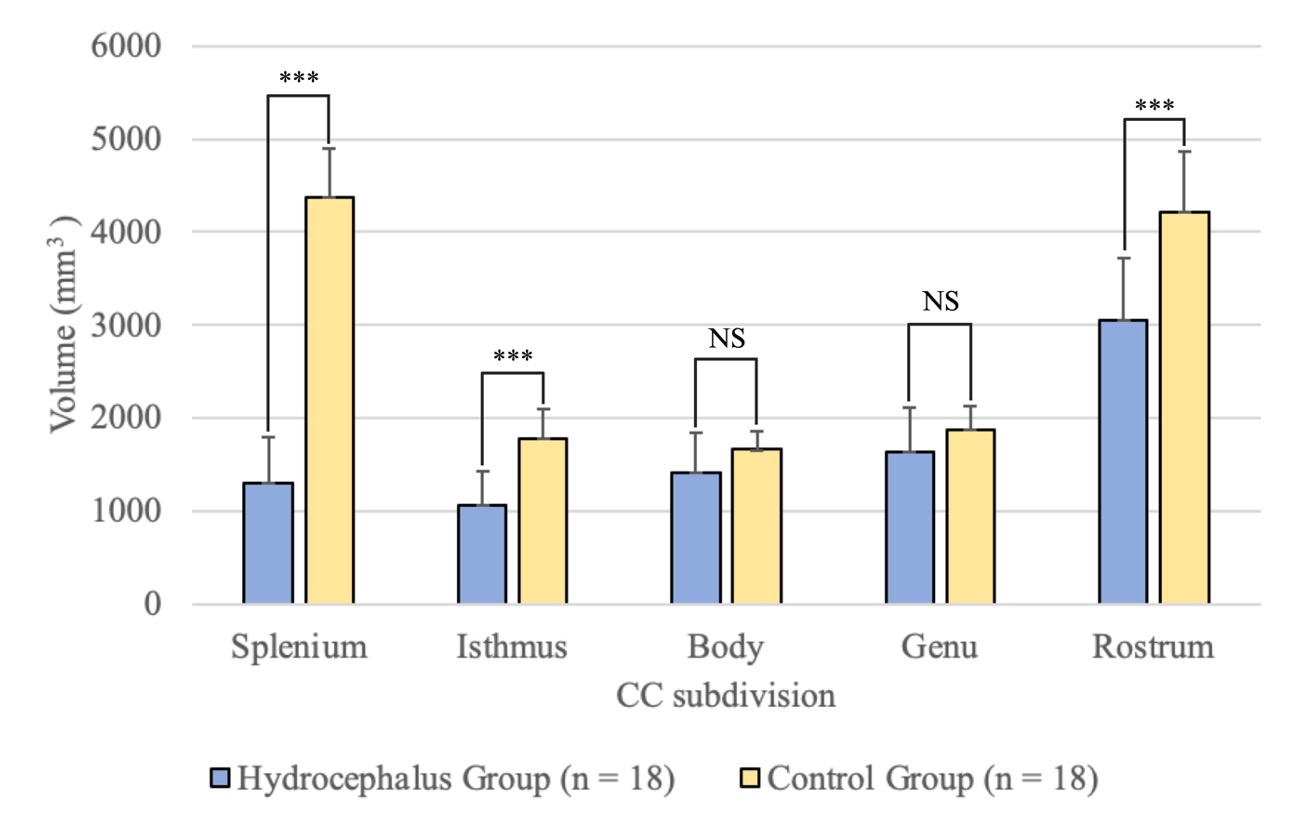
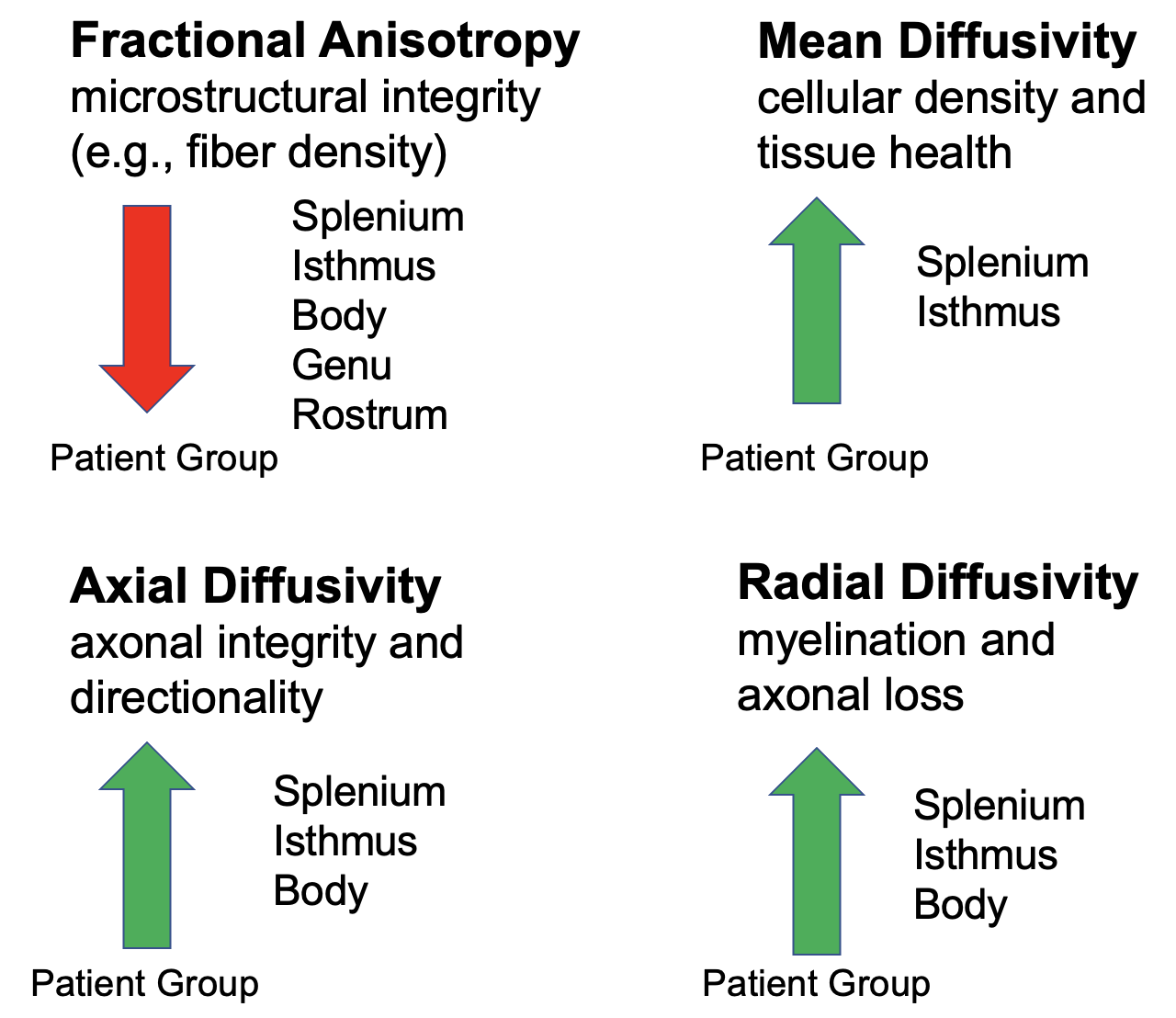
DISCUSSION
Differences in CC volume reflect regional functional specialization. The splenium, isthmus, and rostrum showed significant volume differences, playing roles in visual processing and motor coordination9,10,11,12,13. These areas are closely affected by hydrocephalus-related changes, suggesting complex interactions within the CC, including potential compensatory mechanisms.
Patients exhibited significantly lower white matter integrity across all CC regions, indicating disruptions to axonal fiber organization. Higher overall water diffusion in the splenium and isthmus suggests tissue damage and cellular changes. Additionally, increased diffusion along and across axonal fibers in these regions includes microstructural alterations due to demyelination and axonal damage.
Patients exhibited significantly lower white matter integrity across all CC regions, indicating disruptions to axonal fiber organization. Higher overall water diffusion in the splenium and isthmus suggests tissue damage and cellular changes. Additionally, increased diffusion along and across axonal fibers in these regions includes microstructural alterations due to demyelination and axonal damage.
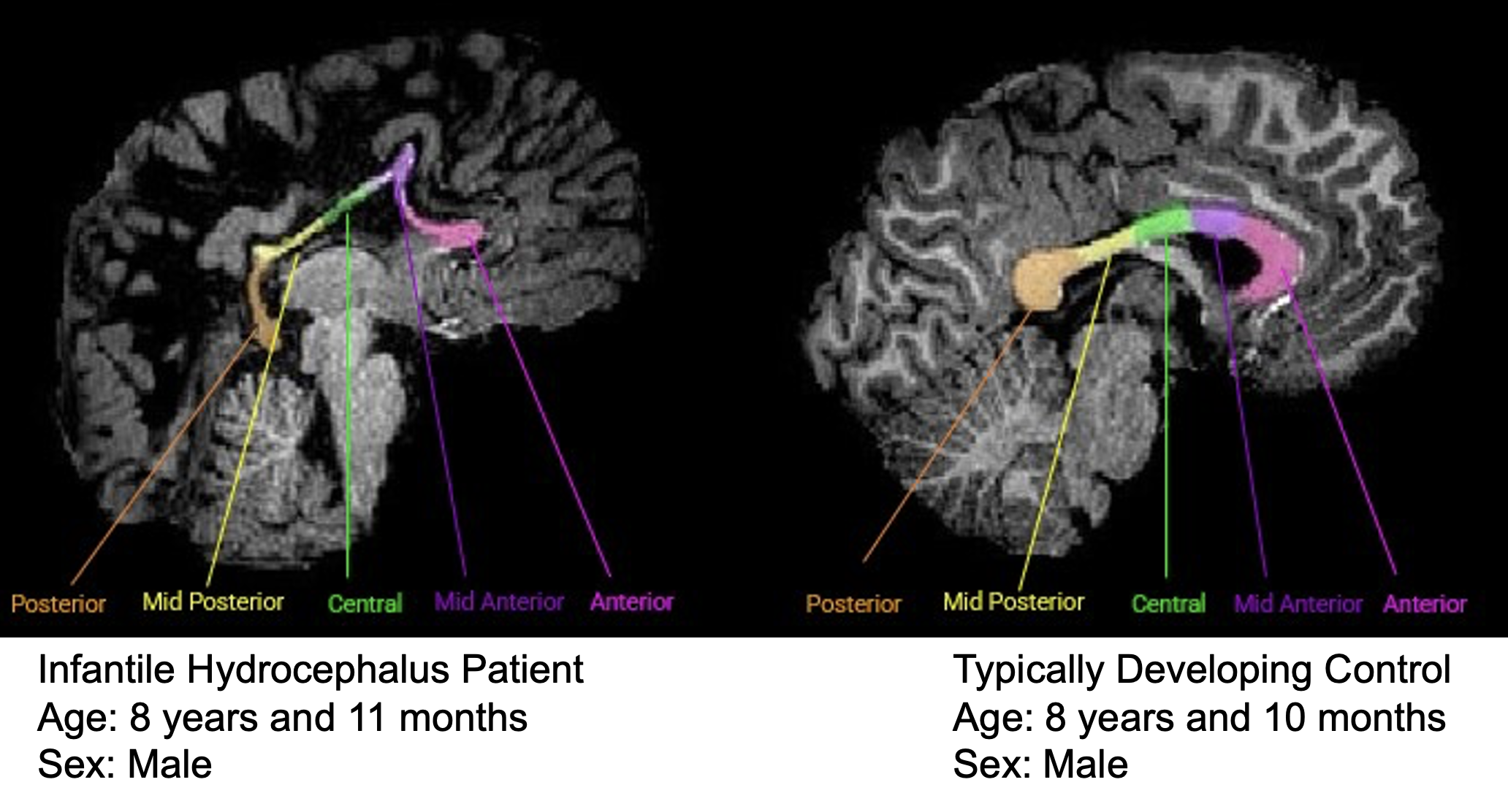
CONCLUSION
These findings suggest disruptions in white matter integrity in patients with infantile hydrocephalus. Future studies conducting functional connectivity analyses should consider the health of the CC given the neural signal transmission between interhemispheric brain regions involved in cognitive and motor processes.
How often does digital subtraction angiography change management in CT angiogram negative subarachnoid hemorrhages?

Introduction
- Subarachnoid hemorrhages (SAH) can be spontaneous or due to trauma.
- 85% of spontaneous SAH are attributed to ruptured aneurysms, but a significant number do not have detectable etiologies on initial imaging.
- These include idiopathic perimesencephalic subarachnoid hemorrhages (PMSAH), a subset with a good prognosis often attributed to small, spontaneous ruptures in venous vessels.
- Diagnosis of SAH involves non-contrast CT followed by CT angiogram (CTA) and then digital subtraction angiogram (DSA) used for cases with uncertain etiology.
- The invasiveness and associated risks of DSA warrant careful consideration, especially in cases with favourable prognoses.
- It is unclear how often DSA alters surgical or endoscopic treatment in patients with a spontaneous, CTA-negative SAH.
Objectives
To determine how often a DSA in patients with a spontaneous CTA-negative SAH identifies pathology that requires surgical or endoscopic management.
Methods
Retroactive chart analysis on patients who presented with a spontaneous SAH to Vancouver General Hospital with no etiology found on CTA who then received a DSA. Patient demographics, initial presentation, radiologic findings, clinical course, and complications of treatment were recorded.

Results
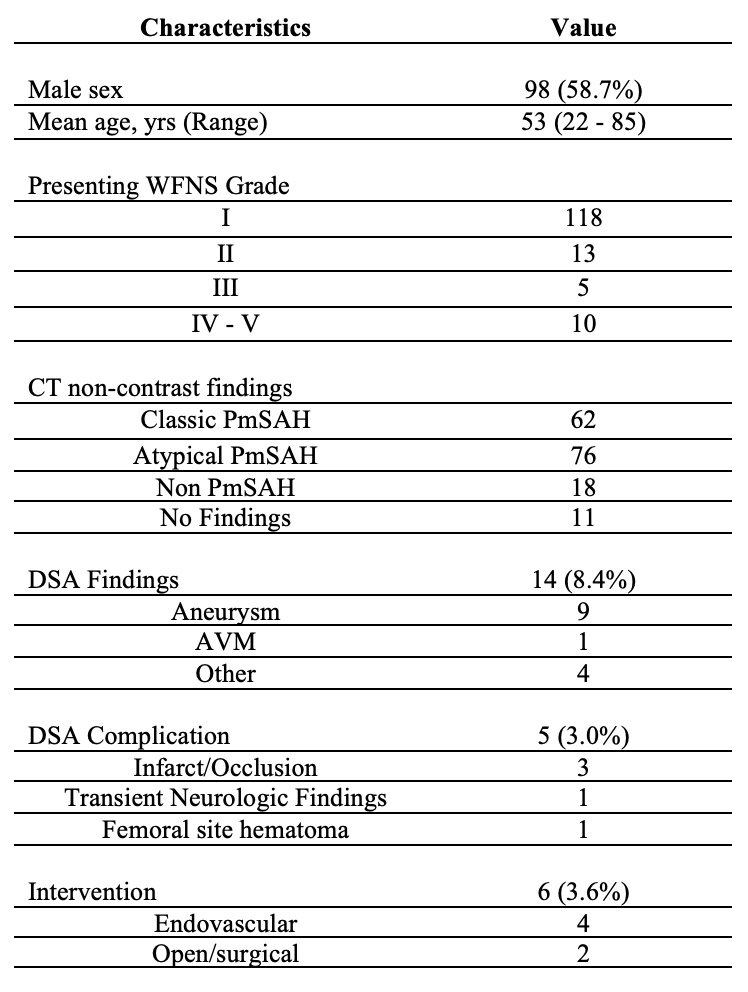
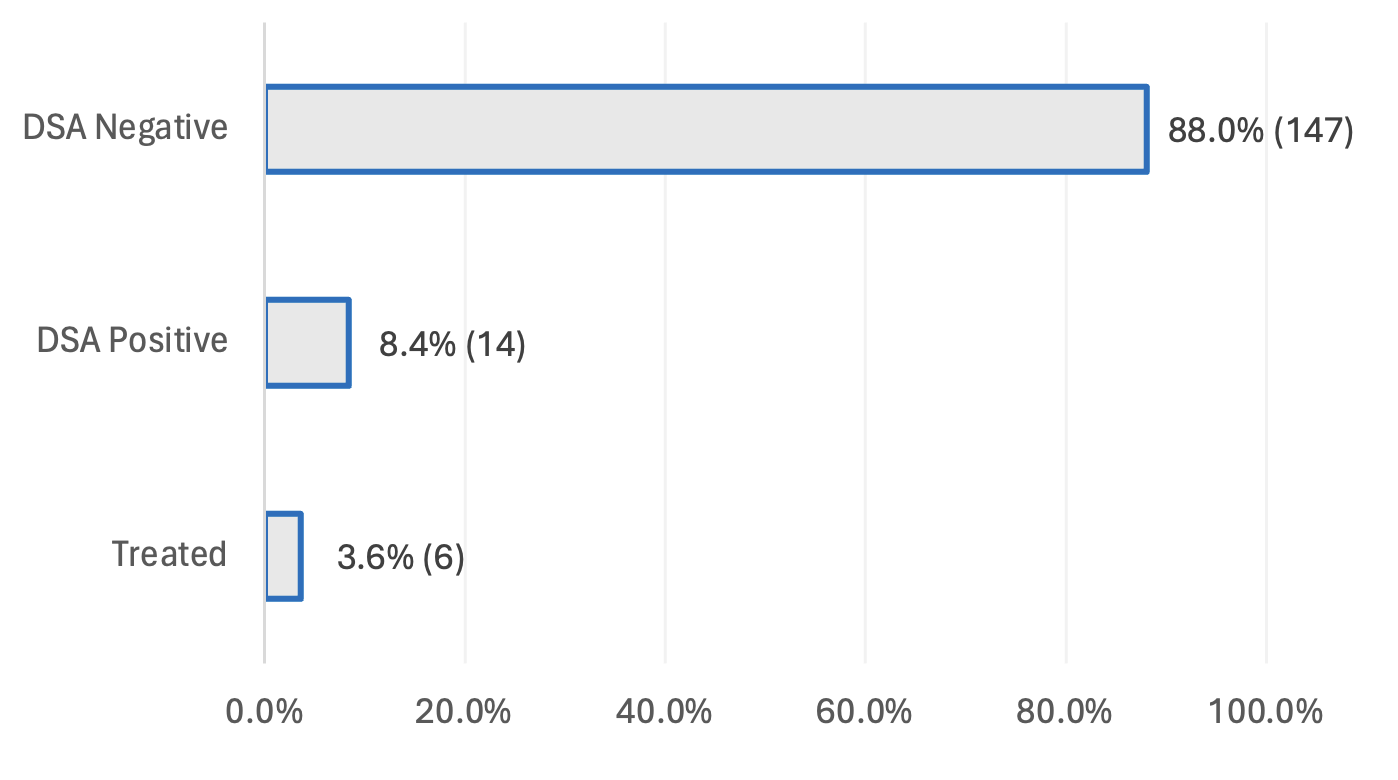
Conclusion
- The majority of CTA-negative patients had favourable clinical presentations and initial CT non-contrast findings.
- DSA resulted in complications in 5 cases (3.0%). It identified pathology in 14 (8.4%) cases, of which 6 (3.6%) were actionable.
- The utilization of DSA only occasionally alters patient management in this population and should be carefully considered.
The Surgeon Experience of Flow

INTRODUCTION
Traditional cognitive flow domains1
1. Complete concentration
2. Clear goals and feedback
3. Time speeding up/slowing down
4. Intrinsically rewarding
5. Challenge with balance of demands & skills
6 Feeling in control
7. Merging of action and awareness
8. Loss of self-conscious rumination
1. Complete concentration
2. Clear goals and feedback
3. Time speeding up/slowing down
4. Intrinsically rewarding
5. Challenge with balance of demands & skills
6 Feeling in control
7. Merging of action and awareness
8. Loss of self-conscious rumination
Flow has been linked with:
• Enhanced performance
• Wellness, decreased burnout
• Career satisfaction
While flow has not been widely studied in healthcare, it has been strongly adopted in other domains, such as elite sport.
To date, flow has been studied as a cognitive experience.
Study goal:
Understand the surgeon experience of flow through a multidimensional lens.
Cognitive:
“I would say with a really sick patient you get into the [flow] zone. Things happen very quickly, time contracts and expands, you really have no knowledge of what’s happening outside. You’re just focused on this and rolling with the punches… You feel like you’re in total control… it’s an opportunity to say nothing else matters on the planet right now.” (P14)
Physical:
“It’s also like that physical, physicality, of having your hands doing something… you have to physically focus, it’s different than having to focus on like a person’s problem or their story.” (P8)
Affective:
“I feel badly for my colleagues who don’t have the same excitement about what they do that I do. And surgery is not something you should do if you don’t have that feeling… It’s too much.” (P15)
Sociocultural:
“Surgery with them almost felt like dancing. It was the most effortless, we understood each other, we knew what our next move was going to be… I almost didn’t need to communicate. We worked in tandem so well with each other.” (P15)
Environmental:
“One thing that really enhances [that flow] state is that in the operating room, in a way you can’t be disturbed. You have your pager with you, but you kind of have an allowance to almost ignore it… You kind of can divorce yourself from everything else. Emails piling up in your inbox, you’re not aware of it. Time goes by and it’s raining outside, you don’t know. There’s a fire alarm, it doesn’t matter. You’re just in this protected place where all you have to really do is focus on this thing.” (P16
METHODS

DISCUSSION: SUPPORTING FLOW
Considering a multidimensional approach
to flow may help in optimizing
performance and promoting flourishing
Understanding Obstacles: A Neurosurgical View On Gender Disparities In Career Progression

Abstract
Background: Gender disparities persist in neurosurgery, unfortunately impacting career progression for women. Understanding these challenges is vital for fostering inclusivity.
Methods: An international survey designed using a physician wellness framework was sent to neurosurgeons. Univariate analysis (Kruskal-Wallis Test) was performed to assess various aspects of perceived career progression as a function of gender.
Results: Of the total 537 respondents (64% neurosurgeons, 6% fellows, and 30% residents), 69% identified as male, 29% as female, and 2% as other. Compared to their male colleagues, female neurosurgeons expressed greater desire to advance in their career (p<0.05) and to leave their home country in the interest of job prospects (p<0.05). Despite these aspirations, female neurosurgeons reported that they did not have available career advancement opportunities (p<0.05), that the culture in their country inhibited their career advancement (p<0.05), and that they felt subject to harassment at their workplace (p<0.05).
Conclusions: Our survey highlights significant gender-related obstacles in neurosurgical career advancement. Female neurosurgeons express strong career aspirations but face barriers such as limited opportunities, cultural impediments, and harassment. Addressing these challenges is crucial for achieving gender equity in neurosurgery.
Introduction
Despite increasing proportions of female medical students, neurosurgery remains a male-dominated field1,2. While previous research has identified several barriers impeding female neurosurgeons' career progression, such studies are limited in scope and in geographic extent. A global and in-depth understanding of these disparities is crucial for developing targeted interventions and fostering equity and inclusion within the entire field. To that end, this study assessed variations in the international neurosurgical community’s perceptions of career support and progression, with an emphasis on gender-based differences.
Methods
Informed by a comprehensive literature review investigating key challenges faced by neurosurgeons, a questionnaire addressing multiple topics was developed: the focus of this study is data on career progression comprising 16 Likert-scale questions. To reach a geographically diverse cohort, the questionnaire was administered on Survey Monkey (SurveyMonkey Inc., San Mateo, California, U.S.A) and strategically distributed globally. Data were coded from -2 (Strongly Disagree) to 2 (Strongly Agree) prior to examination by the Kruskal-Wallis H test using Python. Ethical approval was obtained by the Research Ethics Board of Unity Health at St. Michael’s Hospital.
Results
Of 657 total responses to our questionnaire, 537 respondents provided complete data on the career progression components and were included in this study (completion rate 84.3%): 68.5% (N = 368) were male, 29.2% (N = 157) female, 0.2% (N = 1) non-binary, 0.2% (N = 1) gender-fluid, and 1.8% (N = 10) preferred not to answer. The latter three groups were excluded from downstream analysis due to sample-size limitations. Male respondents consisted of 27.7% (N = 102) residents, 4.9% (N = 18) fellows, and 67.4% (N = 248) staff; female respondents of 36.3% (N = 57) residents, 8.9% (N = 14) fellows, and 54.8% (N = 86) staff. All continents were represented in this study, with respondents from Asia (38.2%, N = 205), Africa (13.2%, N = 71), North America (11.5%, N = 62), Europe (8.2%, N = 44), South America (2.2%, N = 12), and Oceania (1.9%, N = 10); continent information was not available for 133 respondents. Seven of the 16 examined questions were found to be statistically significant and are presented in Figure 1.
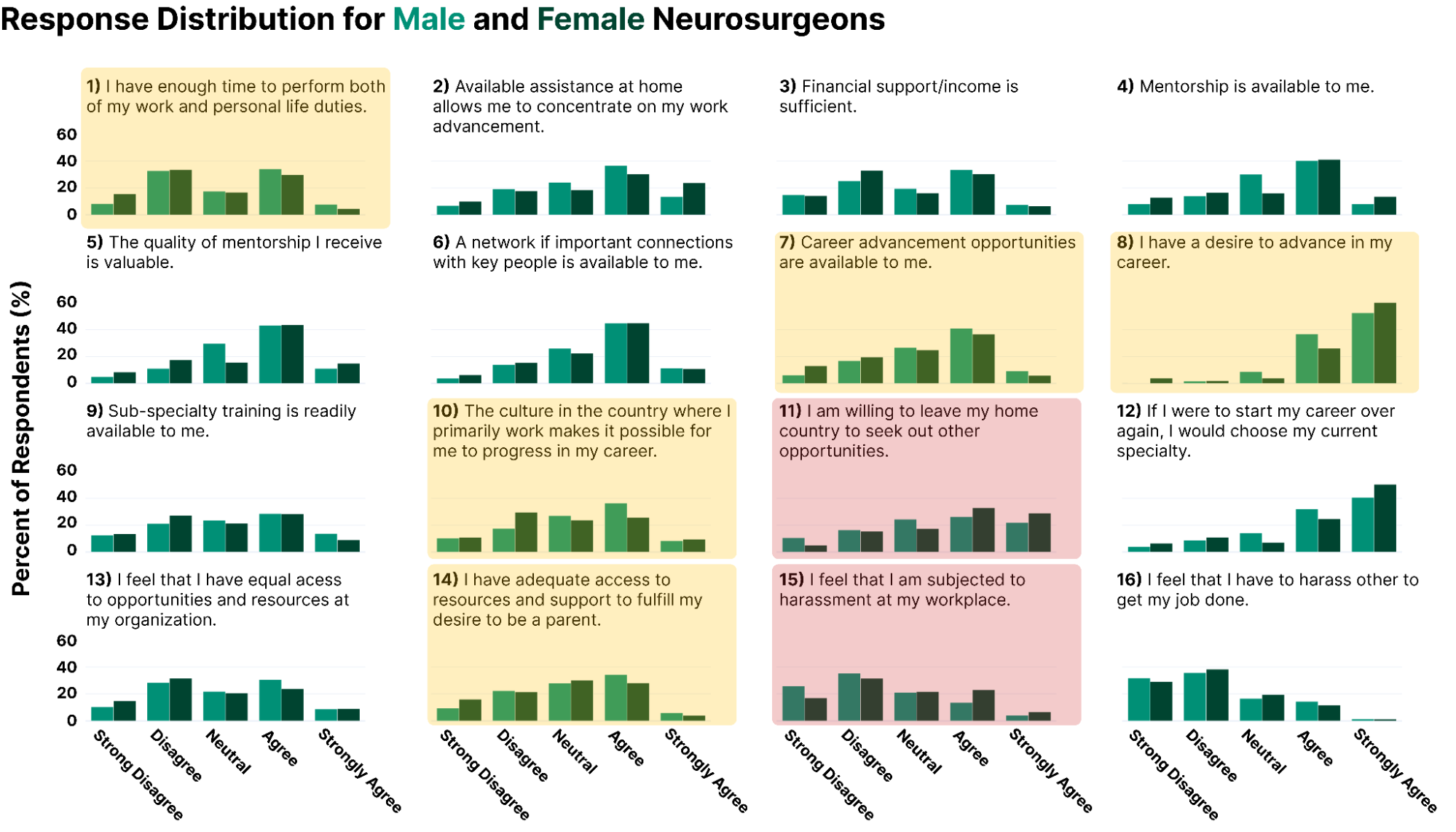
Figure 1: Respondent distribution to the 16 Likert-scale questions enquired in this study. Female neurosurgeons more strongly endorsed questions eight, 11, and 15 and less strongly endorsed questions one, seven, 10, and 14. Percents are reported out of a total for each gender. Yellow- and red-shaded areas denote statistical significance (p<.05 and p<.01, respectively).
Figure 2: A tripartite plan to move forward emphasising mentorship, parental leave policies, and a dedication to workplace equity, based on the amalgamated work of several researchers1,7,8.
Discussion
This study offers global insight into gender-based differences in perceptions of career support and progression among neurosurgeons. Females reported greater work-life balance conflicts, limited career advancement opportunities, restrictive cultural norms, and diminished access to the resources and support necessary to being a parent. Disturbingly, they also cited increased experiences of workplace harassment. Despite these systemic impediments, female respondents expressed both exceptional ambition to advance in their career and greater willingness to relocate for professional development. Work-life balance challenges, coupled with the perception of parenthood as incompatible with the demands of the specialty, create significant barriers for female neurosurgeons which are further exacerbated by restrictive cultural norms1,3. The increased incidence of inequity reported by women elucidates a nefarious yet under-discussed problem4.
While this study's global scope is a strength, limitations include the potential for self-reporting bias within survey methodologies. Nonetheless, our findings necessitate the need for prompt and systemic transformation. To that end, we echo what previous researchers have called for1,5: the establishment of formal mentorship programs, robust parental leave policies, and a zero-tolerance policy for workplace inequity. Ultimately, gender equity in neurosurgery is not simply a moral imperative; it is a practical necessity that enhances patient-provider interactions and surgical outcomes6.
While this study's global scope is a strength, limitations include the potential for self-reporting bias within survey methodologies. Nonetheless, our findings necessitate the need for prompt and systemic transformation. To that end, we echo what previous researchers have called for1,5: the establishment of formal mentorship programs, robust parental leave policies, and a zero-tolerance policy for workplace inequity. Ultimately, gender equity in neurosurgery is not simply a moral imperative; it is a practical necessity that enhances patient-provider interactions and surgical outcomes6.
References
1. Plonsker JH, Benzil D, Air EL, Woodrow S, Stippler M, Ben-Haim S. Gender Equality in Neurosurgery and Strategic Goals Toward a More Balanced Workforce. Neurosurgery. 2022;90(5):642-647.
2. Pickel L, Sivachandran N. Gender trends in Canadian medicine and surgery: the past 30 years. BMC Méd Educ. 2024;24(1):100.
3. Samuel N, McQueen SA, Barnett RR, Everson MC, Fiala C, Lau R, et al. Parenting and Childbearing in Neurosurgical Residency: Perspectives from the United States and Canada. J Surg Educ. 2023;80(4):572-580.
4. Benzil DL, Muraszko KM, Soni P, Air EL, Orrico KO, Rutka JT. Toward an understanding of sexual harassment in neurosurgery. J Neurosurg. Published online 2020:1-10.
5. Balasubramanian S, Palanisamy D, Bakhti S, Abbadi NE, Collange N, Karekezi C, et al. Women in Neurosurgery (WIN): Barriers to progress, world WIN directory and the way forward. Asian J Neurosurg. 2020;15(04):828-832.
6. Wallis CJD, Jerath A, Coburn N, Klaassen Z, Luckenbaugh AN, Magee DE, et al. Association of Surgeon-Patient Sex Concordance With Postoperative Outcomes. JAMA Surg. 2022;157(2):146-156.
7. Balasubramanian, S. et al. Women in Neurosurgery (WIN): Barriers to progress, world WIN directory and the way forward. Asian J. Neurosurg. 15, 828–832 (2020).
8. Kearns, K. N. et al. Gender Equity of Promoting Practices in Academic Neurosurgery in the United States. World Neurosurg. 158, 139–147 (2022).
2. Pickel L, Sivachandran N. Gender trends in Canadian medicine and surgery: the past 30 years. BMC Méd Educ. 2024;24(1):100.
3. Samuel N, McQueen SA, Barnett RR, Everson MC, Fiala C, Lau R, et al. Parenting and Childbearing in Neurosurgical Residency: Perspectives from the United States and Canada. J Surg Educ. 2023;80(4):572-580.
4. Benzil DL, Muraszko KM, Soni P, Air EL, Orrico KO, Rutka JT. Toward an understanding of sexual harassment in neurosurgery. J Neurosurg. Published online 2020:1-10.
5. Balasubramanian S, Palanisamy D, Bakhti S, Abbadi NE, Collange N, Karekezi C, et al. Women in Neurosurgery (WIN): Barriers to progress, world WIN directory and the way forward. Asian J Neurosurg. 2020;15(04):828-832.
6. Wallis CJD, Jerath A, Coburn N, Klaassen Z, Luckenbaugh AN, Magee DE, et al. Association of Surgeon-Patient Sex Concordance With Postoperative Outcomes. JAMA Surg. 2022;157(2):146-156.
7. Balasubramanian, S. et al. Women in Neurosurgery (WIN): Barriers to progress, world WIN directory and the way forward. Asian J. Neurosurg. 15, 828–832 (2020).
8. Kearns, K. N. et al. Gender Equity of Promoting Practices in Academic Neurosurgery in the United States. World Neurosurg. 158, 139–147 (2022).
Mind The Gap: Illuminating Gender Disparities In Neurosurgical Inclusion And Diversity

Abstract
Background: Gender disparities endure in neurosurgery, impacting the experiences of female practitioners. Unveiling these challenges is crucial for promoting inclusivity and addressing the unique obstacles faced by women in the field.
Methods: An international survey designed using a physician wellness framework was sent to neurosurgeons. Univariate analyses was performed to assess feelings of inclusion and diversity as a function of gender.
Results: Of the total 384 respondents (65% neurosurgeons, 6% fellows, and 29% residents), 71% identified as male, 27% as female, and 2% as other. Compared to their male colleagues, female neurosurgeons more strongly endorsed feeling that their career progression has been limited by their gender (p<0.05) and were less likely to feel entrusted in their surgical ability (p<0.05) or to have equal access to surgical resources (p<0.05). Furthermore, they were less likely to endorse feelings that leaders in their department were committed to creating an inclusive environment (p<0.05).
Conclusions: Our survey sheds light on significant gender-related disparities in neurosurgery. Female neurosurgeons express heightened concerns about gender-limiting career progression, reduced trust in their surgical abilities, and disparities in resource access. These findings underscore the imperative to foster a more inclusive and supportive environment within the field
Introduction
While the medical field is becoming more gender-balanced1,2, neurosurgery lags behind: indeed, women are dramatically underrepresented in neurosurgery across the globe1,3, and this lack of diversity extends across all levels of training and practice, from medical school to staff life. This unfortunately has significant implications for both career progression for women in the field and patient care, as research suggests diverse healthcare teams lead to better outcomes4. In light of this, the present study aims to quantify the extent of gender disparities in neurosurgery globally by assessing perceptions of equity, diversity, and inclusion (EDI) within the field, and identify putative causes of unequal treatment experienced by neurosurgeons.
Methods
A questionnaire was developed to assess neurosurgeons' perceptions of EDI. To reach a geographically diverse cohort, the questionnaire was administered electronically (SurveyMonkey Inc., San Mateo, California, U.S.A) and distributed globally. Likert-scale data were analyzed using the Kruskal-Wallis H test and binary data using logistic regression. Ethical approval was obtained from St. Michael’s Hospital.
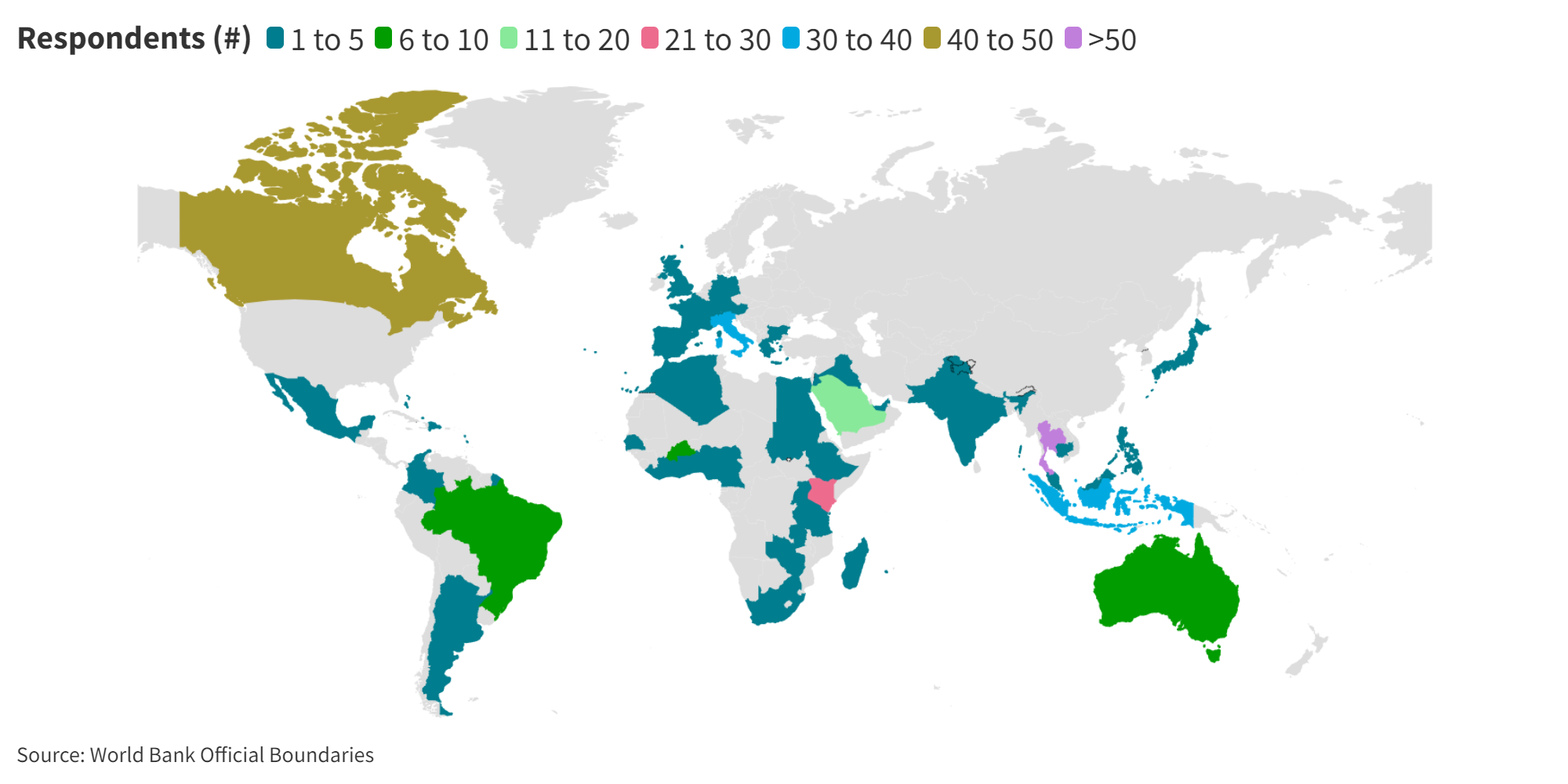
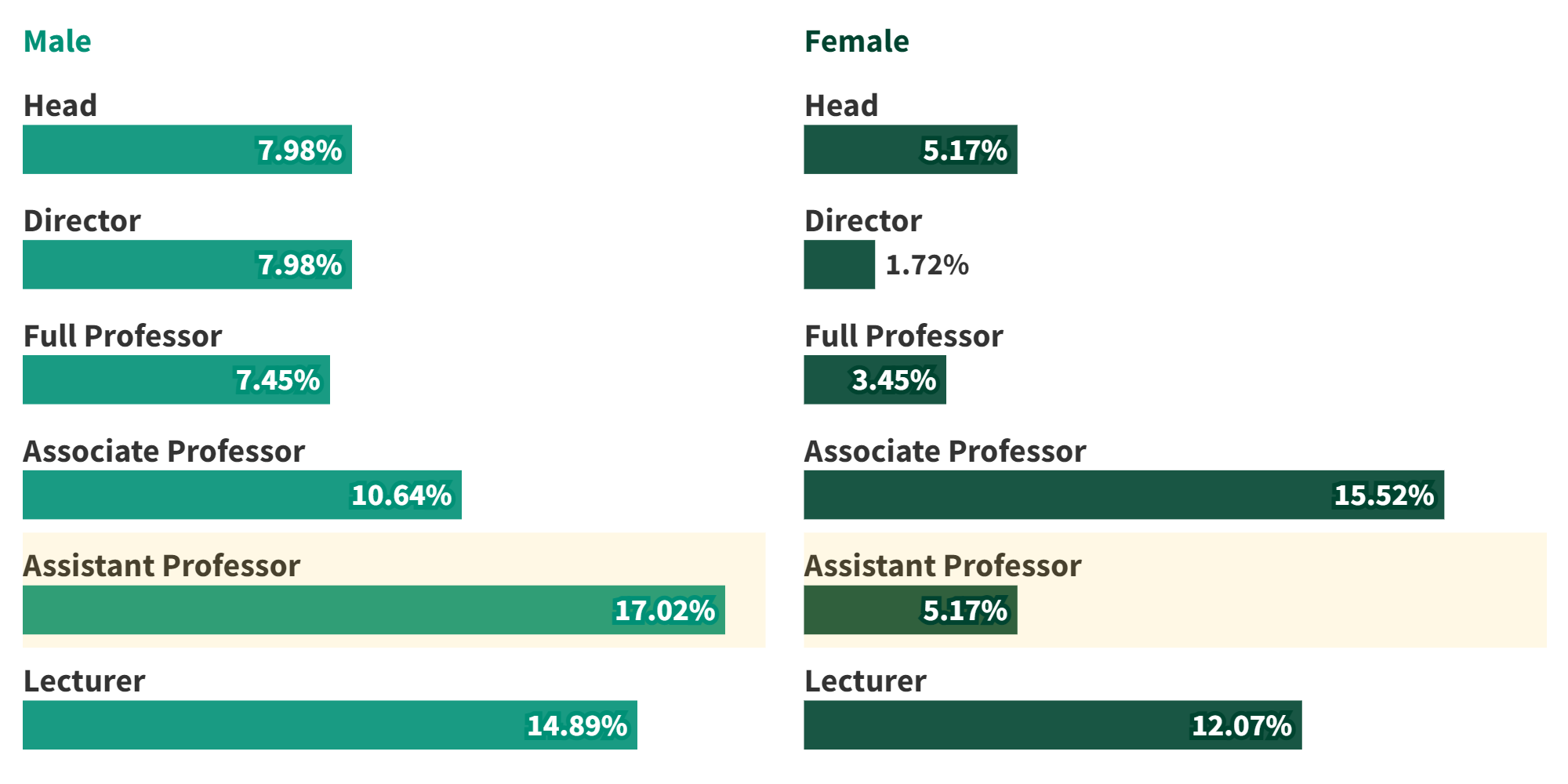


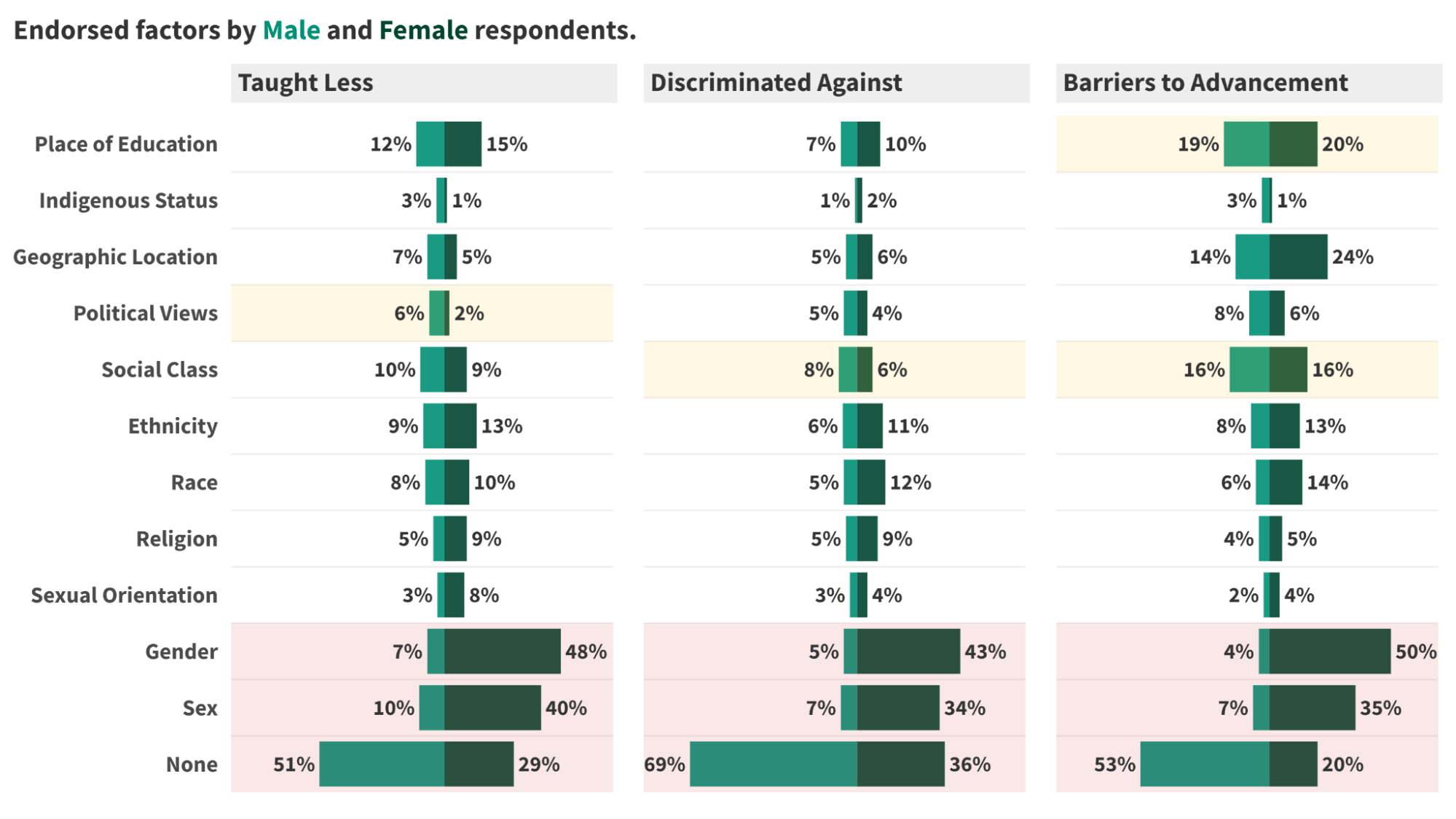
Discussion
Despite increasing numbers of women entering medicine1,2, female neurosurgeons report systemic barriers and a lack of inclusive culture, underscoring the need for cultural change beyond simply increasing female representation. Key findings of our study include:
- Gender bias impacts skill development, teamwork, and patient care: female neurosurgeons report less access to resources, less trust in their abilities, and hindered career progression, despite demonstrating great ambition.
- Regional differences in gender disparities: responses of female and male neurosurgeons showed signficiant continent interactions, emphasizing the need for context-specific, culturally-informed solutions5.
- Multiple factors contribute to perceptions of unequal treatment: gendered stereotypes, work-life balance conflicts, political views, and social class all play a role.
- Men also report inequities: this suggests a growing awareness of privilege and its impact on creating barriers as well as the need for holistic change in neurosurgical culture encompassing the unique desires of various stakeholders.
References
1. Pickel L, Sivachandran N. Gender trends in Canadian medicine and surgery: the past 30 years. BMC Méd Educ. 2024;24(1):100.
2. Sepúlveda-Vildósola, A. C., González, H.-M., López-Sepúlveda, M. F. & Martínez-Escobar, C. B. Trends in Medical Specialization and Employability in Mexico According to Gender. Arch. Méd. Res. 53, 205–214 (2022).
3. Odell, T. et al. Gender Disparity in Academic Neurosurgery. Cureus 11, e4628 (2019).
4. Wallis, C. J. et al. Comparison of postoperative outcomes among patients treated by male and female surgeons: a population based matched cohort study. BMJ 359, j4366 (2017)
5. Monrouxe, L. V. et al. Medical Students’ and Trainees’ Country-By-Gender Profiles: Hofstede’s Cultural Dimensions Across Sixteen Diverse Countries. Front. Med. 8, 746288 (2022).
6. Plonsker JH, Benzil D, Air EL, Woodrow S, Stippler M, Ben-Haim S. Gender Equality in Neurosurgery and Strategic Goals Toward a More Balanced Workforce. Neurosurgery. 2022;90(5):642-647.
7. Balasubramanian, S. et al. Women in Neurosurgery (WIN): Barriers to progress, world WIN directory and the way forward. Asian J. Neurosurg. 15, 828–832 (2020).
2. Sepúlveda-Vildósola, A. C., González, H.-M., López-Sepúlveda, M. F. & Martínez-Escobar, C. B. Trends in Medical Specialization and Employability in Mexico According to Gender. Arch. Méd. Res. 53, 205–214 (2022).
3. Odell, T. et al. Gender Disparity in Academic Neurosurgery. Cureus 11, e4628 (2019).
4. Wallis, C. J. et al. Comparison of postoperative outcomes among patients treated by male and female surgeons: a population based matched cohort study. BMJ 359, j4366 (2017)
5. Monrouxe, L. V. et al. Medical Students’ and Trainees’ Country-By-Gender Profiles: Hofstede’s Cultural Dimensions Across Sixteen Diverse Countries. Front. Med. 8, 746288 (2022).
6. Plonsker JH, Benzil D, Air EL, Woodrow S, Stippler M, Ben-Haim S. Gender Equality in Neurosurgery and Strategic Goals Toward a More Balanced Workforce. Neurosurgery. 2022;90(5):642-647.
7. Balasubramanian, S. et al. Women in Neurosurgery (WIN): Barriers to progress, world WIN directory and the way forward. Asian J. Neurosurg. 15, 828–832 (2020).
The Impact of Screening for Anxious and Depressive Symptoms on the Outcome of Patients with a Mild Traumatic Brain Injury
INTRODUCTION
An estimated 27-69 million individuals worldwide sustain a Traumatic Brain Injury (TBI) each year, establishing it as a prominent contributor to health impairment and disability1,2. Most cases (70-90%) fall under the category of mild with an estimated annual incidence rate of 100-300 cases per 100,000 individuals treated in hospitals3. This figure, however, does not encompass the numerous untreated cases, suggesting that the true population-based incidence could be considerably higher, emphasizing the significance of mild TBI (mTBI) as a critical public health concern3. Many victims experience post-injury neuropsychological issues such as anxiety and depression4, which are associated with more post-concussive symptoms and worse functional outcomes5. These psychiatric disorders occur at a higher prevalence and for a longer duration in TBI patients compared to the general population6,7.
OBJECTIVE
The overarching objective of the project is to assess if the early identification of these symptoms through the administration of questionnaires may serve as an effective tool to help clinicians detect mTBI patients at risk of developing anxiety and/or depression and thus refer them to the necessary interventions to prevent negative impacts on their recovery and ultimately improve outcome.
HYPOTHESIS
We believe that the results from the questionnaires will aid clinicians to properly refer patients to resources and treatments targeting anxious and/or depressive symptoms and in doing such, improve their outcome.
METHODOLOGY
QUESTIONNAIRES

RESULTS
Table 1. Prescribed Interventions in Pre- and Post-Questionnaire Groups

Indicates the number of patients that were referred to specific resources to help improve their recovery and outcome, including vestibular therapy, neuropsychology, out-patient rehabilitation, and psychology. The numerical values signify the raw count of patients, while the figures in parentheses denote the corresponding percentage within the sample. The patients in the post-questionnaire group were more frequently referred to each intervention compared to those in the pre-questionnaire group, with a significant difference between both groups for vestibular therapy.
Table 2. Descriptive Statistics and Correlations between Variables of Post-Questionnaire Group
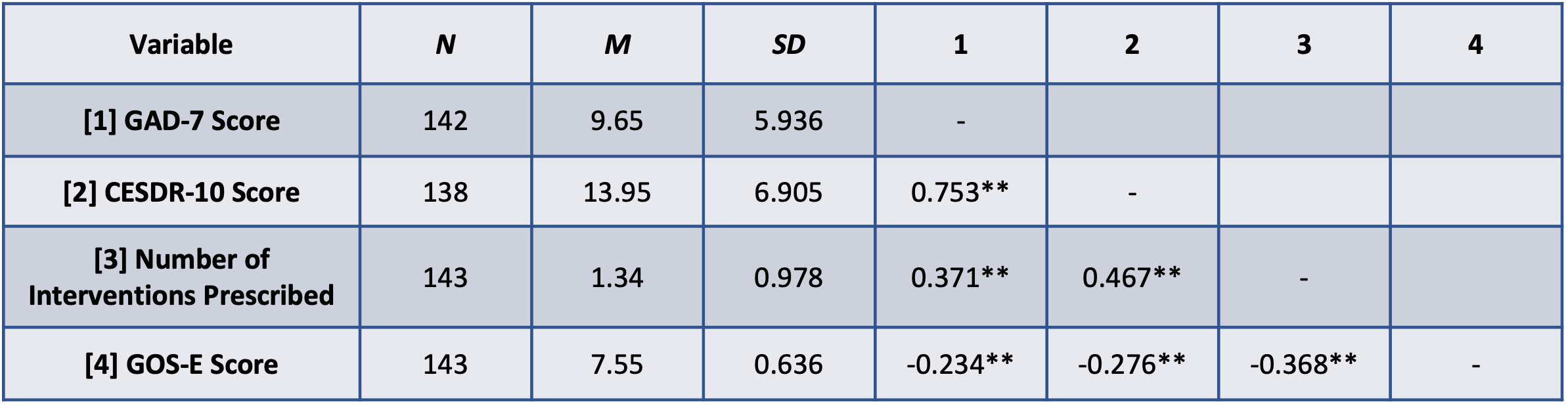
**, correlation is significant at the 0.01 level
The sample size, mean, and standard deviation of each variable is presented in this table. The variables, which include GAD-7 score, CESDR-10 score, number of interventions prescribed, and Glasgow Outcome Scale-Extended (GOS-E) score, were correlated between each other. The Pearson correlation coefficient (r) is reported in the table and indicates that all variables significantly correlate with one another.
RESULTS cont.
Figure 1. Mean Number of Referrals to Various Interventions
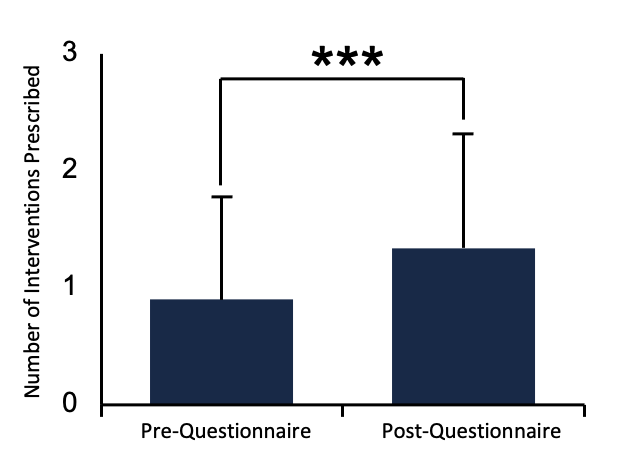
Compared the mean number of referrals to various interventions between the pre- and post-questionnaire groups using ANOVA. Patients who received the questionnaires (M=1.34, SD=0.978) were referred to significantly more interventions than those who did not (M=0.90, SD=0.876, p<0.001).
Figure 2. Mean GOS-E Score
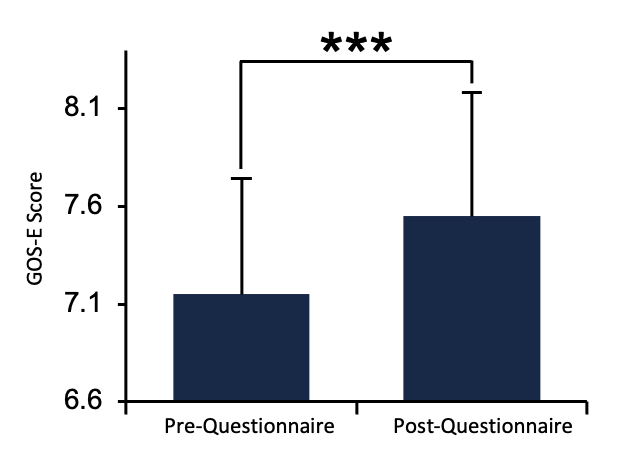
Compared the mean GOS-E score between the pre- and post-questionnaire groups using ANOVA. Patients who received the questionnaires (M=7.55, SD=0.636) have significantly higher GOS-E scores than those who did not (M=7.15, SD=0.595, p<0.001).
CONCLUSION
Patients who were provided with the questionnaires were directed to a significantly greater number of resources compared to those who were not. Specifically, among the four interventions assessed, only vestibular therapy showed significantly more referrals in the post- compared to the pre-questionnaire group. In the post- questionnaire cohort, higher scores on both questionnaires correlated with lower GOS-E scores. This suggests that patients experiencing heightened levels of anxiety and/or depression exhibit poorer outcomes compared to those with lower levels of these psychiatric conditions. Additionally, as the number of interventions increase, patient outcomes worsen, which is likely due to greater clinical complexity and thus, the requirement for more treatment. In summary, although the administration of these questionnaires did not have a significant impact on referrals for most of the specific interventions, our data shows that patients suffering from anxiety and depression post mTBI generally require more interventions and have poorer outcomes than those who do not.
REFERENCES
[1] Statistics. Brain Injury Canada. braininjurycanada.ca/en/statistics/#TBI. [2] Williamson C, Rajajee V. Traumatic brain injury: Epidemiology, classification, and pathophysiology. Wolters Kluwer. 2023. [3] Cassidy JD, et al. J Rehabil Med. Feb 2004;(43 Suppl):28- 60. [4] Delmonico RL, et al. Pm r. Jul 2022;14(7):753-763. [5] Marinkovic I, et al. Brain Sci. Nov 27 2020;10(12). [6] Schwarzbold M, et al. Neuropsychiatr Dis Treat. Aug 2008;4(4):797-816. [7] Koponen S, et al. Am J Psychiatry. Aug 2002;159(8):1315-21. [8] Spitzer RL, et al. Arch Intern Med. May 22 2006;166(10):1092-7. [9] Björgvinsson T, et al. Assessment. Aug 2013;20(4):429-36. [10] Miller WC, et al. Spinal Cord. Apr 2008;46(4):287-92. [11] Radloff LS. Applied Psychological Measurement. 1977;1(3):385-401.
ACKNOWLEDGMENTS

The national impact of traumatic brain injury on labor markets: a canada-wide observational cohort study of post-injury employment and personal income loss
Background
•Traumatic brain injury frequently affects working age patients and contributes to substantial worldwide morbidity, reduced quality of life and mortality
•Interviews with TBI survivors highlight that economic consequences matter to patients but are neglected
Study Aim
To quantify the labor market costs of TBI among tax-filing survivors over a 3-year post-injury period in a Canadian cohort. We also sought to estimate the national labor market losses incurred over the study period
Study Design
•We identified tax-filing adult survivors (age 19-61) with TBI between 2007-2017
•Matched difference-in-difference analysis
•Primary outcomes: change in employment and personal income loss. Comparison group is comprised of resampled individuals from the cohort of interest in their pre-injury years
Cohort creation with reasons for inclusion and exclusion.
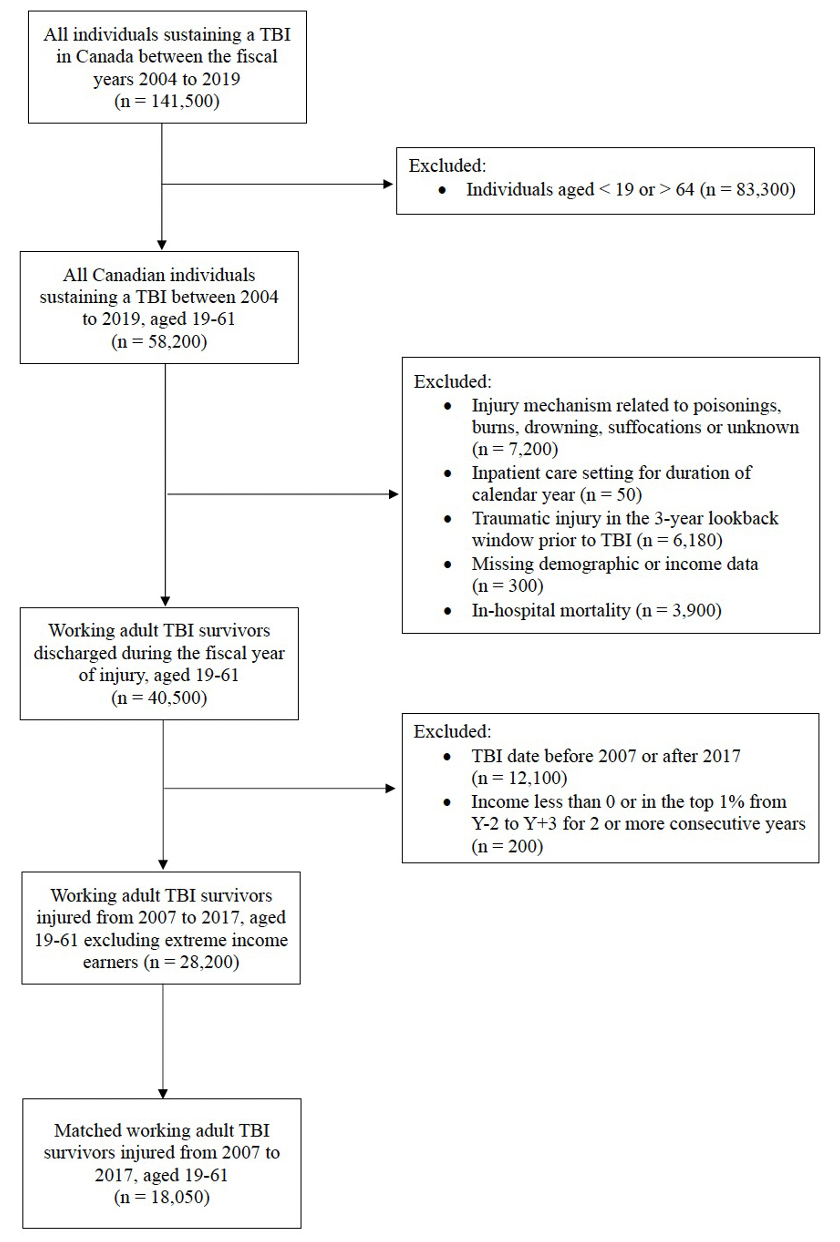
Matched Cohort Schematic
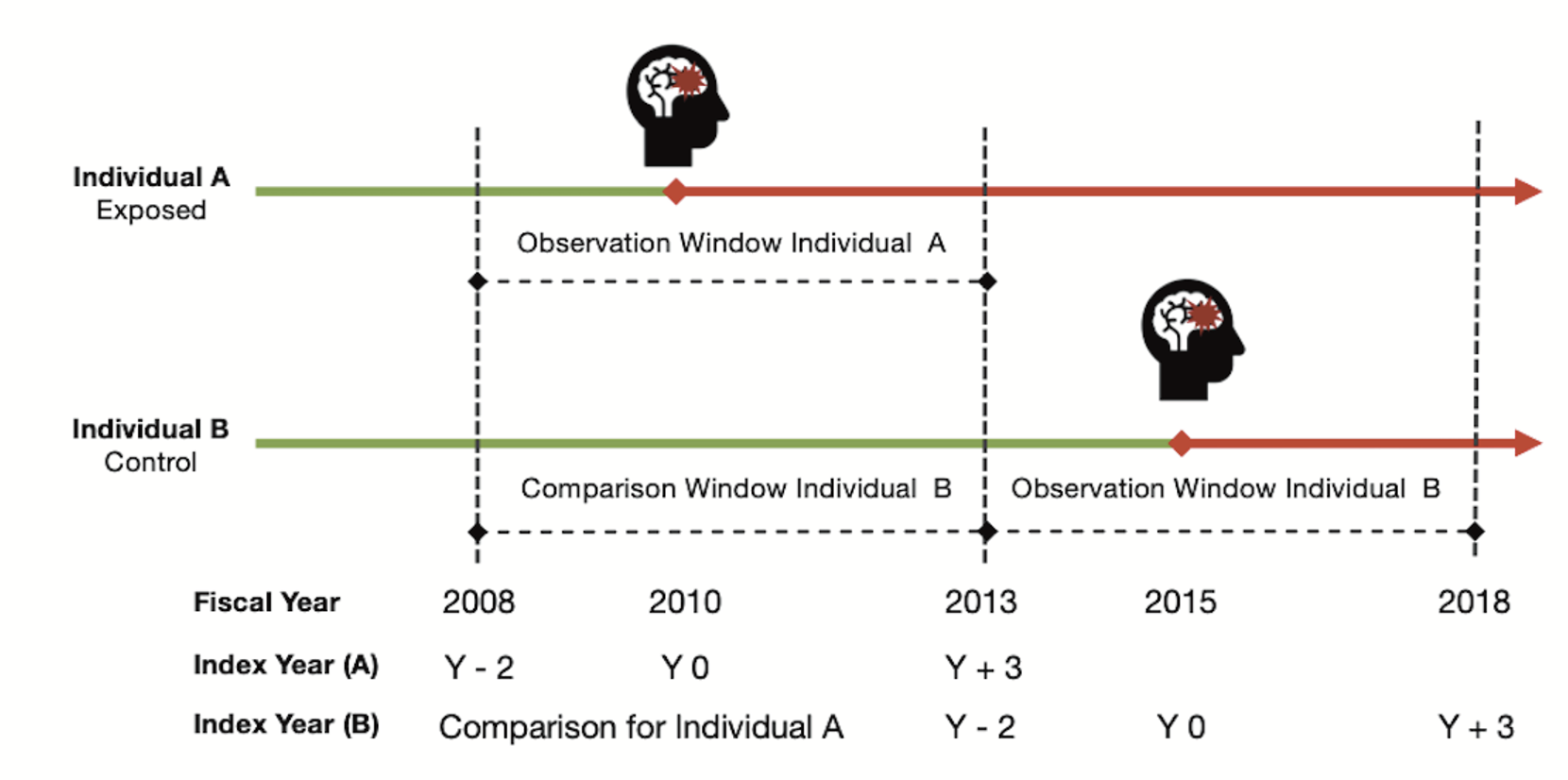
Results
18,050 matched TBI survivors, of whom 82% were employed at time of injury. Mean income was $46,000 CDN.Using the overall annualized DID quantities, the estimated total income loss incurred by the TBI survivor cohort was $500 million CDN between Y+1 to Y+3. We estimated that 7.8% (or 2,195) TBI survivors were displaced per annum from the workforce (newly unemployed after TBI) for three post-injury years, Y+1 to Y+3
Difference in difference plots depicting changes in income and employment after TBI.
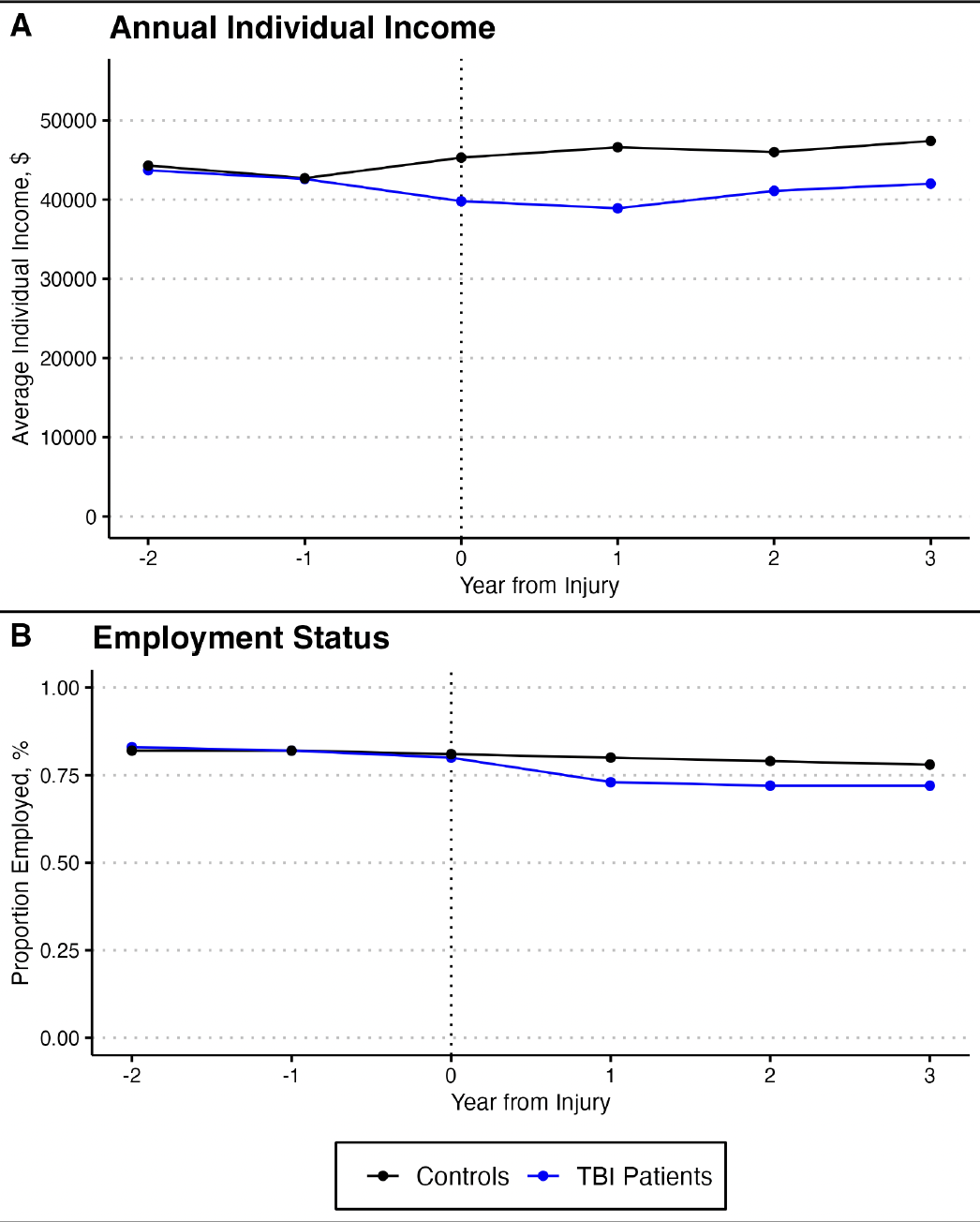
Days at home after traumatic brain injury: moving beyond mortality to evaluate patient-centered outcomes using population health data
Background
- Days at home (DAH) is an outcome measure that is now widely applied to various clinical trial and health service evaluation initiatives across a spectrum of diseases
- DAH is considered a patient-centered outcome that incorporates a functional dimension beyond mortality, resulting in a pragmatic, easily calculated metric with face validity and correlation to patient values
- The measure of DAH has therefore emerged as a compelling, interpretable and meaningful instrument to more holistically measure quality of life, duration of life, and intensity of health resource utilization in health administrative contexts
Objective
Our specific aims were to report DAH at differing post-injury time points and select a sufficiently responsive outcome assessment point for moderate to severe TBI patients. We additionally sought to assess the construct and predictive validity of DAH and to determine its minimally important difference (MID).
Methods
This multicenter retrospective observational cohort study utilized linked health administrative data sources to identify adults with moderate to severe TBI presenting to trauma centers in Ontario, Canada between 2009 and 2021.
- DAH at 180 days (DAH180days) reflects the total number of days spent alive and at home excluding the days spent institutionalized in acute care, rehabilitation, inpatient mental health settings or post-acute readmissions.
- Construct validity was determined using hierarchical quantile regression to assess the associations between clinical and injury covariates with DAH180days.
- Predictive validity was assessed using Spearman rank correlation between DAH180days and future DAH time points.
- We estimated minimally important difference (MID) in DAH180days using both anchor and distribution-based methods.
Cohort creation diagram depicting reasons for subject exclusion.
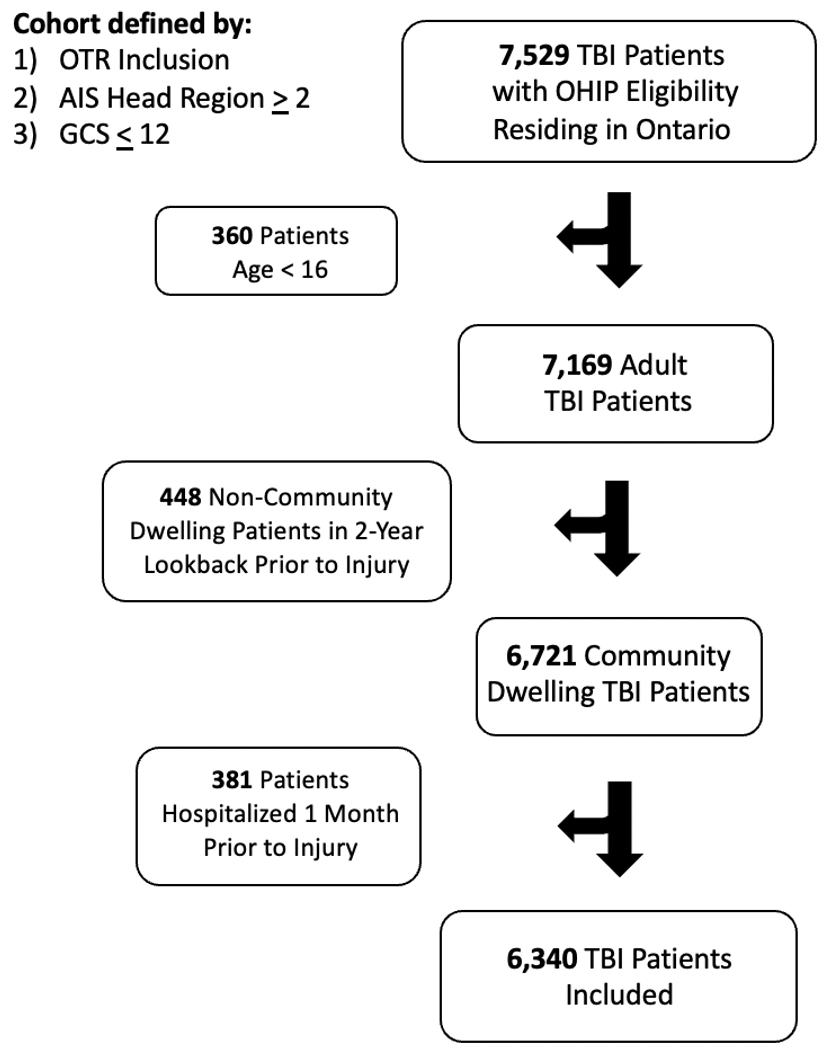
Results
- There were 6340 patients that met inclusion criteria. Median DAH180days was 70 days (interquartile range 0-144). Mortality occurred in 2162 (34.1%) patients within 90 days following injury.
- Patients in the lower DAH180days group were more commonly older with higher pre-injury health resource utilization and greater injury severity.
- Increased health resource utilization at baseline, older age, increasing cranial injury severity and major extracranial injuries were significantly associated with fewer DAH180days. DAH180days was correlated to DAH counts at 1 year, 2 years and 3 years.
- The average MID estimated from anchor-based and distribution-based methods was 18 days.
Histograms depicting days at home outcome distributions at 30-, 90-,180-days, 1 year, 2 years and 3 years (panels A-F).
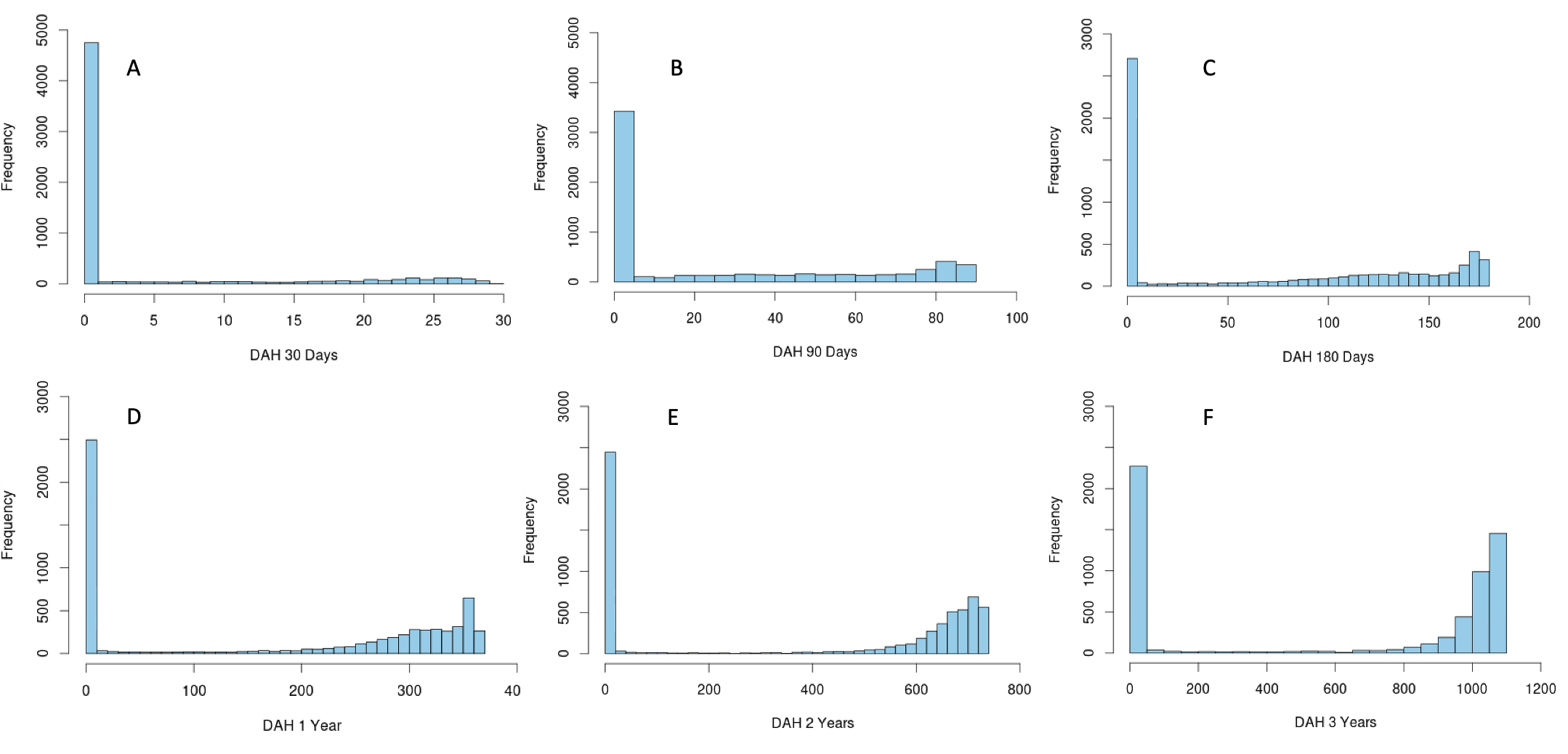
NIRS regional oxygen saturation based cerebrovascular reactivity in the recovery from moderate/severe TBI
Background
- Significant advancements have been made in the role of cerebrovascular reactivity (CVR) monitoring in the acute phase following moderate-to-severe TBI.1 Near-infrared spectroscopy (NIRS) regional cerebral oxygen saturation (rSO2)-based CVR monitoring has enabled entirely non-invasive, continuous monitoring during both acute and long-term phases of care.2
- To date, long-term post-injury CVR has not been properly characterized after traumatic brain injury (TBI). This study aims to compare CVR in those recovering from moderate-to-severe TBI with a healthy control group.
Methods
- This prospective study consisted of two distinct cohorts. The first group consisted of healthy adult volunteers. The second consisted of adult patients that sustained moderate-to-severe TBI with recordings performed at 3-, 6-, and 12-month follow-up.
- Arterial blood pressure (ABP) was collected continuously and non-invasively through a Finapres Nova finger cuff. Right and left frontal rSO2 was also collected continuously with the Covidien INVOS 7100. These were utilized to calculate an entirely non-invasive collection of the ABP-based cerebral oxygen index (COx_a). (Figure 1)

Figure 1. The setup of an entirely non-invasive collection of COx_a.
Results
- In total, 101 healthy volunteers were recruited with one 30-min recording for each subject.
- There were 29 chronic TBI patients for which at least one follow-up recording was available at 3-,6-, or 12-months and a total of 65 30-min recordings were per-formed during follow-up.
- In the healthy cohort,COx_a was not statistically different between males and females or in the dominant and non-dominant hemi-spheres.
- In the TBI cohort, COx_a was not statistically different between the first and last available follow-up or by the side of cranial surgery. Surprisingly, CVR, as measured by COx_a, was statistically better in those recovering from TBI than those in the healthy cohort. (Figure 2)
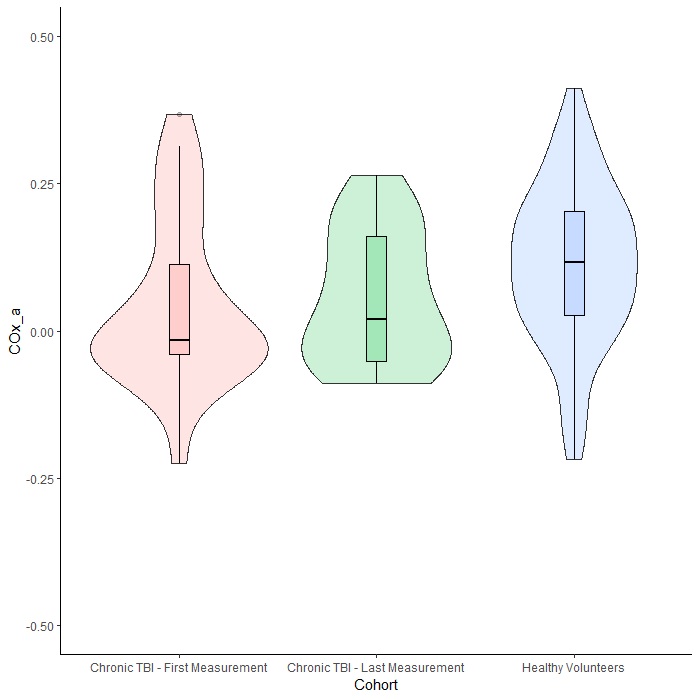
Figure 2. A violin plot of the distribution of average arterial blood pressure (ABP)-derived cerebral oxygen index (COx_a) by cohort. Note the significantly higher values of the healthy volunteer group (blue) compared to the first available (rose) or last available (green) measurement in the chronic traumatic brain injury (TBI) cohort; however, a high degree of overlap is still present.
Conclusions
This prospective study leveraged novel techniques of non-invasively measuring CVR to evaluate various metrics in both healthy volunteers and chronic TBI patients. Within the cohort of healthy volunteers, CVR, as measured by COx_a, did not differ by biologic sex or the hemisphere of language dominance. Compared to the healthy volunteers, chronic TBI patients had more active CVR at follow-up with a trend towards normalization of CVR at last available follow-up, as determined by COx_a.
References
- Czosnyka, M.; Smielewski, P.; Piechnik, S.; Steiner, L.A.; Pickard, J.D. Cerebral Autoregulation Following Head Injury. J. Neurosurg. 2001, 95, 756–763.
- Gomez, A.; Dian, J.; Zeiler, F.A. Continuous and Entirely Non-Invasive Method for Cerebrovascular Reactivity Assessment: Technique and Implications. J. Clin. Monit. Comput. 2020, 35, 307–315.
Acknowledgements
Alwyn Gomez is supported through a CIHR Fellowship (Grant #: 472286)

Gomez, A.; Marquez, I.; Froese, L.; Bergmann, T.; Sainbhi, A.S.; Vakitbilir, N.; Islam, A.; Stein, K.Y.; Ibrahim, Y.; Zeiler, F.A. Near-Infrared Spectroscopy Regional Oxygen Saturation Based Cerebrovascular Reactivity Assessments in Chronic Traumatic Neural Injury versus in Health: A Prospective Cohort Study. Bioengineering 2024, 11, 310.
Left temporal aneurysm resection: surgical approach in Pial-Pial collateral formation from the posterior temporal artery secondary to left internal artery occlusion

BACKGROUND
- Carotid occlusion may lead to formation of intracranial non-moyamoya collateral circulatory networks
- Uncommonly, hemodynamic stress in these fragile collateral networks may lead to aneurysm formation
- Treatment of these anuerysms is nuanced and often through open neurosurgery due to the small size of these collateral vessels
CASE REPORT
- 69 year old, right hand dominant man presented with 1 week history of headache and sudden altered level of consciousness
- Patient was stabilized and brought to the ER where CT scan showed a left temporal intraparenchymal hemorrhage
- CT angiography showed a 4 mm aneurysm inside the temporal hematoma; DSA was also done
Figure 1

A. Plain CT head showing a left temporal intraparenchymal hemorrhage
B. CT angiography showing a 4 mm aneurysm (red arrow) at the antero-infero-medial aspect of the left temporal hematoma; we also noted left cervical ICA occlusion (not shown)
C. 3D reconstruction of CTA showing the left temporal aneurysm with no clear vessel of origin
B. CT angiography showing a 4 mm aneurysm (red arrow) at the antero-infero-medial aspect of the left temporal hematoma; we also noted left cervical ICA occlusion (not shown)
C. 3D reconstruction of CTA showing the left temporal aneurysm with no clear vessel of origin
Figure 2
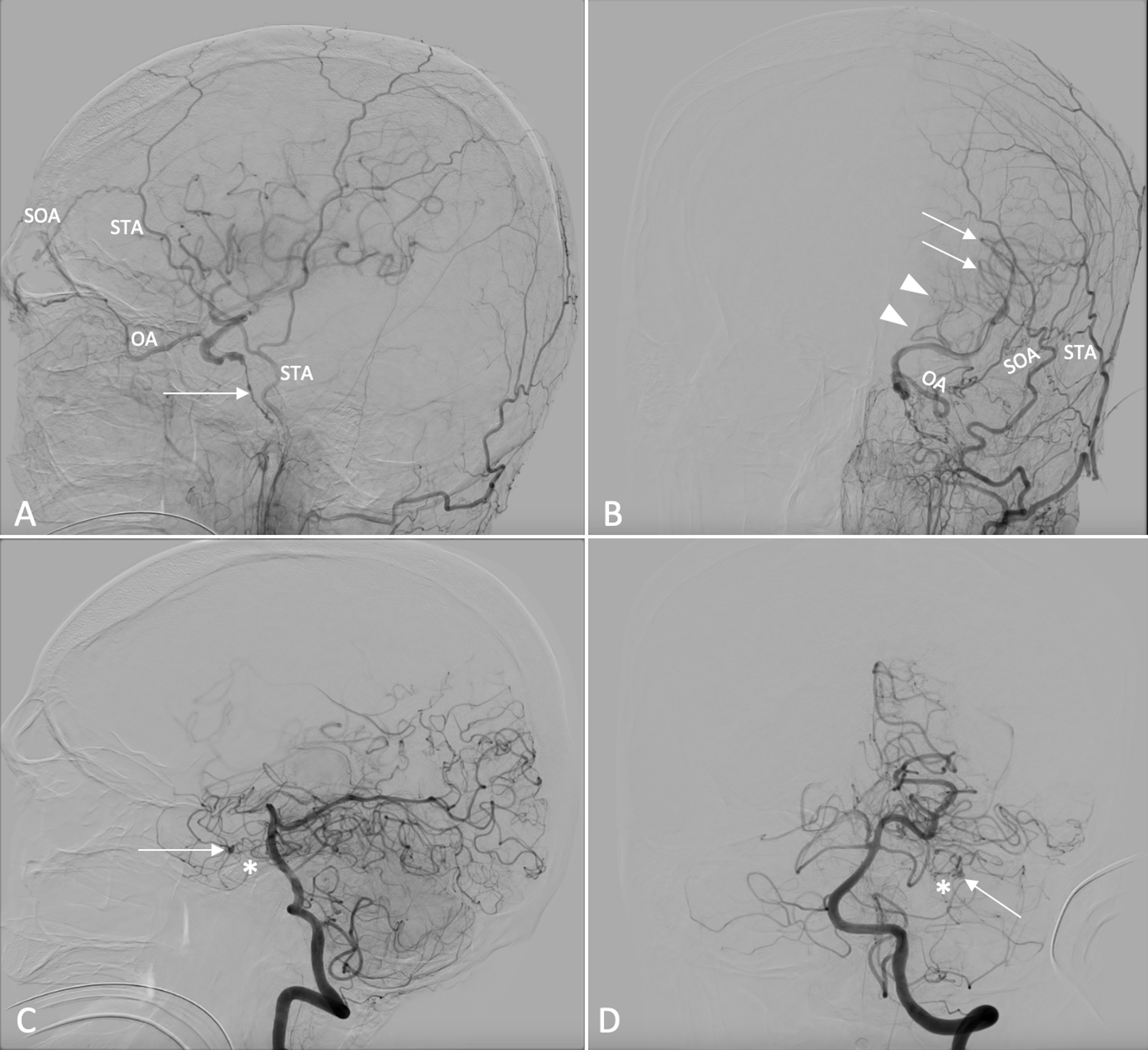
A. DSA lateral view of the left common carotid artery showing flow through the left superficial temporal artery (STA) supplying the left superior orbital artery (SOA), providing retrograde flow to the left ophthalmic artery (OA) and subsequently the superior trunk of the left MCA. Also shown is retrograde flow through the occluded left ICA (arrow)
B. Oblique view of A
C: DSA lateral view of the left vertebral artery showing the pial- pial collateral network mainly from the posterior cerebral artery via the posterior temporal artery, supplying the left temporal lobe (asterisk) and the aneurysm within this network (arrow)
D: A-P view of C, collateral network (asterisk) and aneurysm (arrow) are shown
B. Oblique view of A
C: DSA lateral view of the left vertebral artery showing the pial- pial collateral network mainly from the posterior cerebral artery via the posterior temporal artery, supplying the left temporal lobe (asterisk) and the aneurysm within this network (arrow)
D: A-P view of C, collateral network (asterisk) and aneurysm (arrow) are shown
MANAGEMENT
- Decision was made to evacuate the hematoma and obliterate the aneurysm
- Pre-operative keypoints:
- STA preservation is key as it supplies the supraclinoid internal carotid through the OA
- Excision of aneurysm preferred as the pial-pial network collaterals are small and fragile
- We then proceeded with a left temporal craniotomy, with evacuation of hematoma and resection of aneurysm, cognizant of STA dissection and preservation in our approach
Figure 3
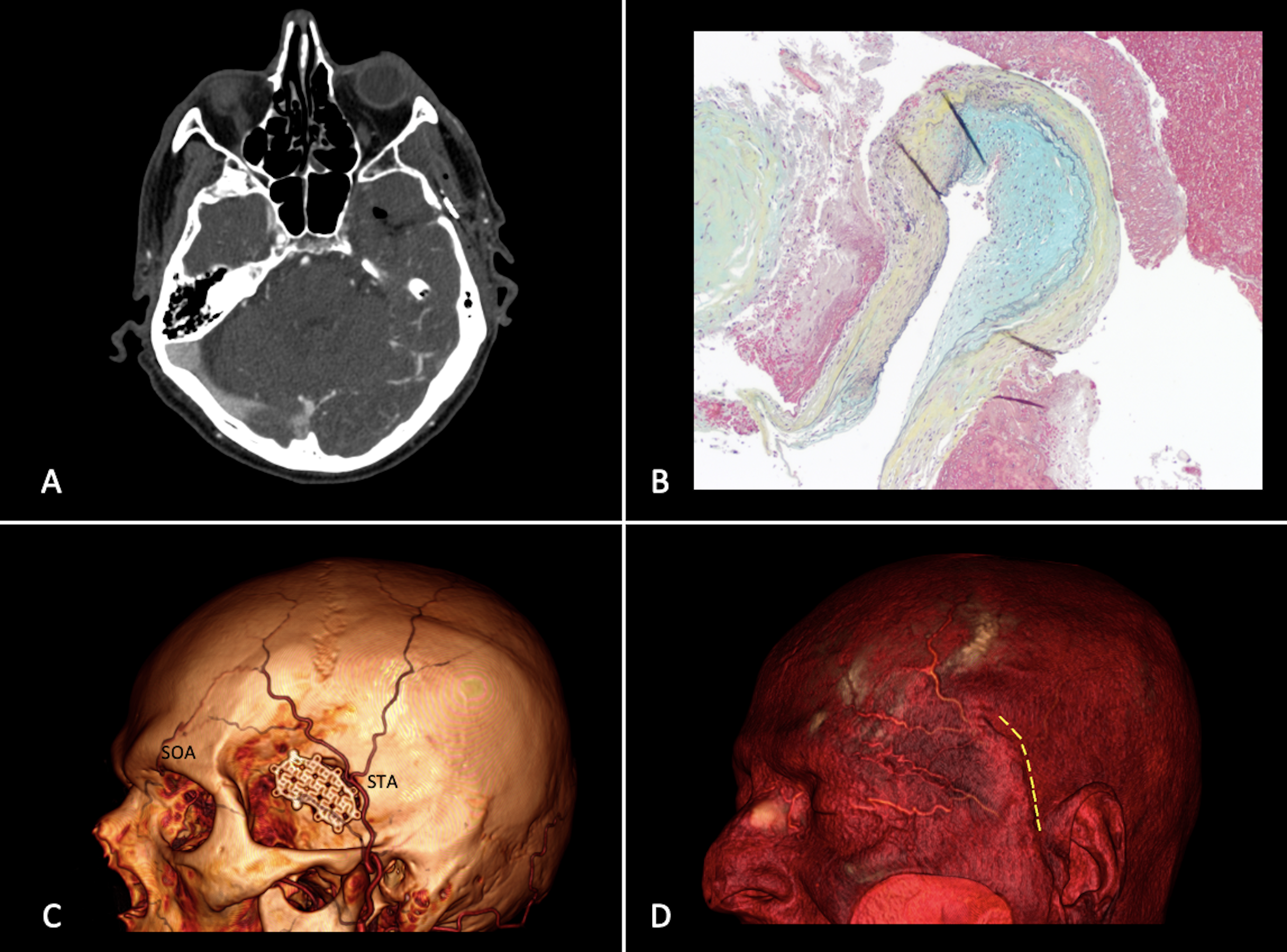
A. Postoperative cranial CTA showing excision of the aneurysm along with the adjacent pial vascular network
B. Histopathological slide showing focal intimal thickening, alternating with loss of the internal elastic lamina and thinning/loss of the media, leaving only abnormal in- timal and attenuated adventitial layers (Musto/Movat stain)
C. 3D reconstruction of postoperative CTA showing preservation of the STA and ECA-ICA anastomosis
D. Soft tissue overlay of the three-dimensional reconstruction in C showing the skin incision (adjacent dashed yellow lines) in relation to the STA
PATIENT COURSE
- Patient had gradual improvement after surgery; to extubated on post-operative day 7
- Admitted for 3 weeks, for rehabilitation and physical therapy
- On 3 month follow-up was ambulatory, conversant, and independent in all tasks; has some memory disturbances
LESSONS
- This case highlights the importance of accurately assessing cerebrovascular anatomy in patients with carotid occlusion and collateral network aneurysms
- Open surgery is preferred in these case due to the distal location and fragile nature of parent vessels
- Preservation of key feeding arteries and major collateral ciurculation is vital in maintaining cerebral perfusion, and must be balanced with aneurysm obliteration
Is there an association between geographical location of patients in NS and management of unruptured, incidental intracranial aneurysm?

Background
- Management of unruptured intracranial aneurysms (UIA) takes 2 major forms: monitor or repair.
- Decision is not always straightforward.
- Many factors are considered in decision making but rarely distance from care centre.
- Relevant studies have mixed results.
Objectives
- To determine whether proximity to our tertiary care centre was associated with the management of patients incidentally found to have a UIA.
Methods
iHRM: inside of the Halifax Regional Municipality
oHRM: outside of the Halifax Regional Municipality
The tertiary care center is within the Halifax Regional Municipality (HRM)
oHRM: outside of the Halifax Regional Municipality
The tertiary care center is within the Halifax Regional Municipality (HRM)
Results
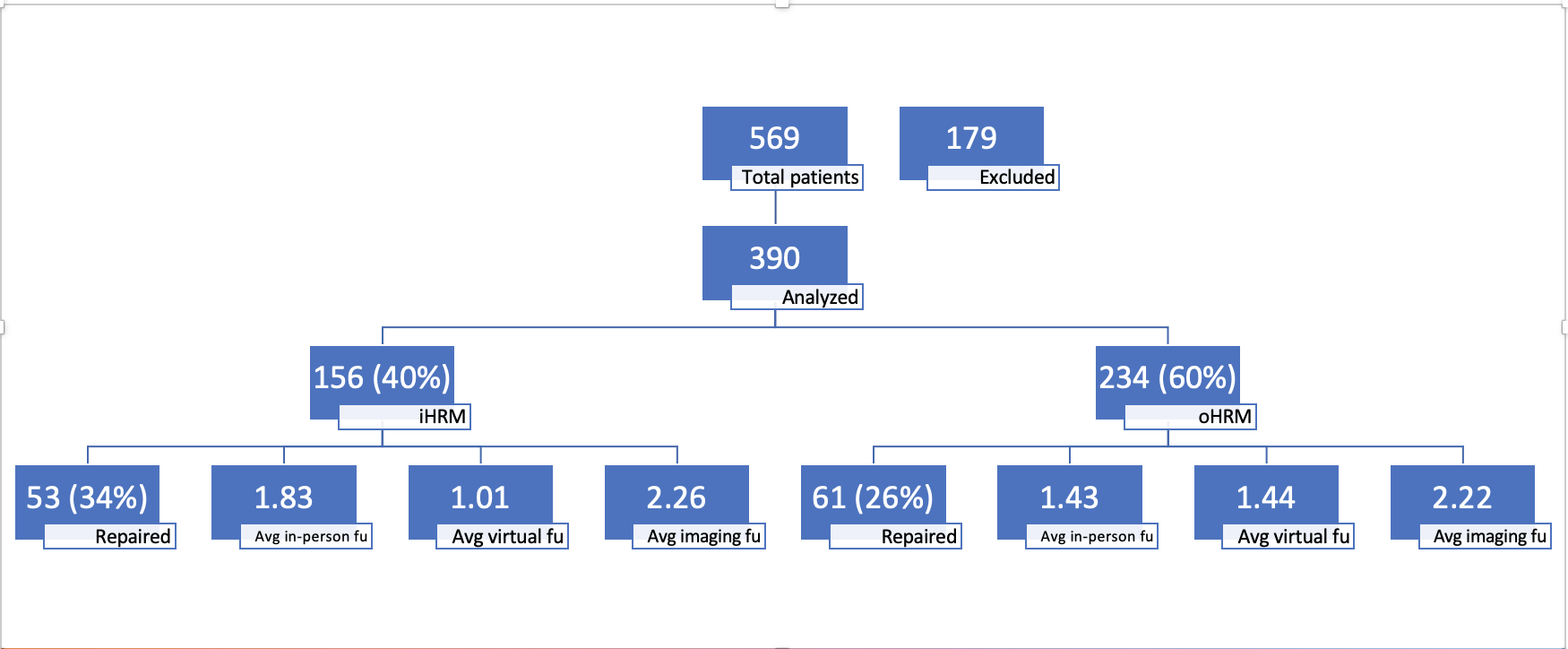
Figure 1. Overview of Results
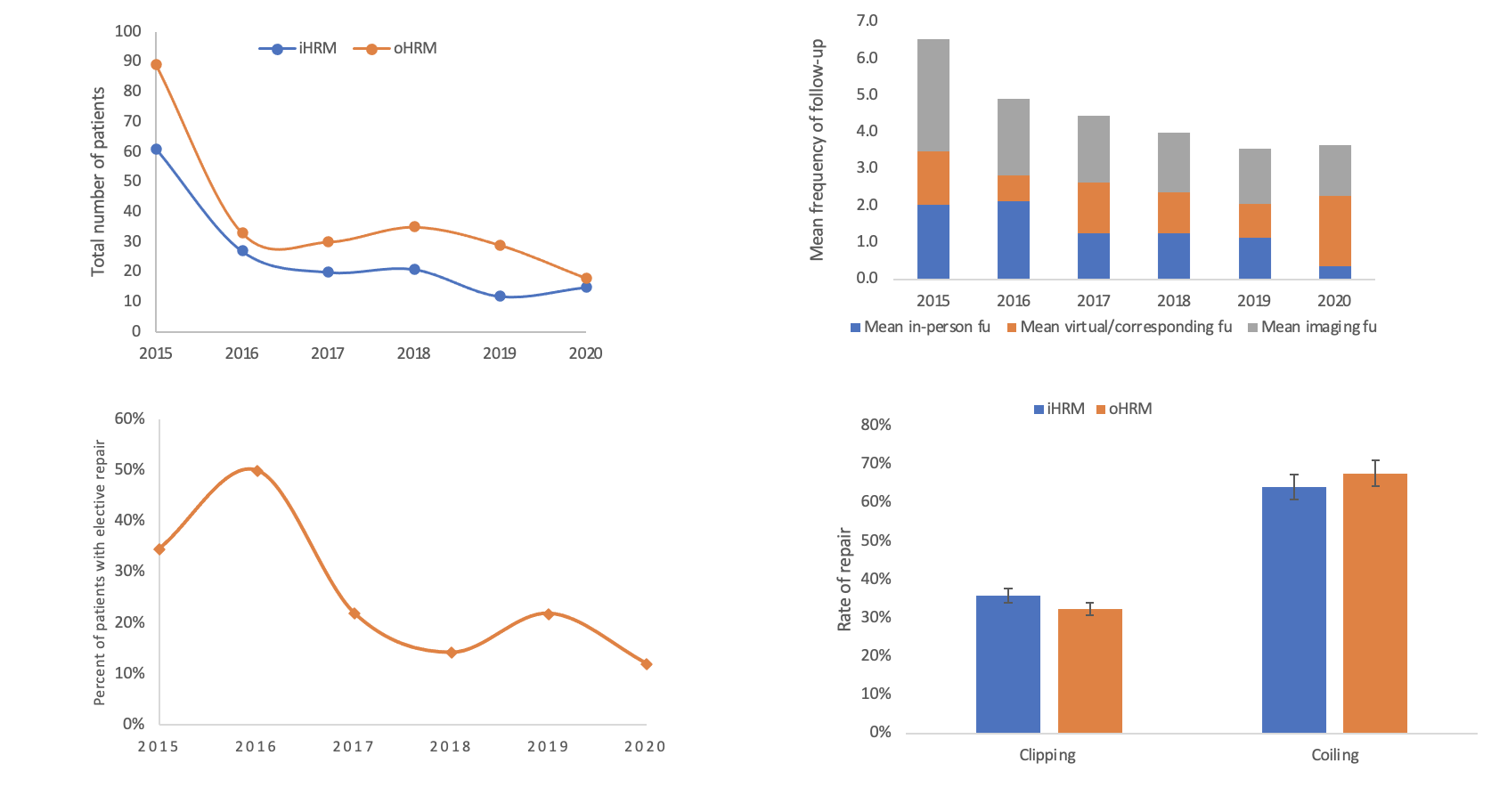
Figure 2. Result in graphs.
Conclusion
Limitations and future directions
- Retrospective study and its inherent limitations to confounders.
- UIAT scores limitations by default.
- Single center.
- A deeper look into socioeconomic status, racialized and marginalized population.
Acknowledgement
- Mentor : Dr. Gwynedd Pickett
- RIM director : Dr. Melissa Andrew
- Data management and statistics, Dalhousie University
Assessing the Fragility Index of Randomized Controlled Trials on Carotid Artery Stenosis: Systematic Review

Introduction
- Fragility Index (FI) measures the robustness of clinical trials with dichotomous outcomes
- A longstanding debate exists between carotid artery stenting (CAS) and endarterectomy (CEA) in the treatment of atherosclerotic carotid artery stenosis
- Although many RCTs have compared the outcomes of the two, little is known about the fragility of these results
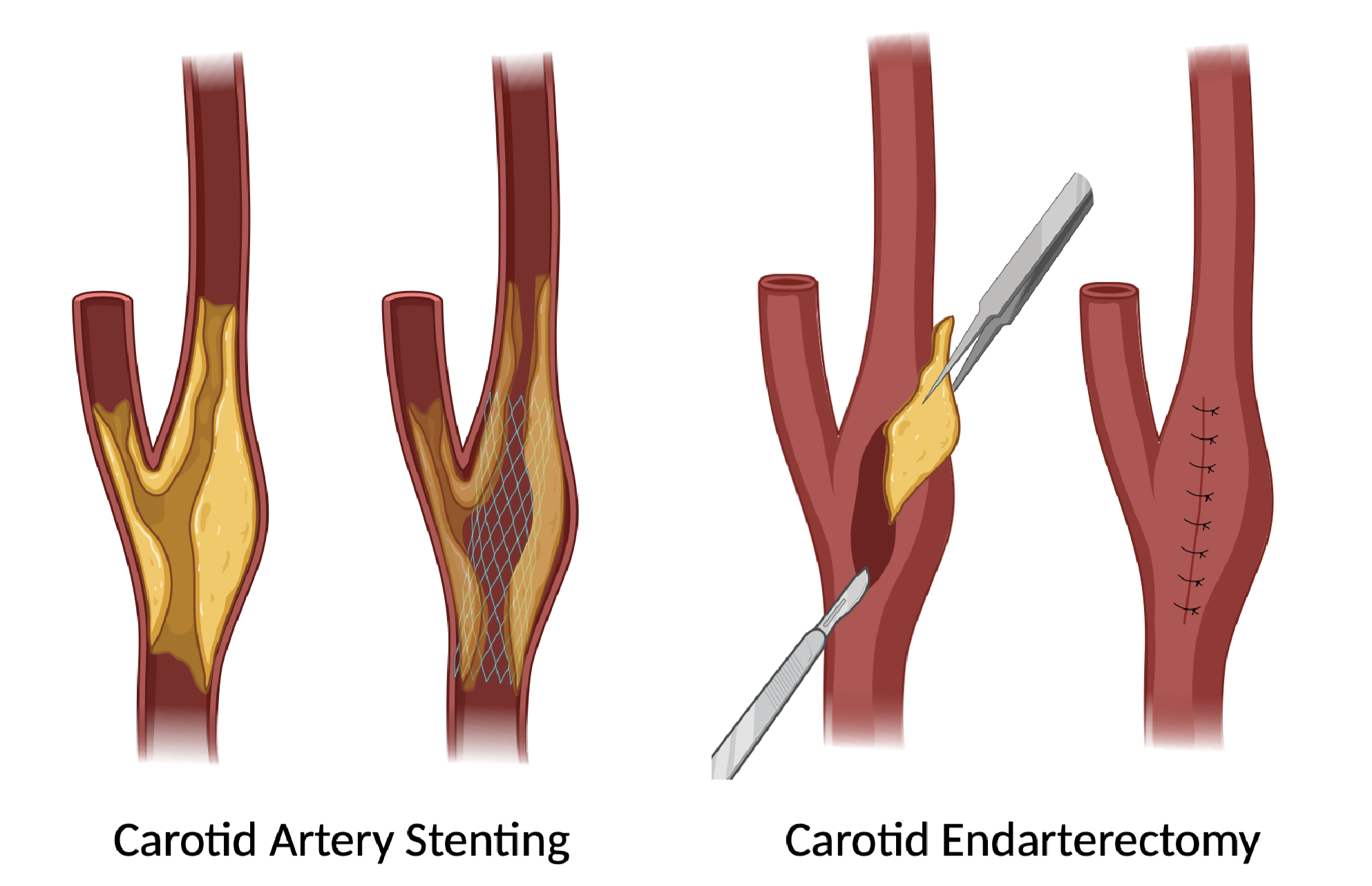
Purpose
The primary objective of this systematic review is to analyze the fragility index (FI) of RCTs comparing CAS and CEA with statistically significant and dichotomous outcomes.
Methods
A search was conducted in MEDLINE, Embase and PubMed. Preferred Reporting Items for Systematic Reviews and Meta- analyses (PRISMA) guidelines were followed.
Inclusion criteria:
1) Randomized control trials comparing carotid artery stenting and carotid endarterectomy with statistically significant and dichotomous primary outcomes
2) Studies in humans
3) Studies in English
Exclusion criteria:
1) Non-randomized control trials
2) Studies not comparing carotid artery stenting and carotid endarterectomy
Methods
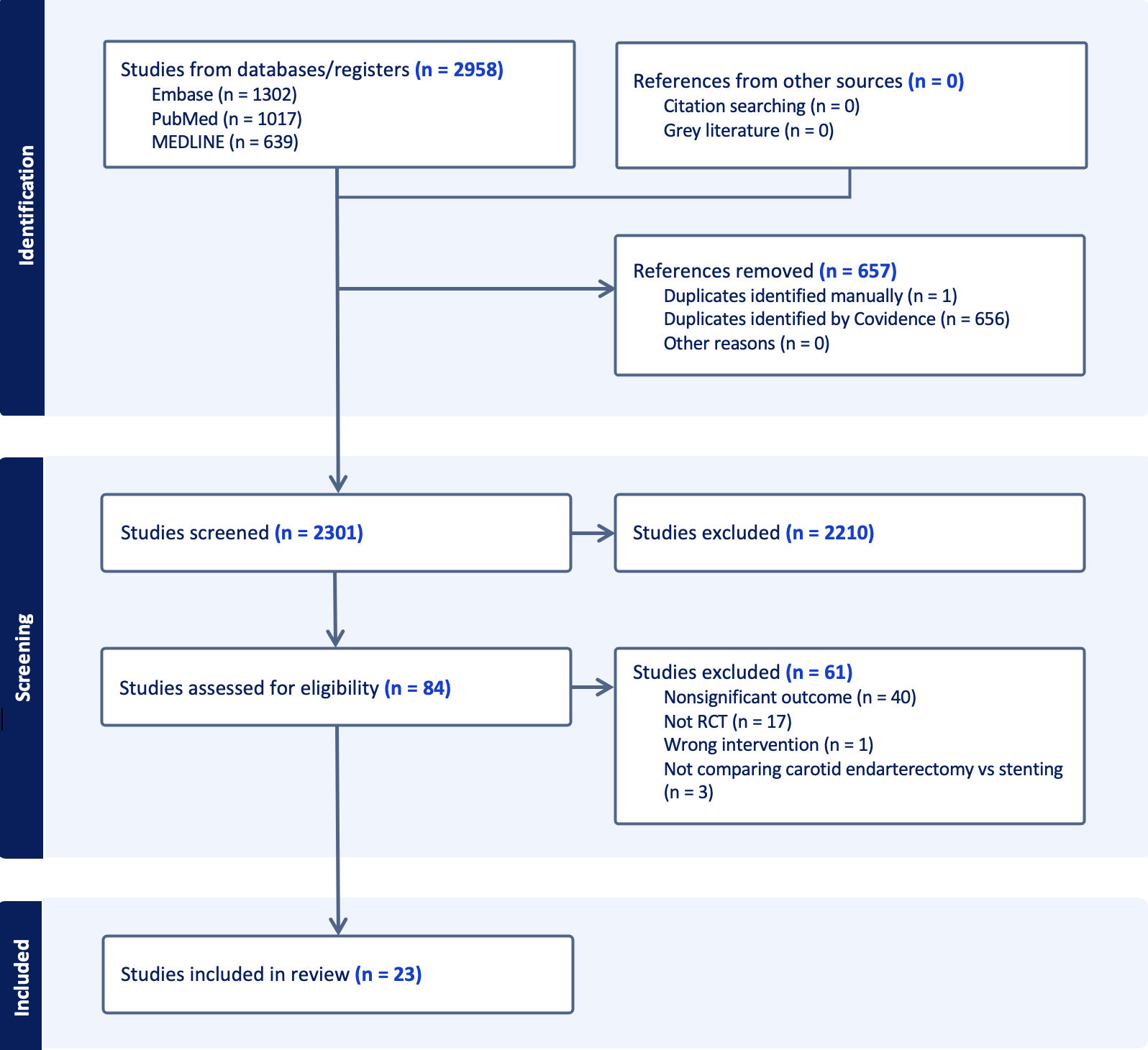
Study Characteristics
- Our literature search identified 10 RCTs: 2 index studies, 2 follow-up studies, and 6 sub-analyses
- Total of 9382 patients (4734 CEA, 4648 CAS)
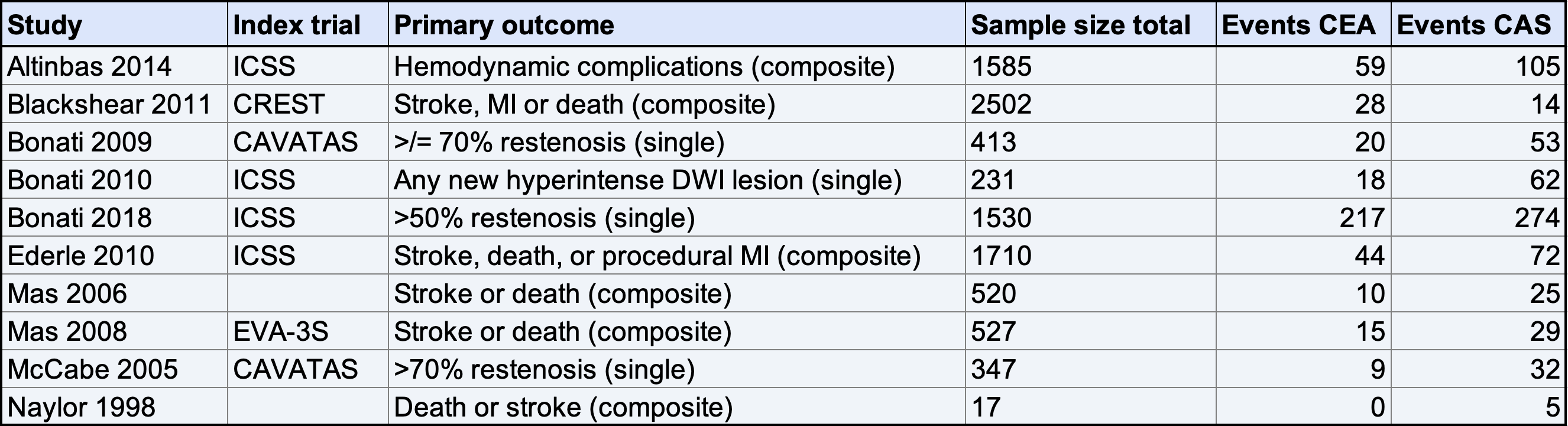
Results
- Median FI was 9.5 with an interquartile range of 2.25-21.25 (19)
- 100% of the studies had lost-to-follow-up (LTFU) greater than its fragility index (FI)

Conclusion
- A small number of events (median 9.5) is required to change outcomes of carotid artery stenosis RCTs comparing CEA and CAS from statistically significant to statistically insignificant.
- As LTFU was greater than FI for all of the included studies, this calls into question the robustness of the RCT results
Contact Information
Eva Liu, MD University of Saskatchewan eva.liu@usask.ca
Saskatchewan spine pathway classification is associated with post-operative outcome and improved quality-adjusted life years following lumbosacral fusion
Background
Low back pain (LBP) is a common cause of disability and decreased quality of life. The Saskatchewan Spine Pathway classification (SSPc) is a method for triaging patients who are candidates for surgery. We have previously shown that this system is efficacious for selecting surgical candidates. No prior work examines the utility of this pathway in predicting outcomes following spine surgery based on pre-operative pain patterns.
The SSPc stratifies patient into 4 groups based on their pain pattern: back dominant pain aggravated by flexion (pattern I); back dominant pain aggravated by extension but not increased with flexion (pattern II); leg dominant pain that is constant, associated with positive neurological findings, and aggravated by back movement (pattern III); leg dominant pain that is intermittent, aggravated by activity in extension, and relieved by rest in flexion (pattern IV)
The SSPc stratifies patient into 4 groups based on their pain pattern: back dominant pain aggravated by flexion (pattern I); back dominant pain aggravated by extension but not increased with flexion (pattern II); leg dominant pain that is constant, associated with positive neurological findings, and aggravated by back movement (pattern III); leg dominant pain that is intermittent, aggravated by activity in extension, and relieved by rest in flexion (pattern IV)
Methods
Consecutive patients who underwent lumbosacral instrumented fusion for degenerative spinal pathology from Jan 1, 2012, to Sept 20, 2018, by a single surgeon at our institution were retrospectively reviewed. Patients were stratified by SSPc into 4 groups based on pain pattern.
Inclusion criteria included age>18 years and degenerative spinal pathology being treated with elective lumbosacral fusion with assigned SSPc classification. We excluded groups with less than 5 patients, due to inability to analyze data otherwise. We also excluded patient files with missing baseline or follow-up data, worker’s compensation patients , and surgery performed for reasons other than degenerative spine diseases such as infection, trauma, malignancy, and emergent surgery for cauda equina syndrome.
Demographic and clinical data were collected. We measured VAS back, VAS leg, Oswestry Disability Index (ODI), EQ-5D Quality-Adjusted Life Years (QALY) and overall state of health (EQ-VAS) scores before surgery before surgery and at early and late follow-up.Outcomes were compared between cohorts both for absolute values and achieving MCID.
Inclusion criteria included age>18 years and degenerative spinal pathology being treated with elective lumbosacral fusion with assigned SSPc classification. We excluded groups with less than 5 patients, due to inability to analyze data otherwise. We also excluded patient files with missing baseline or follow-up data, worker’s compensation patients , and surgery performed for reasons other than degenerative spine diseases such as infection, trauma, malignancy, and emergent surgery for cauda equina syndrome.
Demographic and clinical data were collected. We measured VAS back, VAS leg, Oswestry Disability Index (ODI), EQ-5D Quality-Adjusted Life Years (QALY) and overall state of health (EQ-VAS) scores before surgery before surgery and at early and late follow-up.Outcomes were compared between cohorts both for absolute values and achieving MCID.
Results
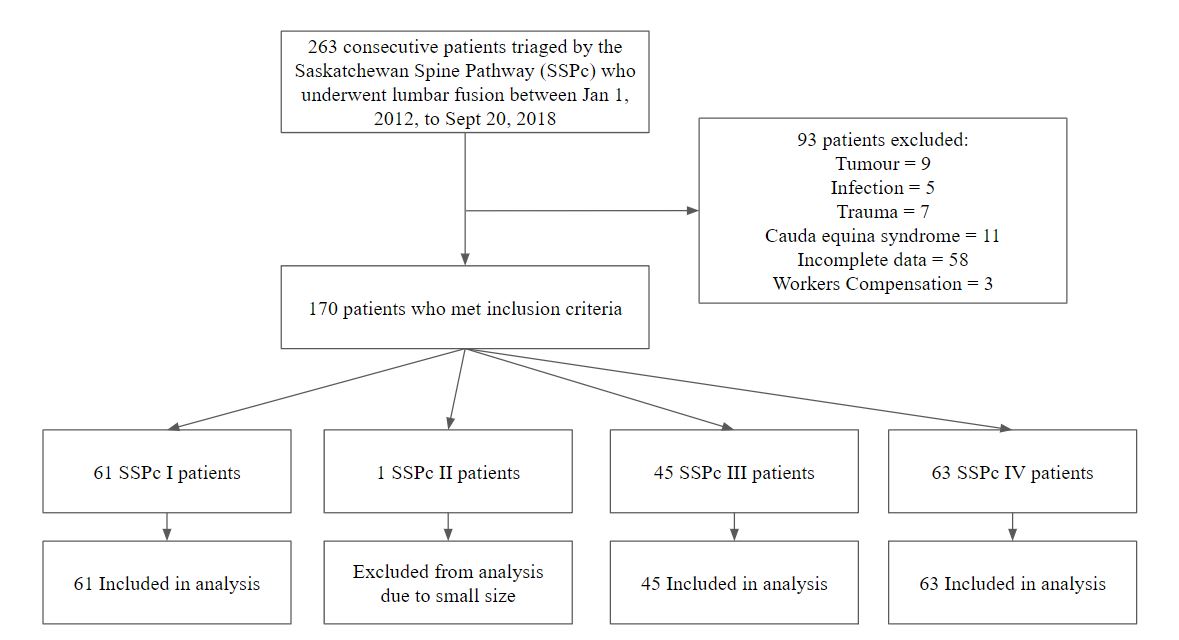
Figure 1. Summary of patients included
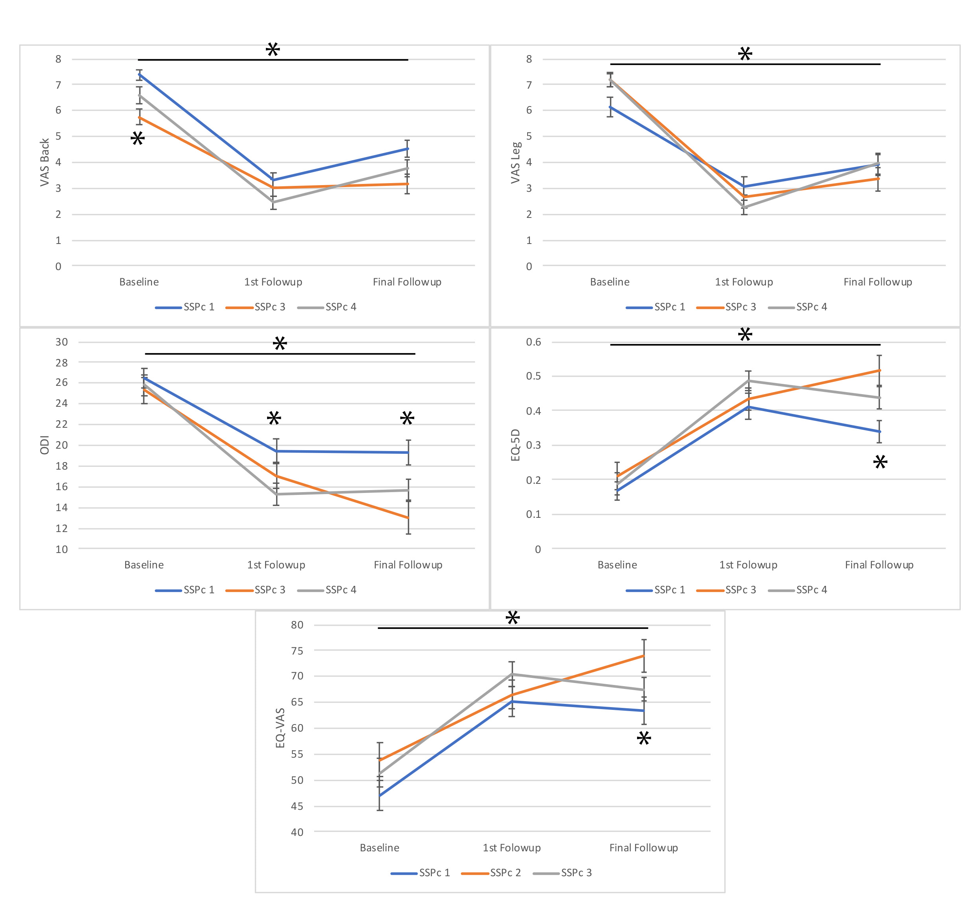
Patient-reported outcomes grouped by SSPC Class
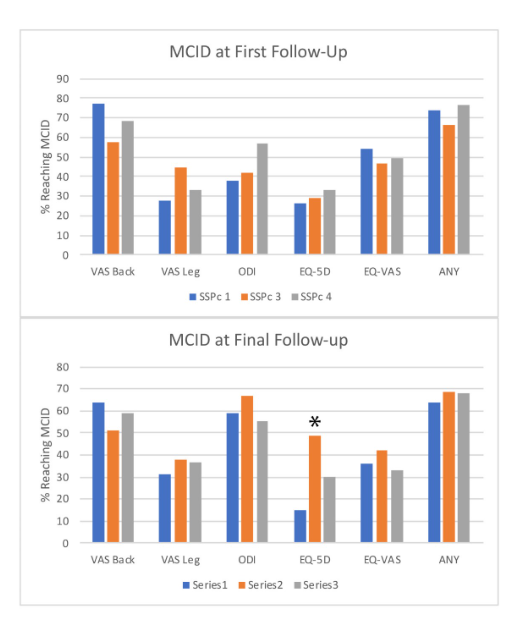
MCID outcome based on SSPC Class
Conclusion
The SSPc classification is associated with outcomes following lumbosacral fusion. In particular, patients with SSPc pattern 3 had better outcomes and improved QALY
References
- Frank JW, Kerr MS, Brooker AS, DeMaio SE, Maetzel A, Shannon HS, Sullivan TJ, Norman RW, Wells RP. Disability resulting from occupational low back pain. Part I: What do we know about primary prevention? A review of the scientific evidence on prevention before disability begins. Spine (Phila Pa 1976). 1996 Dec 15;21(24):2908-17.
- Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine (Phila Pa 1976). 2006 Nov 1;31(23):2724-7.
- Mirza SK, Deyo RA. Systematic review of randomized trials comparing lumbar fusion surgery to nonoperative care for treatment of chronic back pain. Spine (Phila Pa 1976). 2007 Apr 1;32(7):816-23.
- Brox JI, Reikerås O, Nygaard Ø, Sørensen R, Indahl A, Holm I, Keller A, Ingebrigtsen T, Grundnes O, Lange JE, Friis A. Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: a prospective randomized controlled study. Pain. 2006 May;122(1-2):145-55.
- Kindrachuk DR, Fourney DR. Spine surgery referrals redirected through a multidisciplinary care pathway: effects of nonsurgeon triage including MRI utilization. J Neurosurg Spine. 2014 Jan;20(1):87-92.
- Fourney DR, Dettori JR, Hall H, Härtl R, McGirt MJ, Daubs MD. A systematic review of clinical pathways for lower back pain and introduction of the Saskatchewan Spine Pathway. Spine (Phila Pa 1976). 2011 Oct 1;36(21 Suppl):S164-71
Antiplatelet and Anticoagulation Use and Outcomes Following Chronic Subdural Hematoma Drainage: Systematic Review and Meta-Analysis
BACKGROUND
-
Chronic subdural hematoma (CSDH) is a neurosurgical condition commonly treated with surgical evacuation
-
Significant proportion of patients presenting with CSDH recieve antiplatelet or anticoagulation at baseline1
-
Impact of pre-operative antiplatelet or anticoagulation on the outcome of CSDH evacuation, recurrence, and thromboembolic event remains unclear
OBJECTIVE
- To determine the risk of recurrence of CSDH post surgical evacuation and risk of thromboembolic events in patients receiving antiplatelet therapy, anticoagulation therapy, or no antithrombotics
METHOD
-
Comprehensive literature search was conducted in the MEDLINE, EMBASE, and PubMed databases on pre-operative use of antipatelet or anticoagulation therapy and outcome following CSDH evacuation
-
Screening protocol was adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines
RESULT
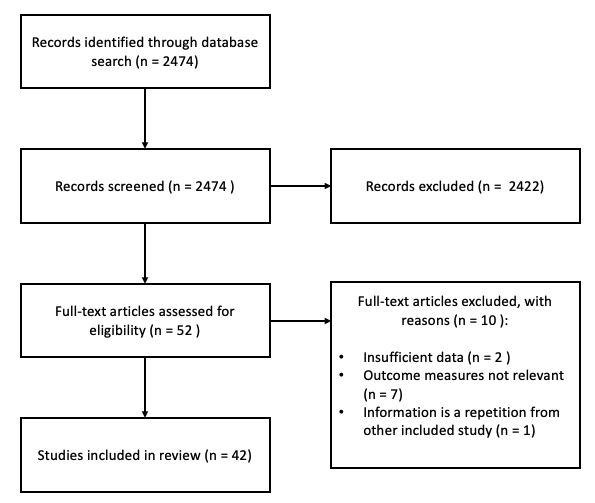
Figure 1. PRISMA flow diagram
Patient Demographic
-
14, 410 patients were included for analysis
- 3, 218 patients were on antiplatelet (22%)
- 1, 731 patients were on anticoagulation (12%)
- 9, 537 patients were not on any form of antithrombotic (66%)
- 3, 394 female patients (29.6%)
- Weighted mean age of 73.9 years
RESULT
Recurrence of CSDH
- Patients with pre-operative use of antiplatelet demonstrated significantly higher rate of recurrence compared to those not on antithrombotics (OR = 1.21, 95% CI = 1.04 to 1.30, P = 0.01)
- Patients with pre-operative use of anticoagulation demonstrated significantly higher rate of recurrence compared to those not on antithrombotics (OR = 1.39, 95% CI = 1.15 to 1.68, P = 0.0007)
Thromboembolic Events
- 3.92% of patients on pre-operative antithrombotic had reported thromboembolic event, compared to 0.63% in the patient group without antithrombotic therapy (OR 5.41, 95% CI = 3.16 to 9.26, P < 0.00001)
CONCLUSION
-
Patients on antithrombotic therapy have both higher risk of recurrence and higher thromboembolic risk compared to patients not on antithrombotic therapy
-
Clinicians need to weigh the risk of recurrence against thromboembolism when deciding when to hold and resume antithrombotic therapy
REFERENCES
- Kerttula, Santtu, et al. "The effect of antithrombotic therapy on the recurrence and outcome of chronic subdural hematoma after burr-hole craniostomy in a population-based cohort." Acta Neurochirurgica 164.10 (2022): 2699-2708.
Cerebral AVM recurrence post gamma knife obliteration: a 20 year single centre retrospective analysis and review of literature
INTRODUCTION
- Arteriovenous malformations (AVMs) are rare in pediatric populations, but despite this they are the leading cause of intracranial hemorrhage (ICH) in children, accounting for 14-57% of all ICH in patients younger than 18.
- AVMs can be treated with several modalities, including microsurgical disconnection, endovascular embolization, and stereotactic radiosurgery (SRS).
- SRS is often completed using Gamma Knife (GK), where a single dose of radiation is delivered to stimulate the involution of the target lesion.
- AVMs are traditionally considered to be congenital lesions, and de-novo development of AVMs is considered rare.
- However, AVM recurrence is a rare but known complication after obliteration of AVMs in pediatric populations.
- While a few studies have looked at AVM recurrance, most have focused on the phenomena after microsurgical obliteration, and there is little literature investigating recurrance after GK.
- As such, we reviewed all pediatric AVMs treated at our institution over the past twenty years, with particular focus on the risk of recurrence, and completed a review of literature to investigate reported prevelance in other datasets.
METHODS
Cohort Study
- Data from consecutively enrolled patients in a database of GK procedures completed at our institution from the initiation of our GK program in November 2003 until March 2024 were filtered to select patients 18 years of age and under who had at least one GK treatment of an AVM.
- Records meeting these inclusion criteria were obtained and coded by two independent reviewers. The following data were extracted from the records: patient demographics, presenting features, AVM characteristics, Spetzler-Martin grade, Pollock radiosurgery grade, treatment response, timing of response, AVM recurrence, and other complications. Data were stored on an encrypted hard drive.
- A comprehensive literature search of PubMed Central was completed using the keywords; arteriovenous malformation, AVM, recurrent, recurrence, reappearance, recur*, gamma knife, radiosurgery, radio surgery, GKRS, Pediatric, Child, Childhood, used in combination utilizing the boolean operators OR and AND.
- Papers with ten or more participants were included. Papers that did not specifically address pediatric populations (less than 18 years old) or did not include pediatric subgroup analysis were excluded. Papers that did not include analysis of cases treated with gamma knife were excluded.
- Two reviewers selected the included studies. Inconsistencies were resolved by consensus.
- In our cohort study, we analyzed the differences between children with radiographically proven AVM obliteration and AVM recurrance. Appropriate univariate analysis tests were selected for each variable. Data were analyzed using SPSS (IBM SPSS Statistics for Windows, Version 29.0.2.0 Armonk, NY: IBM Corp)
Results
Cohort Analysis
Cohort Analysis
- 26 pediatric patients with AVMs treated with GK were identified in our dataset. Of these, 7 were undergoing ongoing followup, 4 were lost to followup, 11 had radiographically confirmed AVM obliteration with no recurrence, and 3 had AVM obliteration with recurrence.
- The recurrence rate of after AVM obliteration was 20%. When comparing patients with obliterated AVMs to those who had recurrence, both groups received a mean radiation dose of 20 gy, the mean age of patients with obliterated AVMs was 11.25 (SD 3.57) while the mean age of patients with recurrent AVMs was 9.00 (SD 6.25). Recurrent AVMs were more likely to be a spetzler-martin grade 4 (66%) vs obliterated (16%), and recurrent AVMs were more likely to be located in the posterior fossa (66%) vs obliterated (8%). However, due to the small size of our sample, our analysis was underpowered and differences were not significant.
- Among the 97 studies screened for review, 5 papers with a total of 108 children were included in the review. See flowchart for details. All papers were retrospective studies. Overall recurrance rate in the collected papers was 5.6%, with a range from 0-13.6%.
- Raw data were not available, and thus more detailed subgroup analyses were not completed.
Literature Review Flow Diagram
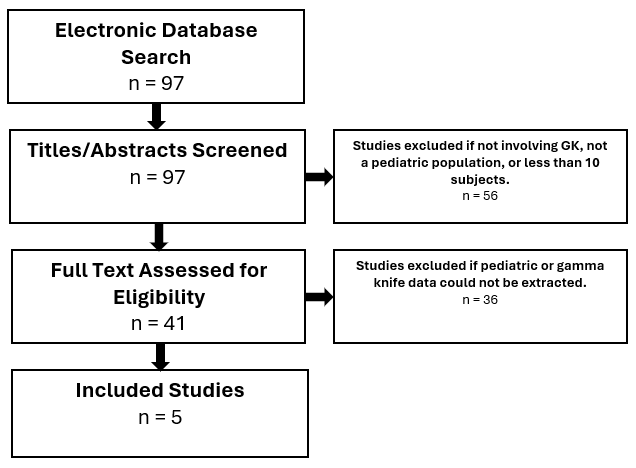

DISCUSSION
- Recurrence of AVMs after treatment is a rare but known phenomena with an incompletely understood mechanism, occurring more often in pediatric populations. Our dataset had a 20% AVM recurrence rate after GK obliteration, though this may have been artificially inflated as patients who returned to their home province would be "lost" to followup if stable, but may have been more likely to be re-referred for consideration of repeat GK. Our literature search indicates this recurrence percentage is slightly higher than most observations (reported range of 0-13.6%). If all cases of AVM treated with GK are considered, the recurrence rate is 11.5%.
- Recurrence of AVMs in adult populations is reported far less frequently, and it has been suggested that this is a result of the immature vascular environment in the pediatric brain. Dysregulated angiogenesis has been implicated in the recurrence of AVMs, with increased expression of VEGF and endothelial progenitor cell markers (CD31, CD34, and CD105) were noted in AVM tissue samples taken from individuals with surgical treatment of AVM recurrence. Alternatively, some AVM recurrences may not be recurrences at all, but rather undetected AVM remnants that were not noted postoperatively due to altered hemodynamics.
- Limitations of this study include the small sample size, which led to a lack of statically significant results in our cohort analysis. Further, a reasonably significant portion of our sample was lost to followup (15%) as they returned to their home province or were otherwise lost. Additionally, the portion of our sample who were undergoing ongoing followup (27%) could conceivably have future AVM recurrence, and similarly the population with obliterated AMVs could conceivably eventually develop recurrence in an extremely delayed fashion.
Illustrative Case
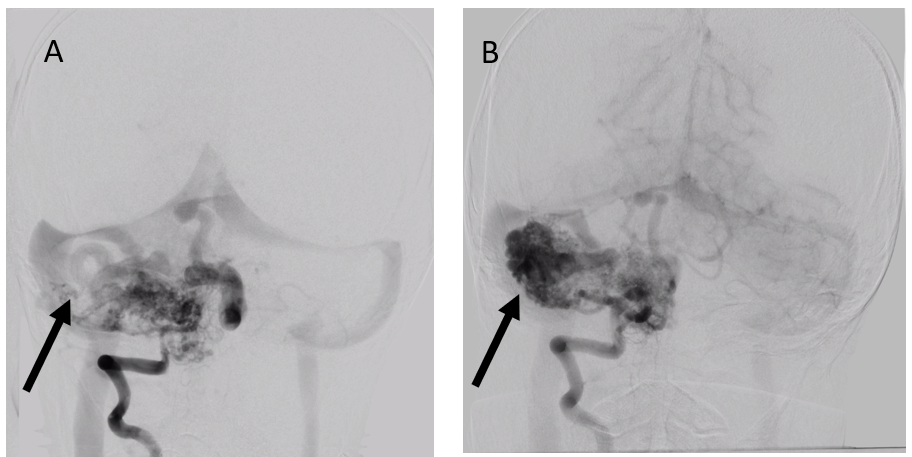
Coronal DSA with R vertebral injections. A) DSA completed before initial GKRS treatment. B) Approximately 3 years later, DSA shows development of AVM in an adjacent area of previously unaffected tissue.
CONCLUSION
- These investigations highlight the importance of long-term follow-up and surveillance imaging in pediatric patients after GK for AVM. Clinicians should be aware of the potential for recurrence, and include this when making a decision about treatment modality. Clinicians should structure their patient counselling and follow-up examinations with this in mind.
Quality of Life (QoL) Using EORTC QLQ-C30 and BN20 among Patients who Underwent Brain Tumor Resection in a Tertiary Hospital in Saudi Arabiaa
Introduction
Quality of life (QoL) is the awareness of individuals’ well-being in life in physical, personal, mental and social wellbeing. Brain tumors are classified into primary and secondary tumors. Survival rates depend on the histopathology grade of tumor. QoL needs to be addressed in brain tumor patients. Up to our knowledge, there is scarcity of research in our region- the Middle East- studying the QoL in brain tumor patients.
Methods
A retrospective study conducted in 2017 in a single academic center King Abdulaziz University Hospital, Jeddah, Saudi Arabia that included patients diagnosed with brain tumors in a 10 year period (2007-2017). The exclusion criteria were patients who were not diagnosed by histopathology, not undergone surgical procedure nor were reachable to assess quality of life. Data included patients’ demographic data, diagnosis, histopathology, date of surgery, treatment modality, postoperative complications or recurrence. The assessment of the QoL was done in translated Arabic questionnaire by using the European Organization for Research and Treatment of Cancer (EORTC), a standardized model (QLQ-C30) that assess several domains (Global Health, Physical function, Role functioning, Emotional Functioning, Cognitive functioning, social functioning and symptoms domain) and Brain cancer model (BN20) to assess symptoms to evaluate all aspects of wellbeing. The study was approved by the institutional review board at King Abdulaziz University Hospital following Helsinki declaration.
Results
The total number of patients included in this study is 76 patients. There was no gender predilection. The most common brain tumor in our study was meningioma by 40% followed by glioma/ others. More than half of the brain tumor patients had a WHO grade I (65%), intermediate grading grade II (15%) and higher grading grade III/IV (20%). The commonest
Quality of life (QoL) is the awareness of individuals’ well-being in life in physical, personal, mental and social wellbeing. Brain tumors are classified into primary and secondary tumors. Survival rates depend on the histopathology grade of tumor. QoL needs to be addressed in brain tumor patients. Up to our knowledge, there is scarcity of research in our region- the Middle East- studying the QoL in brain tumor patients.
Methods
A retrospective study conducted in 2017 in a single academic center King Abdulaziz University Hospital, Jeddah, Saudi Arabia that included patients diagnosed with brain tumors in a 10 year period (2007-2017). The exclusion criteria were patients who were not diagnosed by histopathology, not undergone surgical procedure nor were reachable to assess quality of life. Data included patients’ demographic data, diagnosis, histopathology, date of surgery, treatment modality, postoperative complications or recurrence. The assessment of the QoL was done in translated Arabic questionnaire by using the European Organization for Research and Treatment of Cancer (EORTC), a standardized model (QLQ-C30) that assess several domains (Global Health, Physical function, Role functioning, Emotional Functioning, Cognitive functioning, social functioning and symptoms domain) and Brain cancer model (BN20) to assess symptoms to evaluate all aspects of wellbeing. The study was approved by the institutional review board at King Abdulaziz University Hospital following Helsinki declaration.
Results
The total number of patients included in this study is 76 patients. There was no gender predilection. The most common brain tumor in our study was meningioma by 40% followed by glioma/ others. More than half of the brain tumor patients had a WHO grade I (65%), intermediate grading grade II (15%) and higher grading grade III/IV (20%). The commonest
|
Quality of Life Score (QOL-30 and QLQ-BN20) Categorized by WHO Grade |
P-value |
||||
|
Grade I mean score (+/- SD) N=50 |
Grade II mean Score (+/- SD) N=11 |
Grade III mean Score (+/- SD) N=6 |
Grade IV mean Score (+/- SD) N=9 |
||
|
QOL-C30 Physical Functioning Role function Emotional function Cognitive function Social function Global health quality of life Symptom ScaleFatigue Nausea and vomiting Pain Dyspnea Insomnia Appetite loss Constipation Diarrhea Financial difficulties |
81.7 (30.35) 79 (28.33) 74.3 (29.01) 82.7 (32.11) 76.7 (25) 20.4 (25.53) 43.7 (22.81) 17 (26.19) 9.3 (21.34) 29.3 (40.2) 14 (28.64) 21.3 (37.95) 6 (16.06) 20 (36.27) |
65.2 (40.45) 70.5 (29.9) 68.2 (34.52) 91 (17.26) 74.2 (24.28) 24.2 (24.75) 40.9 (15.57) 22.7 (23.89) 15.2 (27.34) 27.3 (46.71) 3 (10.05) 18.2 (31.14) 3 (10.05) 18.2 (34.52) |
69.4 (26.7) 86.1 (8.61) 72.2 (31.03) 88.9 (13.61) 76.4 (20.69) 31.5 (36.8) 38.9 (13.61) 22.2 (22.77) 0 (0) 22.2 (27.22) 22.2 (40.37) 22.2 (27.22) 5.6 (13.61) 33.3 (36.52) |
59.3 (42.58) 69.4 (33.07) 68.5 (34.81) 87 (26.06) 70.4 (26.06) 43.2 (27.5) 50 (33.33) 22.2 (28.87) 11.1 (23.57) 33.3 (40.83) 18.5 (24.22) 25.9 (36.43) 0 (0) 25.9 (40.06) |
0.20 0.76 0.94 0.9 0.83 0.13 0.91 0.59 0.57 0.97 0.35 0.82 0.65 0.78 |
|
QLQ-BN20 Future uncertainty Visual disorder Motor dysfunction Communication deficit Headaches Seizures Drowsiness Itchy skin Hair loss Weakness of legs Bladder control |
18.2 (23.9) 20.2 (28.28) 14.7 (23.7) 9.6 (21.76) 37.3 (36.04) 11.3 (24.84) 17.3 (28.76) 3.3 (16.84) 0 (0) 12.7 (28.48) 12 (31.41) |
23.5 (18.94) 17.2 (21.87) 14.1 (27.26) 26.3 (40.45) 33.3 (39.44) 21.2 (34.23) 18.2 (34.52) 3 (10.05) 12.1 (27) 15.2 (27.34) 9.1 (21.56) |
12.5 (11.49) 13 (17.8) 24.1 (19.14) 24.1 (31.75) 16.7 (27.89) 16.7 (40.82) 33.3 (36.52) 16.7 (27.89) 33.3 (42.16) 0 (0) 11.1 (27.22) |
20.4 (14.5) 17.3 (23.64) 42 (32.77) 1.2 (3.7) 29.6 (38.89) 14.8 (24.22) 33.3 (33.33) 25.9 (36.43) 11.1 (23.57) 44.4 (47.14) 11.1 (33.33) |
0.5 0.99 0.01 0.13 0.52 0.70 0.25 0.003 0.0002 0.04 0.99 |
Conclusion
Quality of life in brain tumor patients seemed poor regardless of the type. Further prospective studies with large samples are needed to assess quality of life in brain tumor patients worldwide.
Endoscopic fenestration of trapped fourth ventricle

Background
-
Trapped fourth ventricle (TFV) is a rare entity that occurs when the fourth ventricle is obstructed and isolated from the normal cerebrospinal fluid (CSF) circulation.
-
While not always symptomatic, TFV can lead to compression of the cerebellum and brainstem, with potential for serious consequences.
-
Treatment of TFV can be challenging, with options including CSF diversion via shunts versus open or endoscopic fenestrations.
-
In this report, we describe a case of TFV that was managed endoscopically.
Pre-operative
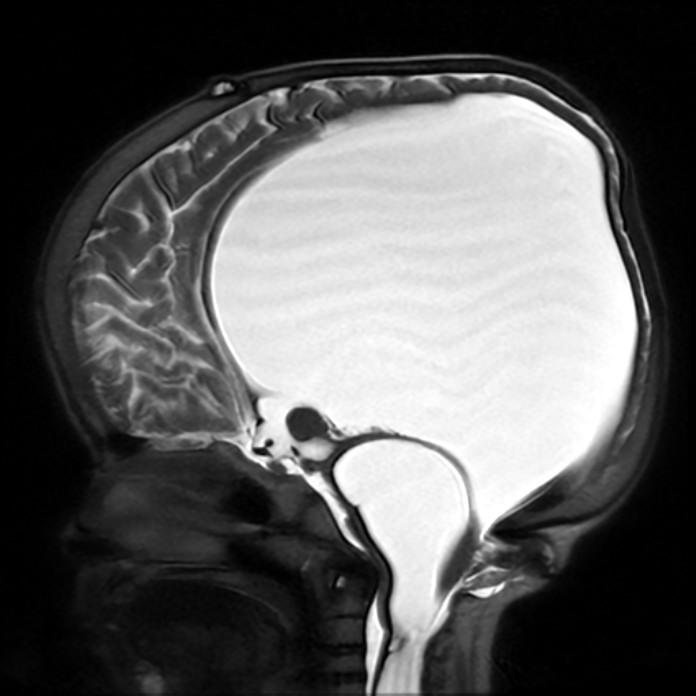
Pre-operative brain MRI, sagittal view.
Case Report
- A young girl with a history of myelomeningocele and hydrocephalus arrives in Canada following an international adoption.
- The patient’s neural tube defect had been closed at birth and a ventriculoperitoneal (VP) shunt was placed in early infancy.
- At age seven, the patient now presents with a change in neurological status, manifested by extremity weakness and intermittent drowsiness.
- Imaging of the brain and spine reveals markedly dilated ventricles, a trapped fourth ventricle, and syringomyelia.
- An endoscopic approach was used to fenestrate the wall of the fourth ventricle. The patient’s VP shunt was also completely revised at this time.
-
While there was an early favorable outcome, the first fenestration closed over within one month, requiring a repeat endoscopic fenestration.
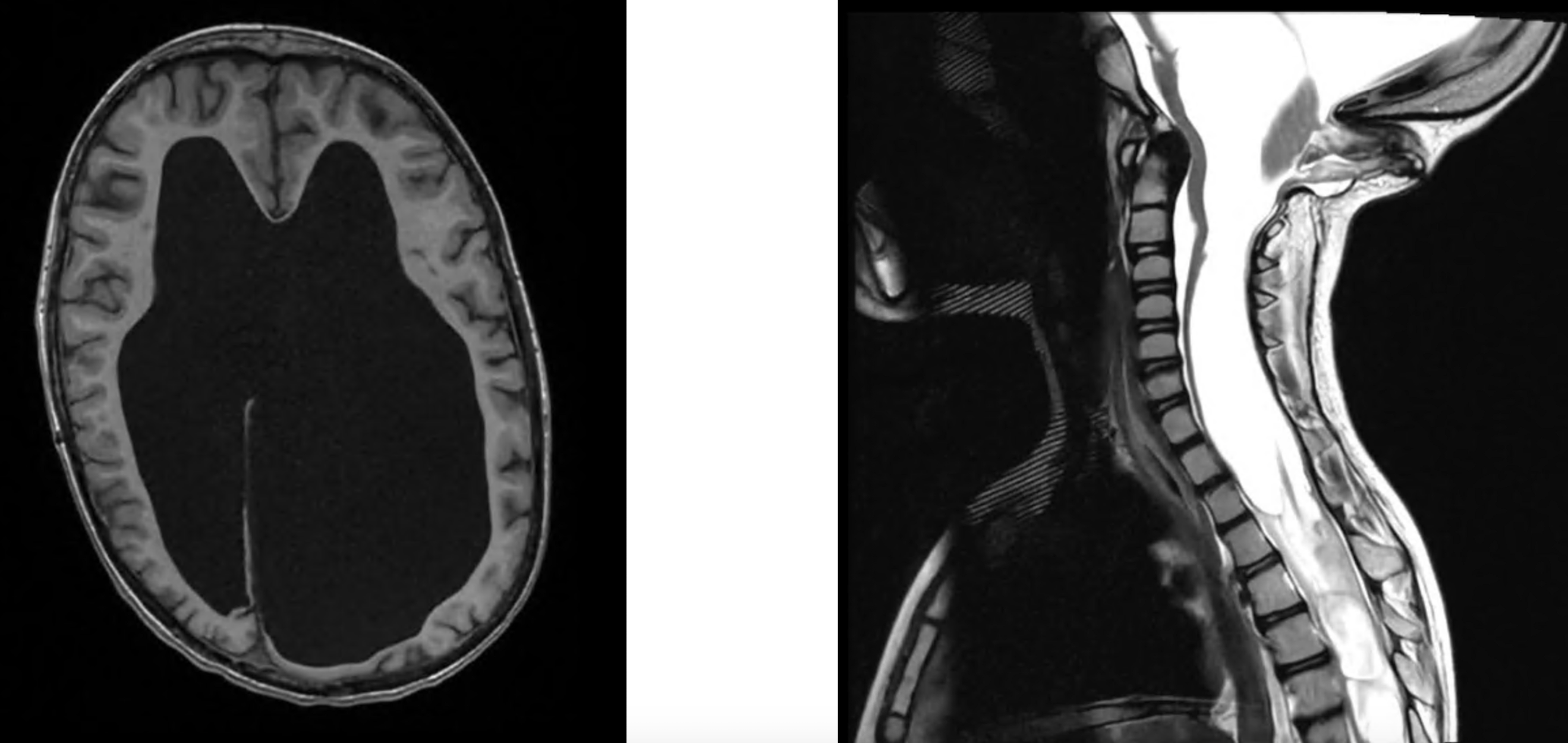
Pre-operative brain MRI, Pre-operative spine MRI,
axial view. sagittal view.
axial view. sagittal view.
Discussion
Post-operative
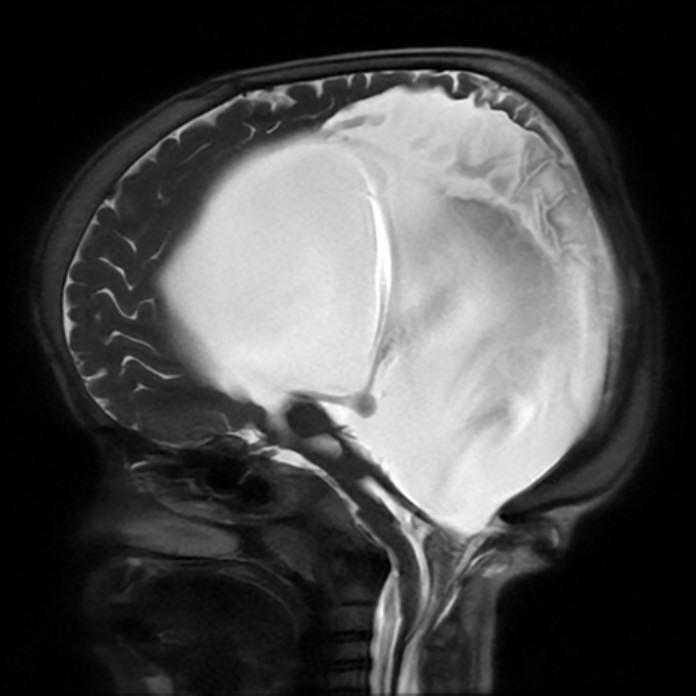
Post-operative brain MRI, sagittal view, one
month after the repeat endoscopic fenestration.
- Both procedures were complicated by transient seizures. An admission to the pediatric intensive care unit (PICU) was required after the second intervention.
- Large lateral ventricles and decreased cerebral hemisphere volumes were redemonstrated on post-operative imaging following the repeat endoscopic fenestration. The fourth ventricle demonstrated a significant decrease in size.
- The patient recovered well following the second procedure and returned to school 10 days post-op. Bowel function improved in early follow-up and mobility remained stable.
Conclusions
- Endoscopic fenestration can be an effective treatment option for management of TFV.
- The patient, family, and treating team should be prepared to deal with acute peri-operative complications that may require PICU management.
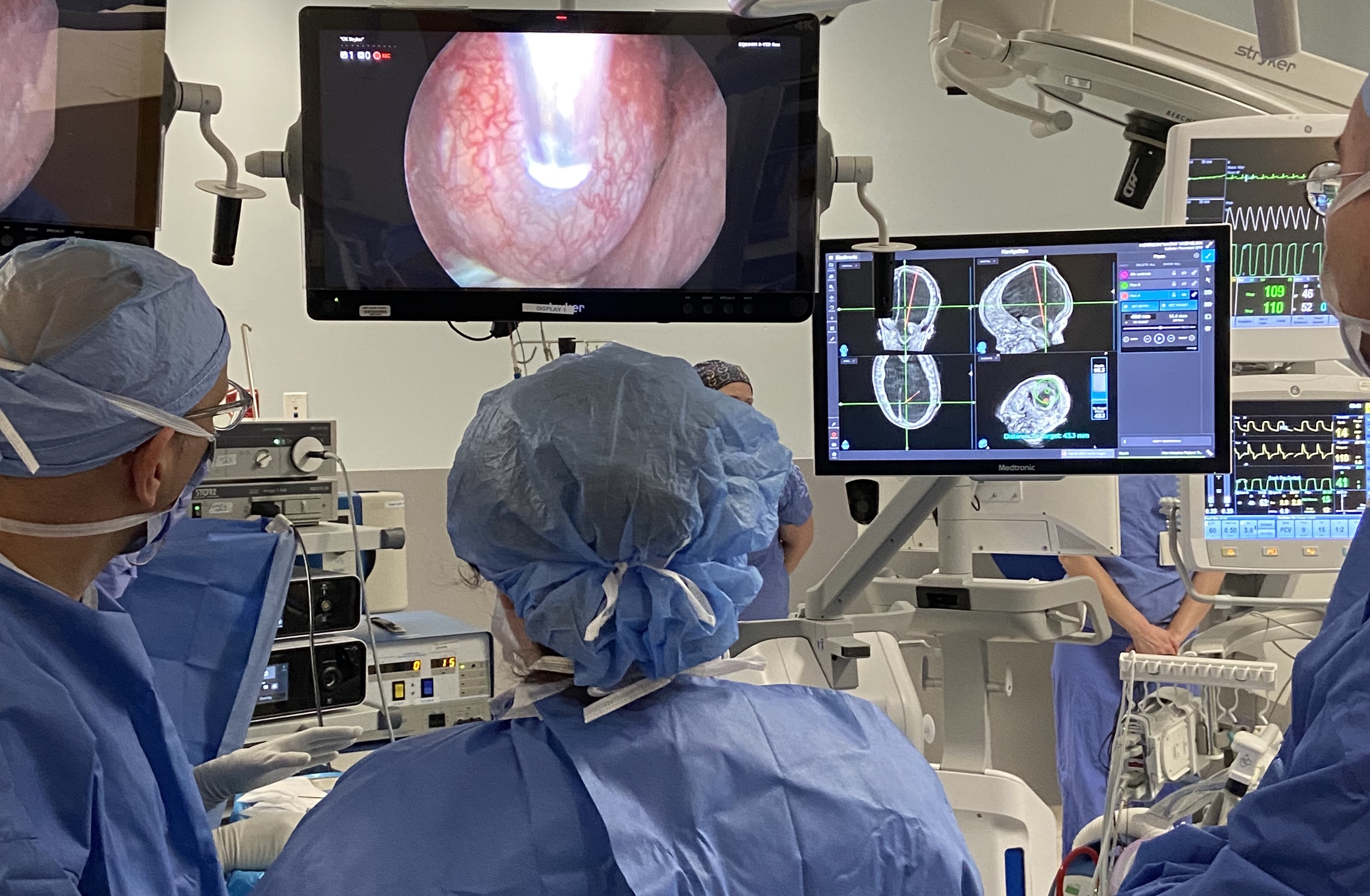
Intraoperative photo during endoscopic fenestration.
References
- Armbruster, L., Kunz, M., Ertl-Wagner, B., Tonn, J.-C., & Peraud, A. (2012). Microsurgical outlet restoration in isolated fourth ventricular hydrocephalus: a single-institutional experience. Child’s Nervous System, 28(12), 2101–2107. https://doi.org/10.1007/s00381-012-1887-5
- Gallo, P., Rodrigues, D., & Afshari, F. T. (2023). Endoscopic fenestration of the superior medullary velum for the treatment of a trapped fourth ventricle—technical note. Child’s Nervous System, 39(4), 1041–1044. https://doi.org/10.1007/s00381-023-05881-9
- Tubbs, R. S., Wellons III, J. C., Salter, G., & Oakes, W. J. (2004). Fenestration of the superior medullary velum as treatment for a trapped fourth ventricle: A feasibility study. Clinical Anatomy (New York, N.Y.), 17(2), 82–87. https://doi.org/10.1002/ca.10185
- Udayakumaran, S., Biyani, N., Rosenbaum, D. P., Ben-Sira, L., Constantini, S., & Beni-Adani, L. (2011). Posterior fossa craniotomy for trapped fourth ventricle in shunt-treated hydrocephalic children: long-term outcome: Clinical article. Journal of Neurosurgery. Pediatrics, 7(1), 52–63. https://doi.org/10.3171/2010.10.PEDS10139
- Villavicencio, A. T., Wellons III, J. C., & George, T. M. (1998). Avoiding Complicated Shunt Systems by Open Fenestration of Symptomatic Fourth Ventricular Cysts Associated with Hydrocephalus. Pediatric Neurosurgery, 29(6), 314–319. https://doi.org/10.1159/000028745
Comparison of interhemispheric and transcortical approaches for resection of colloid cysts of the third ventricle

Introduction
Colloid cysts are rare benign lesions of the third ventricle of the brain near the foramen of Monroe that can cause dangerous hydrocephalus and intracranial hypertension. They are typically detected incidentally or through symptoms such as headaches and cognitive decline. Their consequence can be fatal and lead to death. Their primary treatment is surgical removal when cyst become symptomatic or when there is presence of hydrocephalus. The surgical approaches include microsurgery and endoscopy. Although open surgery presents the best opportunity for total resection of the cyst, there is no consensus regarding the optimal choice between the interhemispheric approach and the transcortical approach. The objective is to compare these two surgical approaches to establish the difference in regard of the radicality of excision, the recurrence rate, and the surgical imprint.
Methodology
List of patients files provided by the Neurosurgery department of HEJ of the CHU of Quebec between January 1, 2003 and January 1 2023.
Population: Patient who underwent surgery for colloid cyst resection of the third ventricle.
Cases studied: 26
Collected data: Demographic data, pre-operative data, surgical indication, peri-operative data, post-operative data, pre-operative MRI data and post-operative MRI data.
Population: Patient who underwent surgery for colloid cyst resection of the third ventricle.
Cases studied: 26
Collected data: Demographic data, pre-operative data, surgical indication, peri-operative data, post-operative data, pre-operative MRI data and post-operative MRI data.

Figure 1. Methodology used to compare both surgical approches
Results
Comparison of pre-operative data between the two approaches
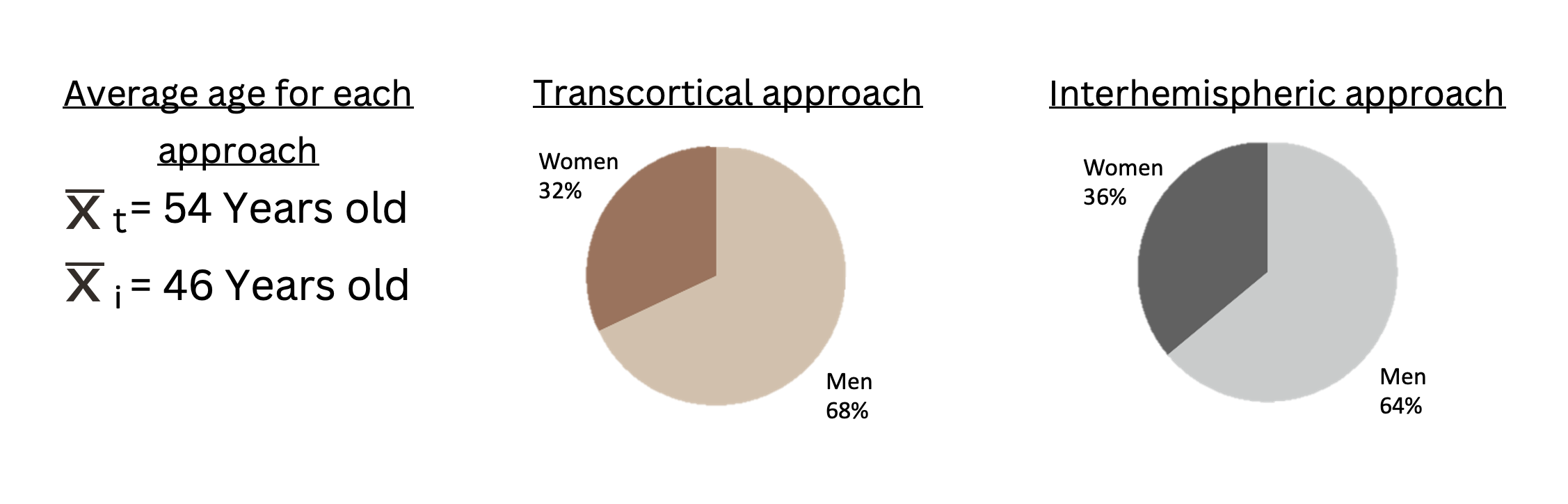
Figure 2. Age and sex distributions between the two groups

Figure 3. Symptoms of both groups of patients prior to cyst resection
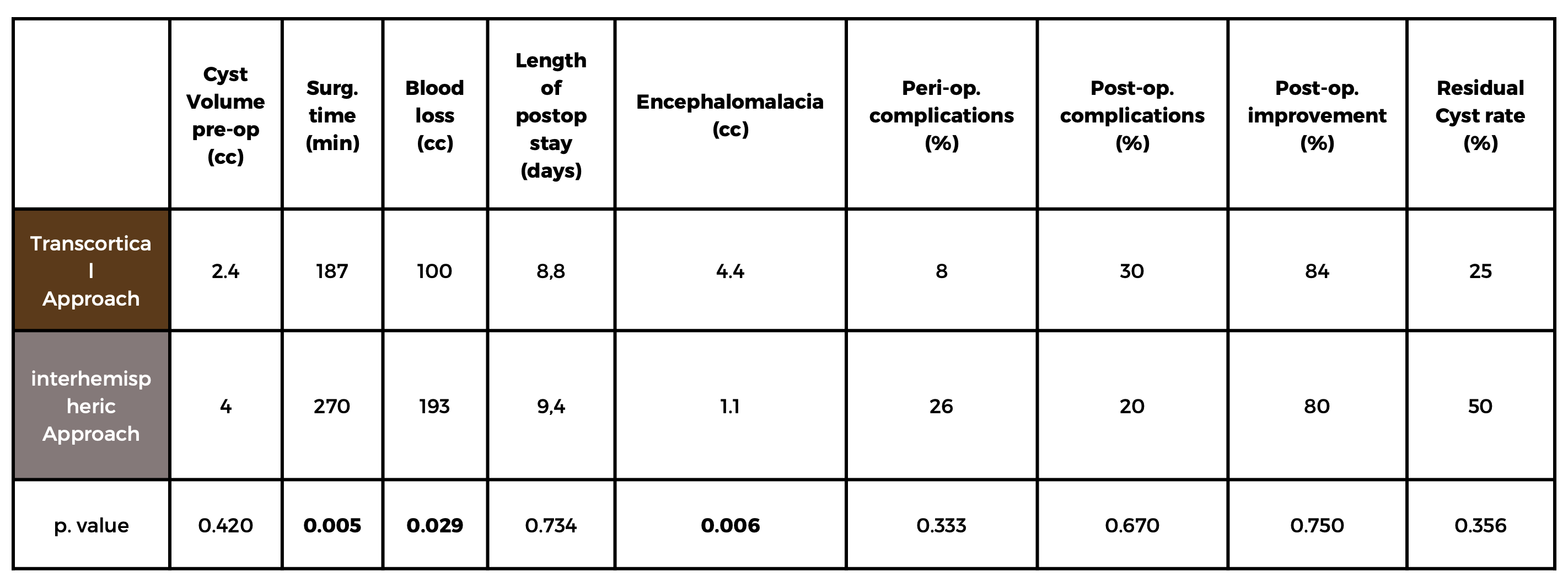
Table 1. Results obtained for each surgical approach
Discussion
- The interhemispheric approach for resection is associated with significantly increased operative time and blood loss, highlighting its complexity.
- We observed a significant reduction in the volume of encephalomalacia associated with the interhemespheric approach, indicating its potential for preserving brain tissue integrity.
- Clinical improvements were observed for both approaches but the difference was not statistically significant, likely due to the small cohort size and the rarity of the lesion.
Conclusion
- The interhemispheric approach for resection may offer advantages, including potentially fewer consequences related to reduced encephalomalacia.
- Further research with larger populations is necessary to confirm these benefits given the rarity of this tumor.
- The use of more sensitive neurocognitive tools should be considered to evaluate the approach's impact on clinical outcomes more comprehensively and potentially have more significant results.
- Perspective: A comparative study within a group of patients who underwent surgery by the same clinician could provide valuable insights into how the experience of the clinician impacts the choice of the approach.
References
- HELLER, Robert S, HEILMAN, Carl. Colloid Cysts: Evolution of Surgical Approach Preference and Management of Recurrent Cysts, Operative neurosurgery, 2020
- BEAUMONT, Thomas L. and al. Natural history of colloid cysts of the third ventricle, JNS, 2016
- GERALD, Musa and al. Clinical and radiological characteristics in fatal third ventricle colloid cyst. Literature review, Journal of clinical neuroscience, 2020
- Zeineddine, Hussein A. and al. Risk analysis and management of third ventricular colloid cysts, World Neurosurgery, 2010
Blood loss quantification and management strategies in cranial neurosurgery: a systematic review
Background
●Blood loss in cranial neurosurgery is an important perioperative metric
●No standardized blood loss measurement or reduction protocols currently exist
○Surgeon/visual estimation or anesthesia records are common methods, but significantly inaccurate.1
●Main Question:
○Which perioperative blood loss management techniques and intraoperative quantification techniques are most commonly utilized in cranial neurosurgery?
●Main Objectives
○Synthesize the current literature on blood loss quantification methodologies and perioperative management in cranial neurosurgery.
Figure 1: Nested Knowledge PRIMSA Flowchart
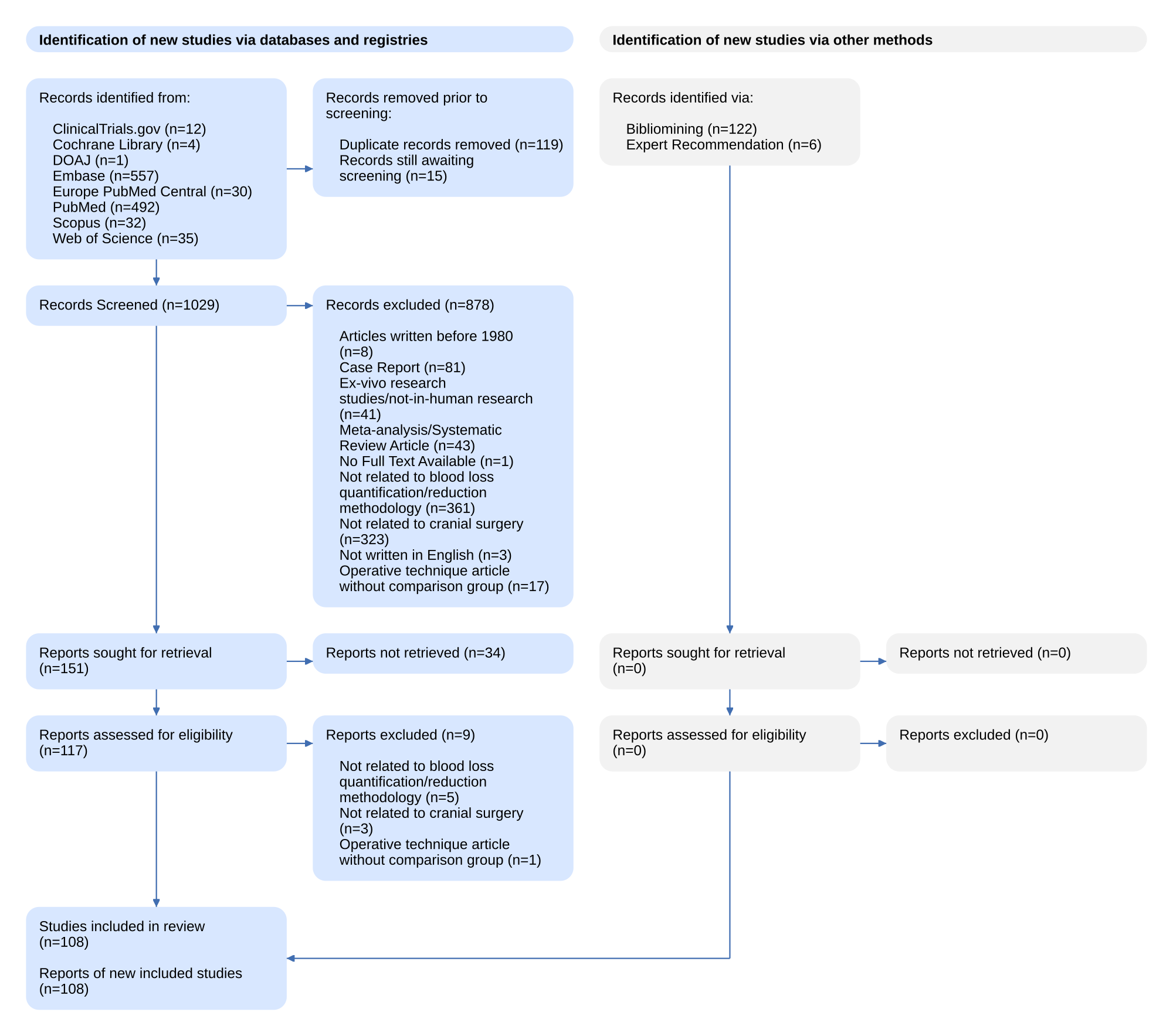
Figure 1. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flowchart.
NK Tagging Hierarchy QR

Methods
●Performed a systematic review of the current literature on blood loss quantification and management in cranial neurosurgery
●Utilized a novel semi-automated software platform (AutoLit, Nested Knowledge) to isolate 1029 abstracts from search of multiple databases
●Performed dual screening of abstracts (full-text blinded)
○Screened according to pre-established inclusion and exclusion criteria
●Tagged 108 full-text manuscripts
Results
Table 1: Frequency of Conditions Investigated
| Condition | Frequency (n=108) |
| Craniosynostosis | 45 |
| Tumor | 39 |
| Trauma | 15 |
| Cerebrovascular | 7 |
| Functional/Epilepsy | 2 |
Figure 2: Blood Loss Quantification Methodology
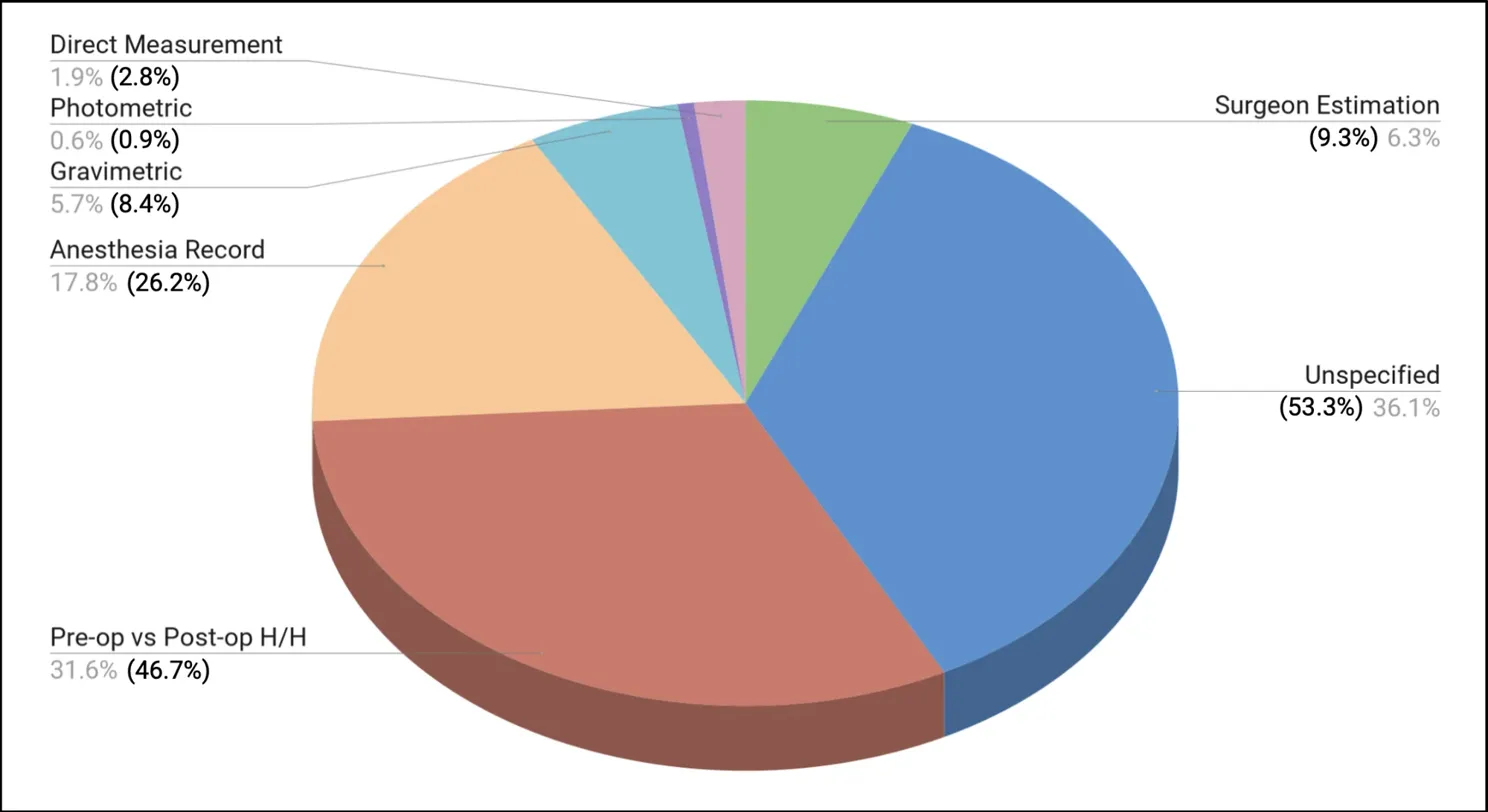
Summary data for EBL quantification method represented as percentage of studies utilizing each method. The grey number reflects the relative percentage compared to others. The black number in parentheses reflects the gross percentage of studies tagged with each EBL method, summating to147.6% as some studies reported multiple quantification methods. H/H = Hemoglobin/Hematocrit.
Figure 3: Perioperative Blood Loss Management Strategies
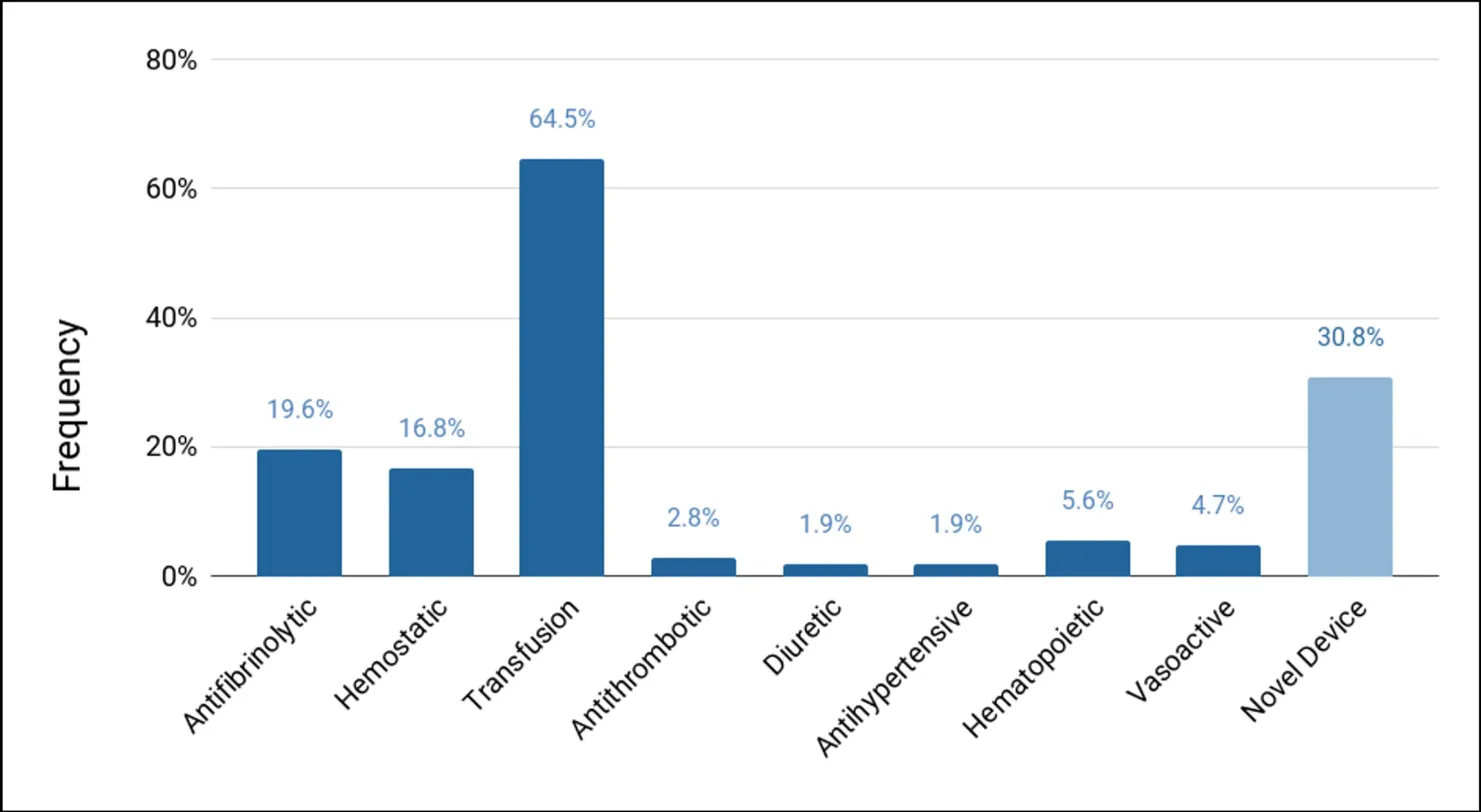
Summary data for blood loss management. Dark blue bars reflect well-defined medical agents or techniques (i.e. transfusion). Light blue bar represents category of strategies consisting of various devices and technologies.
Conclusions and Discussion
●The majority (53.3%) of published studies include data on estimated blood loss (EBL), but do not specify a quantification method.
●Beyond this, there is heterogeneity in how blood loss is quantified.
●Beyond this, there is heterogeneity in how blood loss is quantified.
●Transfusion is the most frequently utilized perioperative management strategy. Various devices and hemostatic agents have a role, but little research specifically investigates these technologies in specific surgical contexts.
●Limitations
○Comparison of EBL across numerous different surgical procedures with variable blood loss is difficult.
○No meta-analysis performed due to significant heterogeneity.
○Majority of included studies were retrospective in nature.
References
1.Rothermel, L. D., & Lipman, J. M. (2016). Estimation of blood loss is inaccurate and unreliable. Surgery, 160(4), 946–953. https://doi.org/10.1016/j.surg.2016.06.006
Neurons in the lateral prefrontal cortex encode task features during virtual navigation

Introduction
- Lateral prefrontal cortex (LPFC) is uniquely found in primates.1
- Associated with context dependent learning and behaviour.2,3
- Single neurons in the LPFC are tuned to task-relevant features.4,5
- LPFC neuron tuning has not been explored in naturalistic settings.
Methods
Figure 1. Experimental Design
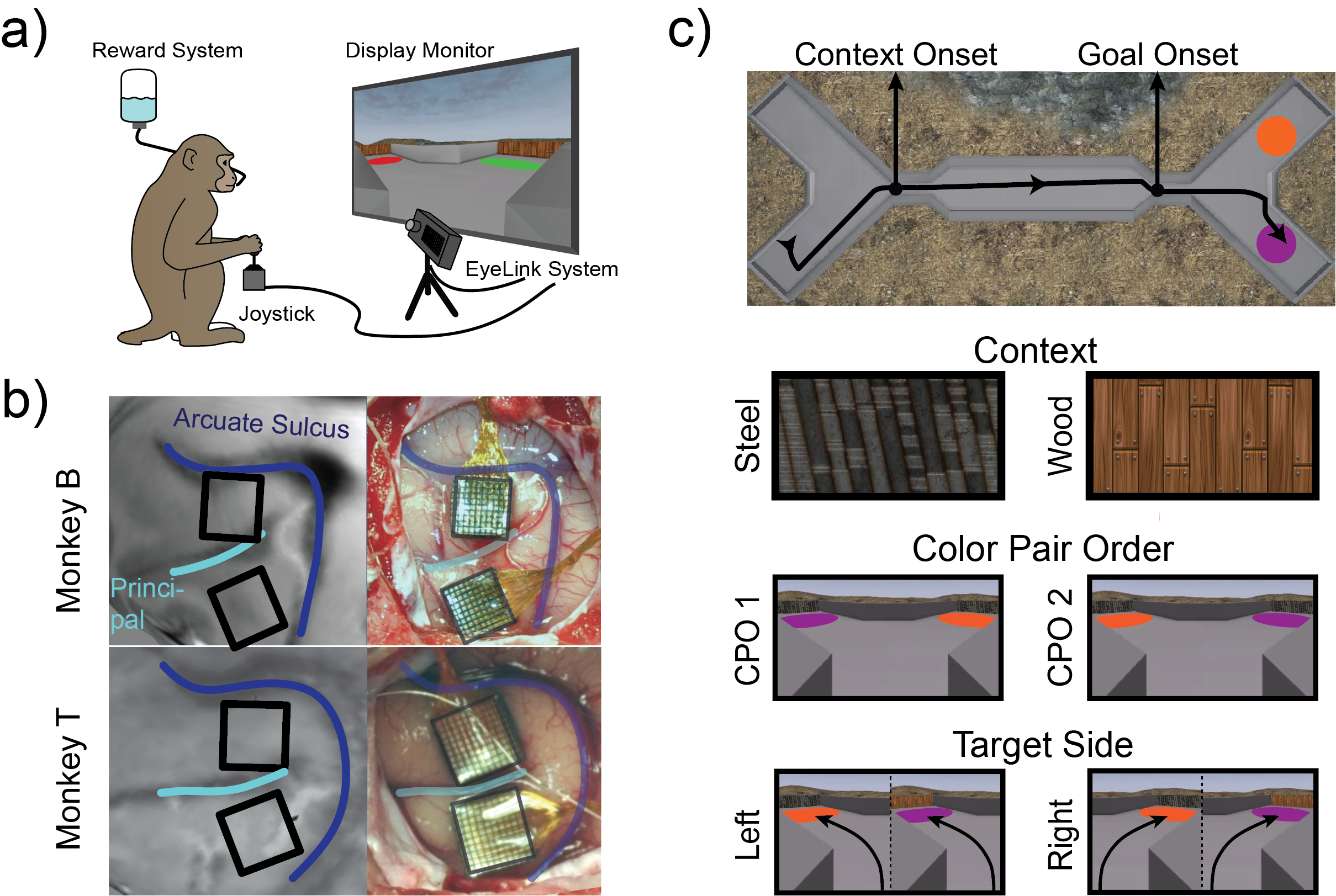
a) Monkeys were seated in front of a monitor and used a joystick to navigate. b) Utah arrays, placed in the dorsal (areas 9/46d) and ventral (area 9/46v) lateral prefrontal cortex c) Overview of X-maze, with an example path taken during one trial, with the onset of the context (steel or wood) and goal (coloured discs) indicated. Task conditions shown are context, color pair order (CPO), and target side.
- Mean firing rate (FR) for each neuron was computed over running 400ms time bins.
- Individual neuron tuning to eye position and task features were assessed with multivariate linear regressions.
- Neuron population analysis was performed using two methods:
- Task features were decoded from population activity using a support vector machine, with 5-fold cross validation.
- Linear discriminant analysis was used on population activity to find orthogonal axes explaining task features.
Results
- Task completed with mean accuracy (± standard error) accuracy of 80.9 ± 0.02%.
- During this, a total of 813 neurons were recroded from.
- The dorsal and ventral LPFC had different tuning profiles (Chi-Square, χ = 30.36, p<0.001)
Figure 2. Single Neuron Tuning around Goal Onset
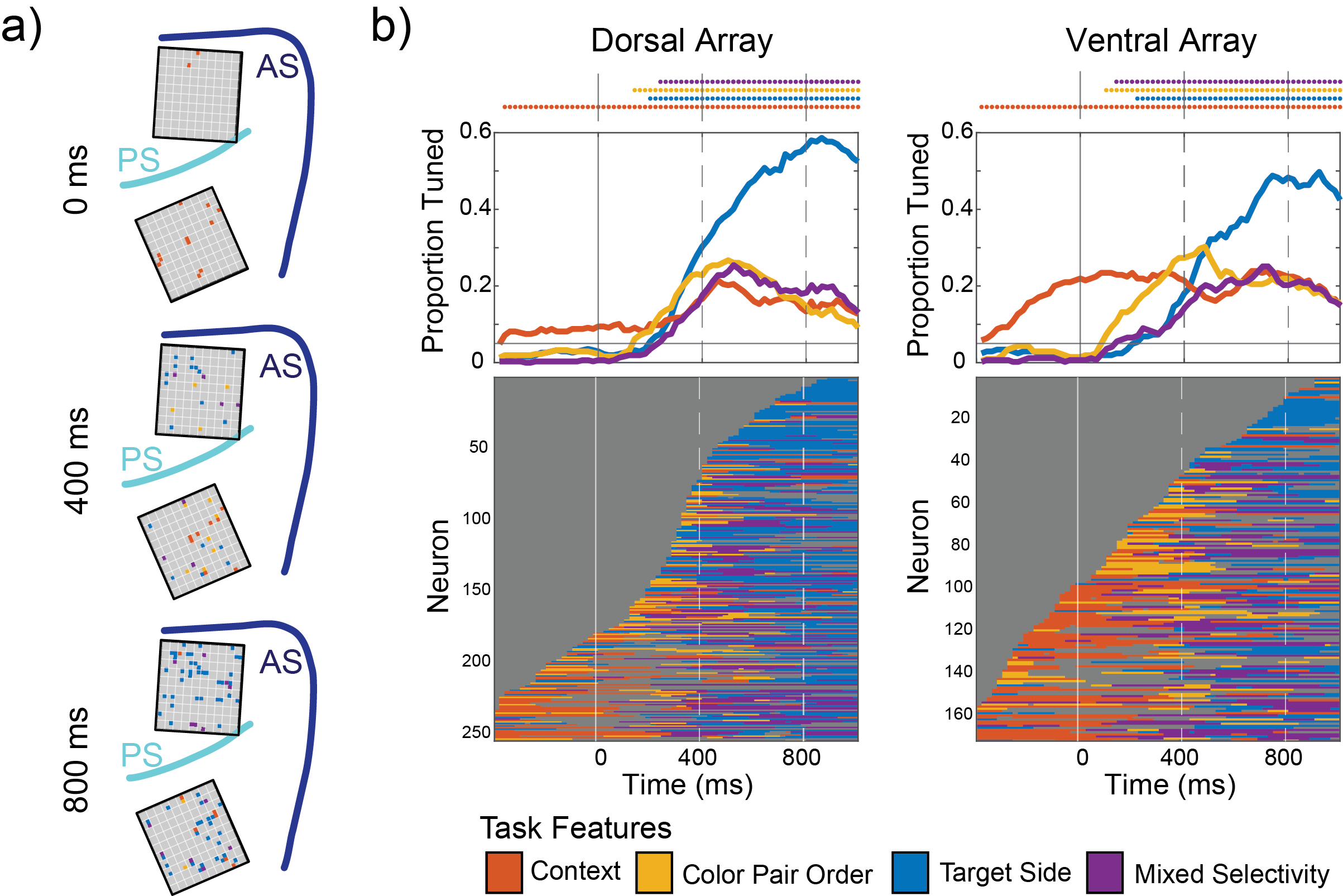
a) Location of tuned neurons within the Utah arrays at 0ms, 400ms, and 800ms. b) Total proportion of tuned neurons over time. Top plots show the total proportion of neurons tuned to task features, with the points above indicating a proportion above 0.05. Bottom plots represent each unit’s tuning over time, sorted from bottom to top by onset of tuning to any feature.
Figure 3. Decoding Task Features across Sessions
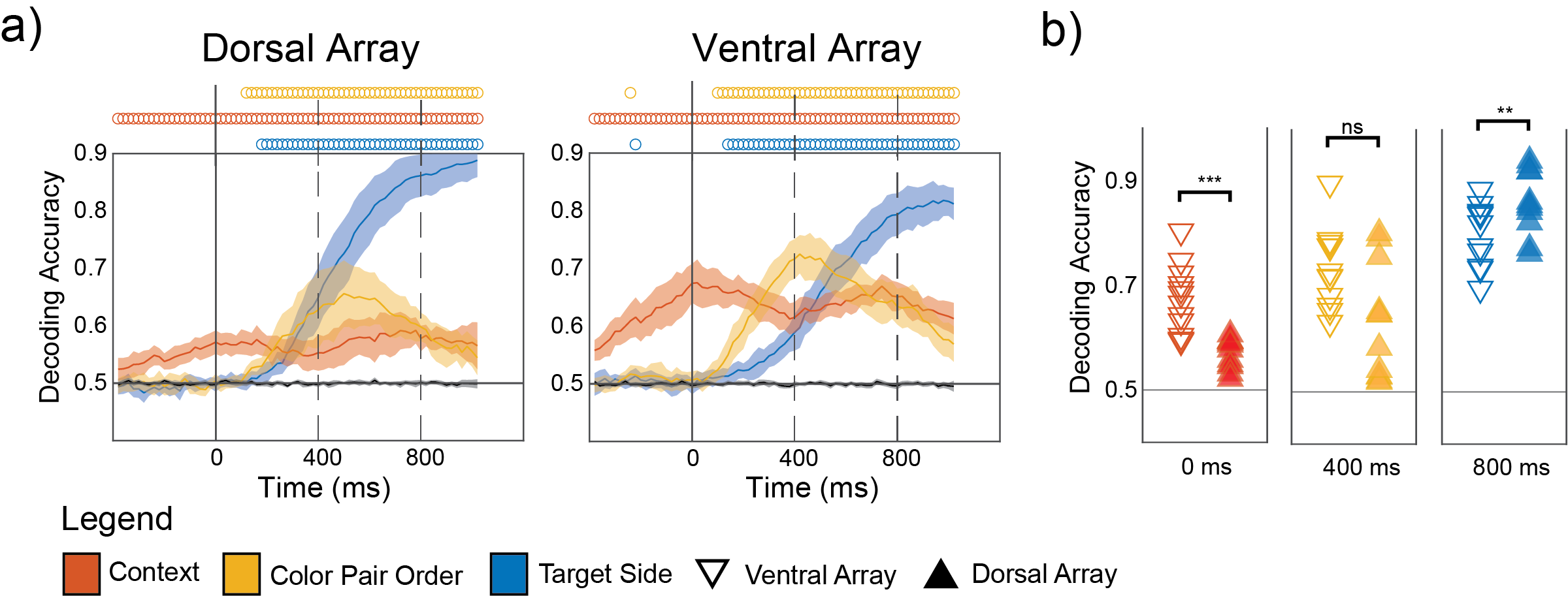
a) Mean (±2SE) decoding accuracies of task features across sessions. b) Comparing decoding accuracy between the ventral and dorsal LPFC (ns p>0.05, * p<0.05, ** p<0.01, *** p<0.001).
Figure 4. Neural Trajectories Along Task Dimensions
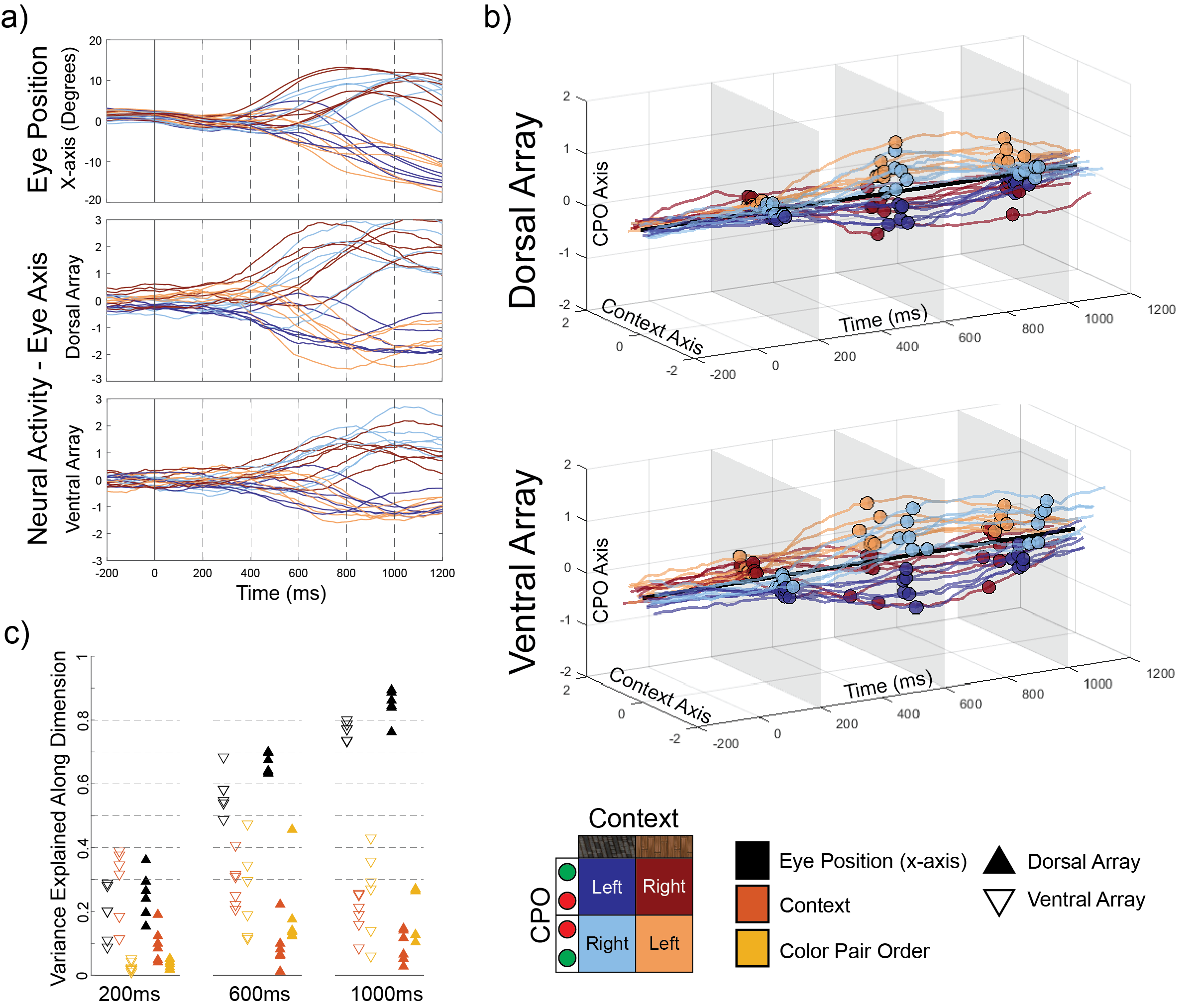
a) Mean x-axis eye position across sessions (top), neural activity projected on the eye position dimension for the dorsal (middle) and ventral arrays (bottom). b) Neural activity projected on task dimensions (context and CPO) across time, demonstrating separation of the different task conditions. This separation was greater in the ventral array compared to the dorsal array. c) Variance of neural activity along task dimensions explained by the task features.
Discussion
- Our main findings were:
- LPFC neurons were tuned to task features in a naturalistic setting.
- LPFC neurons exhibited mixed selectivity, changing over time.
- Dorsal and ventral neurons encoded spatial and visual features respectively.
- Despite individual neurons showing mixed selectivities, task features were separated across populations of neurons along few dimensions.
- The LPFC has been suggested as a potential brain machine-interface target6, which is further supported by this work.
References
1. DOI: 10.1073/pnas.1721653115 2. DOI: 10.1016/j.neuron.2014.08.011
3. DOI: 10.1016/0166-4328(85)90085-3 4. DOI: 10.1016/s0896-6273(00)80658-3
5. DOI: 10.1038/nature12160 6. DOI: 10.1088/1741-2552/acb5c2
1. DOI: 10.1073/pnas.1721653115 2. DOI: 10.1016/j.neuron.2014.08.011
3. DOI: 10.1016/0166-4328(85)90085-3 4. DOI: 10.1016/s0896-6273(00)80658-3
5. DOI: 10.1038/nature12160 6. DOI: 10.1088/1741-2552/acb5c2
Long-term quality of life deterioration in vestibular schwannoma patients treated with radiotherapy: a matched cohort with surveillance, radiation and surgery
Background: The Dilemma - which treatment option?
With a reduction in mortality rate and the increasing role of radiation therapy in vestibular schwannoma (VS) management amongst other mainstay treatments of surgery and active surveillance, there is a need to understand differences in outcomes of long-term quality of life (QoL) in patients.
The primary aim of treatment is to prevent complications arising from tumor growth
With a reduction in mortality rate and the increasing role of radiation therapy in vestibular schwannoma (VS) management amongst other mainstay treatments of surgery and active surveillance, there is a need to understand differences in outcomes of long-term quality of life (QoL) in patients.
The primary aim of treatment is to prevent complications arising from tumor growth

Research question:
While general long-term QoL data is increasingly available, none have accounted for confounding factors such as patient age and tumor size. Thus, we sought to investigate:
While general long-term QoL data is increasingly available, none have accounted for confounding factors such as patient age and tumor size. Thus, we sought to investigate:
Comparison of long-term impacts on patient quality of life in matched patient cohorts between active surveillance, radiation and surgical management for vestibular schwannomas
Methods
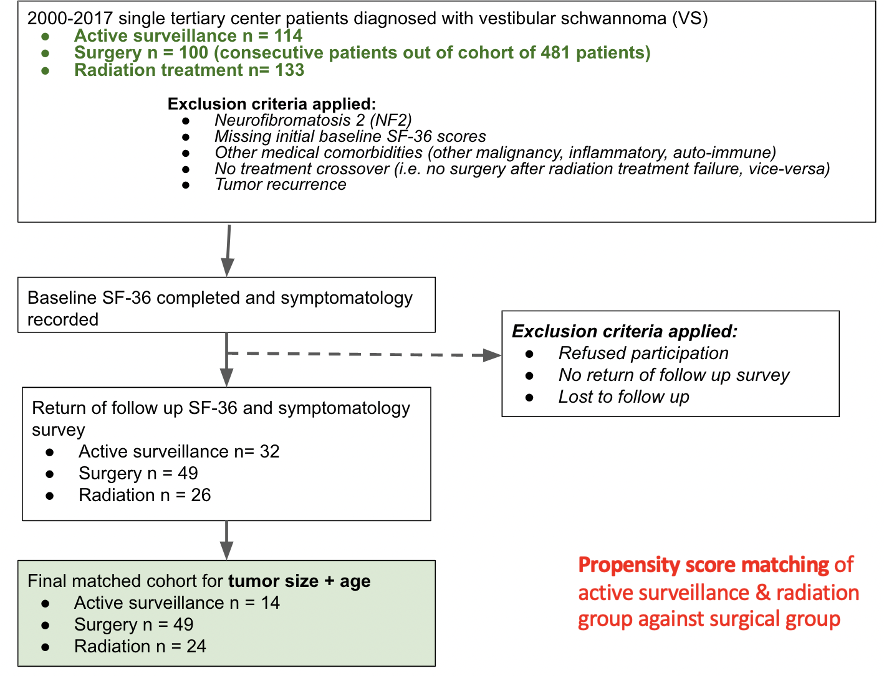
Results: Cohort characteristics
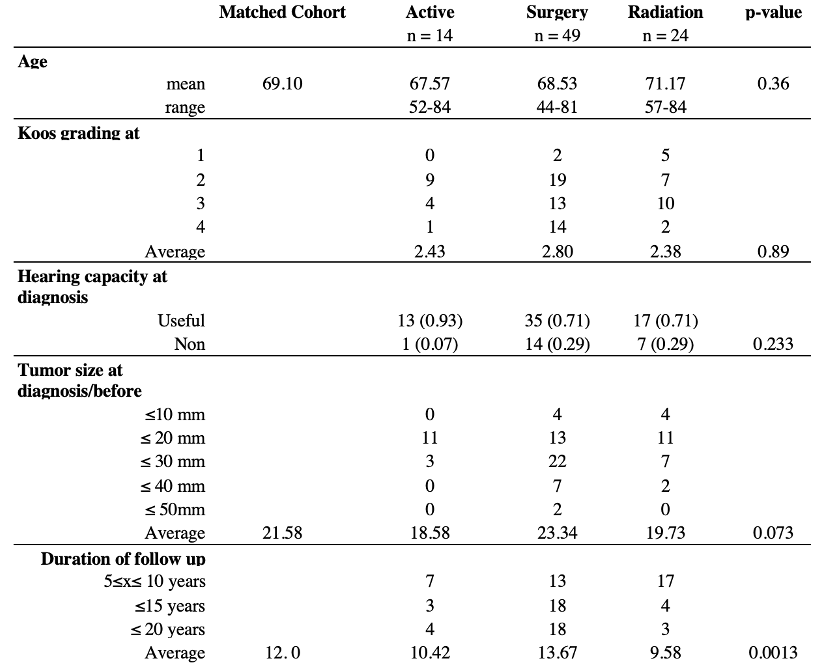
Results: SF-36 summary scores
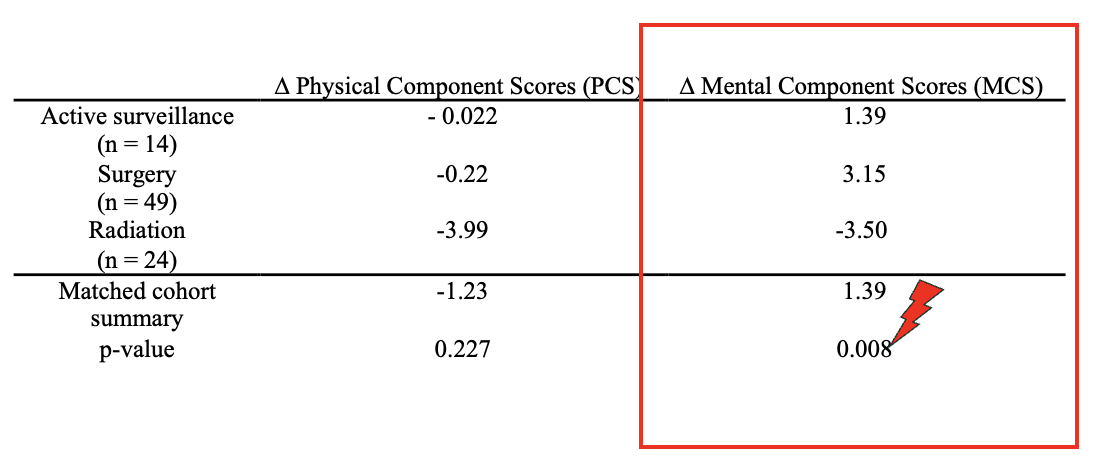
Results: SF-36 subdomain scores

Results: ∆SF-36 Radiation vs Surgery

Results: ∆ in proportion of symptoms
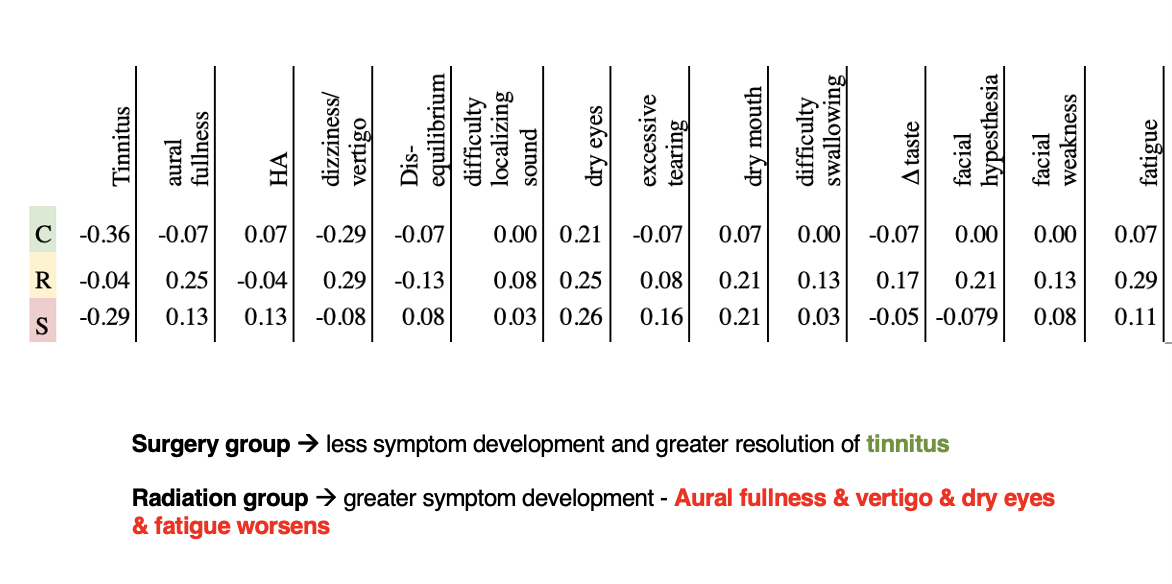
Conclusion
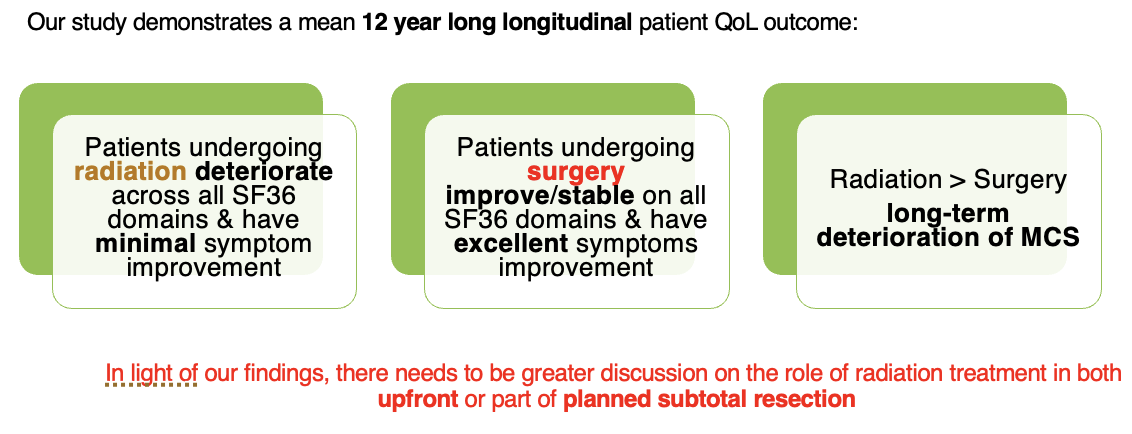
Automated awake brain mapping with eloquentaid: a novel tool for low-resource settings

BACKGROUND
- Intraoperative testing for awake craniotomies requires a multidisciplinary team which may not be available in low-resource settings
- We explored the creation of an AI application to automate an image naming task
METHOD
- We developed a NodeJS application, EloquentAid (https://www.eloquentaid.com/), for language testing automation
- This is a proof of concept, wherein we used an image-naming task based on a 57-item adaptation of the Boston Naming Test
- Images were recreated using OpenAI GPT-4
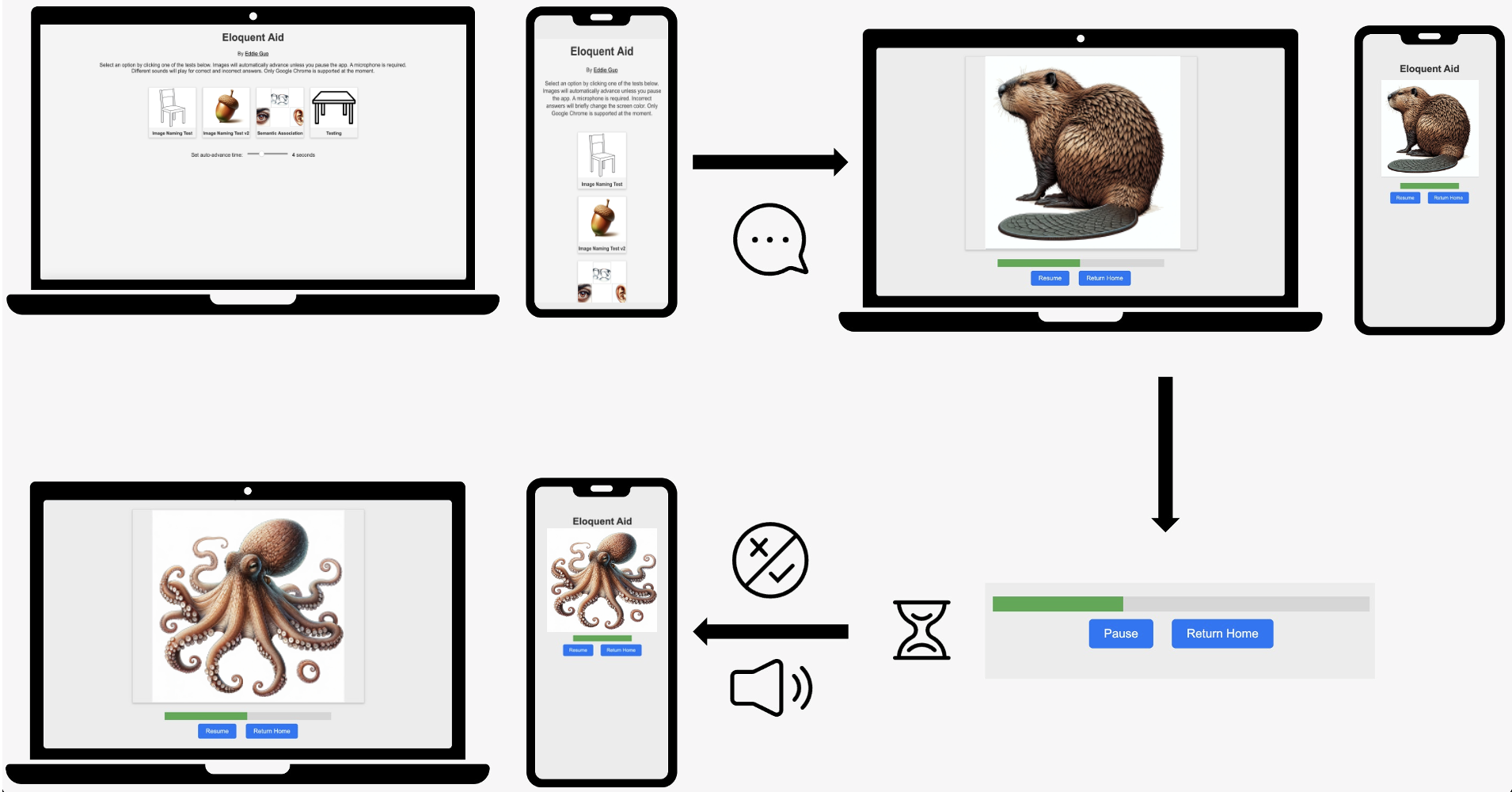
WORKFLOW
- Users open the EloquentAid website on an internet browser on any device with an active internet connection and a microphone (i.e. cellphone, tablet, laptop, desktop)
- They select the length of time a stimulus appears before transitioning to the next one (i.e. 4 seconds)
- They then select the image-naming task
- During the task, the user verbally identifies the image within the time frame selected
- EloquentAid transcribes the response using OpenAI's Whisper transcription service for audio-based input
- EloquentAid evaluates response correctness by checking if the transcribed word matches the correct one
- After the stimulus time passes, feedback is given through auditory (bell with different tones) signals, and it moves to the next item
- The tone codes (correct vs incorrect) would only be known to the investigator
Proof of concept testing
- We iniitally tested EloquentAid amongst the study investigators
- Since the the target of EloquentAid would be use for low-resource settings, neurosurgery and neurology resident volunteers from the Philippines were asked to use EloquentAid through all 57 items (in English)
- All spoke English as their second or third language, as English was the medium of instruction in medical School and in the hospital
- One of the investigators supervised this encounter, and determined the in/correctness of EloquentAid
- Performance metrics and human-application agreement measures were determined
- Qualitative surveys were obtained afterwards
RESULTS
- 798 observations were recorded (N=14; 57 items each)
Confusion Matrix
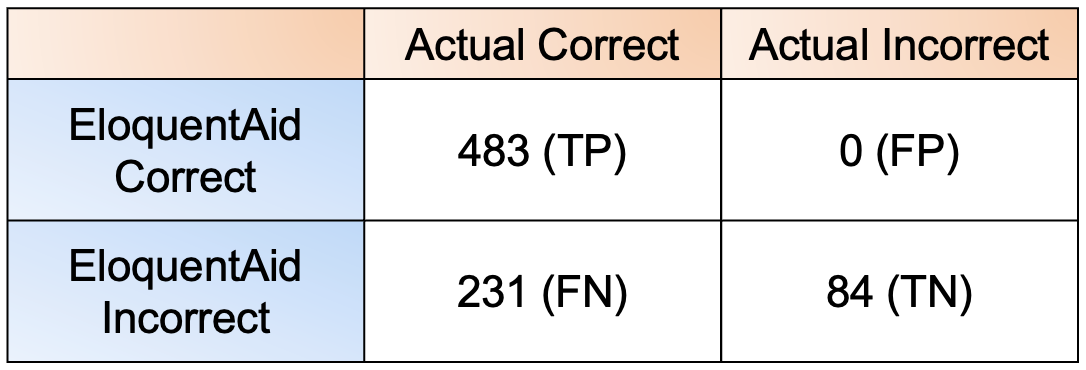
TP -True positive; FP - Flase positive; TN - True negative; FN - False negative
Performance Metrics
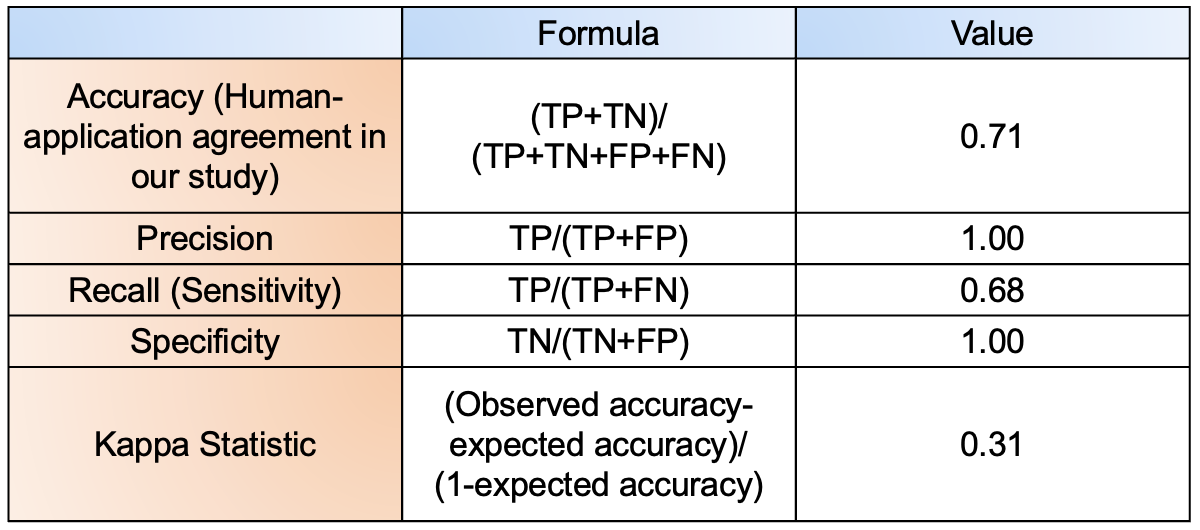
Qualitative comments
- Human error:
- From unfamiliarity with the objects being shown (e.g. "yolk," "trellis")
- From using semantic alternatives (e.g. Stimulus: "Canoe" - Response: "Boat")
- EloquentAid errors:
- Difficulty ascertaining different accents and pronunciations of words
- Slow internet connection causes a delay in transcription leading to an incorrect assessment
- Suggestions for improvement
- Refinement of graphical user interface (GUI) to be more user-friendly (instructions)
- Improvement of speech recognition transcription services

KEY POINTS
- EloquentAid is a promising tool to facilitate automated intraoperative language testing in resource-limited environments
- Among a group with English as the second/third language but used daily in an academic setting, the human-application agreement was 71% and Cohen's Kappa showed a fair agreement (0.31)
- It did not produce any false positive determinations; leading to high precision and specificity
- Human errors were thought to arise from stimuli difficulties - likely from cultural and environmental differences
- EloquentAid errors were thought to be from transcription errors - likely from difficulty with different accents and pronunciations
- More work needs to be done in terms of streamlining the GUI, improving the transcription, and adding additional testing paradigms in the future
Implementation of BC Children’s Hospital’s intraventricular hemorrhage of prematurity management pathway: a quality improvement analysis
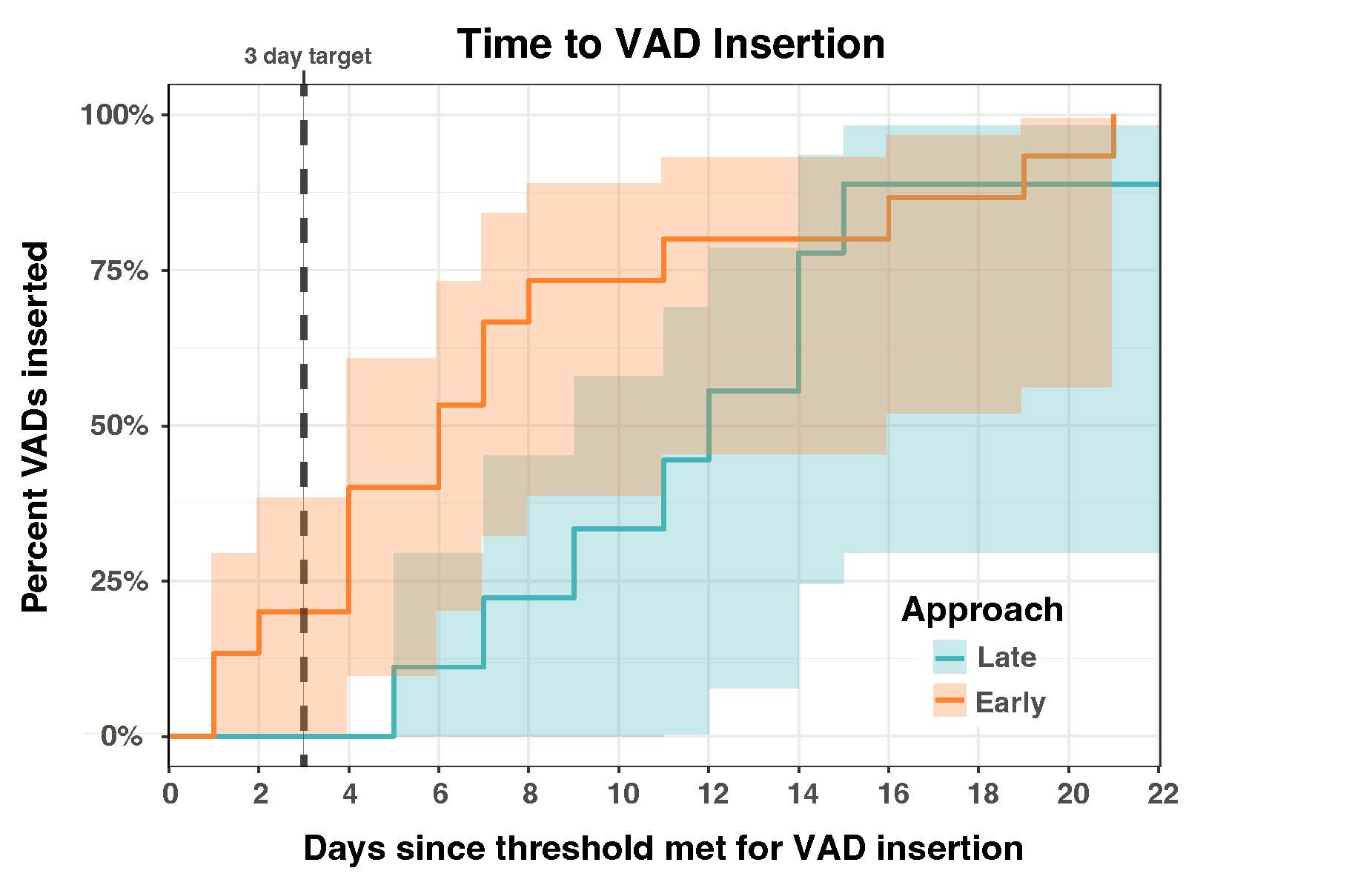

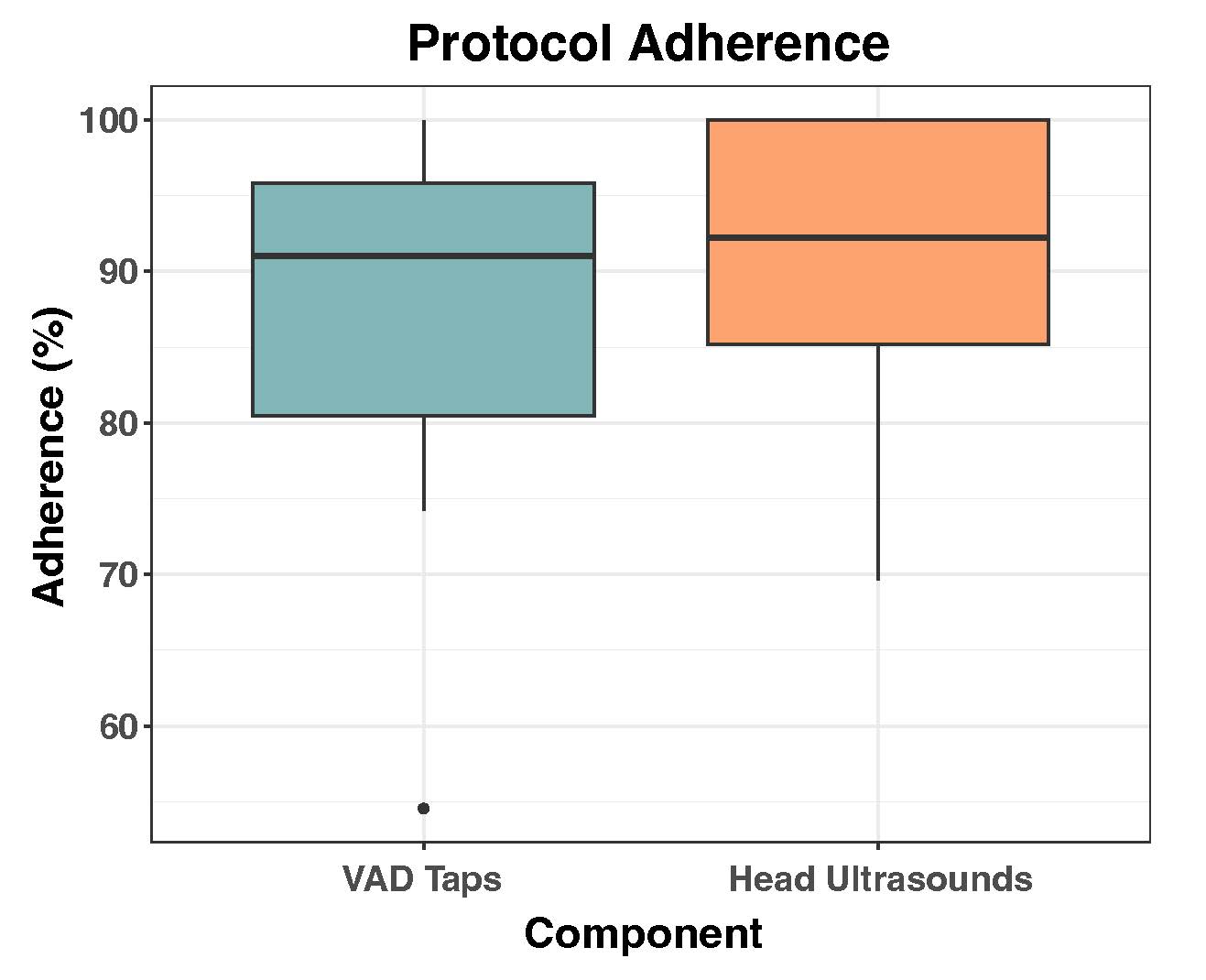
An unlikely impersonator of primary brain tumours: Illustrative case report and literature review of primary angiitis of the central nervous system


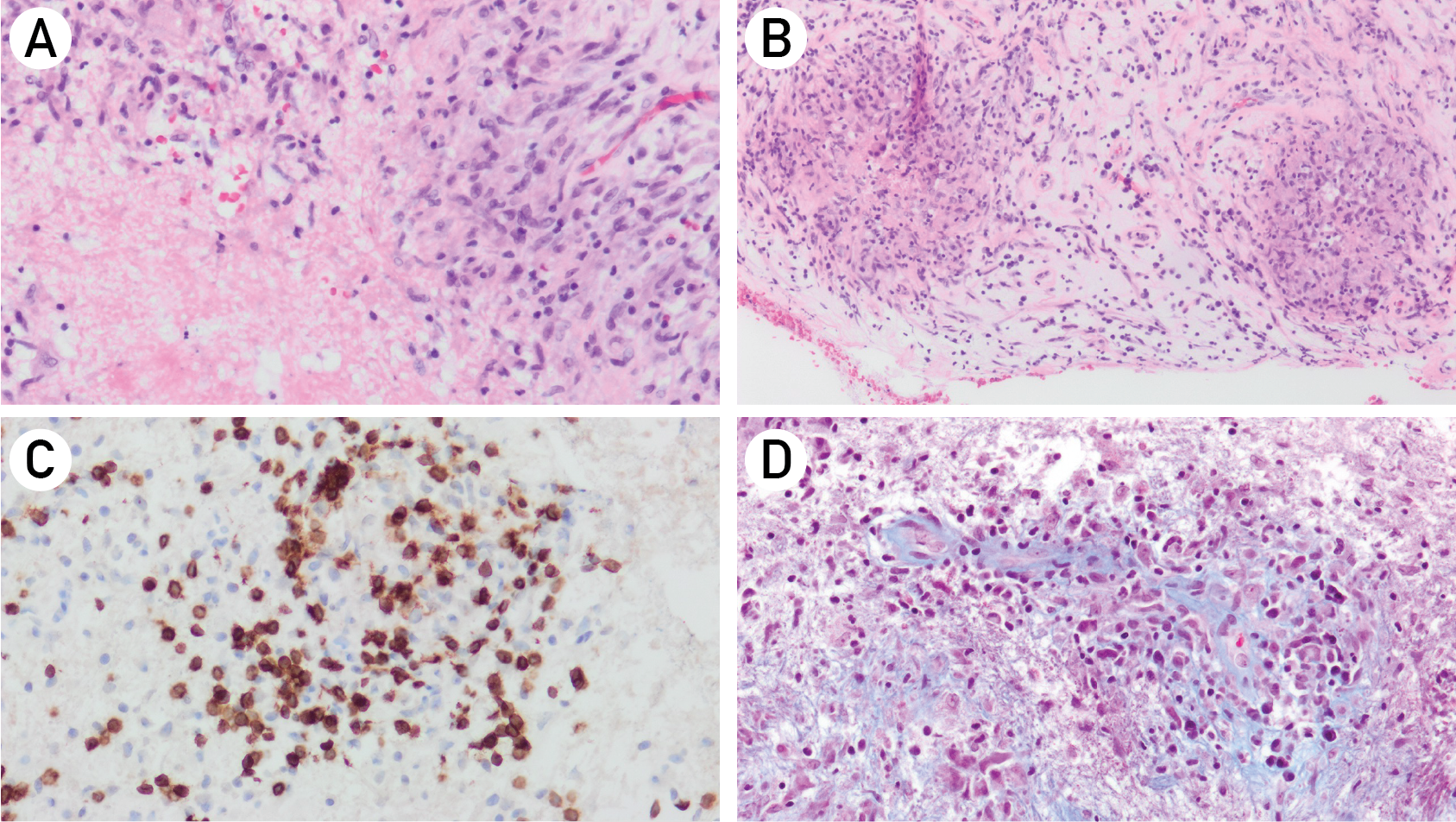


Neurosurgical On-Call Consultations in Nova Scotia: a Descriptive Analysis

Motivation
- Our center services the province of Nova Scotia for all adult neurosurgical care, and the broader Maritime provinces for all pediatric neurosurgical care.
- The NS population estimates continue to grow, with recent figures from July 2023 estimating 1,058,694 people living in NS.
- When including the pediatric catchement area, we service a catchment population of over 2 million people.
- On-call consultations come from many settings (e.g., in-house, outside consults, emergency departments, inpatients, community clinics/offices)
- Dispositions are wide-ranging (e.g., no recommendations, no further investigations/follow up, planned outpatient clinic visits, further workup needed, direct neurosurgical admission, urgent (or delayed) operative management).
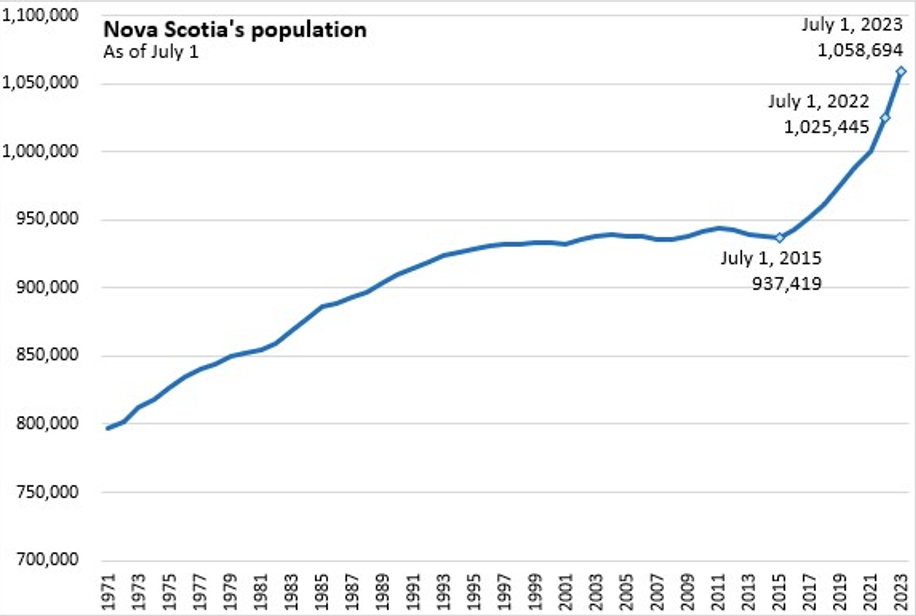
Methods
- Retrospective review of prospectively collected on-call consultation records
- 12 month period (February 2019 to February 2020)
- Consults were coded according to origin and disposition
- No recommendations
- No further investigations/follow up
- Planned outpatient clinic visit
- Further workup needed
- Direct neurosurgical admission
- Urgent (or delayed) operative management
Results
Demographics
- 1916 total consults were reviewed from a 12-month period
- The mean patient age was 60.1+/- 0.4 years
- 55% of patients were male, 45% were female
Consult Details
- 52% of consults came from outside sites, whereas 48% of consults originated within our local institution
- The majority of consults (72%) were from emergency departments, while 19% of consults came from inpatient wards, and the remaining 9% were from office-based settings
- 64% of neurosurgical consults involved cranial cases, and 36% were for spine
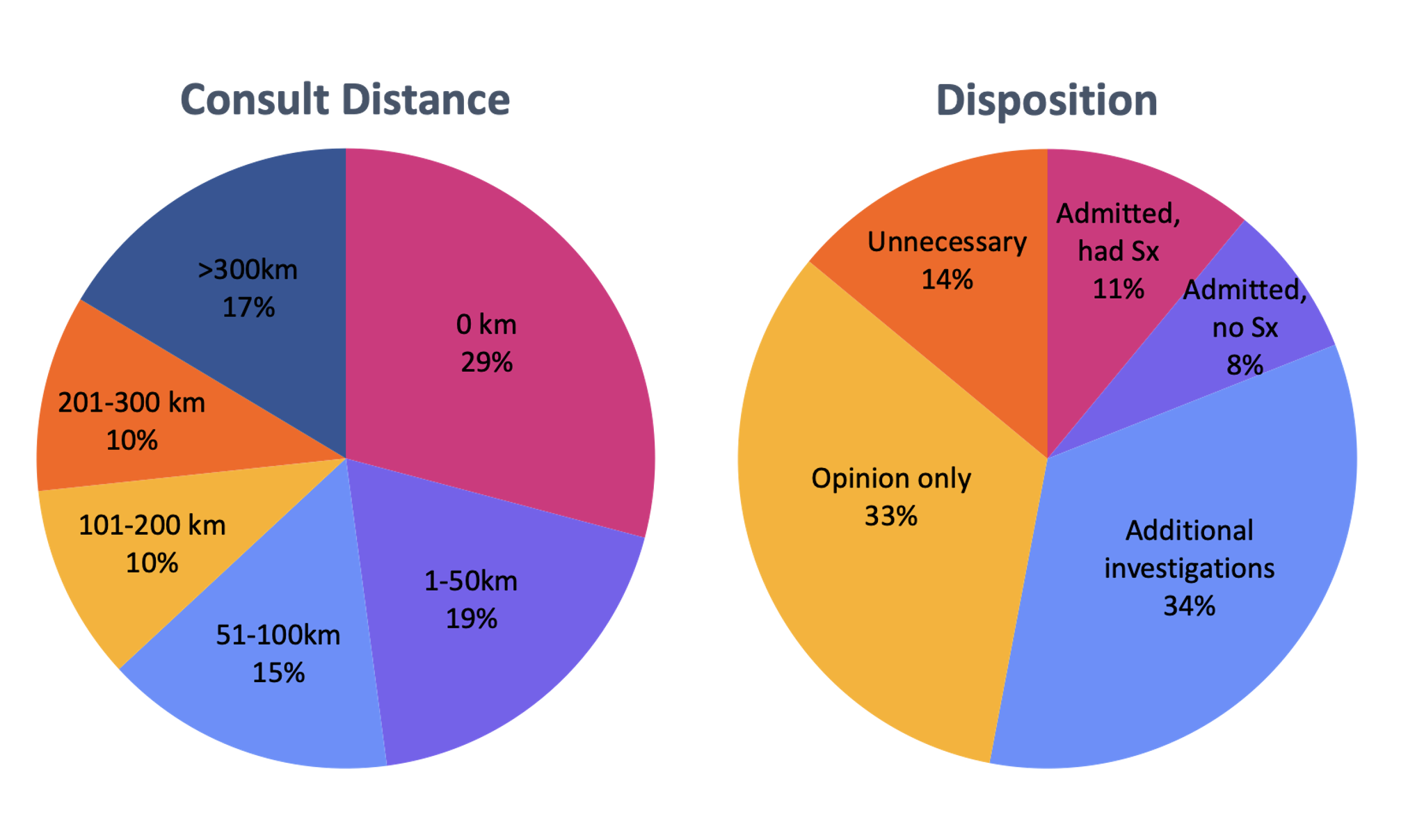
Regression Analysis
In multinomial logistic regression analysis, the following were associated with consult disposition (p < 0.001):
- Patient age
- Geographical distance of the consulting site
- Consult-specific variables (neurosurgical subspecialty, inside versus outside call, emergency department versus inpatient ward versus outpatient office)
Conclusions
- This is the first descriptive analysis of on-call neurosurgical consultations in Canada
- The majority of neurosurgical consults at our center originate from emergency departments and involve cranial cases
- There is a wide variety of consult dispositions, and associated factors identified in multinomial logistic regression include patient age, the distance of the consulting site, and consult-specific details
Future Directions
- Gathering data from a newly implemented system of tracking on-call consults
- By quantifying consultation details, we anticipate an opportunity for future education and clinical pathway development for community and hospital-based referring physicians
Authors' Affiliation
Division of Neurosurgery, Dalhousie University, Halifax, NS, CA
Pituitary Apoplexy: a Retrospective Single Center Cohort Study

Background
- Pituitary apoplexy is an acute clinical syndrome caused by hemorrhagic or non-hemorrhagic necrosis of the sella or a pituitary lesion
- Usually occurs in the setting of existing non-functioning pituitary macoadenoma (60-90%)
- Often involves headache, visual deficits, and endocrine dysfunction
- Conservative or surgical treatment can be offered depending on the circumstance
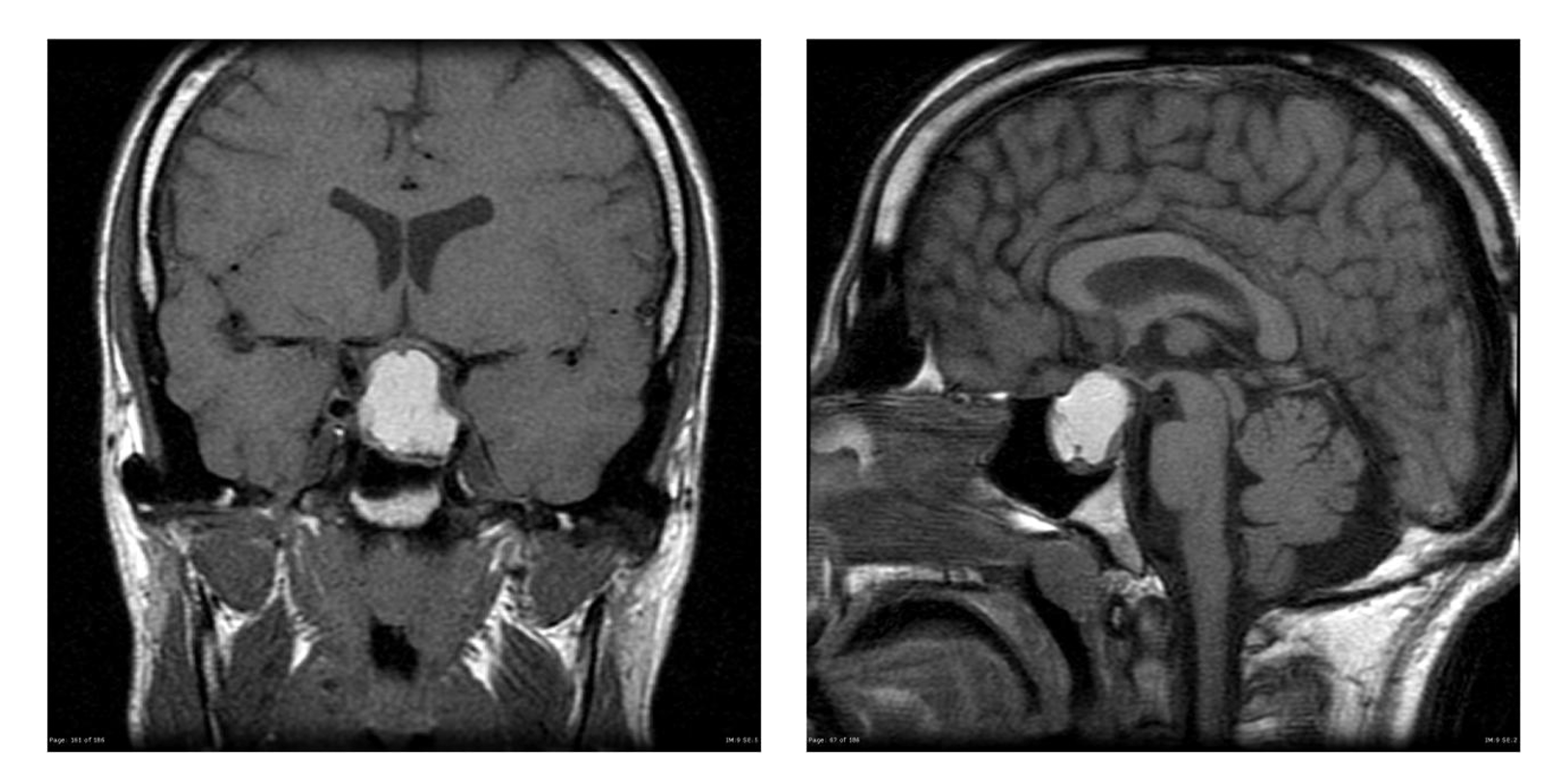
Aims
- Provide a descriptive analysis of patients with pituitary apoplexy treated at our center
- Compare apoplexy patients managed surgically versus conservatively, from acute presentation to longitudinal follow up
Methods
- Single center retrospective cohort study through the Halifax Neuropituitary Clinic
- Patients with symptomatic pituitary apoplexy managed surgically or conservatively from January 2000 to October 2022
- Inclusion criteria: acute clinical presentation with imaging correlate
- Outcomes of interest: demographics, endocrinologic values, radiographic outcomes, clinical outcomes, tumor progression or recurrence
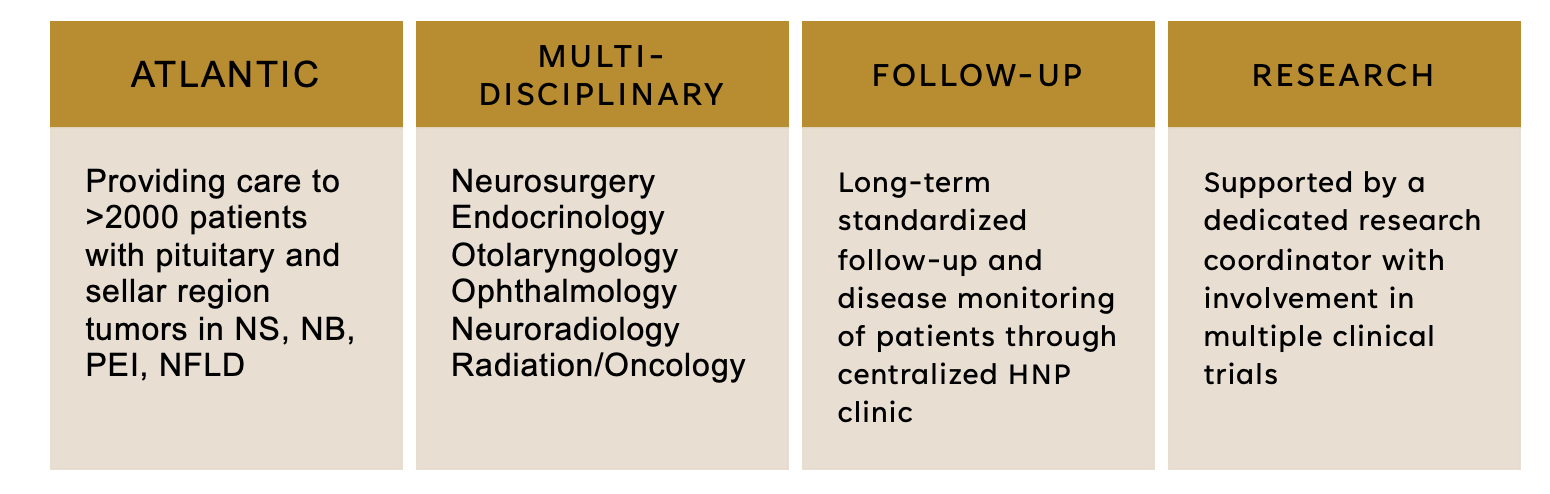
Results
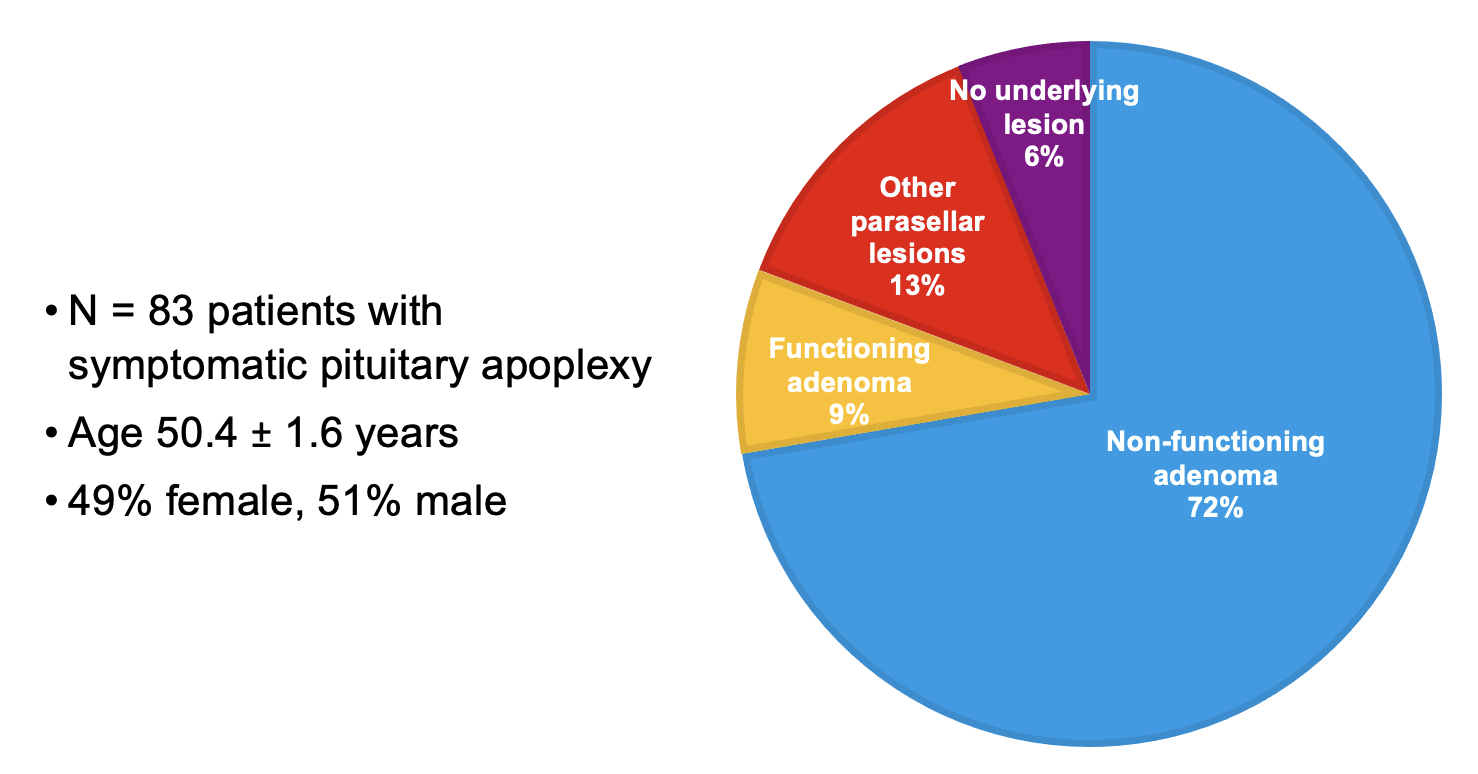
- Patients treated surgically had a tumor size of 27 +/- 14 mm versus 16 +/- 5 mm for those treated conservatively at time of initial presentation
- No group differences in endocrinologic values between groups at time of presentation
- 15% of patients treated surgically underwent an addititonal surgery, of which 67% (n=6) were secondary to tumor recurrence
Results Continued
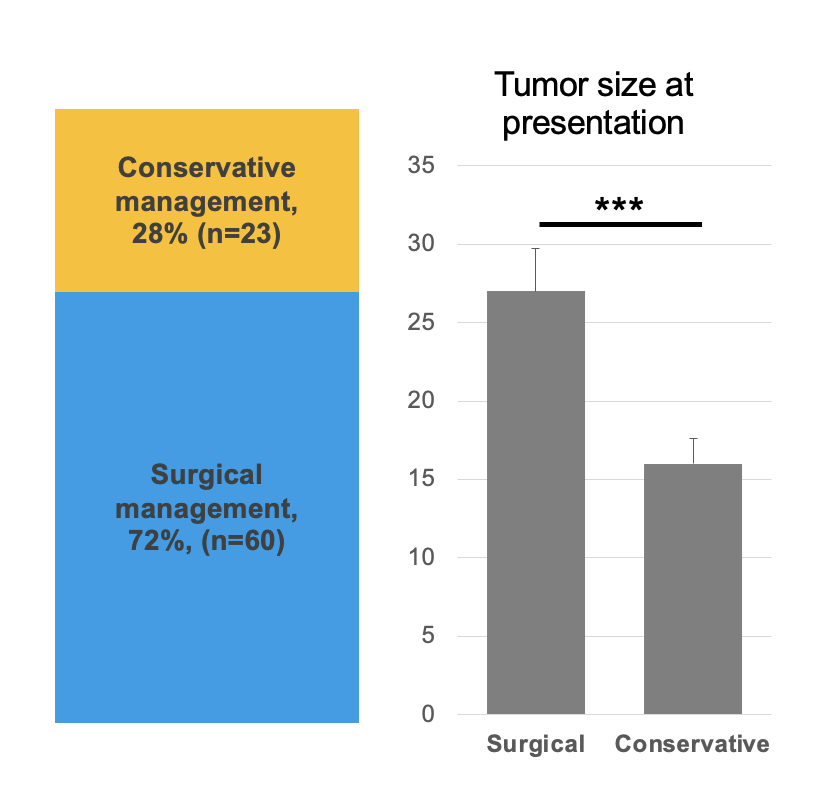
Conclusions
- This is one of the largest reported series of pituitary apoplexy in the literature
- A subset of surgically treated patients will require additional intervention
- Close follow-up is clinically necessary following apoplexy
Future Directions
- Future work will provide further clinical characterization and reasons for surgical intervention versus conservative management
- A detailed analysis of endocrinologic values at presentation and over time will be performed
Acknowledgements
- Thank you to all co-authors for their contrubutions
- EP, SAI, DBC were involved in study conceptualization and design
- EP, MA, AH, and NK were involved in data collection
- EP performed all data analysis
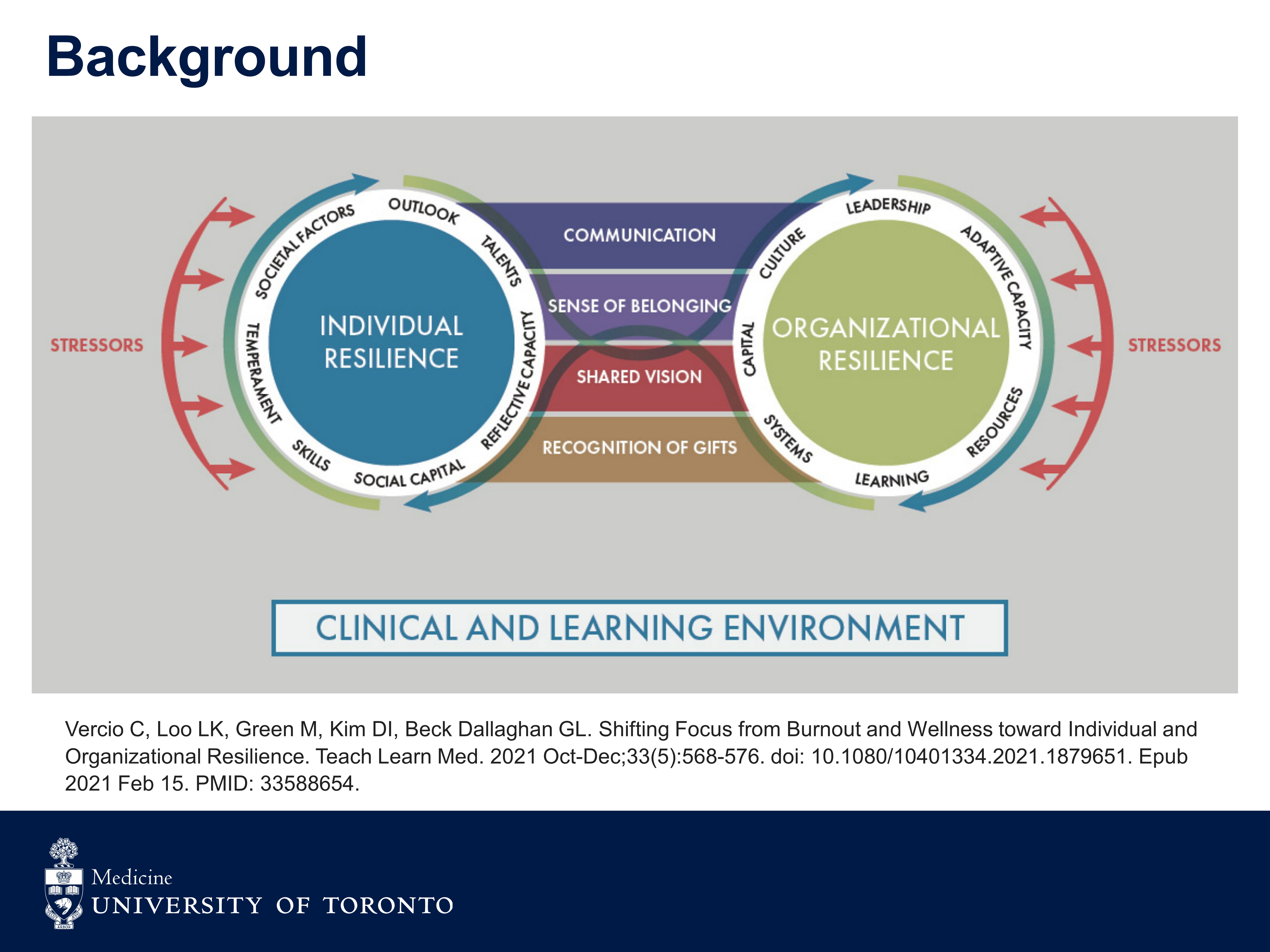

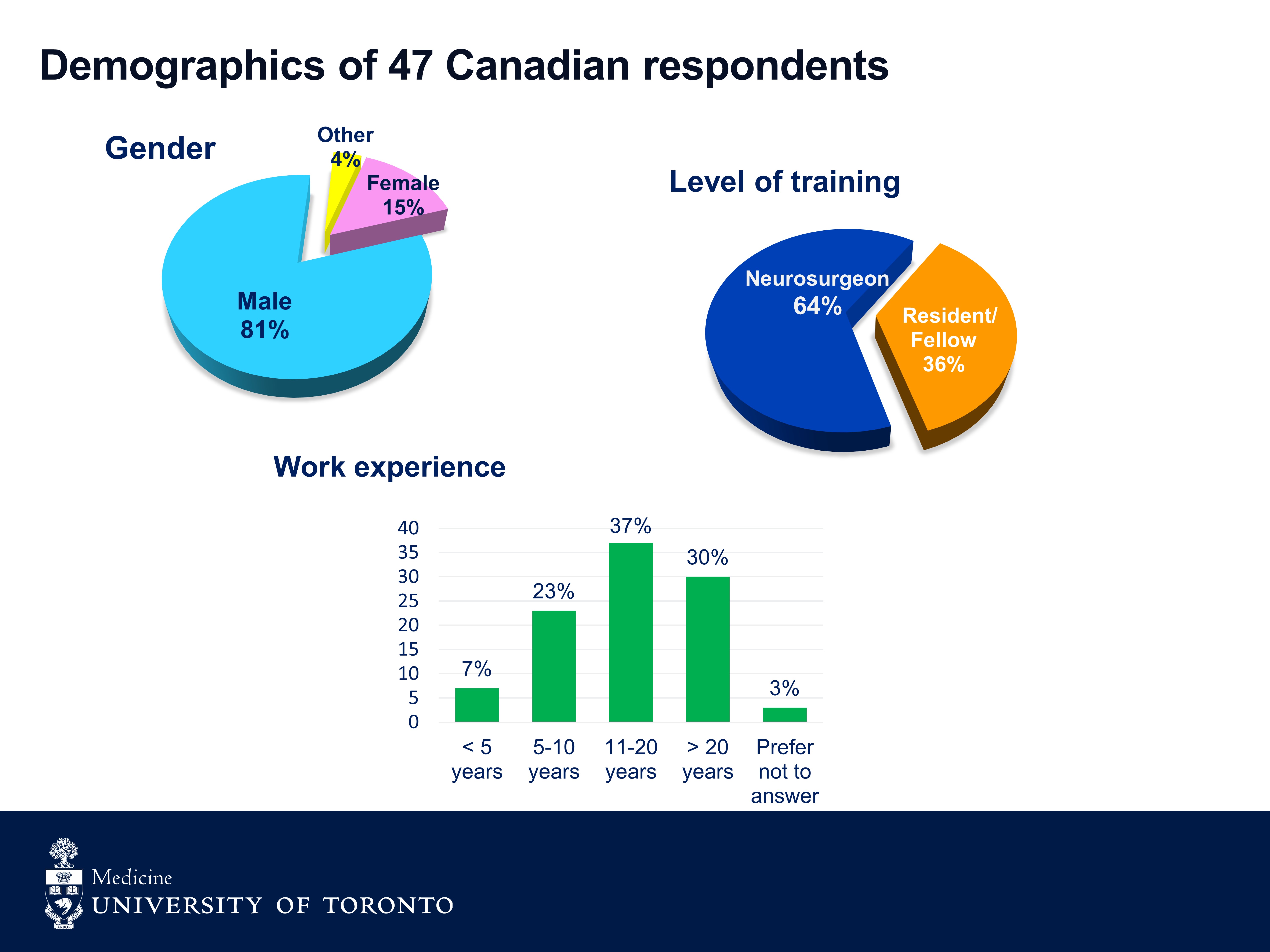
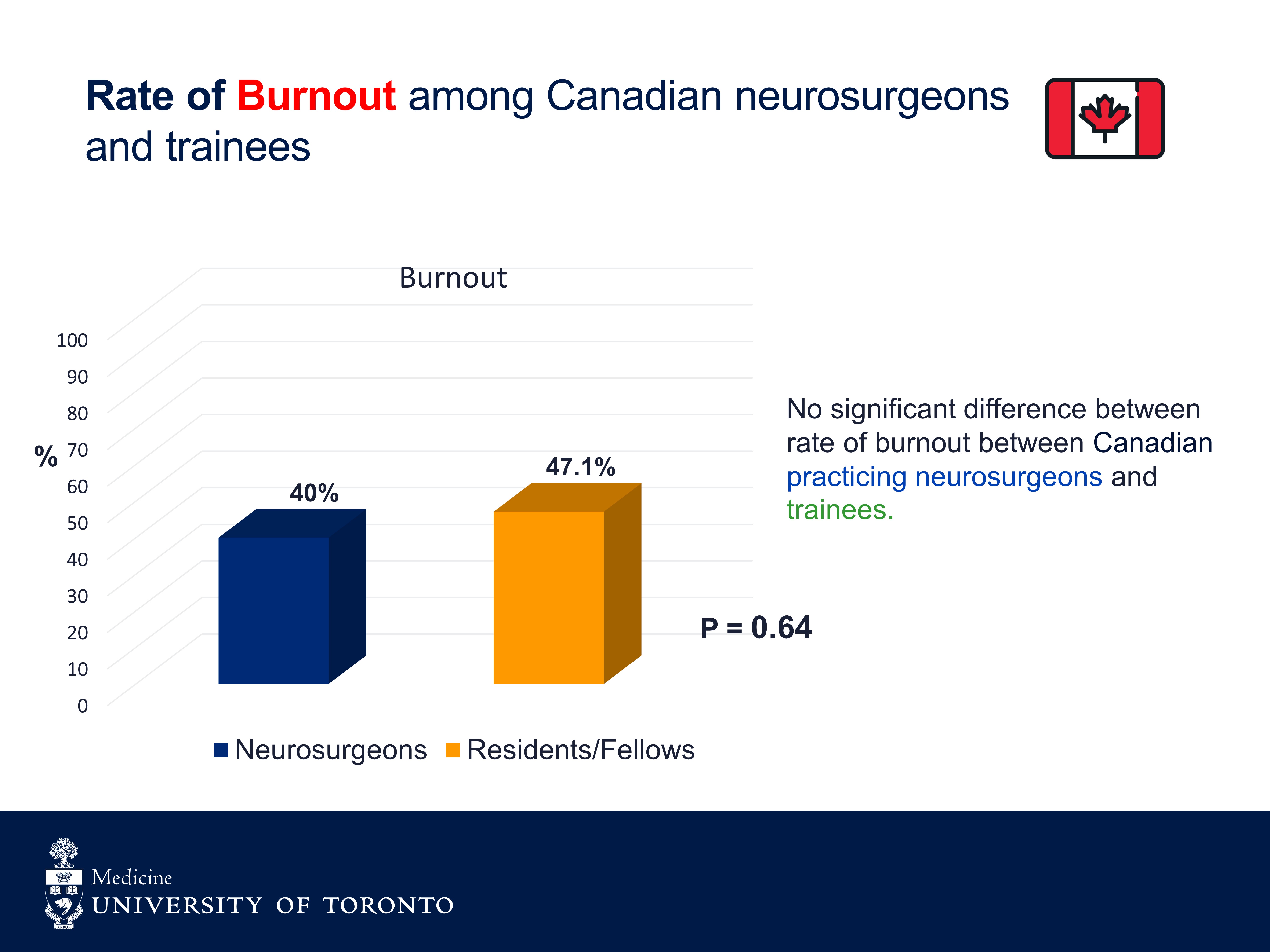


The use of tranexamic acid in craniotomy: a Canadian survey and literature review
INTRODUCTION
- Excess blood loss increases morbidity and mortality during and after neurosurgical procedures.
- There is growing evidence supporting the intraoperative use of an antifibrinolytic agent, tranexamic acid (TXA) to limit blood loss in cardiac, orthopedic, obstetric, and spine surgeries.
- There currently is no guideline regarding the use of TXA in craniotomy.
PURPOSE
- Determine the practice pattern regarding the use of TXA in elective craniotomy in Canada
- Review the current literature on the effect of TXA on the estimated blood loss during elective craniotomy for tumors
METHODS
-
An informal survey was conducted by reaching out to personal contacts.
- Whether or not TXA was routinely used during elective craniotomies
- Indication for intraoperative use of TXA during elective craniotomies
- PubMed was searched for randomized controlled trials reporting the use of TXA in craniotomy for tumors.
RESULTS
- Responses were obtained from 15 neurosurgery programs across Canada.
- None of the 15 centres used TXA routinely in elective craniotomies. 9 centres did not use it, while the remining 6 used it selectively.
- Indications for TXA included expected bleeding risk, intra-op bleeding and surgoen preference.
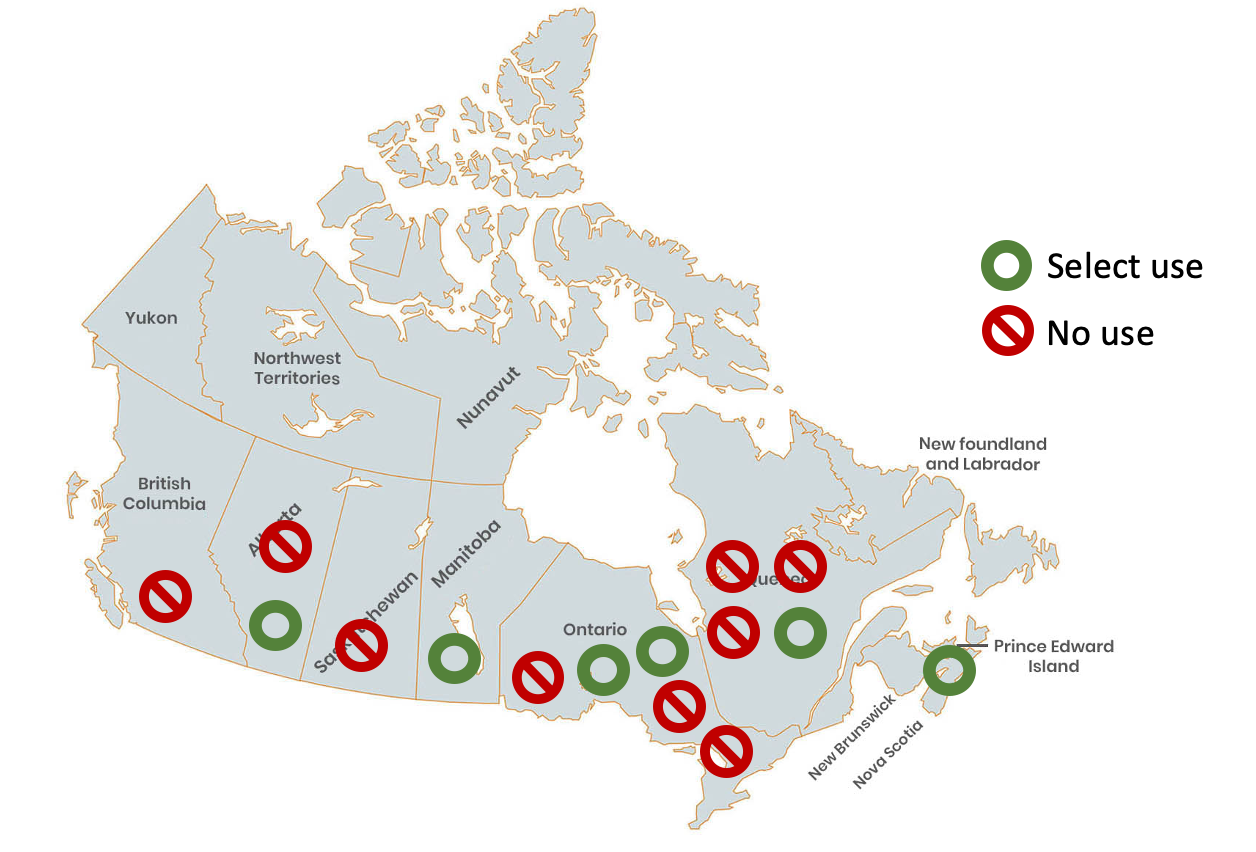
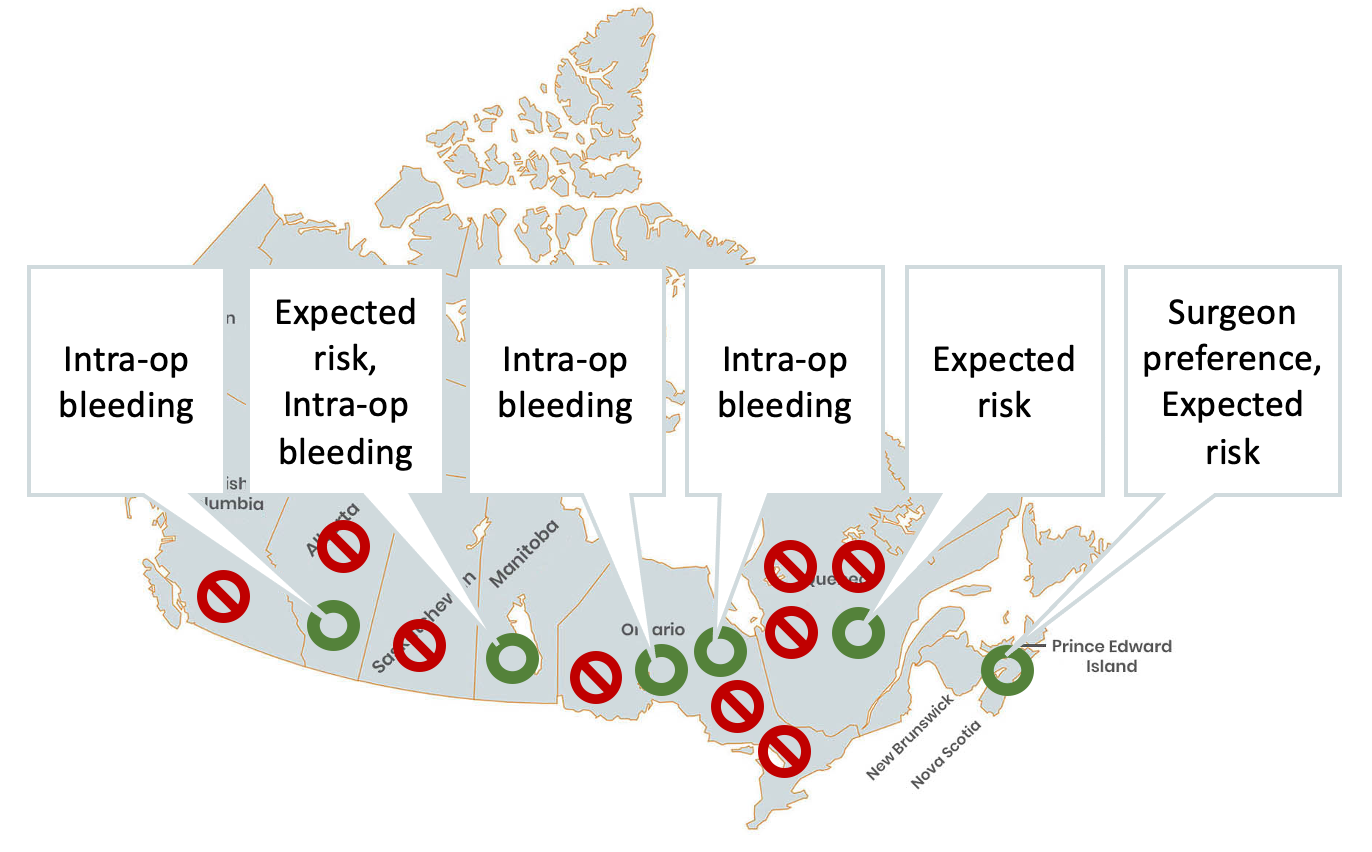
Figure 1. The use of TXA during craniotomies in Canada and its indication.
ACKNOWLEDGEMENT
- Drs. Stephen Lownie and Sean Christie, Lisa Julien, Dr. Ryan Greene
- Responders to survey
- Dalhousie Department of Surgery (DoS) Seed Grant
LITERATURE REVIEW
- 6 studies were published in 2015–2022.
- Sample sizes varied between 30–100.
- Indication for craniotomy was tumor or meningioma.
- There was a significant reduction in estimated blood loss.
- There were variable effects on transfusion requirement, operative duration, and length of hospital stay.
- There was no difference in adverse events.
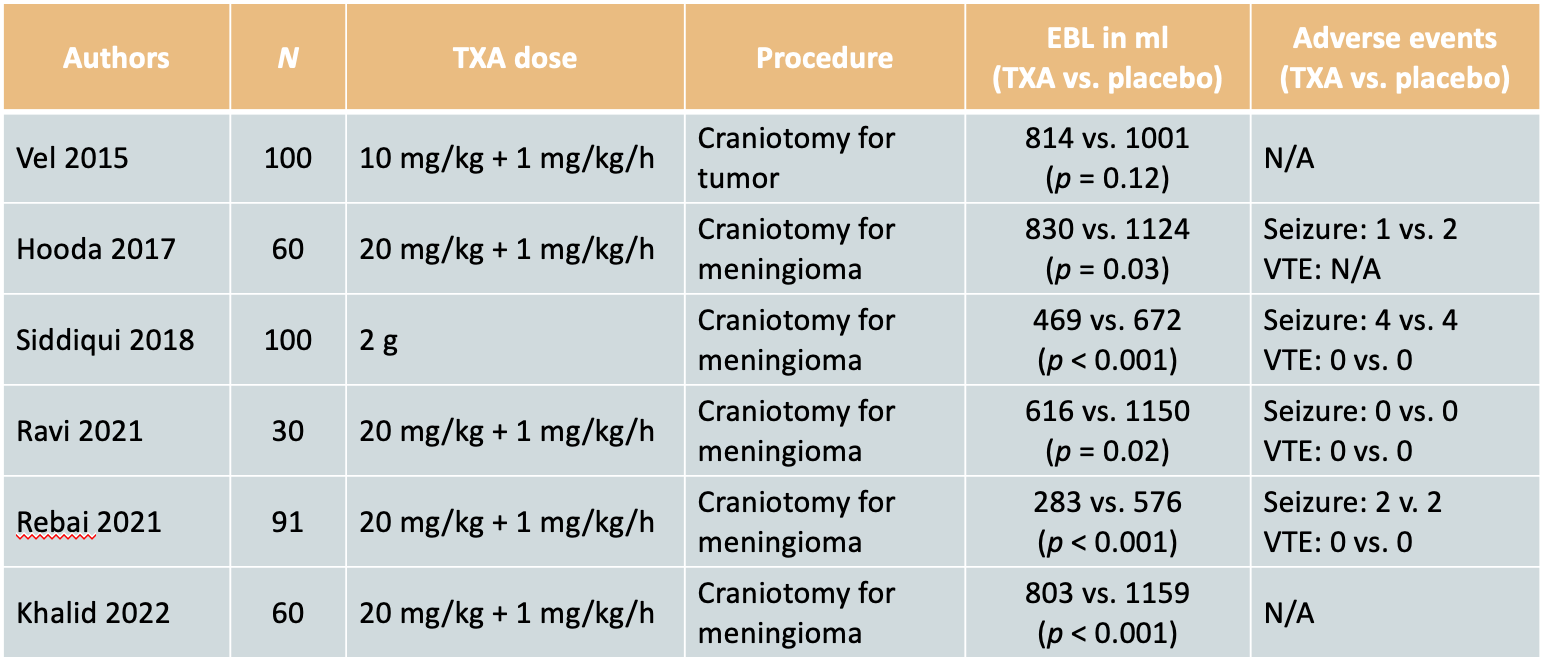
Table 1. Randomized controlled trials reporting the use of TXA in craniotomy for tumors.
CONCLUSIONS
- There are widely divergent indications for intraoperative TXA use in elective craniotomy throughout Canada.
- TXA appears to reduce the amount of blood loss, while its clinical significance remains unclear.
- Further studies are needed to inform the decision regarding intraoperative TXA use.
The Clinical Outcomes of Patients with Normal Pressure Hydrocephalus and Fecal Incontinence
BACKGROUND
Normal pressure hydrocephalus (NPH) is a brain disorder characterized by an abnormal aggregation of cerebrospinal fluid (CSF) in the ventricles of the brain. Individuals with NPH most often present with a combination of Hakim's triad, encompassing urinary incontinence, gait instability, and cognitive impairment. A less commonly known feature of NPH is fecal incontinence. The incidence and treatment of Normal Pressure Hydrocephalus (NPH) in adults have seen a notable rise, typically characterized by the clinical triad of dementia, gait disturbance, and urinary incontinence.
OBJECTIVES
(1) Investigate the prevalence of fecal incontinence in patients diagnosed with NPH
(2) Determine the effects of utilizing ventriculoperitoneal shunts as a treatment for NPH with fecal incontinence
(3) Describe patients who experienced fecal incontinence as a symptom of NPH, pre- and post-shunting.
METHODOLOGY
Case Series
A systematic review and surgical case series was conducted, involving consecutive adults diagnosed with NPH and treated with ventriculoperitoneal shunt (VPS) between September 2016 and September 2022.
Systematic Review
A systematic review following the PRISMA checklist was completed. Electronic searches were conducted on the following databases: PubMed, Ovid MEDLINE, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, and Web of Science. The search strategy employed a combination of keywords and MeSH terms, including "NPH" and "urgency."
A systematic review and surgical case series was conducted, involving consecutive adults diagnosed with NPH and treated with ventriculoperitoneal shunt (VPS) between September 2016 and September 2022.
Systematic Review
A systematic review following the PRISMA checklist was completed. Electronic searches were conducted on the following databases: PubMed, Ovid MEDLINE, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, and Web of Science. The search strategy employed a combination of keywords and MeSH terms, including "NPH" and "urgency."
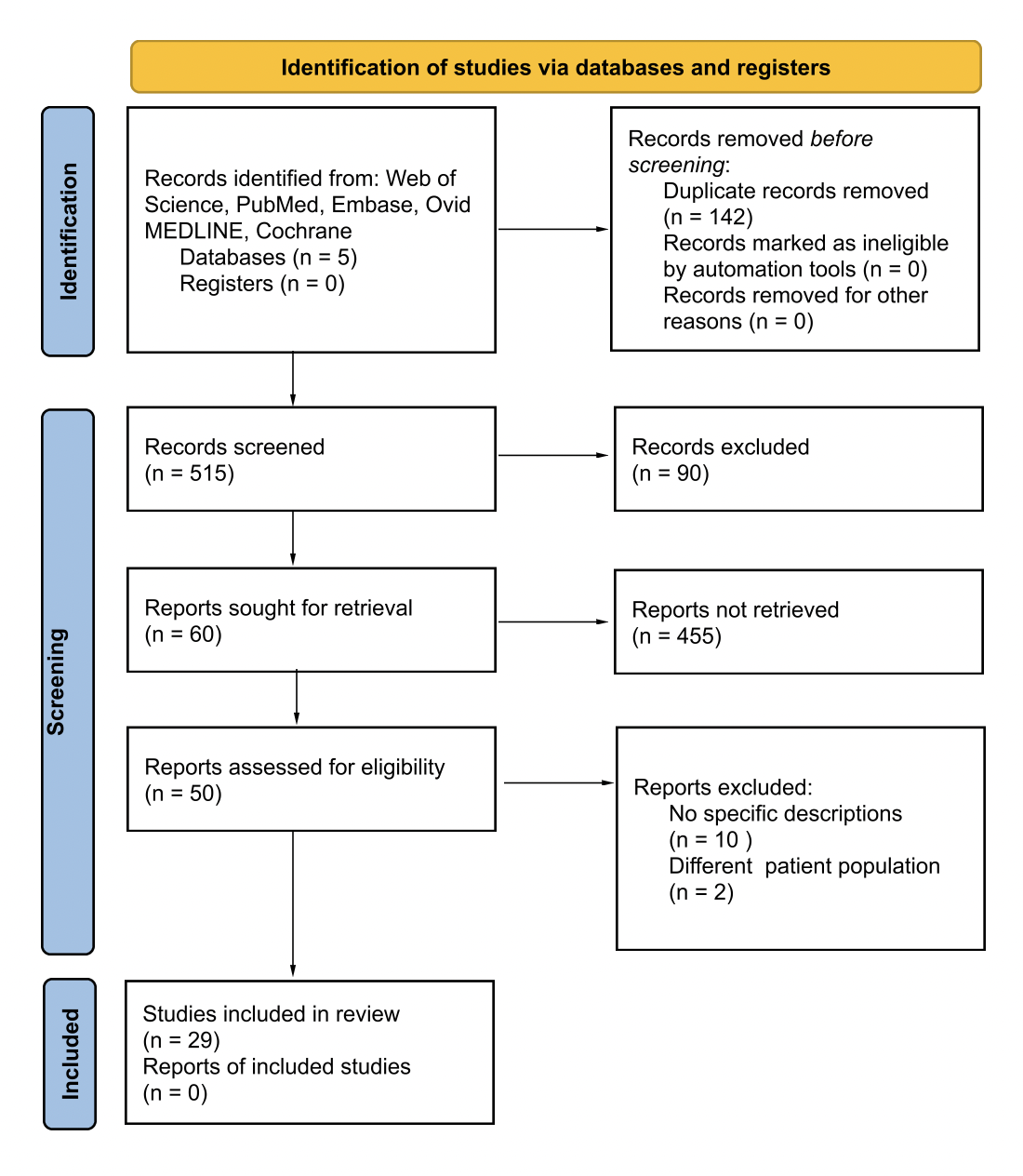
Figure 1. PRISMA flow diagram for systematic review, detailing the databases searched, abstracts screened, full-texts retrieved, and studies included in the review.
RESULTS
Systematic Review
The search for the systematic review was conducted in November 2024 across five electronic databases using keywords and MeSH terms, yielding 515 studies that were screened. Of these, 66 studies were sought for retrieval and 29 were included in review.
The search for the systematic review was conducted in November 2024 across five electronic databases using keywords and MeSH terms, yielding 515 studies that were screened. Of these, 66 studies were sought for retrieval and 29 were included in review.
Case Series
In the cohort of 85 patients, the median duration of NPH symptoms was 3.2 years. Gait and balance symptoms were prevalent in all patients, while cognitive, bladder, and bowel symptoms were observed in 85.9%, 91.8%, and 23.5% of cases. No significant differences were noted in age, sex, neurologic diseases presence, or lower gastrointestinal or pelvic pathology. The prevalence of fecal incontinence pre-surgery, within less than 3 months, and 3 months post-surgery were 23.5%, 32.9%, and 17.6%.
In the cohort of 85 patients, the median duration of NPH symptoms was 3.2 years. Gait and balance symptoms were prevalent in all patients, while cognitive, bladder, and bowel symptoms were observed in 85.9%, 91.8%, and 23.5% of cases. No significant differences were noted in age, sex, neurologic diseases presence, or lower gastrointestinal or pelvic pathology. The prevalence of fecal incontinence pre-surgery, within less than 3 months, and 3 months post-surgery were 23.5%, 32.9%, and 17.6%.
CONCLUSIONS
The study highlights the prevalence and treatment outcomes of fecal incontinence in patients with normal pressure hydrocephalus undergoing ventriculoperitoneal shunt surgery.
Preoperatively, 23.5% of patients experienced fecal incontinence. This temporarily increased post-surgery, but improved to 17.6% three months post-operation. The systematic review supports these findings, indicating that shunt surgery alleviates fecal incontinence in NPH patients. Identifying fecal incontinence as a possible symptom of NPH is vital for comprehensive patient care.
These results demonstrate the importance of surgical interventions to optimize patient outcomes. Future research should explore the mechanisms and long-term effects of treament on fecal incontinence in NPH patients.
Preoperatively, 23.5% of patients experienced fecal incontinence. This temporarily increased post-surgery, but improved to 17.6% three months post-operation. The systematic review supports these findings, indicating that shunt surgery alleviates fecal incontinence in NPH patients. Identifying fecal incontinence as a possible symptom of NPH is vital for comprehensive patient care.
These results demonstrate the importance of surgical interventions to optimize patient outcomes. Future research should explore the mechanisms and long-term effects of treament on fecal incontinence in NPH patients.
BIBLIOGRAPHY AND ACKNOWLEDGEMENTS
We would like to express our gratitude to Colin Galvin, Ben Phan, Elise Atkinson, Mary Beth Anketell, Tina Kapur, and Alexandra Golby from the Brigham and Women's Hospital for their invaluable contributions to this study. Their expertise and support were instrumental in the successful completion of this research.
The use of intraoperative magnetic resonance imaging for endoscopic transnasal transsphenoid surgery in children

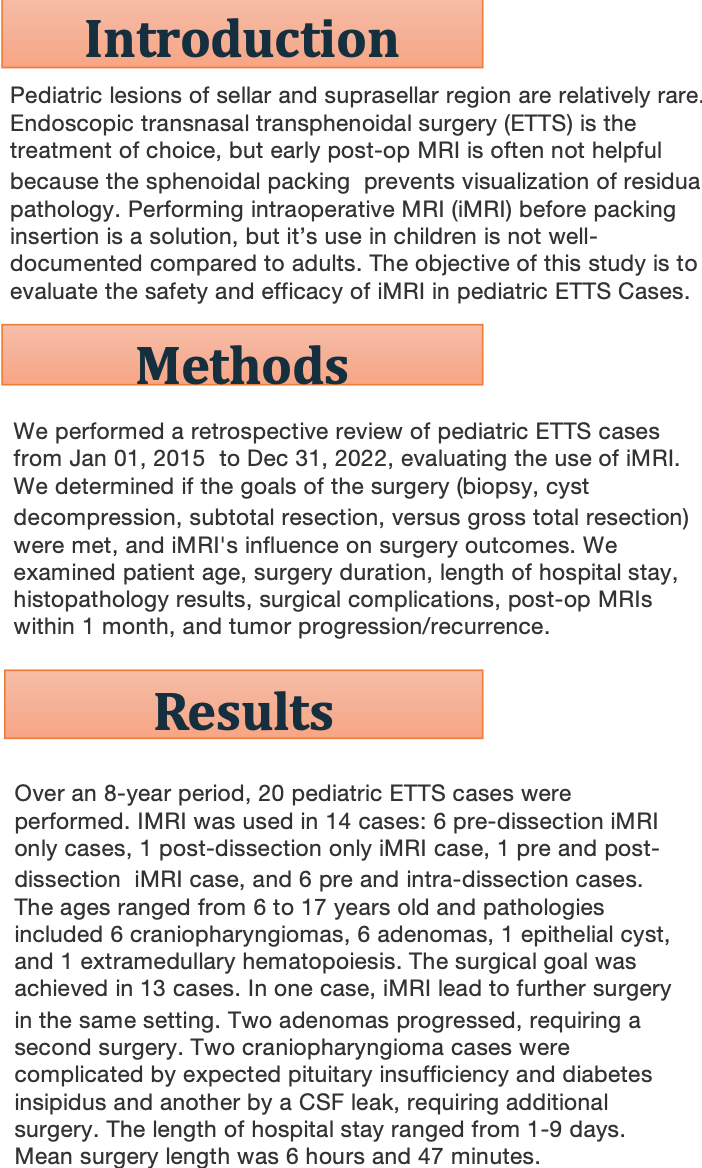
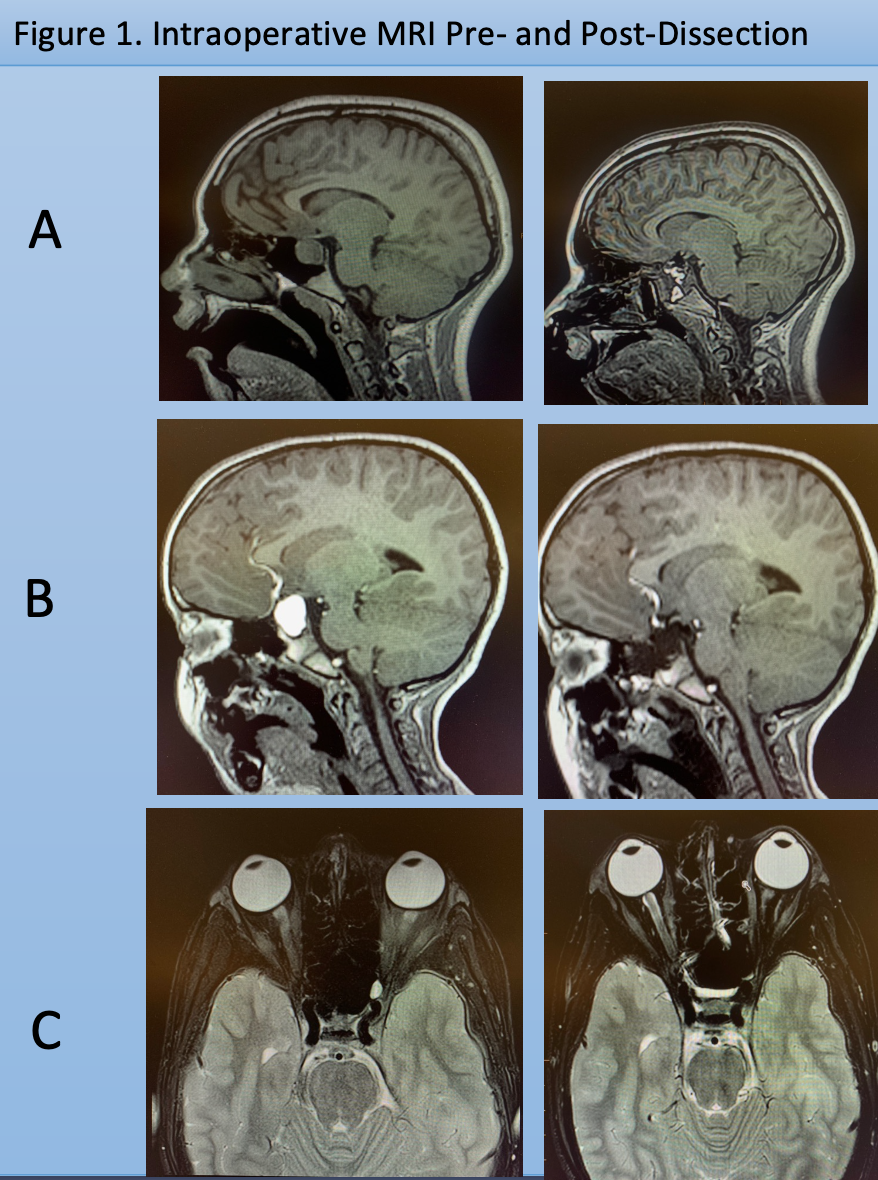
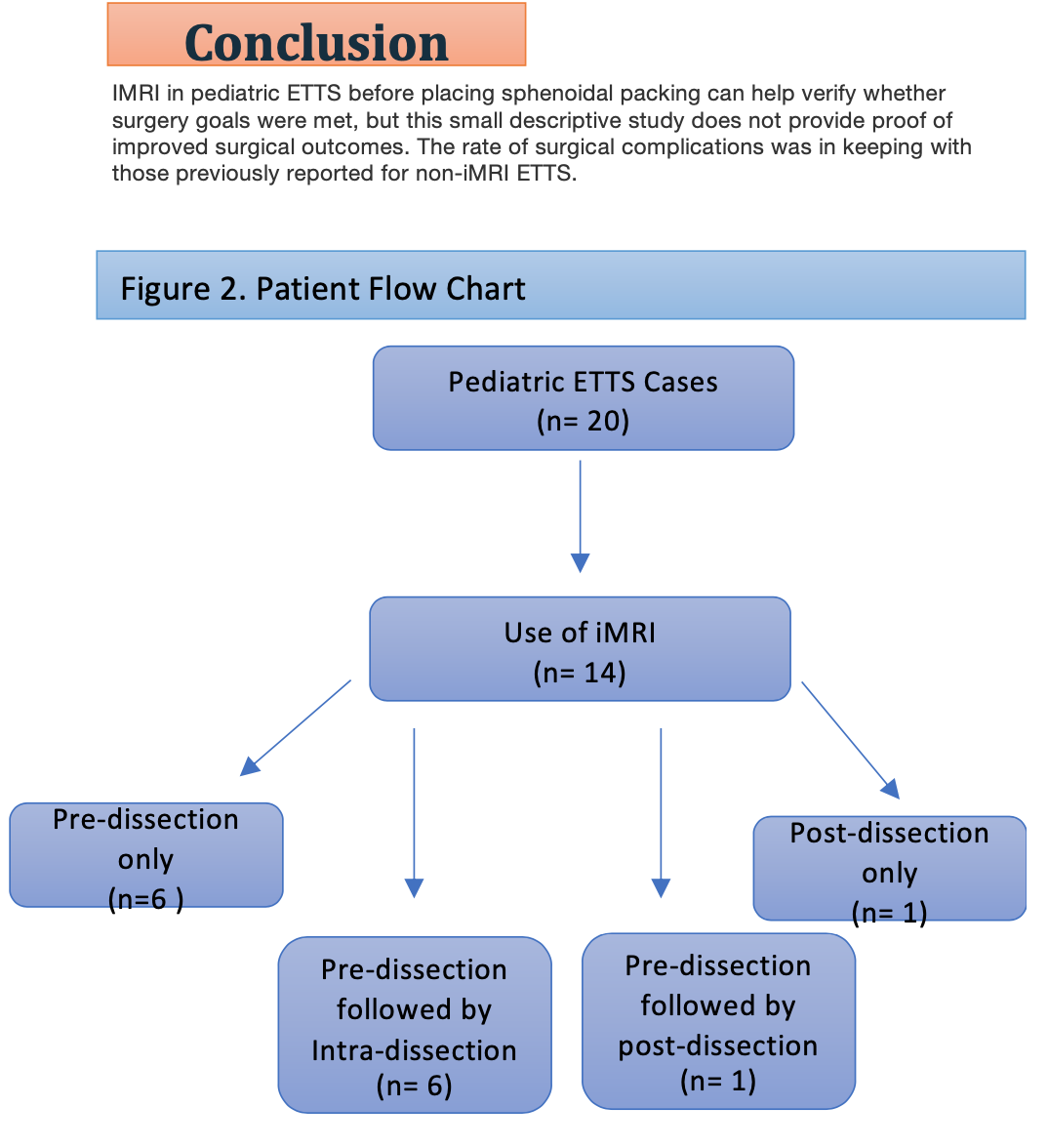
Automated pituitary adenoma segmentation for radiosurgery with deep learning-based model
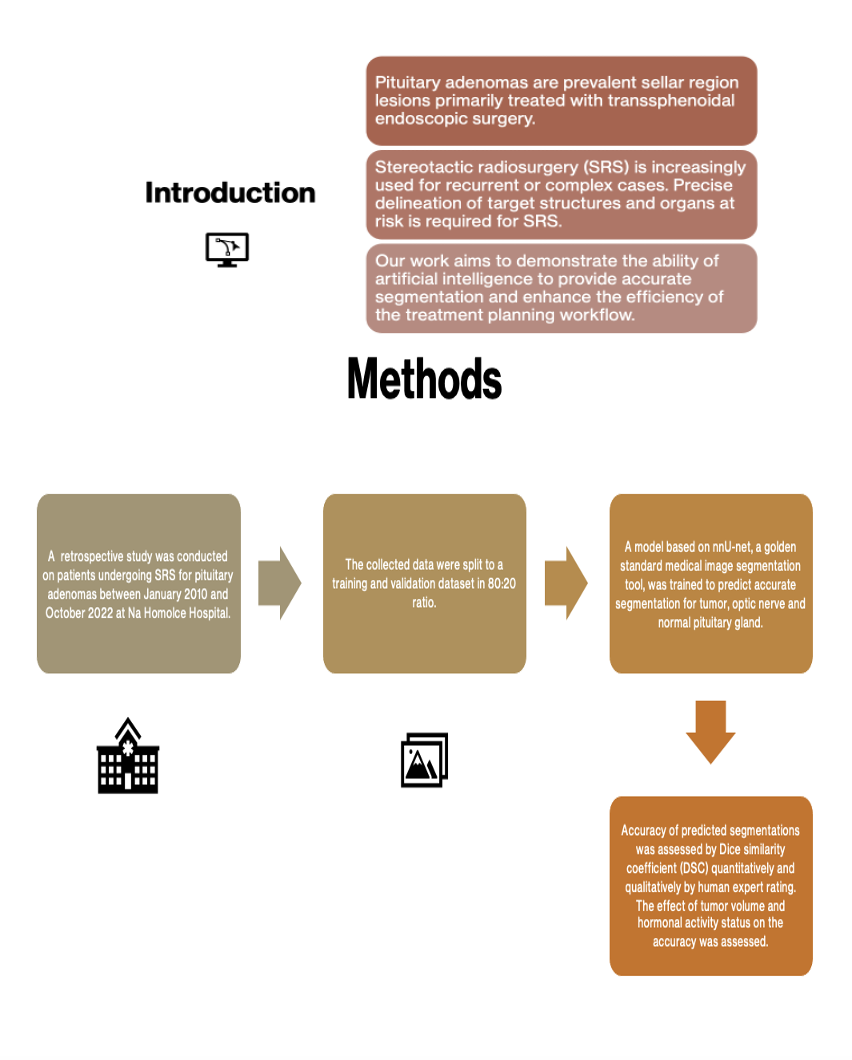
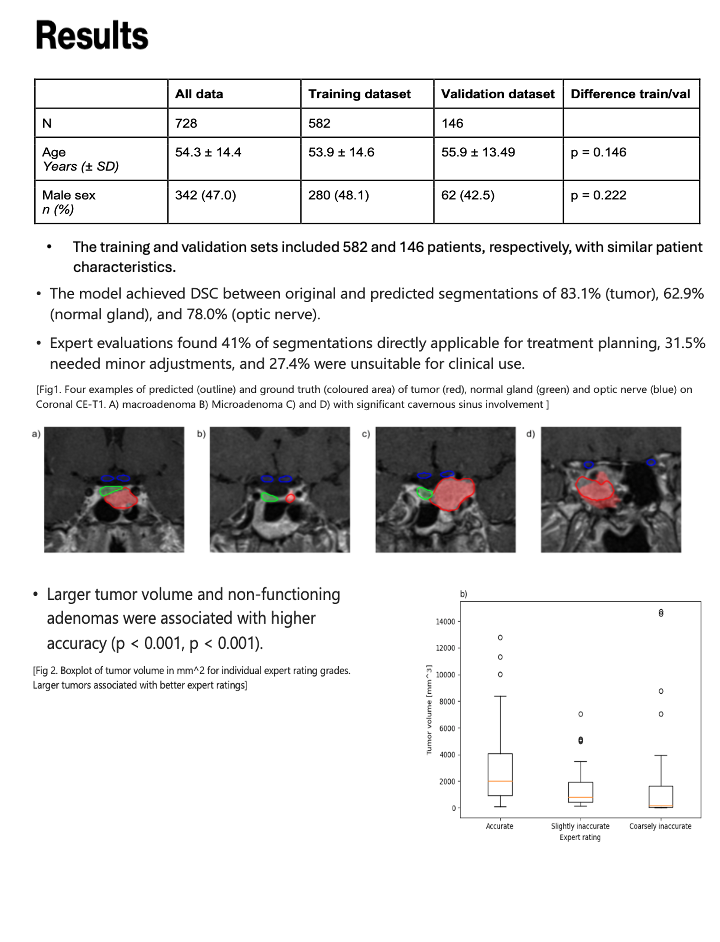
Safety of same-day discharge following incidental durotomy in tubular microdiscectomy: a retrospective cohort study
INTRODUCTION
Incidental durotomy and cerebrospinal fluid leak (CSF leak) is a common complication following lumbar microdiscectomy, with an incidence of 5.5%-9% of primary lumbar spine surgeries. The risk increases to 13.2%-21% with subsequent revision surgeries (1). In one study, open microdiscectomy had two times the risk of CSF leak compared to minimally invasive microdiscectomy (MIM) (1). In that same study, patients with CSF leak after open microdiscectomy were also more likely to require subsequent surgical repair (open = 25%, MIM = 0%, P < .01) (1). Management of incidental durotomy generally includes intraoperative repair followed by a period of bedrest to allow for healing of the injury to the thecal sac without the added hydrostatic pressure conferred by an upright posture.
In MIM, the integrity of the surrounding muscles remains uncompromised, minimizing the potential for CSF accumulation in dead spaces. By maintaining muscle integrity and addressing CSF leaks during surgery, the likelihood of symptomatic postoperative CSF leaks is reduced (1). As such, it is common practice to discharge patients home the same day after surgical repair of CSF leak that occurs during MIM, but not open microdiscectomy. However, there are no published reports that specifically address the safety and long-term outcomes of this practice.
OBJECTIVE
The objective of this retrospective cohort study was to evaluate outcomes in patients with CSF leak after MIM, comparing those admitted to hospital for bedrest versus same-day discharge. Our hypothesis was that patients with CSF leak after MIM may be safely discharged home the same day.
METHOD
- Retrospective cohort study using a prospectively generated database.
- Consecutive patients who underwent minimally invasive tubular microdiscectomy by a single surgeon at the Royal University Hospital in Saskatoon, Saskatchewan from January 1, 2009 to August 31, 2023 were reviewed, and those with an intraoperative dural tear or CSF leak were included.
- Two cohorts: hospital admission vs. same day discharge.
- Patient data was collected based on operative notes, discharge summaries, and follow-up notes.
- The primary outcomes were postoperative CSF leak symptoms, patients presenting to the emergency department or clinic with CSF leak symptoms, and any revision surgery related to the CSF leak.
RESULTS

Figure 1: Summary of Patients Included
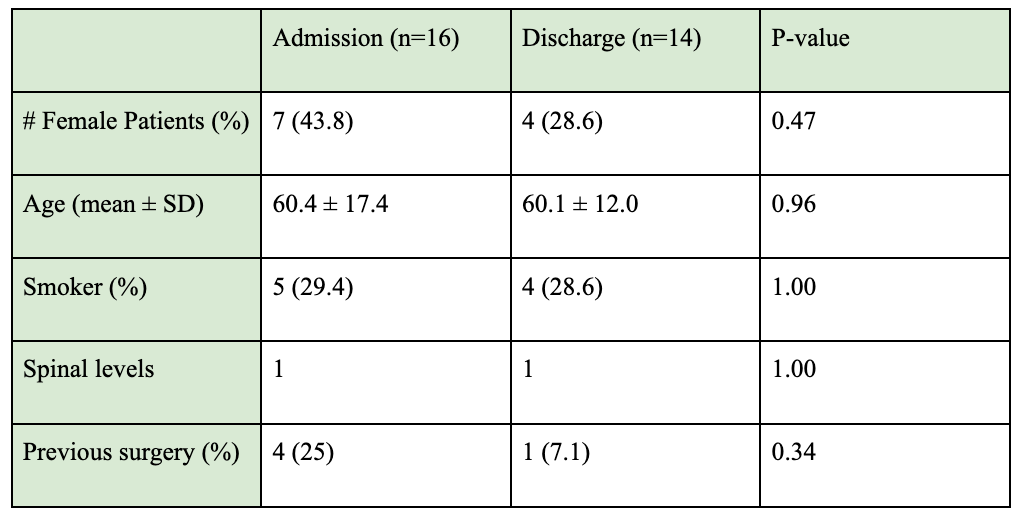
Table 1: Demographic information of included patients.
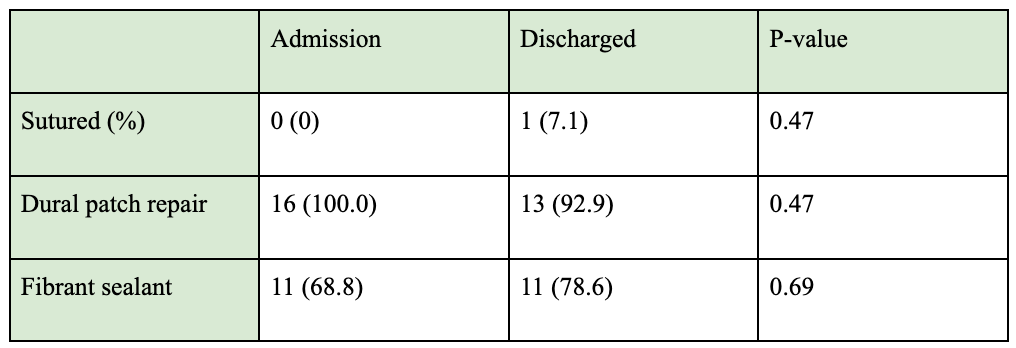
Table 2: Intraoperative duraplasty techniques and materials.
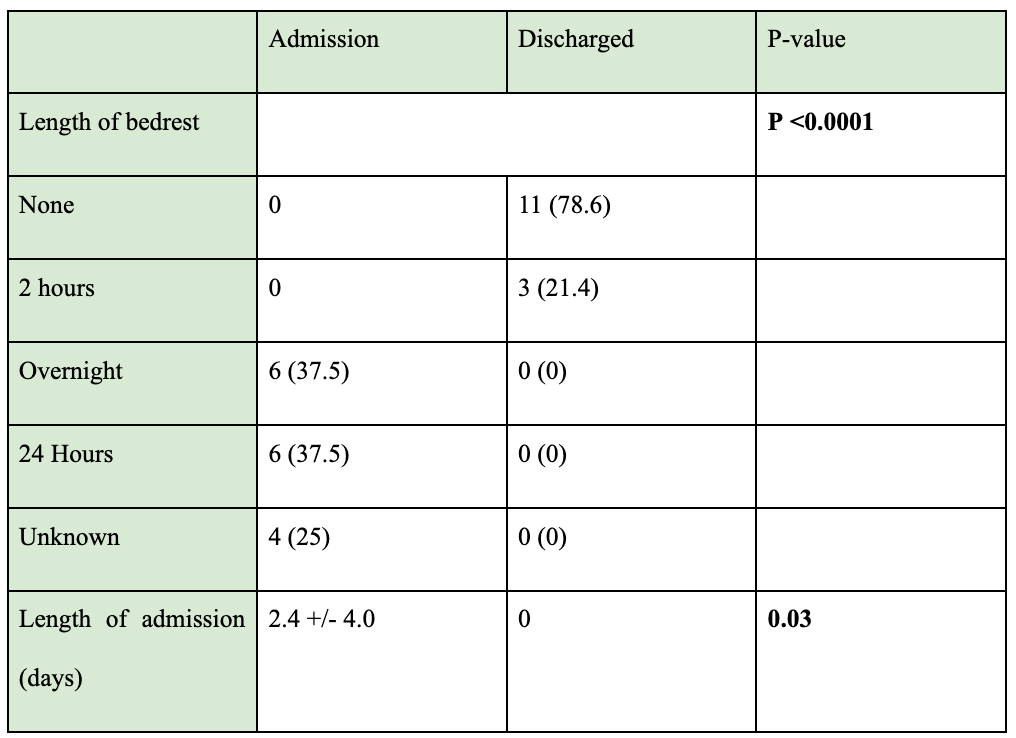
Table 3: Postoperative management of CSF Leaks.
CONCLUSION
Early postoperative mobilization and same-day discharge following minimally invasive microdiscectomy is safe.
Limitations
- Retrospective study
- Small sample size
REFERENCES
-
Wong AP, Shih P, Smith TR, Slimack NP, Dahdaleh NS, Aoun SG, El Ahmadieh TY, Smith ZA, Scheer JK, Koski TR, Liu JC. Comparison of symptomatic cerebral spinal fluid leak between patients undergoing minimally invasive versus open lumbar foraminotomy, discectomy, or laminectomy. World neurosurgery. 2014 Mar 1;81(3-4):634-40.
Comparative analysis of spinal cord-derived and induced pluripotent-derived neural stem & progenitor cells for SCI therapy

Introduction
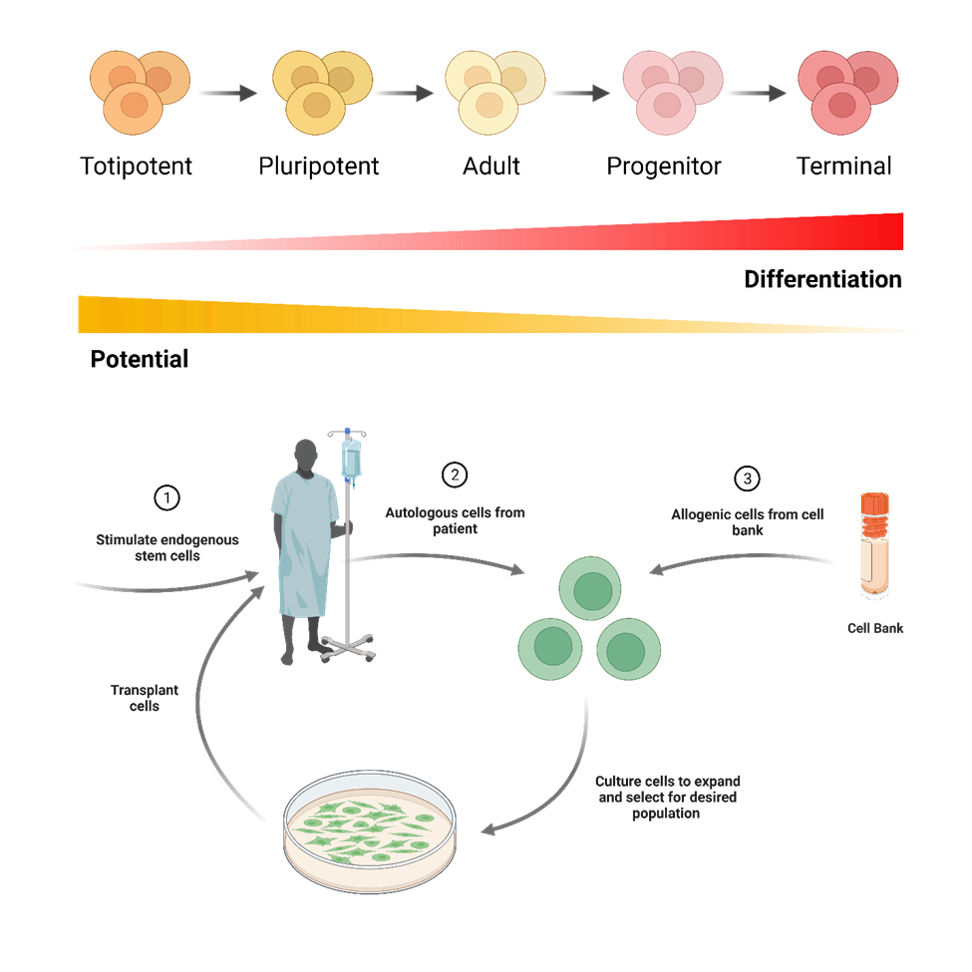
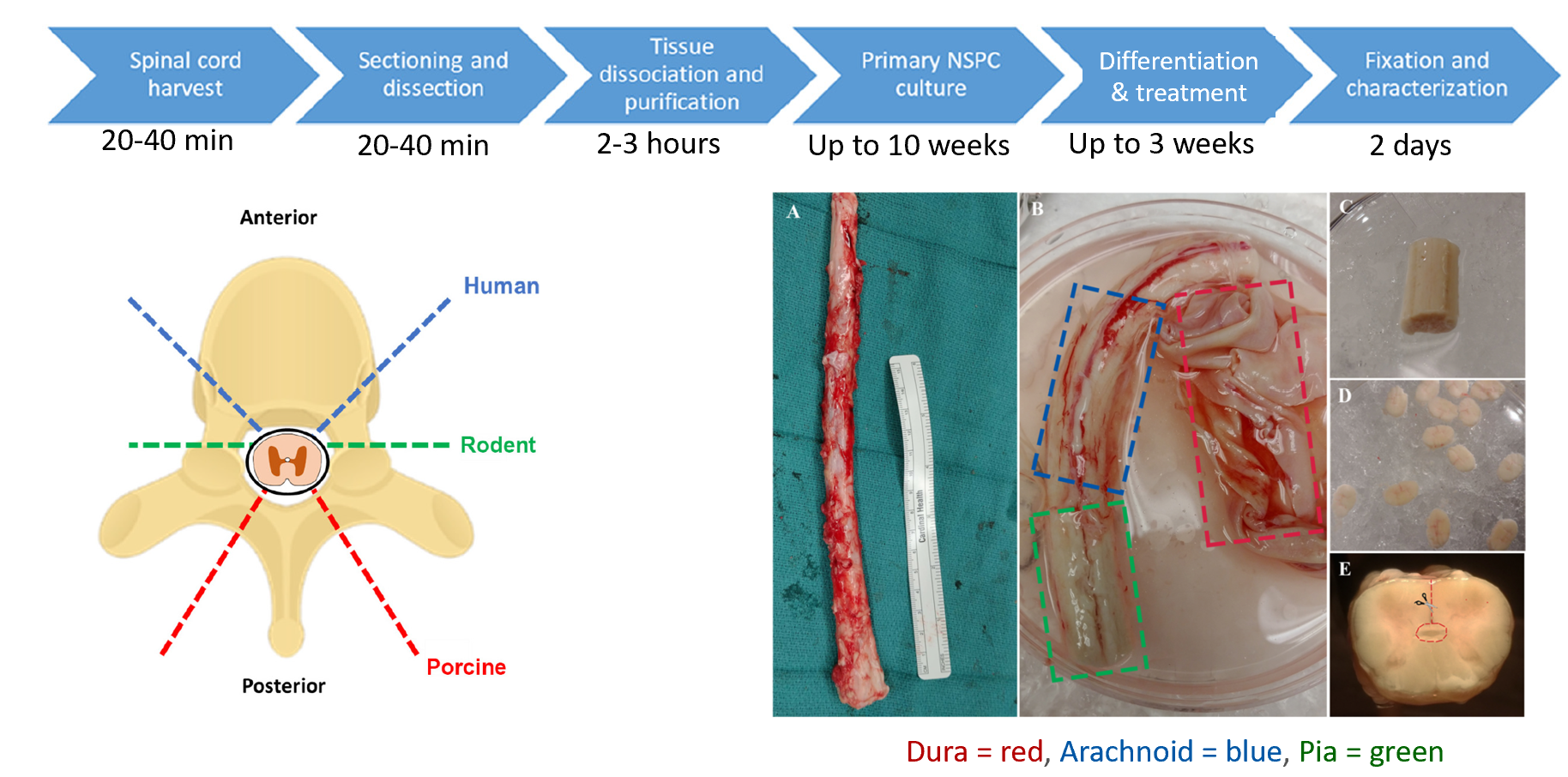

Results
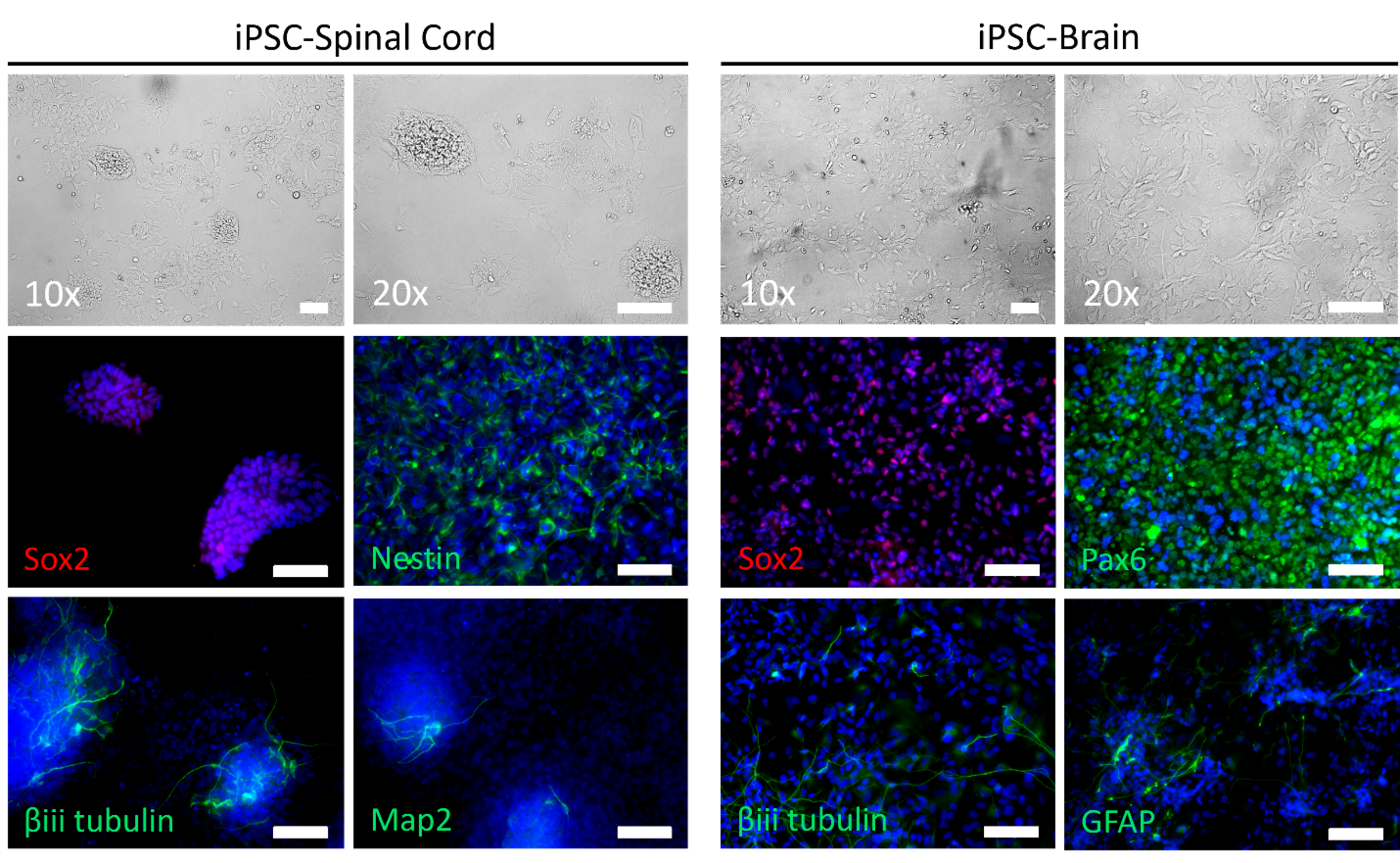
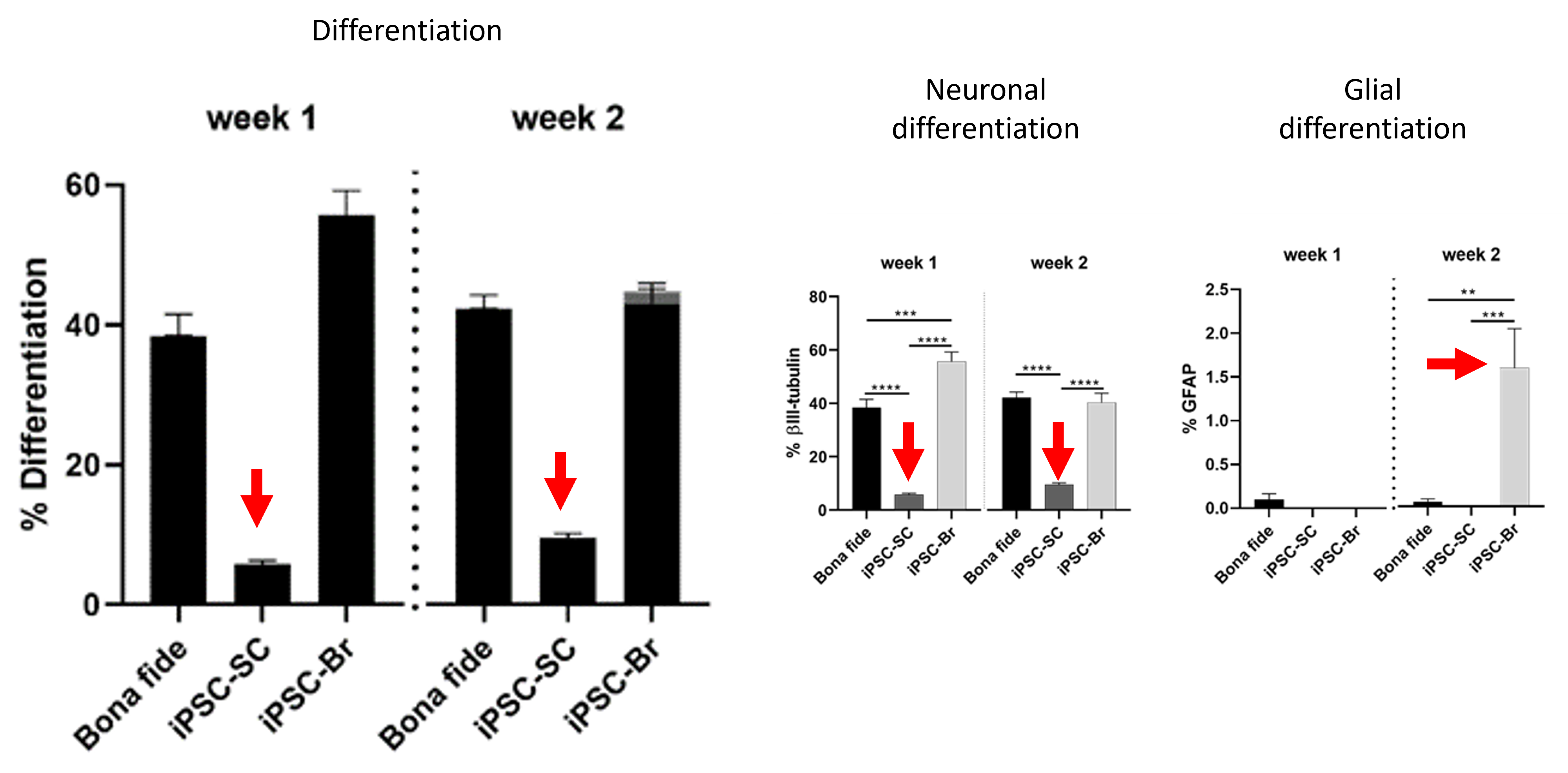

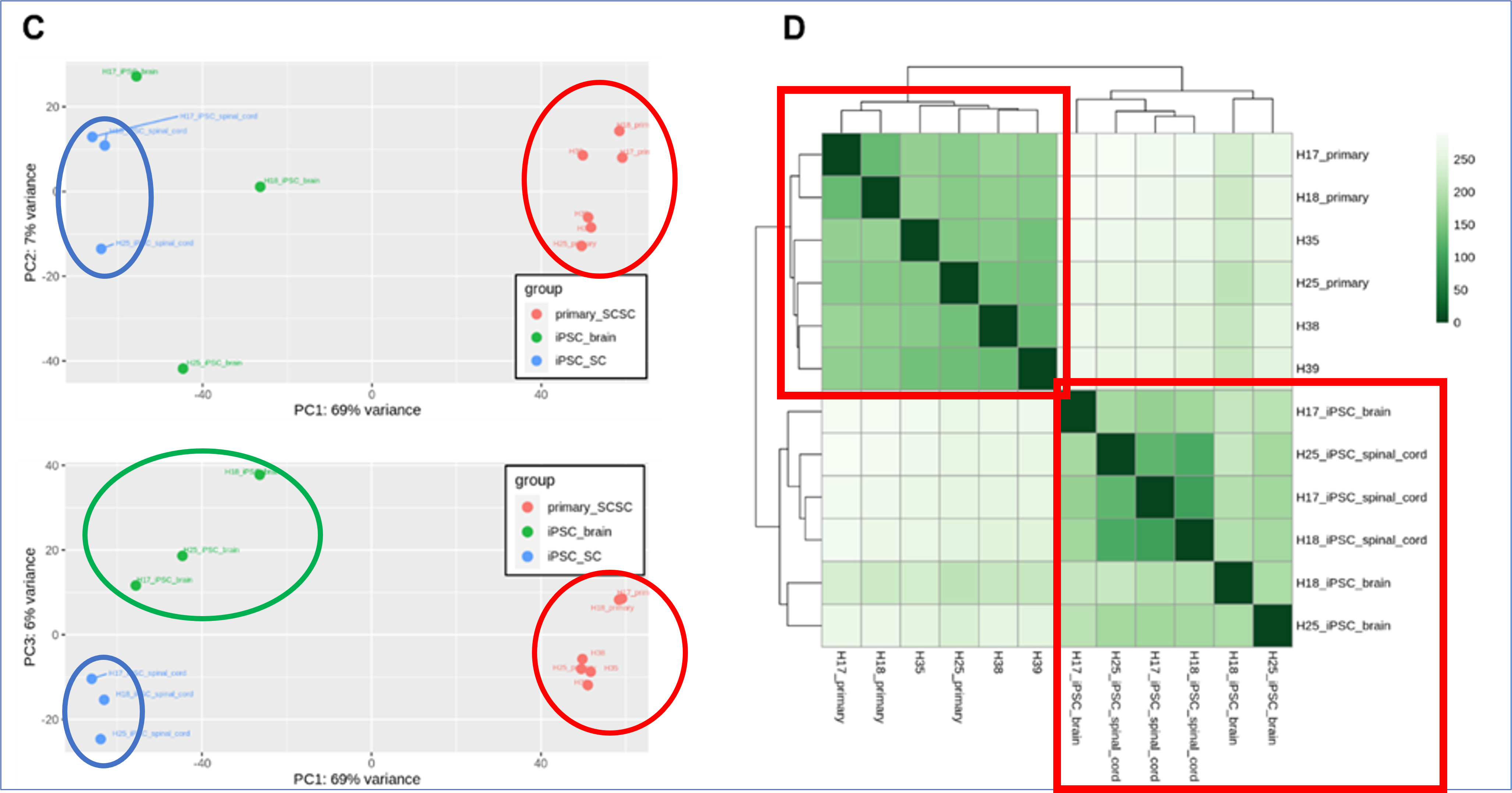
Conclusion
- Spinal cord iPSCs, brain iPSCs, and endogenous spine neural stem cells are far different from each other
- Poses an obstacle for translating using iPSCs or endogenous stem cells in treating spinal cord injury
- Collaboration with basic scientists can help advance understanding of human spinal cord stem cells
The growing problem of spine surgery wait times in British Columbia: longitudinal trends and impacts on perioperative outcomes

Background
• Lumbar degenerative spine disease is common with incidence of 4.5% annually in Canada (Ravindra et al., 2018).
• Long surgical wait times are of growing concern across all surgical specialties (Canadian Institute for Health Information).
• In 2016, Bailey et al. showed that patients who received degenerative spine surgery within 12 months reported greater improvement on Oswestry Disability Index than those who waited >12 months.
Objectives
1. Investigate whether wait times for elective degenerative spine surgery have increased annually between 2009-2020 at Vancouver General Hospital.
2. Investigate whether increasing wait times are associated with increased rates of adverse events (AE), duration of hospitalization, and increased likelihood of discharge to a facility other than home.
Methods
• Prospectively enrolled 10,824 patients who underwent elective degenerative spine surgery at Vancouver General Hospital between Jan 1, 2009, and Dec 31, 2020.
• Wait Time Intervals - T1, Ti, T2, T1+ T2, Total wait time (T1+Ti+T3)
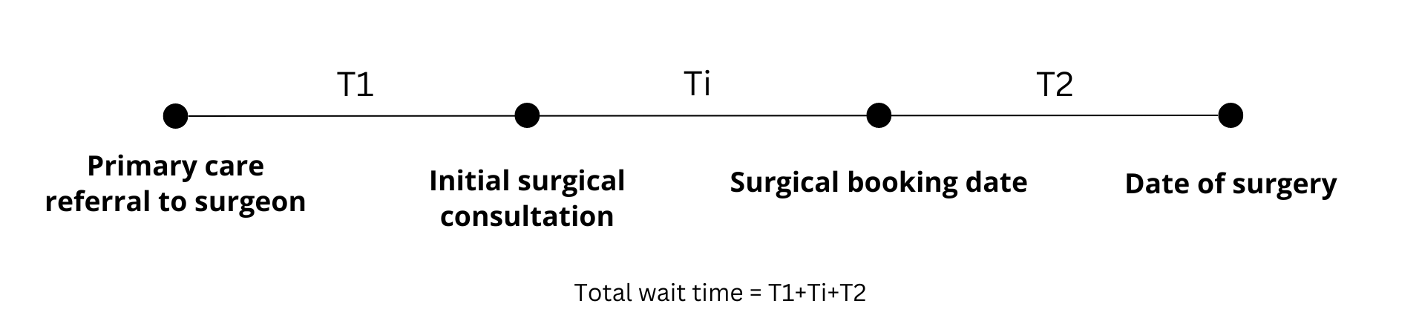
• Spinal Adverse Events Severity System, version 2 (SAVES-V2)
• Length of hospitalization (days)
• Disposition (home vs. other hospital, nursing home, rehab, LTC)
Results
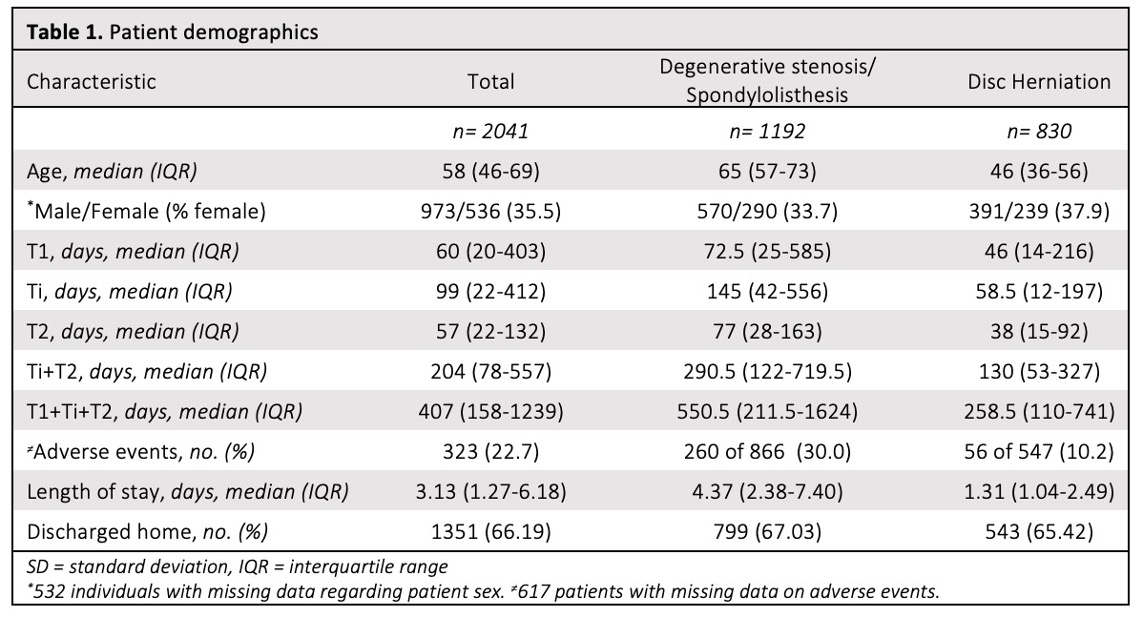
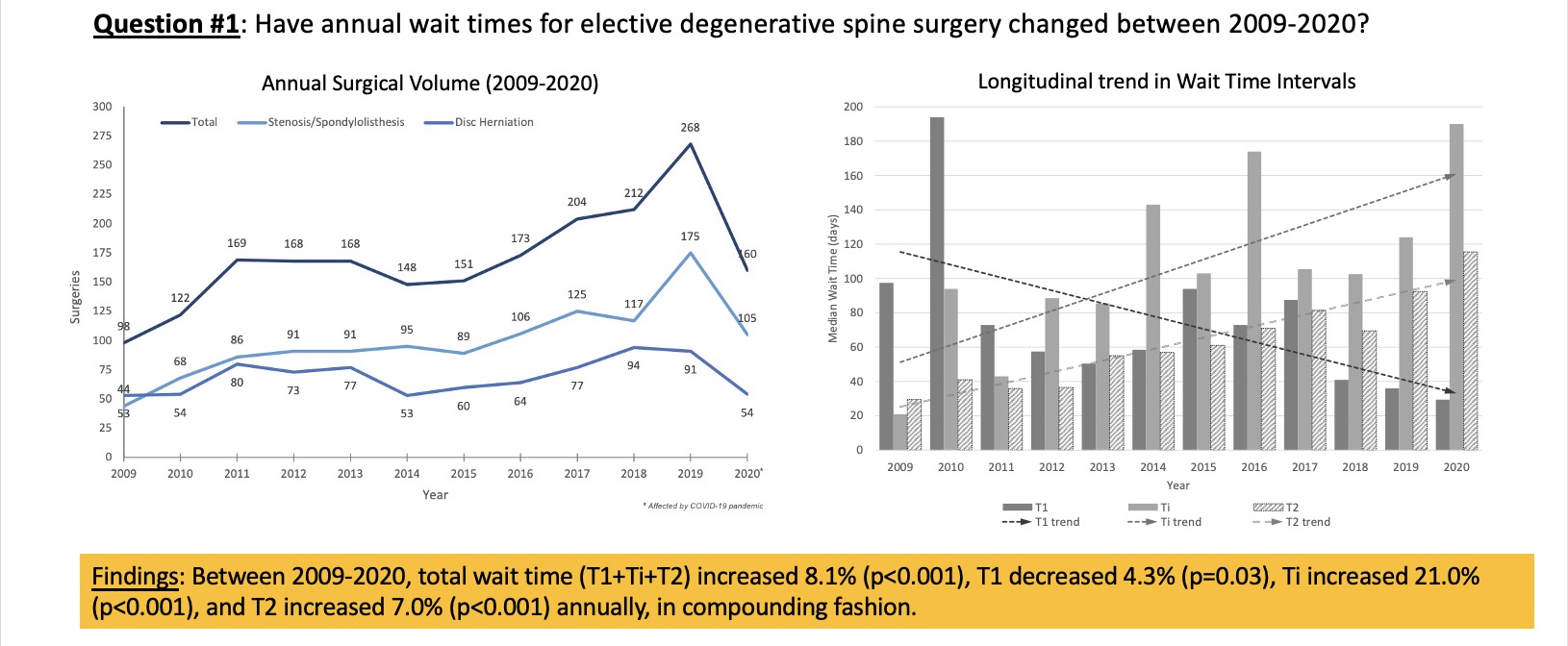
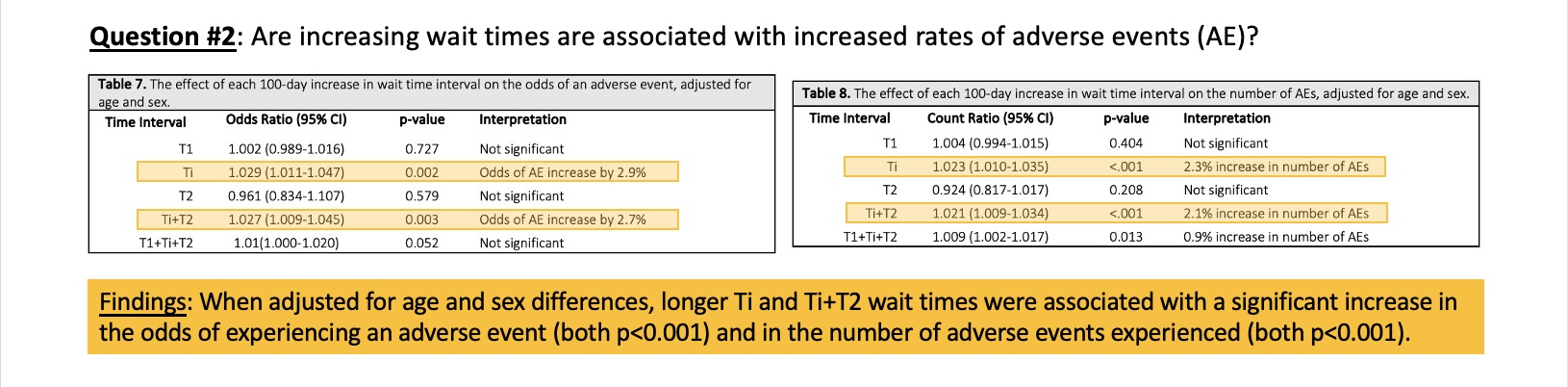
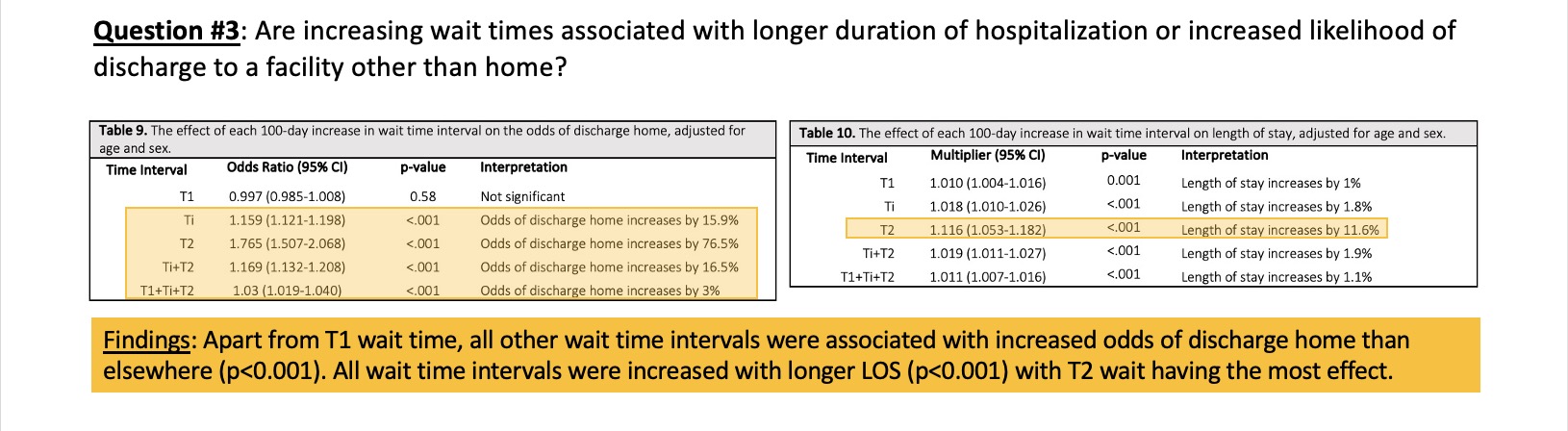
Discussion
Evolution of Wait times between 2009-2020
• Our study shows an 8.1% increase in total wait time annually in compounding fashion (p<0.001).
• The wait time interval with the largest increase is between surgical consultation and surgical booking date (Ti), at 21.0% annually (p<0.001).
This may be due to a growing elderly population with degenerative spine disease and with system delays in obtaining relevant neuroimaging, including outpatient CT and MRI.
Wait times and Adverse Events
• Increases in Ti wait time are significantly associated with 2.9% increased odds of experiencing an AE (p=0.002) and 2.3% increase in the actual number of AEs experienced (p<0.001).
Further studies needed to investigate factors that contribute to delays between surgical consultation and surgery booking date to mitigate effects of delayed care on perioperative AEs – i.e., pre-operative comorbidities that require time for medical optimization.
Wait times and Disposition
• Apart from T1, increased wait times (Ti & T2) are associated with significantly increased odds of discharge home (p<0.001).
Possibly a reverse effect – patients who are less symptomatic or more independent at home are more likely to undergo alternative treatments before surgery is decided and booked, and may tolerate waiting longer before actual date of surgery, and are therefore more likely to return to home in the first place.
Wait times and Length of Stay
• All increases in wait time intervals were associated with significantly increased LOS (p=0.001 for T1 and p<0.001 for Ti and T2), though T2 had the largest multiplier with 11.6% increase in LOS for every 100-day increase in T2.
Efforts to optimize hospitalization costs should target reduction in wait time interval between booking referral and date of surgery as a preoperative measure to reduce patient’s length of stay.
• Our study shows an 8.1% increase in total wait time annually in compounding fashion (p<0.001).
• The wait time interval with the largest increase is between surgical consultation and surgical booking date (Ti), at 21.0% annually (p<0.001).
This may be due to a growing elderly population with degenerative spine disease and with system delays in obtaining relevant neuroimaging, including outpatient CT and MRI.
Wait times and Adverse Events
• Increases in Ti wait time are significantly associated with 2.9% increased odds of experiencing an AE (p=0.002) and 2.3% increase in the actual number of AEs experienced (p<0.001).
Further studies needed to investigate factors that contribute to delays between surgical consultation and surgery booking date to mitigate effects of delayed care on perioperative AEs – i.e., pre-operative comorbidities that require time for medical optimization.
Wait times and Disposition
• Apart from T1, increased wait times (Ti & T2) are associated with significantly increased odds of discharge home (p<0.001).
Possibly a reverse effect – patients who are less symptomatic or more independent at home are more likely to undergo alternative treatments before surgery is decided and booked, and may tolerate waiting longer before actual date of surgery, and are therefore more likely to return to home in the first place.
Wait times and Length of Stay
• All increases in wait time intervals were associated with significantly increased LOS (p=0.001 for T1 and p<0.001 for Ti and T2), though T2 had the largest multiplier with 11.6% increase in LOS for every 100-day increase in T2.
Efforts to optimize hospitalization costs should target reduction in wait time interval between booking referral and date of surgery as a preoperative measure to reduce patient’s length of stay.
Conclusions & Limitations

Consult and Kyphoplasty Delay Impacts on Geriatric Vertebral Compression Fracture Outcomes

Introduction
- Vertebral Compression Fracture (VCF) Overview: Result from spinal vertebral body collapse due to causes like osteoporosis, trauma, or malignancy.
- Clinical Presentation: Includes acute back pain, height loss, deformity, and mobility impairments.
- Impact: Significant morbidity, mortality, and decreased quality of life, with substantial economic burden.
- Age Correlation: Increasing age linked to higher VCF incidence, often due to risk factors like osteoporosis and diabetes.
- Diagnosis Challenges: Around 25-33% of VCFs diagnosed clinically, requiring further imaging and leading to treatment delays.
- Management: Ranges from conservative treatment to surgery, with kyphoplasty showing significant pain relief and functional improvement.
Study Objective
We aimed to determine the association between the delay in a neurosurgical consultation and subsequent kyphoplasty following the radiological diagnosis of a VCF, and surgical outcomes.
Methods
- Ethics: Approval obtained from Hamilton Integrated Research Ethics Board; the need for patient consent was waived.
- Population: Elderly patients (60+) undergoing kyphoplasty at Hamilton Health Sciences (HHS) from Jan 1st, 2012 to Dec 31st, 2022.
- Exclusion criteria: Patients who had not been admitted to HHS under Internal Medicine or other non-spine-surgical specialties within two years prior to their surgery.
- Data: Collected demographics, admitting diagnosis, dates of non-surgical admission, time from diagnosis to consult/kyphoplasty, vertebral height, and focal kyphotic deformity measurements.
- Outcomes: Assessed changes in vertebral height loss and focal kyphotic deformity at various timepoints.
- Analysis: Conducted univariate and multivariate analyses to evaluate correlations between potential determinants and outcome measures.
Radiological Imaging Analysis
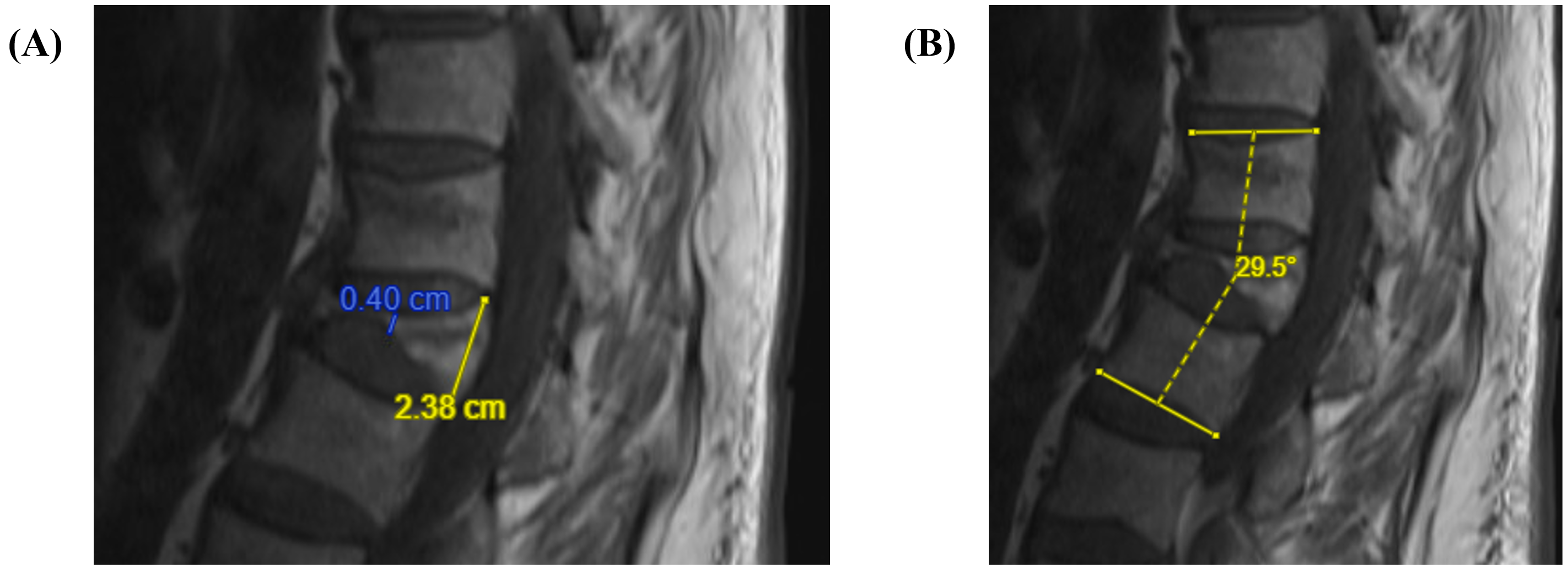
Figure 1: (A) Calculation of the vertebral height loss as the difference between the maximum and minimum height of the vertebra, divided by the maximum height. In this example, it would be (2.38-0.40)/2.38 for a vertebral height loss of 83%. (B) Calculation of the focal kyphotic deformity as the Cobb angle between the superior endplate of the cephalad unaffected vertebra, and the inferior endplate of the caudad unaffected vertebra.
Funding
This research received no specific funding from any public, commercial, or non-for-profit funding agency.
Results
Baseline Characteristics of the Study Population
| Characteristics | |
| Age in years – mean (SD) | 70.5 (8.04) |
| Female sex – n (%) | 58 (52.1%) |
| Thoracic vertebral fracture – n (%) | 60 (55.6%) |
| Lumbar vertebral fracture – n (%) | 76 (70.4%) |
| Number diagnosed at non-surgical admission – n (%) | 44 (40.7%) |
| Time from diagnosis to surgical consult (days) – mean (SD) (n = 119) | 133.2 (225.0) |
| Time from diagnosis to kyphoplasty (days) – mean (SD) (n = 119) | 169.1 (236.0) |
| Time from surgical consult to kyphoplasty (days) – mean (SD) (n = 119) | 35.8 (49.1) |
Primary Outcomes
| Outcomes | |
| Change in focal kyphotic deformity (Degrees) | |
| Diagnosis to pre-kyphoplasty – mean (SD) (n = 41) | 2.19 (8.44) |
| Pre-kyphoplasty to post-kyphoplasty – mean (SD) (n = 38) | 0.06 (5.21) |
| Diagnosis to post-kyphoplasty – mean (SD) (n = 42) | 2.26 (9.31) |
| Change in Vertebral height loss (%) | |
| Diagnosis to pre-kyphoplasty – mean (SD) (n = 58) | 8.45 (14.29)**** |
| Pre-kyphoplasty to post-kyphoplasty – mean (SD) (n = 53) | -6.81 (19.09)* |
| Diagnosis to post-kyphoplasty – mean (SD) (n = 61) | 2.14 (21.99) |
Primary Outcome Correlations
| Effect on Primary Outcomes | Adjusted correlation coefficient (R2) | p-Value |
| Time from diagnosis to surgical consult | ||
| Change in focal kyphotic deformity | ||
| Diagnosis to pre-kyphoplasty (n = 41) | -0.05 | 0.68 |
| Pre-kyphoplasty to post-kyphoplasty (n = 38) | -0.14 | 0.98 |
| Diagnosis to post-kyphoplasty (n = 42) | -0.02 | 0.68 |
| Change in vertebral height loss | ||
| Diagnosis to pre-kyphoplasty (n = 58) | -0.05 | 0.67 |
| Pre-kyphoplasty to post-kyphoplasty (n = 53) | -0.11 | 0.96 |
| Diagnosis to post-kyphoplasty (n = 61) | -0.07 | 0.82 |
| Effect on Primary Outcomes | Adjusted correlation coefficient (R2) | p-Value |
| Time from diagnosis to kyphoplasty | ||
| Change in focal kyphotic deformity | ||
| Diagnosis to pre-kyphoplasty (n = 41) | -0.06 | 0.70 |
| Pre-kyphoplasty to post-kyphoplasty (n = 38) | -0.15 | 0.99 |
| Diagnosis to post-kyphoplasty (n = 42) | -0.08 | 0.86 |
| Change in vertebral height loss | ||
| Diagnosis to pre-kyphoplasty (n = 58) | -0.05 | 0.69 |
| Pre-kyphoplasty to post-kyphoplasty (n = 53) | -0.11 | 0.97 |
| Diagnosis to post-kyphoplasty (n = 61) | -0.07 | 0.86 |
Conclusion
- Retrospective study on elderly VCF patients: analyzed impact of time to kyphoplasty on outcomes.
- Average wait from consult to kyphoplasty is 35.8 days.
- Primary delay is from diagnosis to neurosurgical consult.
- Early kyphoplasty associated with improved outcomes, but no significant correlation between time to treatment and radiographic outcomes.
- Study suggests treatment window for VCFs may be larger than thought; balance needed between early access to kyphoplasty and resource allocation.
- Study limitations: observational nature, single-center, lack of pain scores and functional outcomes documentation.
- Future research should include multicenter trials with broader outcome measures and long-term follow-up data.
Conflict of Interest
The authors declare no competing interests.
Effect of postoperative pain control on length of stay after elective spine surgery
INTRODUCTION
- Prolonged length of stay (LOS) after elective spine surgery increases risk for in-hospital complications and contributes significantly to healthcare costs
- Previous studies have focused on preoperative risk factors for increased LOS
- Impact of pain and other modifiable risk factors on LOS has not been rigorously studied
OBJECTIVE
In patients undergoing elective spine surgery, is poor postoperative pain control in the first 24-hours following surgery a predictor for length of stay?
METHODS
- Patients prospectively and consecutively enrolled, 2014-2017, Foothills Medical Center, Calgary, AB, Canada
-
Inclusion criteria:
- Adults undergoing elective cervical or thoracolumbar spine surgery
- Overnight hospital admission
- At least one documented pain score in first 24-hours postoperatively
-
Primary outcome: in-hospital LOS after surgery
- Extended LOS defined as ≥75th percentile = 5 days
-
Independent variables:
- Poor postoperative pain control, defined as mean Numeric Rating Scale (NRS) pain score >4 in first 24-hours postoperatively
- Other variables known to influence LOS
- Analysis: univariable and multivariable logistic regression
RESULTS
- 1305 eligible patients
- Mean age 60.1 years, 51.9% female
- Mean LOS = 4.38 days (standard deviation 8.18)
- 56.9% had poor postoperative pain control
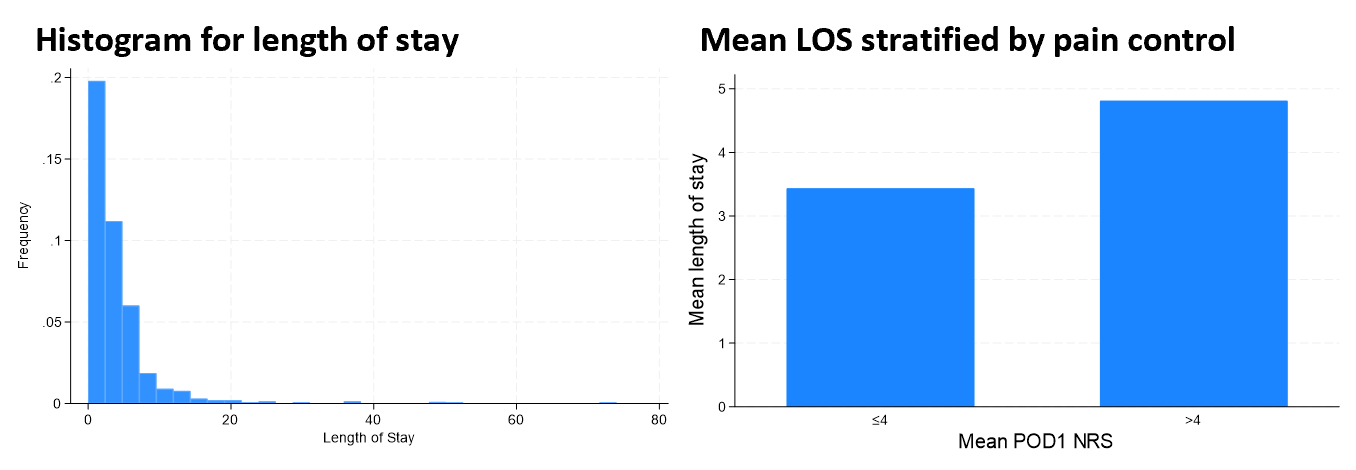
Variables Used in Analysis
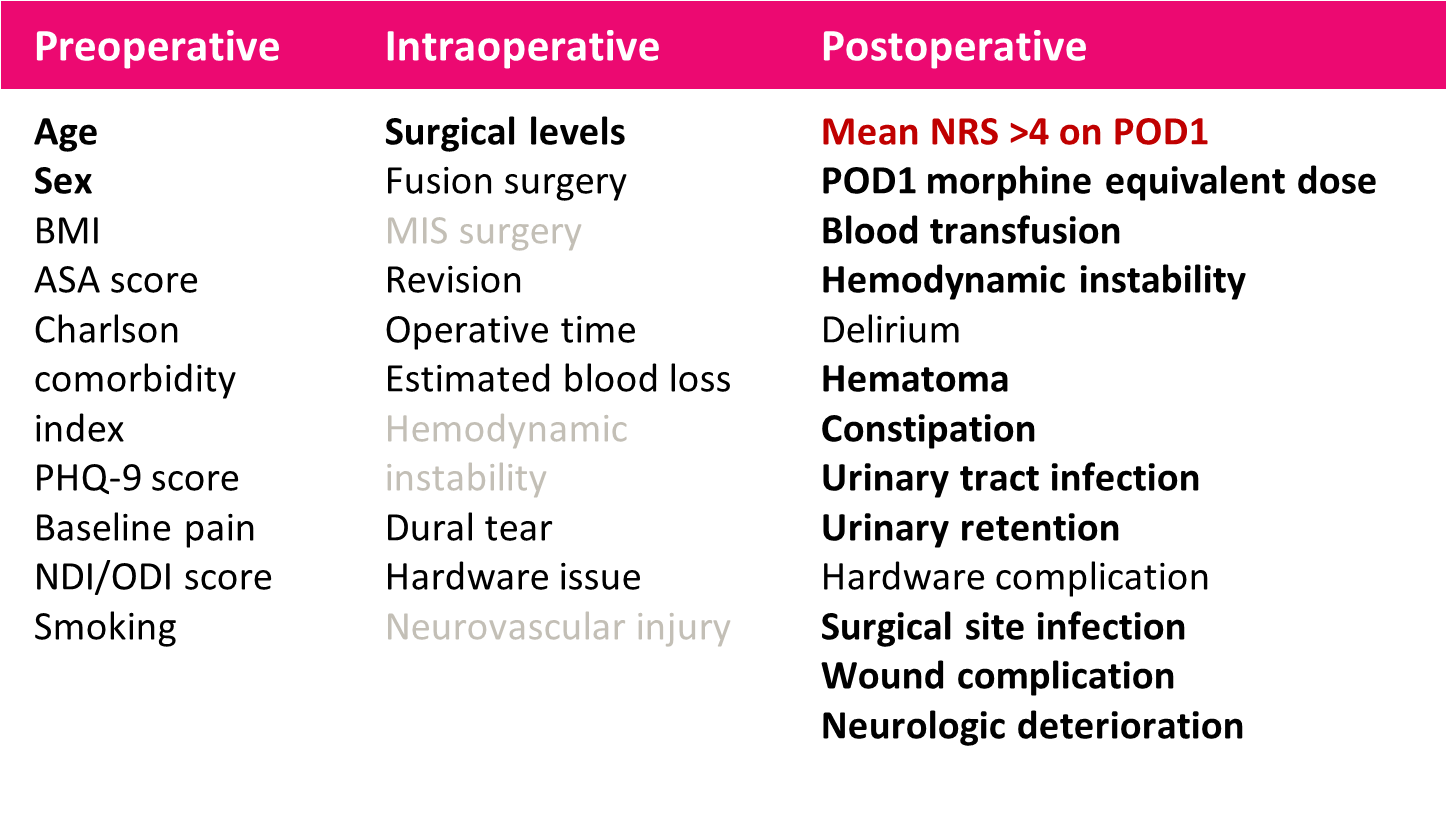
1. Variables with p >0.2 excluded after univariable analysis
2. Remaining variables included in multivariable analysis
3. Variables with p <0.05 included in final model
2. Remaining variables included in multivariable analysis
3. Variables with p <0.05 included in final model
Final Multivariable Model
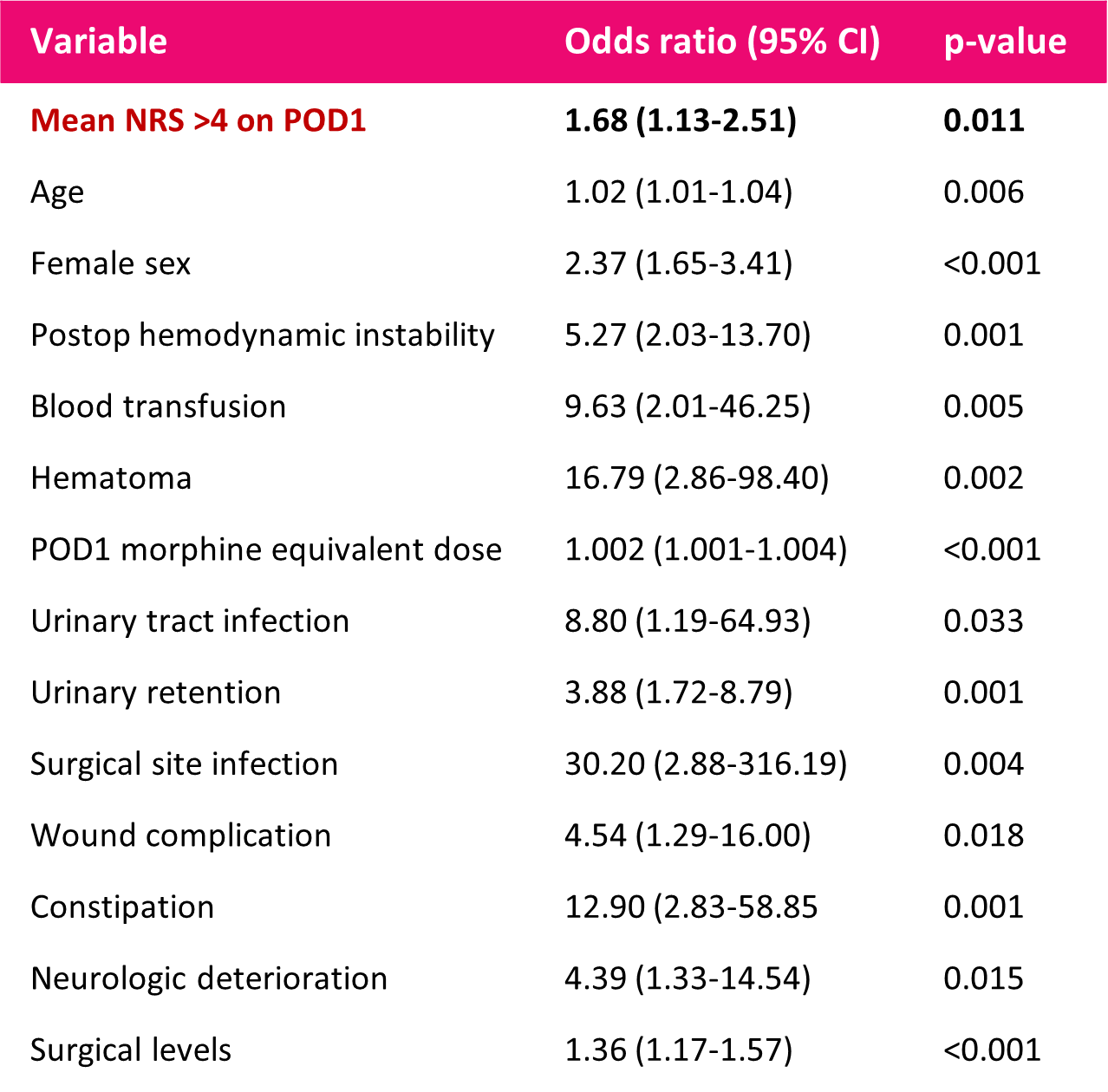
CONCLUSION
- Poor pain control on day 1 after elective spine surgery is independently associated with increased LOS after adjusting for known risk factors
- Multiple modifiable perioperative risk factors contribute to increased LOS
-
Strategies to improve perioperative pain management
- ERAS (enhanced recovery after surgery) protocols
- Preoperative risk stratification
A critical appraisal of the application of frailty and sarcopenia in the spinal oncology population
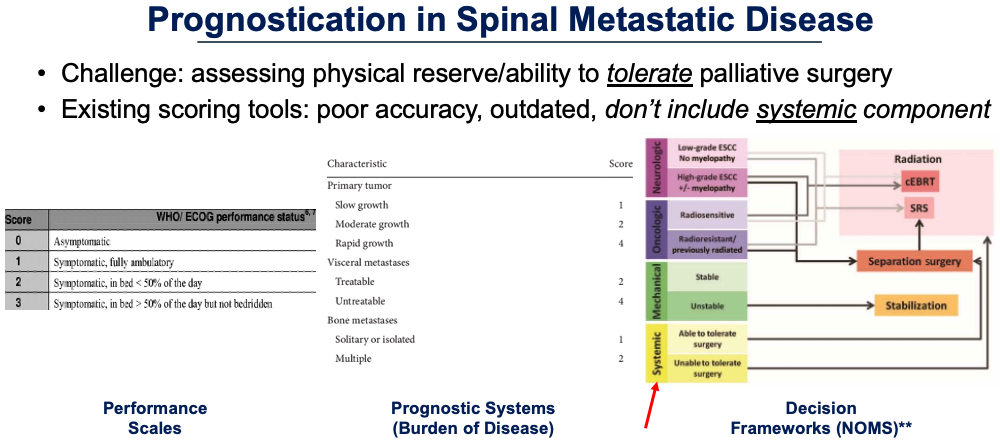
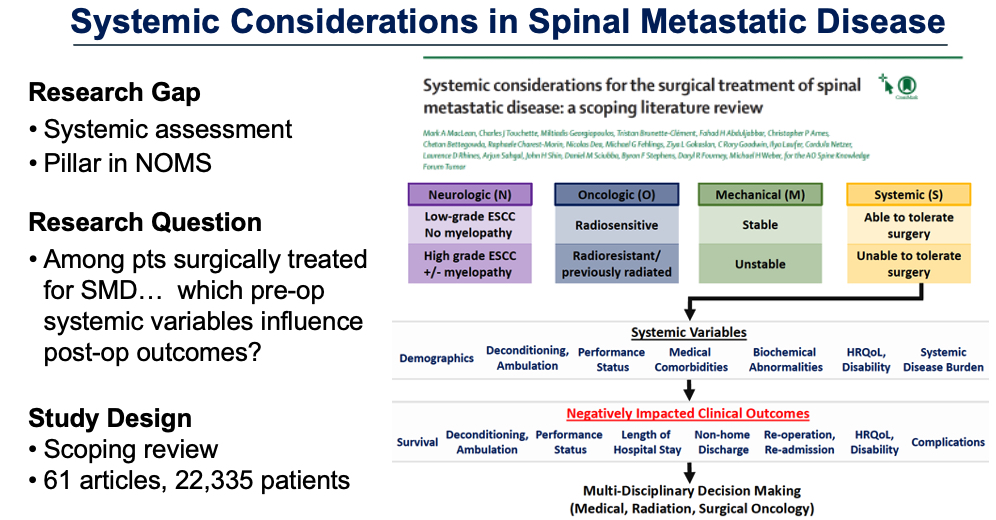
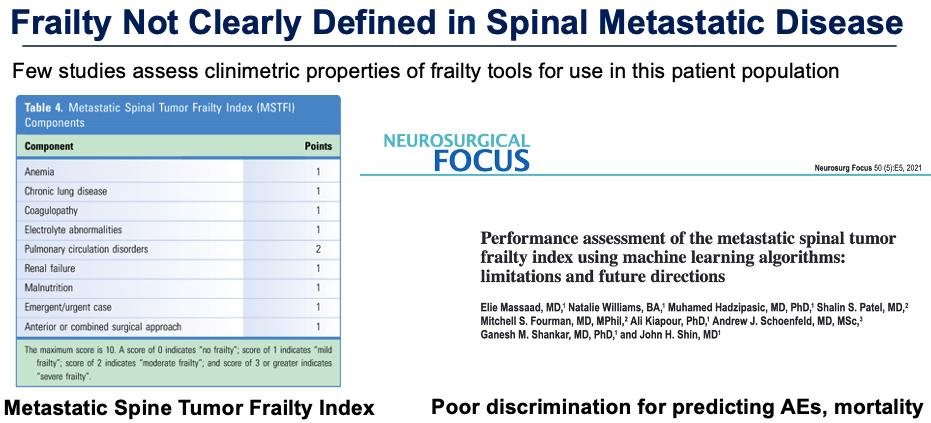

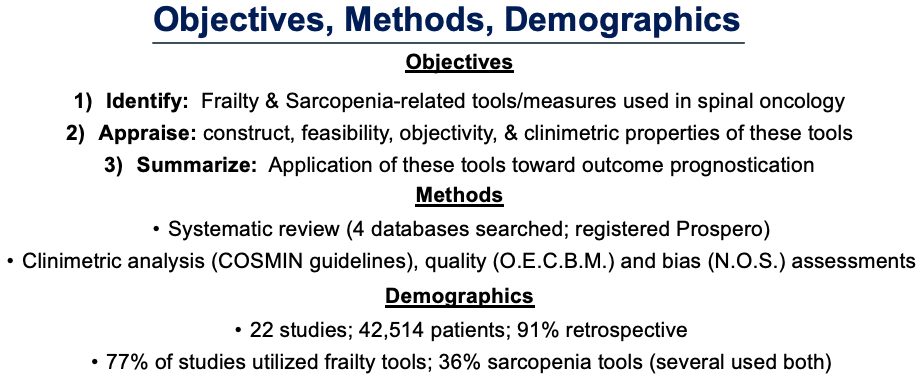
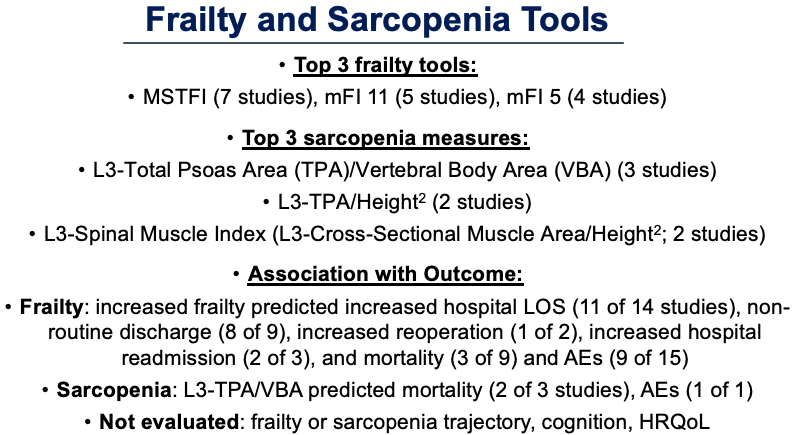
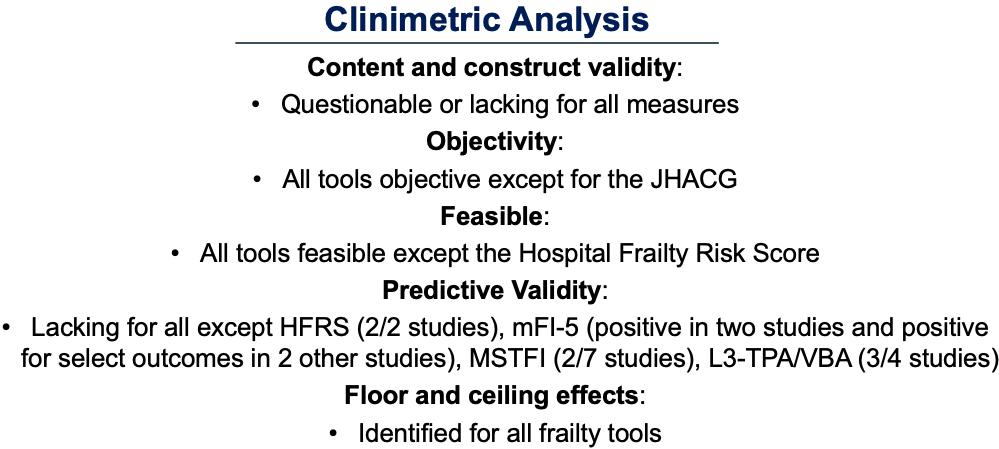
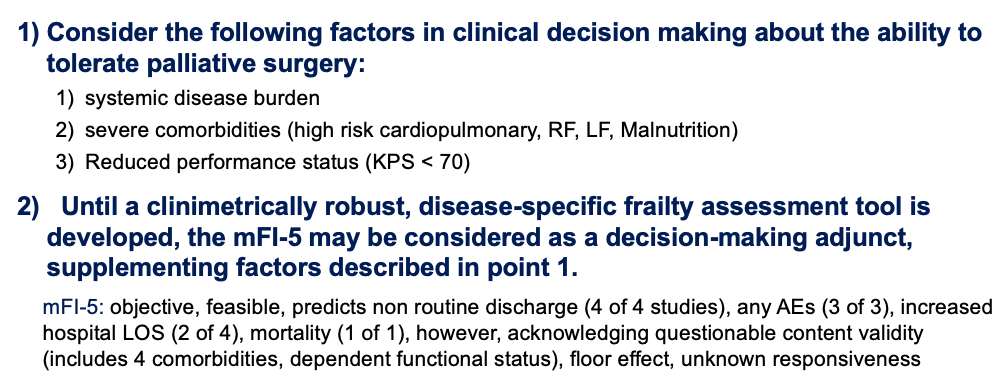
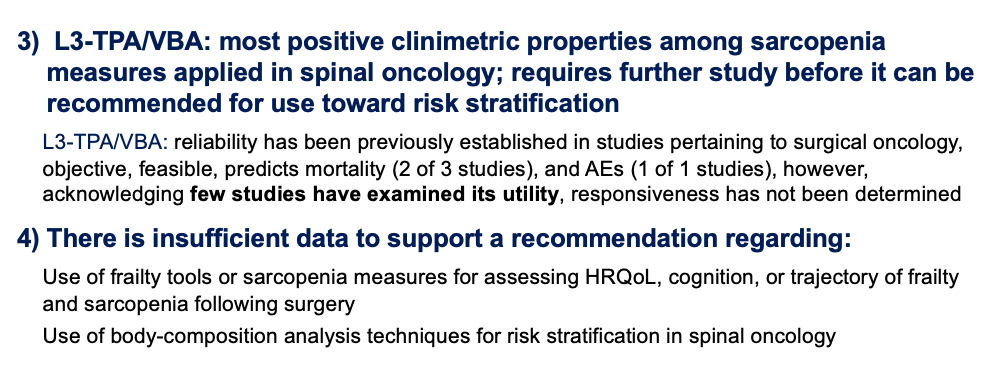
In-vivo Accuracy of Pedicle Screws Utilizing a Supervisory Controlled 7DOF Robot with OCT Guidance
Background
Pedicle screw fixation is an important technique in the armamentarium of neurosurgeons to provide stability to the spine. Violation of the pedicle can lead to neurovascular injury, with possibility of morbidity and mortality.
Early techniques relied on anatomic localization and orientation. Freehand breach rates are reported as high as 31% (1). To reduce the risk of a pedicle breach fluoroscopy, and later optical based guidance with fluoroscopy or CT scan has been developed. Each demonstrating successive improvements in accuracy (2). In a quest to further improve accuracy, the repeatable pose and high precision of robotic technology has been utilized for pedicle placement. Surgical robots fall into three control architectures(3): Supervisory controlled, telerobotic, or shared/supervisory control.
All existing robotic machines are shared control where they offer steady trajectory guidance support for the surgeon(4,5). This work explores the accuracy and precision of a supervisory control architecture 3 arm 7 DOF robot utilizing Optical Coherence Tomography (OCT) for registration to preoperative or intraoperative images for supervised pedicle instrumentation.
Early techniques relied on anatomic localization and orientation. Freehand breach rates are reported as high as 31% (1). To reduce the risk of a pedicle breach fluoroscopy, and later optical based guidance with fluoroscopy or CT scan has been developed. Each demonstrating successive improvements in accuracy (2). In a quest to further improve accuracy, the repeatable pose and high precision of robotic technology has been utilized for pedicle placement. Surgical robots fall into three control architectures(3): Supervisory controlled, telerobotic, or shared/supervisory control.
All existing robotic machines are shared control where they offer steady trajectory guidance support for the surgeon(4,5). This work explores the accuracy and precision of a supervisory control architecture 3 arm 7 DOF robot utilizing Optical Coherence Tomography (OCT) for registration to preoperative or intraoperative images for supervised pedicle instrumentation.
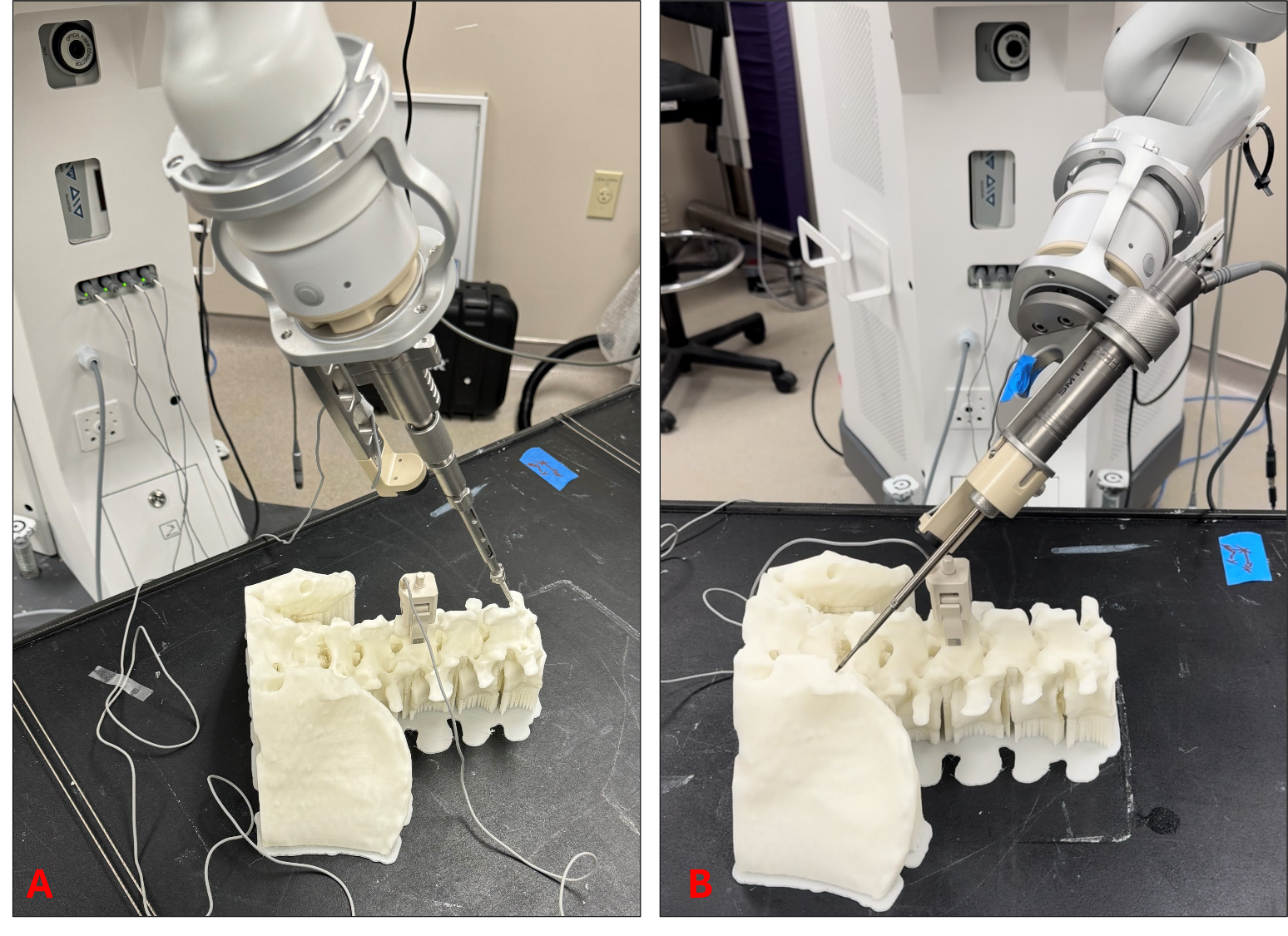
A) High torque screw driver B) Ultrasonic knife on system.
Methods
3 porcine subjects were used with L2, L3, and L4 instrumented with 4.5 x20 mm poly axial screws utilizing the robot in a scan and plan workflow. Following instrumentation all animals were observed for 24 hours with neurological assessment of hind limb function. Then after sacrifice repeat CT was done to assess post operative screw location. Screws were graded clinically utilizing the Gertzbein-Robbins Scale (GRS) clinical acceptability scale. Precision was assessed by utilizing a customized image processing pipeline to register pre and post vertebral level by level that allowed post procedural screw placement relative to planned location and trajectory. Euclidean error was calculated at screw head and screw tip. All points were normalized to a nominal screw coordinate system, allowing for removal of parallax effect. Scatter error orthonormal to the screw axis at the tip and head was utilized to construct confidence ellipses of certainty of screw axis.
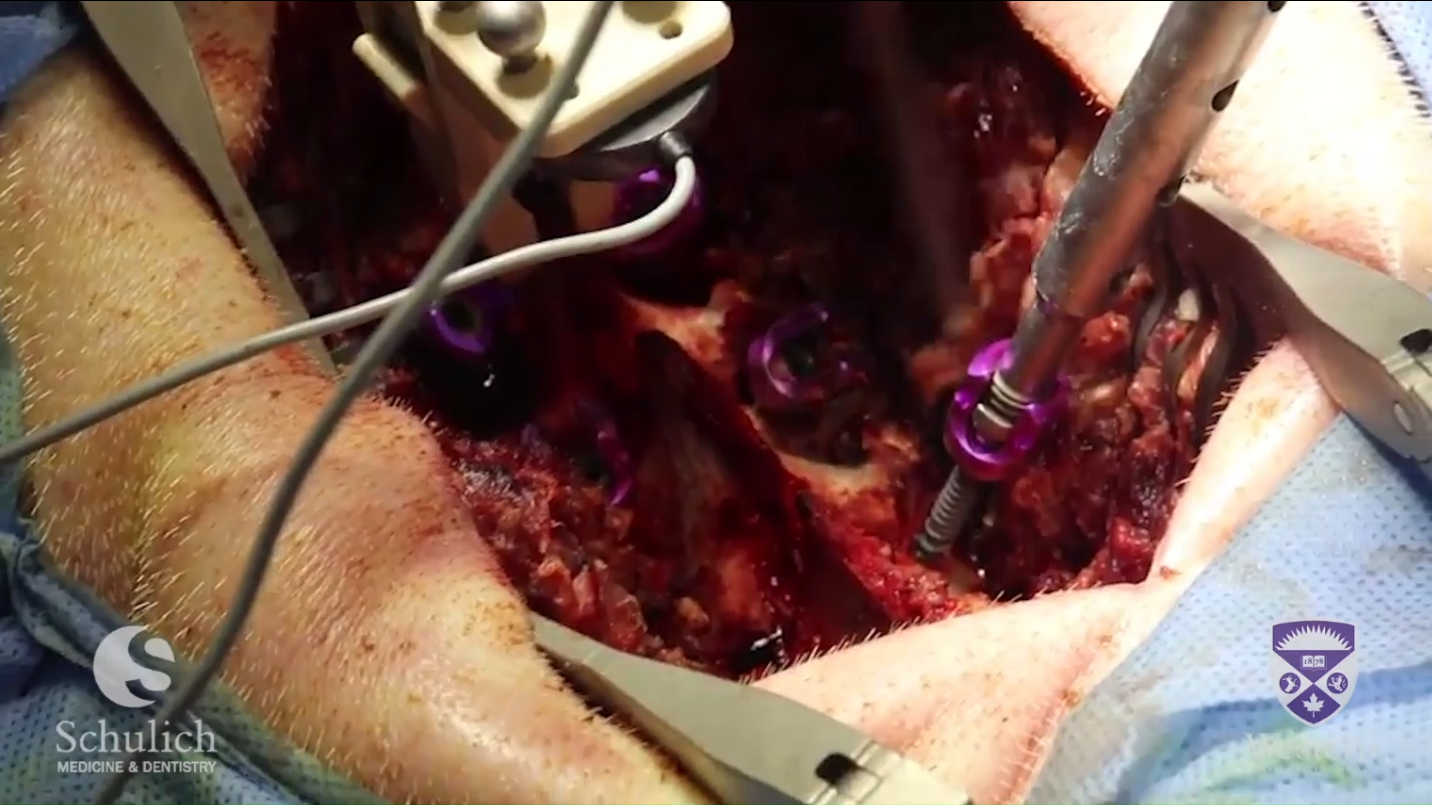
Image of autonomous screw insertion
Results
All (3/3) animals were fully neurologically intact following instrumentation at 24 hours. All (18/18) screws where GRS A with no breach of the pedicle wall. There where 0 grade B, and 0 grade C or D
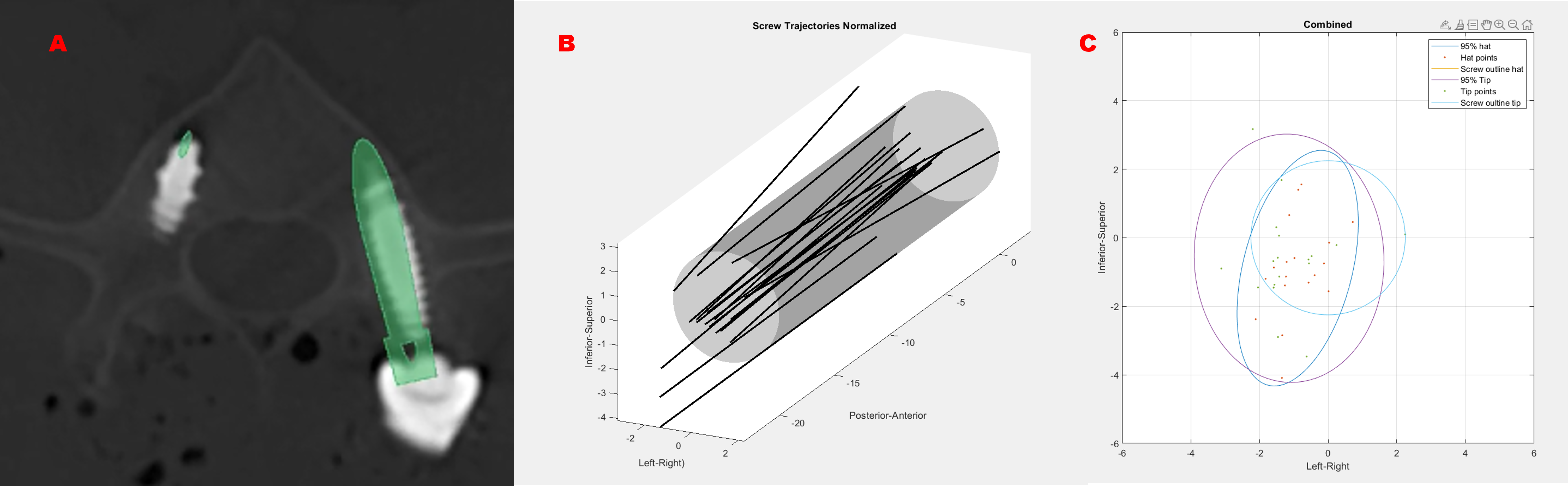
A) Planned screw trajectory in green overlaid to actual screw placement in an axial slice. B) Normalized measured screw trajectories in black, relative to 4.5 mm screw grey. C) 95% confidence bounds of tip (purple) and head (dark blue)
Mean tip and head Euclidean error where 2.47+/- 1.25 mm and 2.25 +/-1.25 mm respectively. The major and minor axes of the confidence ellipse at 99% was 2.19 mm, and 1.28 mm for the tip and 2.07 mm, and 0.42 mm for the head.
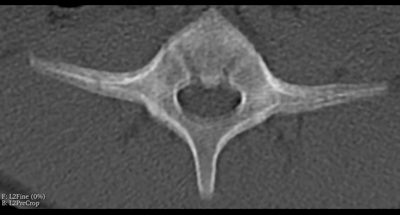
95% confidence ellipse of the screw axis location (red) relative to the outline of screw (yellow). Any violation from the ellipse will generate a breach greater tahn half of a screw diameter.
Conclusion
This work shows the first use of optical coherence tomography guidance in neurosurgery. 100% of screws obtained satisfactory clinical grading, with intact neurological function in all animals post operatively. The error encompasses all sources of error including movement in preoperative scanner of the animals, Preop to OCT measurement, pilot drilling and screw insertion. Screw axis error ellipsoids allow for estimation of safety depending on subject specific pedicle morphology. This is useful for estimating risk of pedicle breech based on patient specific anatomy moving forward.
Although limited sample size, it shows the capability of a supervisory controlled 7DOF robot with OCT registration. Further investigation is warranted to further explore robotic capabilities, sources of error, safety, and cost effectiveness.
Although limited sample size, it shows the capability of a supervisory controlled 7DOF robot with OCT registration. Further investigation is warranted to further explore robotic capabilities, sources of error, safety, and cost effectiveness.
References
1. Gelalis ID, Paschos NK, Pakos EE, Politis AN, Arnaoutoglou CM, Karageorgos AC, et al. Accuracy of pedicle screw placement: a systematic review of prospective in vivo studies comparing free hand, fluoroscopy guidance and navigation techniques. Eur Spine J. 2012 Feb;21(2):247–55.
2. Siccoli A, Klukowska AM, Schröder ML, Staartjes VE. A Systematic Review and Meta-Analysis of Perioperative Parameters in Robot-Guided, Navigated, and Freehand Thoracolumbar Pedicle Screw Instrumentation. World Neurosurg. 2019 Jul;127:576-587.e5.
3. Nathoo N, Cavuşoğlu MC, Vogelbaum MA, Barnett GH. In touch with robotics: neurosurgery for the future. Neurosurgery. 2005 Mar;56(3):421–33; discussion 421-433.
4. Yamout T, Orosz LD, Good CR, Jazini E, Allen B, Gum JL. Technological Advances in Spine Surgery: Navigation, Robotics, and Augmented Reality. Orthop Clin North Am. 2023 Apr;54(2):237–46.
5. Oppermann M, Karapetyan V, Gupta S, Ramjist J, Oppermann P, Yang VXD. The pedicle screw accuracy using a robotic system and measured by a novel three-dimensional method. J Orthop Surg. 2023 Sep 20;18(1):706.
2. Siccoli A, Klukowska AM, Schröder ML, Staartjes VE. A Systematic Review and Meta-Analysis of Perioperative Parameters in Robot-Guided, Navigated, and Freehand Thoracolumbar Pedicle Screw Instrumentation. World Neurosurg. 2019 Jul;127:576-587.e5.
3. Nathoo N, Cavuşoğlu MC, Vogelbaum MA, Barnett GH. In touch with robotics: neurosurgery for the future. Neurosurgery. 2005 Mar;56(3):421–33; discussion 421-433.
4. Yamout T, Orosz LD, Good CR, Jazini E, Allen B, Gum JL. Technological Advances in Spine Surgery: Navigation, Robotics, and Augmented Reality. Orthop Clin North Am. 2023 Apr;54(2):237–46.
5. Oppermann M, Karapetyan V, Gupta S, Ramjist J, Oppermann P, Yang VXD. The pedicle screw accuracy using a robotic system and measured by a novel three-dimensional method. J Orthop Surg. 2023 Sep 20;18(1):706.
Special thanks to the following for their technical support:
K. Lee,C. Leung , K. Pusevetov, and J. Patel.
K. Lee,C. Leung , K. Pusevetov, and J. Patel.
Utility of Neurophysiology in the Diagnosis of Tethered Cord Syndrome (TCS)
Background
-Tethered cord syndrome (TCS) is a clinical condition of classic neurologic, orthopedic and urologic symptoms and signs resulting from abnormal tension on the spinal cord.
-Occult tethered cord syndrome (OTCS) is when a child has some or many clinical findings of tethered cord syndrome but no corresponding radiographic abnormality to indicate a tethered cord1–4.
-The existence and management of OTCS is controversial. 5
-Diagnosis of both TCS and OTCS in children typically involves a three-pronged approach-
1) Clinical signs and symptoms
2) Radiographical assessment with MRI of the neuroaxis to assess for features of occult spinal dysraphism
3) Neurophysiological assessment with transcranial electric stimulation (TES) to obtain somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) under general anesthetic.
-Neurophysiological assessment is often requested when there is a conflict between the clinical picture and the imaging results (eg in OTCS), or when there is another coexisting diagnosis that could explain the clinical picture (e.g. autism spectrum disorder and toe walking).
- In patients with TCS, MEPs to the lower extremities and sphincter may be abnormal due to the tethering of the spinal cord6.
-Transcranial magnetic stimulation (TMS) is a novel technique that uses magnetic fields to stimulate nerve cells in the brain, and sticker electrodes to record the responses in the upper and lower extremities.
-Occult tethered cord syndrome (OTCS) is when a child has some or many clinical findings of tethered cord syndrome but no corresponding radiographic abnormality to indicate a tethered cord1–4.
-The existence and management of OTCS is controversial. 5
-Diagnosis of both TCS and OTCS in children typically involves a three-pronged approach-
1) Clinical signs and symptoms
2) Radiographical assessment with MRI of the neuroaxis to assess for features of occult spinal dysraphism
3) Neurophysiological assessment with transcranial electric stimulation (TES) to obtain somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) under general anesthetic.
-Neurophysiological assessment is often requested when there is a conflict between the clinical picture and the imaging results (eg in OTCS), or when there is another coexisting diagnosis that could explain the clinical picture (e.g. autism spectrum disorder and toe walking).
- In patients with TCS, MEPs to the lower extremities and sphincter may be abnormal due to the tethering of the spinal cord6.
-Transcranial magnetic stimulation (TMS) is a novel technique that uses magnetic fields to stimulate nerve cells in the brain, and sticker electrodes to record the responses in the upper and lower extremities.
Methods
- We describe a novel diagnostic technique to provide evidence that an occult TCS is causing the patient’s symptoms.
- We studied pediatric patients recruited from the office of two pediatric neurosurgeons (JR and AV).
- All of our patients had clinical equipoise regarding whether their spinal cord caused their symptoms. The MRI demonstrated no convincing finding of a tethered spinal cord.
- TMS was done in an outpatient setting. The children were seen by a single neurophysiologist (JN).
- Surface EMG electrodes are placed over the leg muscles. The tibial anterior and gastrocnemius are the target muscles. A double-cone coil is held over the vertex of the head. Stimulation is applied at 80% of maximal stimulation output, and responses are measured. The entire procedure takes approximately 5 minutes.
- We studied pediatric patients recruited from the office of two pediatric neurosurgeons (JR and AV).
- All of our patients had clinical equipoise regarding whether their spinal cord caused their symptoms. The MRI demonstrated no convincing finding of a tethered spinal cord.
- TMS was done in an outpatient setting. The children were seen by a single neurophysiologist (JN).
- Surface EMG electrodes are placed over the leg muscles. The tibial anterior and gastrocnemius are the target muscles. A double-cone coil is held over the vertex of the head. Stimulation is applied at 80% of maximal stimulation output, and responses are measured. The entire procedure takes approximately 5 minutes.
Results
Subjects
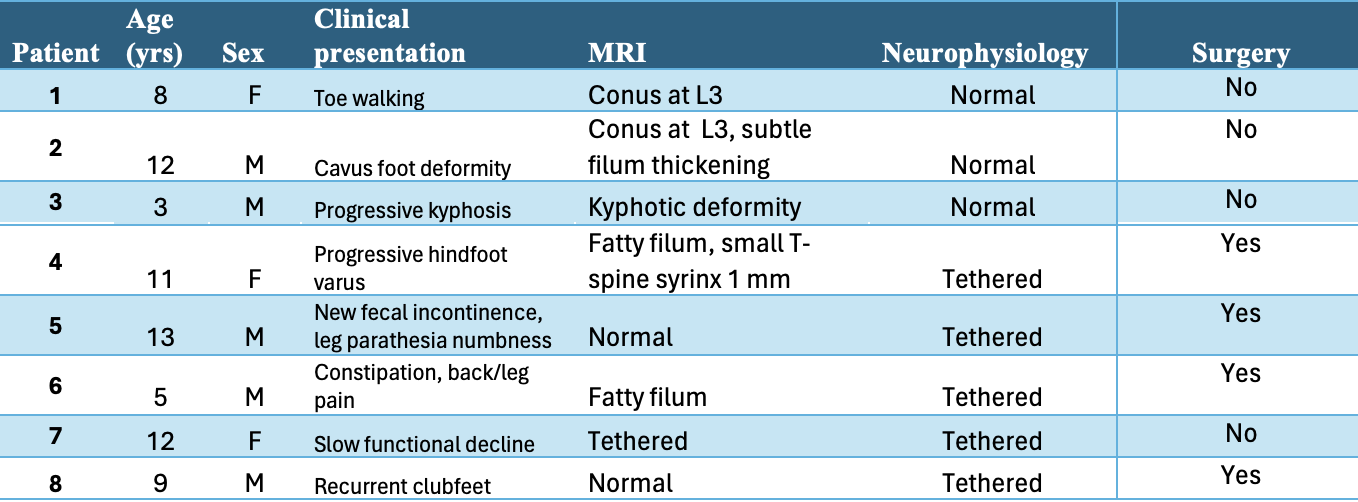
Discussion
-The diagnosis of TCS and OTCS in children is sometimes contentious and difficult.
-Detethering surgery is associated with some significant risks, so the accurate selection of patients who would benefit from surgery is important in ambiguous cases.
-Neurophysiology can help to diagnose TCS and guide patient selection and surgical decision-making in patients with ambiguous clinical and/or radiographic presentations.
-Transcranial magnetic stimulation is a much less invasive and laborious option to other types of neurophysiological testing.
-This study has limitations. It is a small case series with a diverse patient population, and given the novel introduction of this diagnostic test, we have limited long-term outcome data.
-Detethering surgery is associated with some significant risks, so the accurate selection of patients who would benefit from surgery is important in ambiguous cases.
-Neurophysiology can help to diagnose TCS and guide patient selection and surgical decision-making in patients with ambiguous clinical and/or radiographic presentations.
-Transcranial magnetic stimulation is a much less invasive and laborious option to other types of neurophysiological testing.
-This study has limitations. It is a small case series with a diverse patient population, and given the novel introduction of this diagnostic test, we have limited long-term outcome data.
Conclusion
TMS is a useful diagnostic technique to aid in surgical decision-making regarding ambiguous cases of pediatric patients who would have symptoms of TCS.
References
1. Michael MM, Garton AL, Kuzan-Fischer CM, Uribe-Cardenas R, Greenfield JP. A critical analysis of surgery for occult tethered cord syndrome. Childs Nerv Syst. 2021;37:3003-3011.
2. Rezaee H, Keykhosravi E. Effect of untethering on occult tethered cord syndrome: a systematic review. Br J Neurosurg. 2022;36(5):574-582.
3. Steinbok P, Garton HJ, Gupta N. Occult tethered cord syndrome: a survey of practice patterns. J Neurosurg Pediatr. 2006;104(5):309-313.
4. Tu A, Steinbok P. Occult tethered cord syndrome: a review. Childs Nerv Syst. 2013;29(9):1635-1640. doi:10.1007/s00381-013-2129-1
5. Drake JM. Occult tethered cord syndrome: not an indication for surgery. J Neurosurg Pediatr. 2006;104(5):305-308.
6. Leung V, Pugh J, Norton JA. Utility of neurophysiology in the diagnosis of tethered cord syndrome. J Neurosurg Pediatr. 2015;15(4):434-437.
2. Rezaee H, Keykhosravi E. Effect of untethering on occult tethered cord syndrome: a systematic review. Br J Neurosurg. 2022;36(5):574-582.
3. Steinbok P, Garton HJ, Gupta N. Occult tethered cord syndrome: a survey of practice patterns. J Neurosurg Pediatr. 2006;104(5):309-313.
4. Tu A, Steinbok P. Occult tethered cord syndrome: a review. Childs Nerv Syst. 2013;29(9):1635-1640. doi:10.1007/s00381-013-2129-1
5. Drake JM. Occult tethered cord syndrome: not an indication for surgery. J Neurosurg Pediatr. 2006;104(5):305-308.
6. Leung V, Pugh J, Norton JA. Utility of neurophysiology in the diagnosis of tethered cord syndrome. J Neurosurg Pediatr. 2015;15(4):434-437.
Transfer RNA fragments in patient plasma extracellular vesicles as biomarkers of high grade glioma

INTRODUCTION
• High-Grade Gliomas (HGG) are notorious for poor patient outcomes (15-18 months). Following invasive surgical resection, patients undergo radiation/chemotherapy treatment1. The majority of patients progress within 10 months.
• Cells in the tumor microenvironment (TME) communicate to each other to establish and maintain a pro-tumorigenic environment2.
• Extracellular vesicles (EVs) and their cargo (protein, RNA), released by HGGs have been shown to facilitate cell to cell communication to maintain a pro-tumorigenic environment2.
• The contents of these EVs may serve as biomarkers of HGG disease and therapeutic targets in the future.
• Here we classify in 10 HGG patient the Transfer RNA fragments (TfRNA) found in patient plasma EVs compared to 4 non-cancer controls at the time of diagnosis.
• TfRNA have been shown to regulate many process in cancer including inhibiting or increasing translational efficiency, acting as miRNA, modulating invasion, preventing apoptosis and regulating transcription3.
METHODS
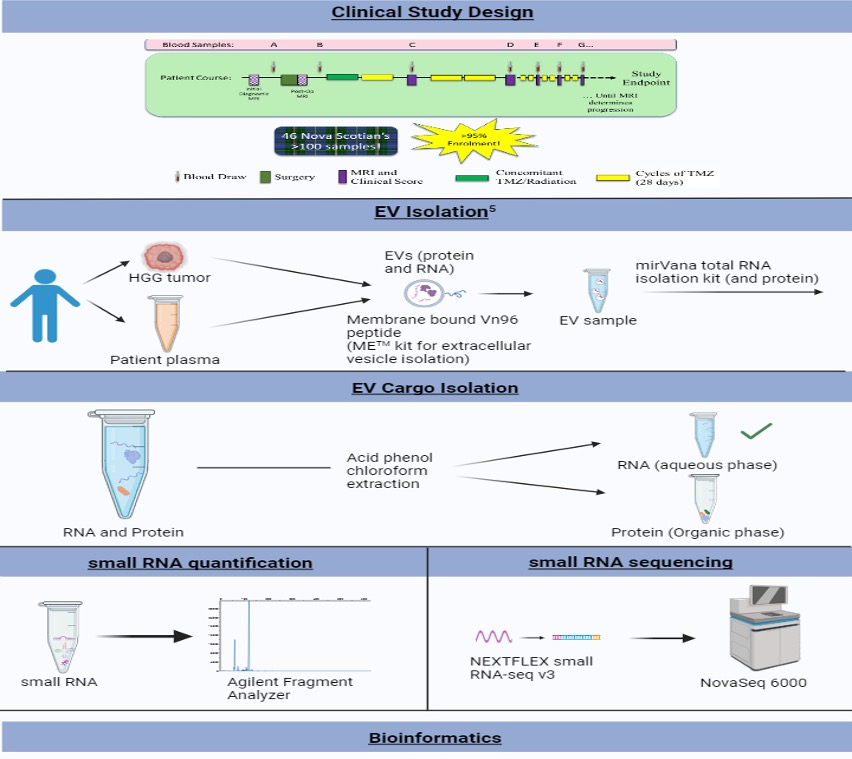
RESULTS
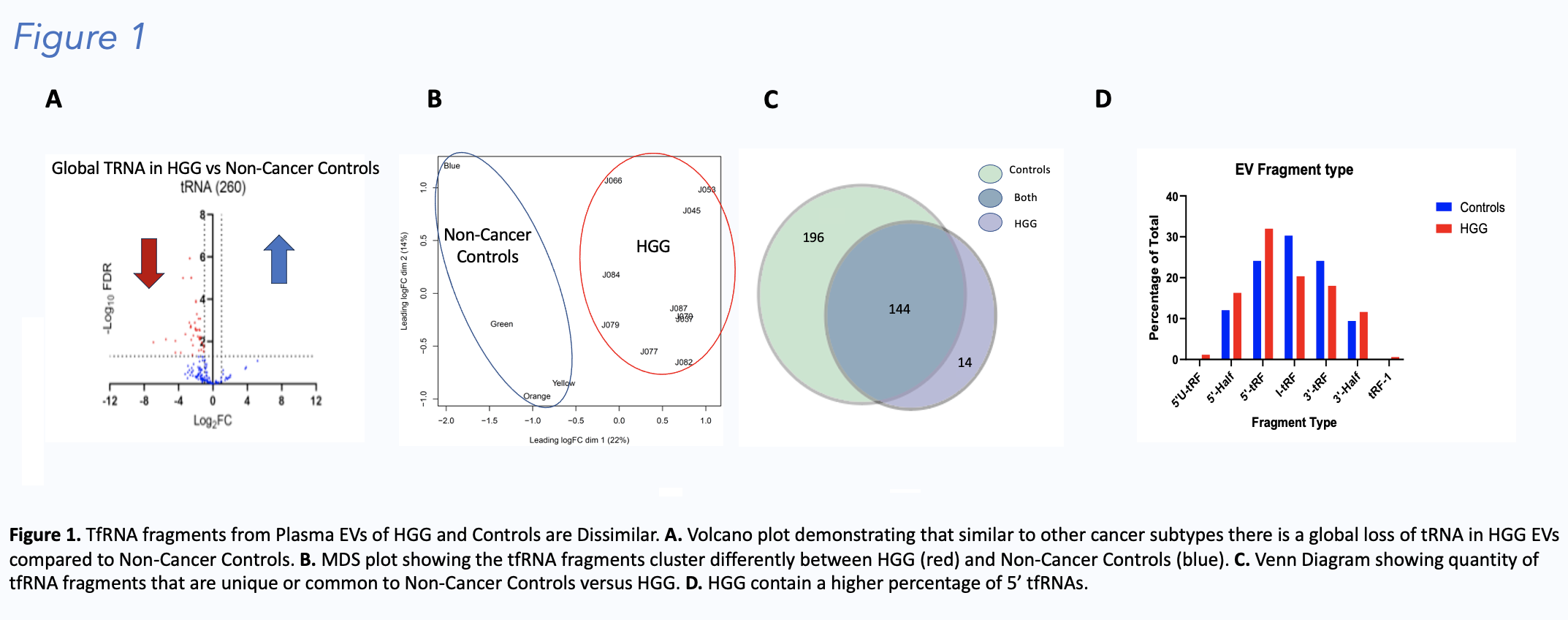


DISCUSSION
• High-Grade Gliomas (HGG) have globally less tfRNA contained in plasma EVs compared to non-cancer controls. This finding is similar to findings in other cancers4.
• tfRNA from HGG contain more 5’ tfRNA compared to non-cancer controls. This is accompanied by a decrease in the amount of I-tRFs and 3’-tRFs.
• Despite a global loss of tfRNA there are certain tfRNA that are significantly differentially expressed or sorted to EVS in HGG and these could serve a biomarkers or therapeutic targets in the future.
• Two different tfRNA fragments from the same parent TRNA molecule are differentially expressed in HGG versus non-cancer controls suggesting increased or decreased expression of the parent tRNA alone does not account for differences between HGG and Control tfRNA expression.
FUTURE DIRECTIONS
• Tracking plasma tfRNA EV expression through HGG disease progression to further understand their potential role as biomarkers
• Analyzing tfRNA expression in the matching tumour tissue is ongoing in our laboratory
• Functional studies to understand the role of tfRNA fragments on tumour and tumour associated cells are being undertaken.
REFERENCES
1. Stupp R, Mason W, et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N Engl J Med. 2005 Mar;352:987-996.
2. Guo X, Sui R, Piao H. Exosomes-mediated crosstalk between glioma and immune cells in the tumor microenvironment. CNS Neurosci Ther. 2023 Aug;29(8):2074-2085.
3. Lee, S., Kim, J., Valdmanis, P.N. et al. Emerging roles of tRNA-derived small RNAs in cancer biology. Exp Mol Med 55, 1293–1304 (2023).
4. Zhou Y, Zhou B, Pache L, Chang M, Khodabakhshi AH, Tanaseichuk O, Benner C, Chanda SK. Metascape provides a biologist-oriented resource for the analysis of systems-level datasets. Nat Commun. 2019 Apr 3;10(1):1523.

Improving care for patients with Neurofibromatosis 1 in British Columbia
Background
Neurofibromatosis 1 (NF1) is a multisystem, neurocutaneous disorder with a predisposition for various malignancies. It is caused by a mutation of the NF1 gene on chromosome 17q11.2 (Ferner et al., 2007). Dysfunction of the NF1 gene causes a loss of Neurofibromin, a tumour suppressor protein (Hirbe et al., 2014). Patients with NF1 have increased morbidity and mortality with a reduced average life expectancy of 8-15 years. This is in part due to the predisposition to malignant peripheral nerve sheath tumours and breast cancer. Vasculopathy, cardiac, renal dysfunction, cognitive impairment and neuropsychiatric conditions are notable comorbidities (Stewart et al., 2018). This disorder affects between 1:2000 to 1:3000 people worldwide. We estimate that there are between 1800 - 2700 people with NF1 in British Columbia.
Currently, there is no established care pathway or multidisciplinary clinic for adult patients with NF1 in BC. Patients may miss timely screening or therapeutic interventions. The development of new therapies for NF1 highlights the urgency for coordinated care.
A multidisciplinary working group was created. It includes a neuromuscular neurologist, adult neuro-oncologist, pediatric neuro-oncologist, medical geneticist, and neuro-ethics researchers. A three-prong approach to address identified gaps was developed

NF1 Focus Groups
Description: This is an explorative descriptive study using focus groups. It received approval from the UBC Research Ethics Board and the Vancouver Coastal Health Research Institute.
Primary objectives:
1. To assess the current health-related needs of adults with NF1 in BC.
2. To explore the opinions and perceptions of the relevant stakeholders regarding future improvements to the health care provided to patients with NF1 in BC.
Methodology: We created two focus groups. One group with adult patients with NF1 and another group for physicians. The prospective patient participants were identified through the shared electronic medical record system of Dr. Kristine Chapman and the Vancouver General Hospital Neuromuscular Disease Unit. The prospective physician participants were identified through internal discussions by the study group members. All prospective participants were contacted through email with a letter of initial contact. The focus groups were audio-recorded and transcribed. The data has been collected and is in the process of undergoing thematic analysis.
Preliminary Results:
Patient Focus Group themes:
- Difficulties finding physicians who can quarterback their care.
- Difficulties accessing timely care and investigations.
- Patients want more information and resources. Currently, they get information from the BC Tumour Foundation and Facebook groups.
Physician Focus Group themes:
- Healthcare delivery to adult patients with NF1 in BC is fragmented.
- Limited evidence makes it challenging to decide on appropriate investigations and treatments.
Care Pathway and Recommendations
The following is a summary of the recommended diagnostic investigations and management for adults with NF1 in BC. Note that recommendations are subject to change as new evidence arises.
Each patient should have an annual assessment from a primary care provider with a thorough medical history, and physical examination. In addition, we recommend an evaluation of possible complications of NF1 (see Recommendations).
The Neurofibromatosis Case Conference
Description: We have developed a quarterly, multidisciplinary, one-hour, virtual meeting that is CME-approved. This has been operational since December 2023.
Case Conference Objectives:
Early Experiences:
Case Conference Objectives:
- Discuss clinical cases of patients with NF1 or NF2 where there is clinical or diagnostic equipoise or challenge
- Enhance understanding of the multi-disciplinary management of patients with NF1/NF2
- Apply current scientific and medical literature regarding neurofibromatosis to the presented cases
- Discuss clinical procedures as they apply to presented cases, in an effort to enhance clinical care of future patients
Early Experiences:
- 3 meetings have been completed.
- Attended by an average of 20 participants, from various health authorities and disciplines in BC.
- Subspecialist attendance have included the following: Medical oncology, Radiation oncology, Neuro-oncology, Neuro-ophthalmology, Neuromuscular neurology, Neuropathology, Neuroradiology, Neurosurgery, Pediatric neurology, and Plastic surgery.
Concomitant corticosteroid use in ravulizumab-treated adults with anti-AChR antibody-positive gMG: results from the CHAMPION MG open-label extension
BACKGROUND
- Approximately 85% of patients with gMG have autoantibodies against anti-acetylcholine receptor (AChR),1 leading to activation of the complement system and damage of the postsynaptic membrane of the neuromuscular junction2
-
Generalized myasthenia gravis (gMG) treatment options include nonspecific immunosuppression with corticosteroids, which are associated with adverse effects, particularly with long-term use of high doses and in patients with comorbidities1,3
- Guidelines recommend steroid-sparing agents when corticosteroids are ineffective, contraindicated, or intolerable4
- In the phase 3 CHAMPION MG study in adults with AChR antibody-positive (AChR-Ab+) gMG, ravulizumab, a C5 inhibitor administered every 8 weeks, demonstrated rapid and significant symptom improvement versus placebo and was well tolerated5
OBJECTIVE
- To evaluate changes in corticosteroid use in adults with AChR-Ab+ gMG treated with ravulizumab
METHODS
Figure 1. CHAMPION MG Study Design5,6
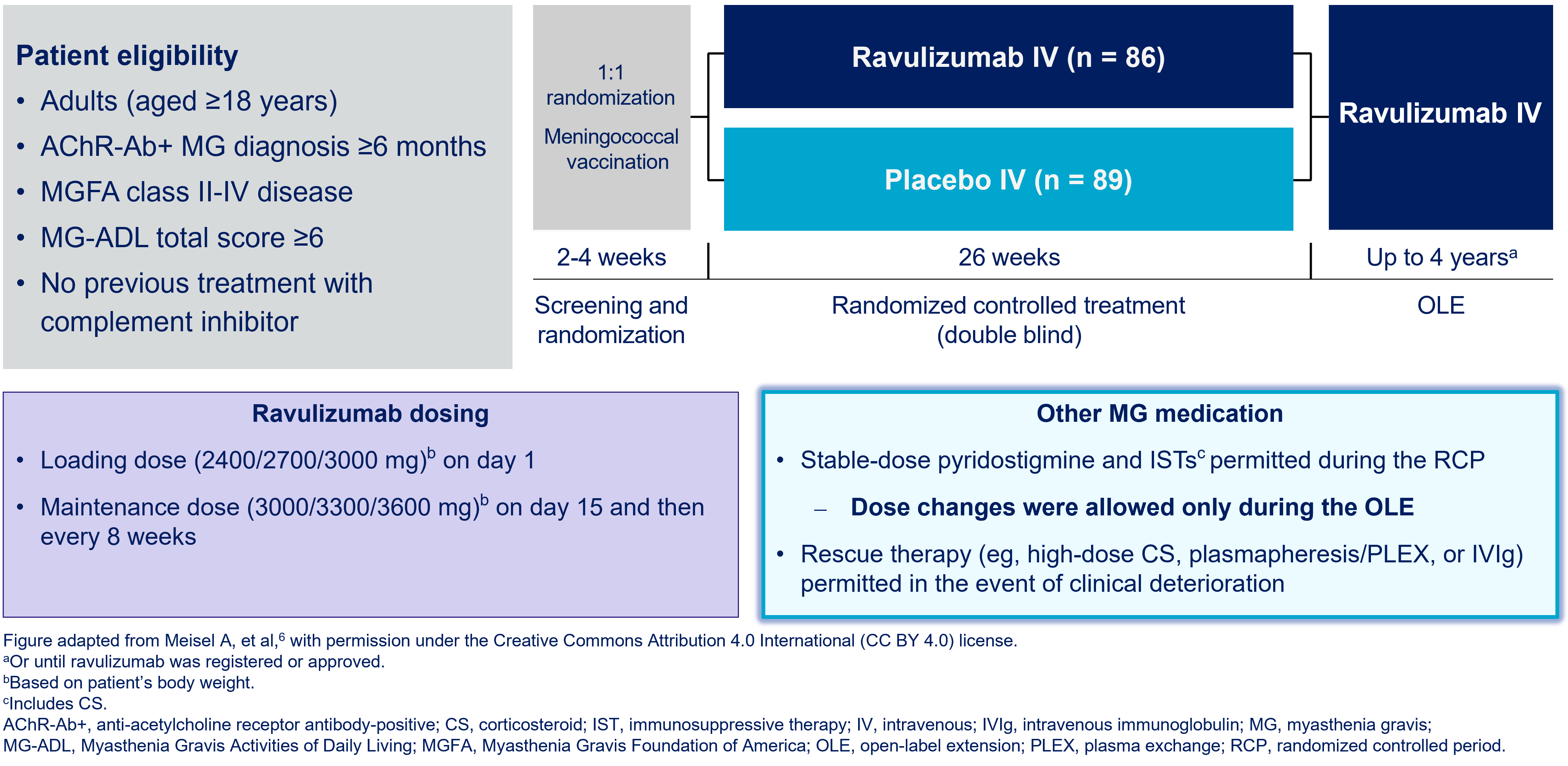
Figure 2. Study Analyses

RESULTS
Table 1. Baseline Characteristics of Patients in the OLE2
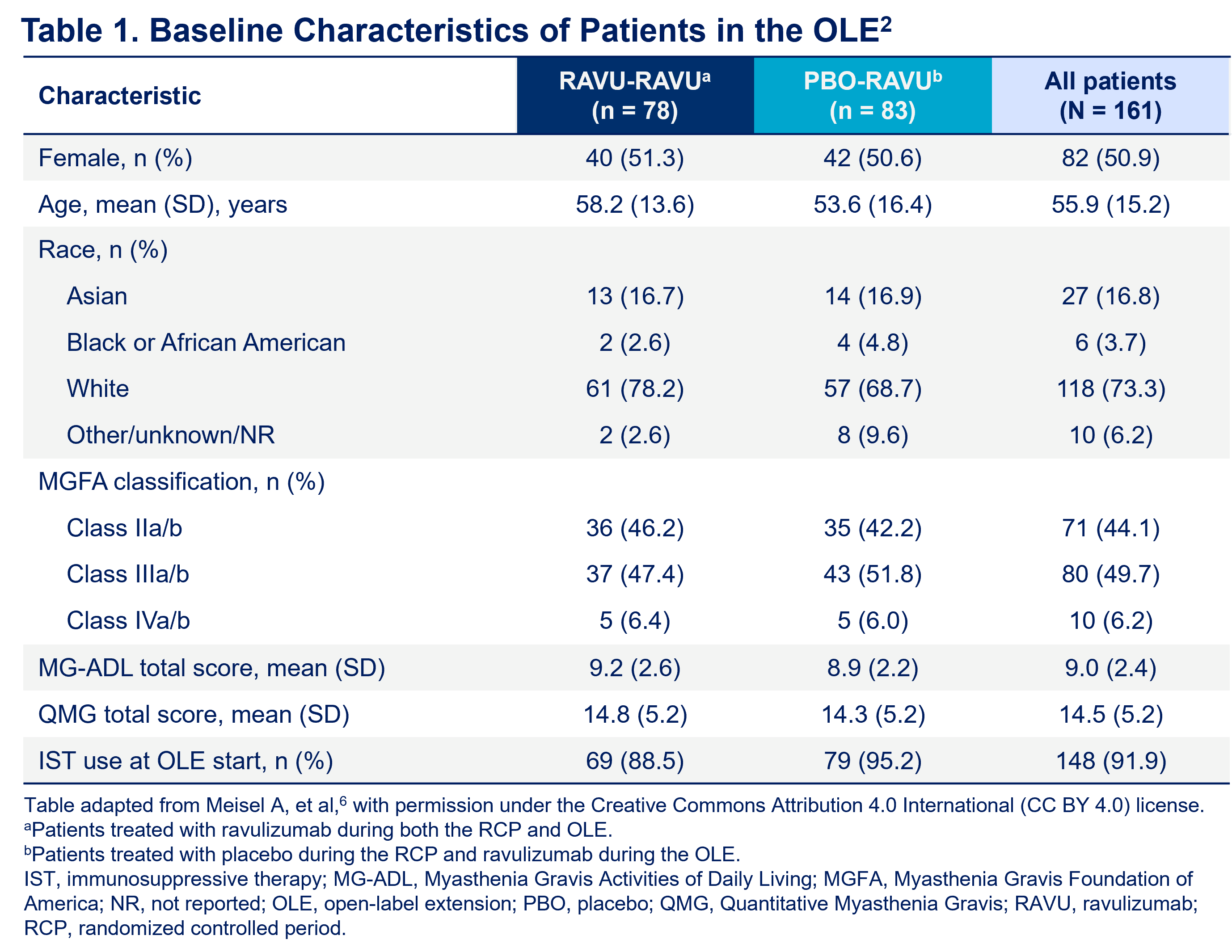
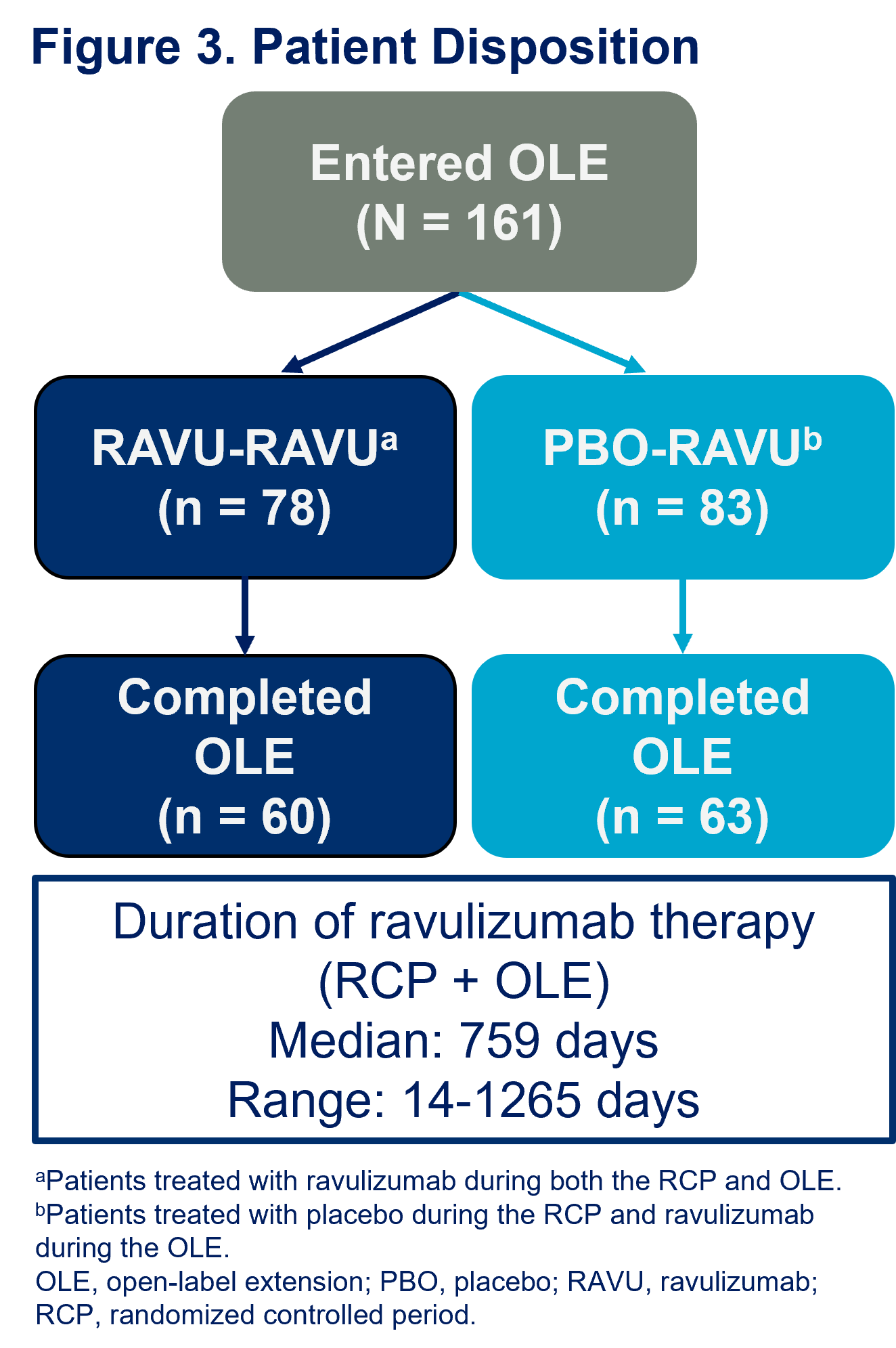
-
During the OLE, 113 patients received oral or enteral CS
- 112 were receiving corticosteroids at the start of the OLE
-
At first reported dose:
- 11 patients (10%) were receiving ≤5 mg/day
- 47 patients (42%) were receiving ≤10 mg/day
-
At last reported dosea:
- 35 patients (31%) were receiving ≤5 mg/day
- 71 patients (63%) were receiving ≤10 mg/day
Figure 4. Changes in Daily Corticosteroid Doses With Ravulizumab During the OLE
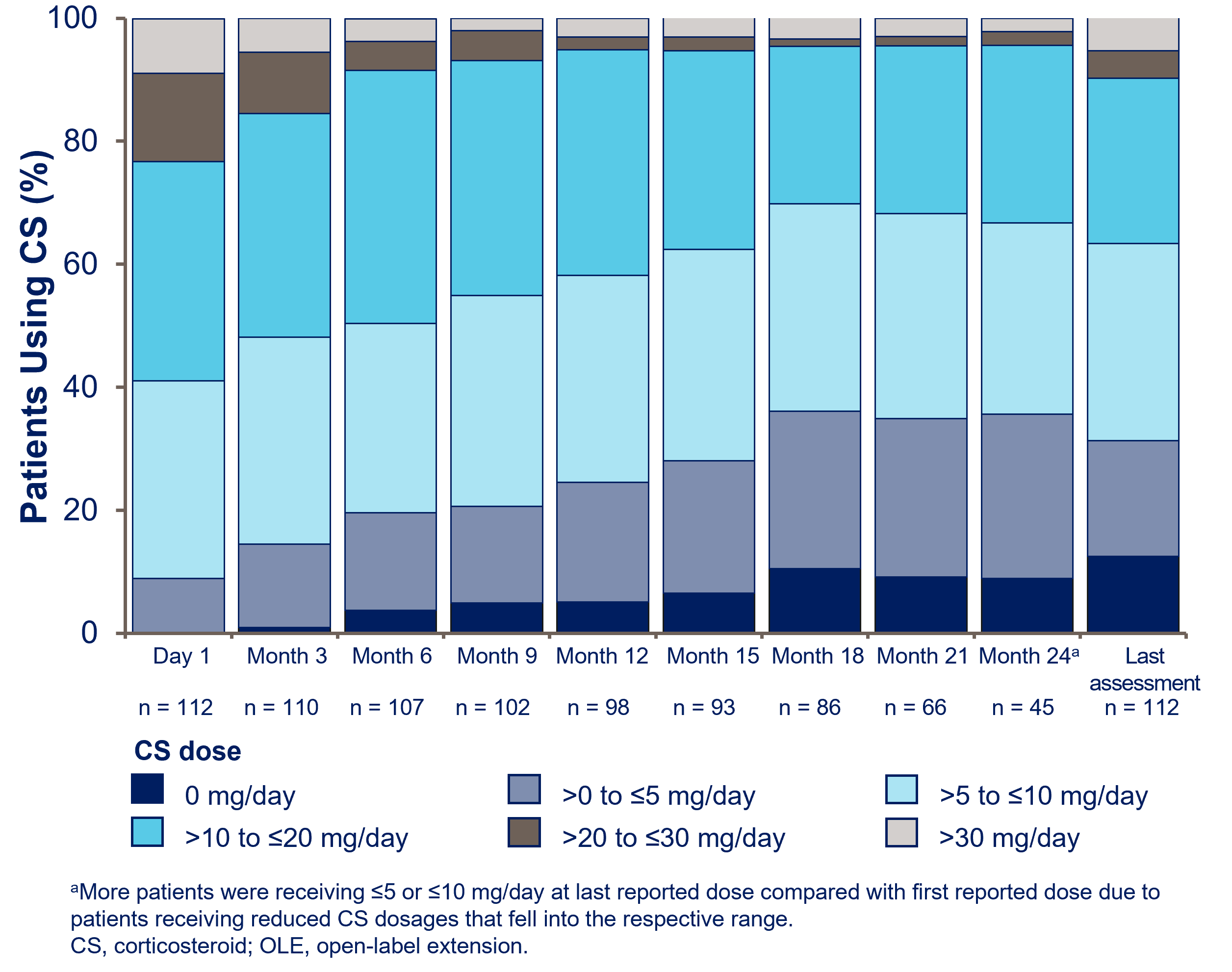
-
Mean (SD) daily dose of corticosteroid:
- First OLE dosage: 17.5 (11.9) mg/day
- Last reported dosage: 11.7 (10.9) mg/day
- Among patients taking corticosteroid at the start of the OLE (n = 113), 12.4% (n = 14) had discontinued by their last assessment
Figure 5. CS Dose Decrease With Ravulizumab in the OLE
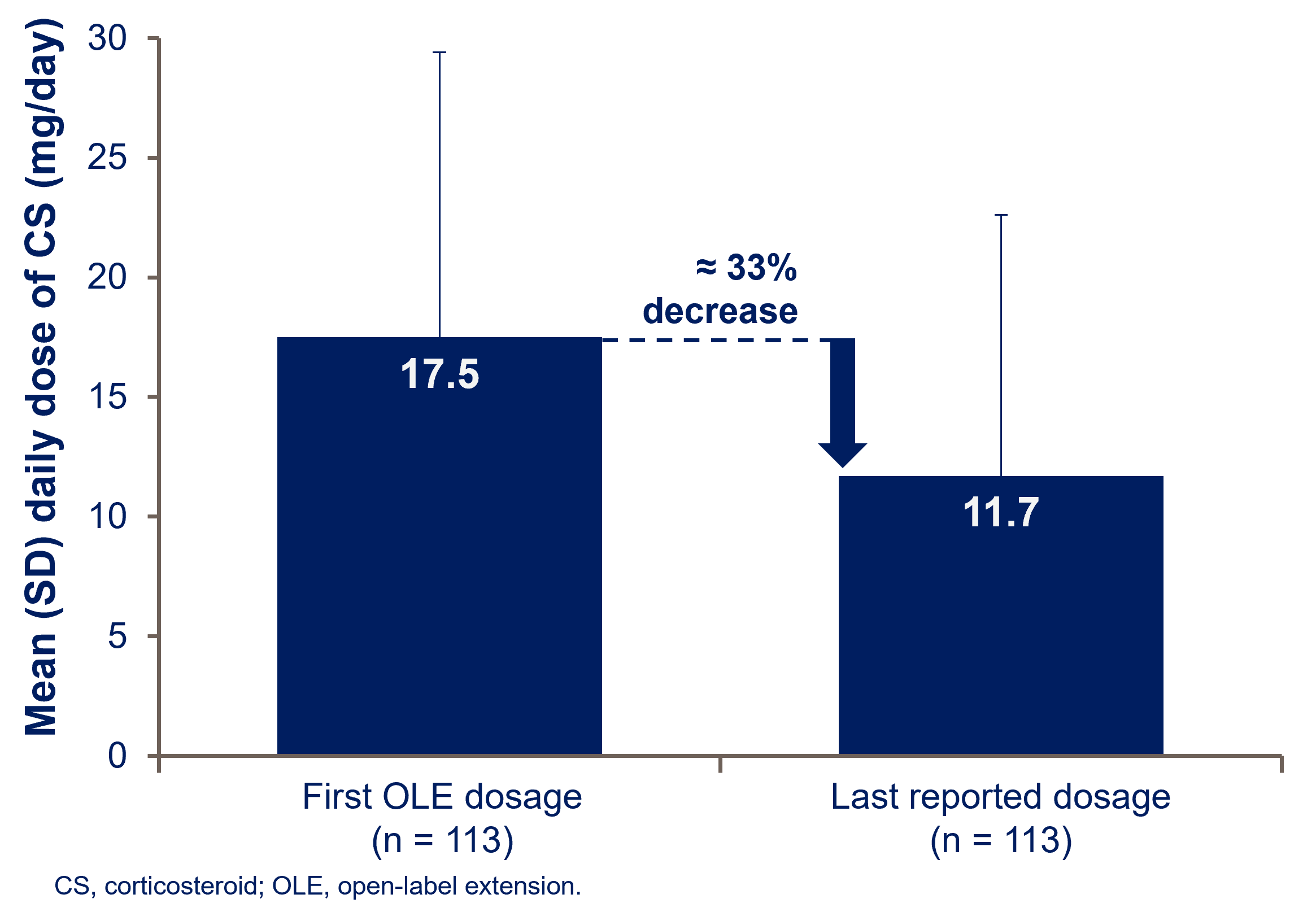
- Among patients taking azathioprine (AZA) at the start of the OLE (n = 39), 7.7% (n = 3) had discontinued AZA by their last assessment
- Among patients taking mycophenolate mofetil (MMF) at the start of the OLE (n = 46), 6.5% (n = 3) had discontinued MMF by their last assessment
Figure 6. AZA and MMF Dose Decreases With Ravulizumab in the OLE

CONCLUSIONS
-
Decreased corticosteroid use was observed in patients with AChR-Ab+ gMG who were treated with ravulizumab during the CHAMPION MG OLE
- Some patients were able to discontinue corticosteroids completely
- Daily doses of AZA and MMF were also reduced in patients treated with ravulizumab during the OLE
- Overall, these findings suggest a steroid-sparing role for ravulizumab